Francesco Prati, Flavio Giuseppe Biccirè
Stents and scaffolds
Updated on May 13, 2021
Percutaneous coronary interventions were revolutionised by the introduction of coronary stents, which were designed to prevent many of the acute complications of balloon angioplasty. Despite their proven benefits in the acute setting, the initial bare metal stent devices were associated with neointimal hyperplasia due to deep arterial injury giving rise to in-stent restenosis in 20-30% of cases. The latter was one of the primary driving forces behind the development of drug-eluting stents with controlled release of anti-proliferative agents released from polymers directly immobilized on the stent surface. Early generation drug-eluting stents releasing sirolimus or paclitaxel successfully addressed the problem of restenosis by reducing the need of repeat revascularization by 50-70% compared with bare metal stents in nearly all patient and lesion subsets. However, safety concerns were raised in relation to their potential to delay arterial healing and to increase the risk of very late stent thrombosis. These concerns prompted modifications to stent design and have resulted in a wide array of newer generation drug-eluting stents which utilise novel anti-proliferative agents, modified stent platforms and polymers with improved biocompatibility and clinical outcomes. This chapter reviews the data supporting the use of current and newly developed drug-eluting coronary stents.
The safety and efficacy of percutaneous coronary interventions (PCI) has improved continuously over the last 40 years. The growth of PCI reflects its widespread acceptance as the preferred revascularization strategy surpassing coronary artery bypass surgery (CABG). The advent of stents has improved the safety of PCI considerably by eliminating peri-procedural vessel closure due to dissections and the need for emergency CABG. The basic mechanism of actions of coronary artery stents are common to all platforms:
The term "stent" was coined in 1916 by Johannes F. Esser, a Dutch plastic surgeon referring to a dental impression compound formerly invented by the English dentist Charles T. Stent. The first vascular stent was developed and implanted in 1968 by Charles T. Dotter in a canine popliteal artery. The first coronary stent resulted from discussions between Hans Wallsten and Ake Senning, two Swedish expatriates in Switzerland, the former a paper engineer and the latter chief cardiac surgeon collaborating with Andreas Grüntzig during the first coronary angioplasties in Zurich, Switzerland. The very first coronary stent, called the Wallstent, was self-expanding and was developed by Medinvent in cooperation with Ulrich Sigwart. It was first implanted by Jacques Puel (Toulouse, France) in March 1986 in a 63 year old male suffering from restenosis after plain balloon angioplasty of the left anterior descending artery (Figure 1). The first bail-out stenting was performed by Ulrich Sigwart during a live course in June 1986 in a 50 year old female suffering from occlusive dissection of the left anterior descending artery after balloon angioplasty. The use of bare metal stents increased continuously, however in-stent restenosis was not infrequent, and limited the indications for its use. Further research led to the development of the combination of a metallic platform, a polymer and a drug released from the polymer, which showed effective inhibition of smooth muscle cells proliferation, dramatically reducing rates of restenosis and improving long-term clinical outcomes.
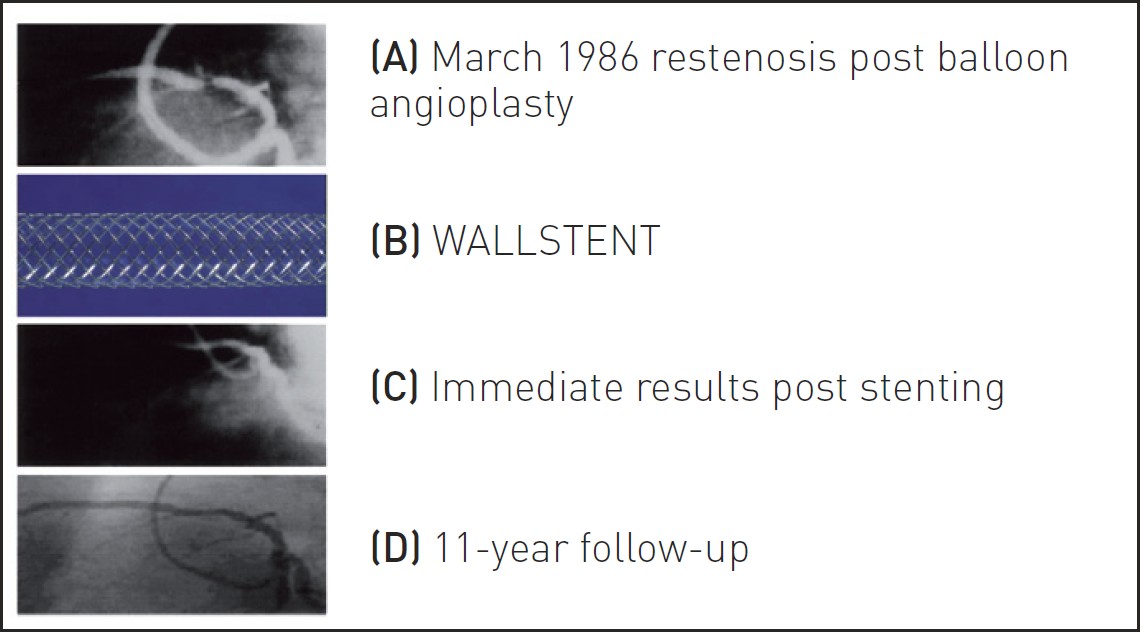
First human coronary stent implantation in March 1986. (a) Restenosis post balloon angioplasty (b) Self-expanding WALLSTENT (c) Immediate results post stent (d) Angiographic results at 11-year follow-up.
The Gianturco-Roubin stent, a balloon-expandable stent had a coil design manufactured from a single strand of stainless-steel wire. The stent was approved in the United States in 1993 for the treatment of coronary dissections during balloon angioplasty. Similar to the Wallstent, the Gianturco-Roubin stent had a great degree of flexibility but poor radial strength resulting in increased rates of restenosis as well as stent thrombosis (ST).
In the late 1980s, Julio C. Palmaz, an Argentinian radiologist - designed a vascular stent from a model taken from a piece of metal. Together with Richard A. Schatz, a cardiologist from San Antonio (Texas, USA), he modified the initial version of this prototype to bend the first tubular slotted design balloon-expandable coronary stent. In October 1987, the first peripheral Palmaz-Schatz stent was placed in Freiburg (Germany) and in December of the same year the first Palmaz-Schatz stent was implanted into a coronary artery in Sao Paolo, Brazil. The stents were manually crimped on the balloon by the interventional cardiologists, a method which resulted in frequent stent loss.
The widespread acceptance of coronary artery stenting resulted from the results of the BElgian NEtherlands STENT (BENESTENT) and the STent REStenosis Study (STRESS) trials, which showed superiority of stents compared with balloon angioplasty in terms of restenosis and need for repeat revascularization. Since then, tremendous progress has been made in improving stent material, design and processing resulting in superior deliverability and procedural success. The improved results with coronary artery stenting over time were also related to expansion of the indications for stent implantation and the discovery that dual antiplatelet therapy (DAPT) (instead of oral anticoagulation) lowered both the incidence of ST and haemorrhagic complications (Figure 2) . Of note, these studies also strongly suggested that platelets had a mechanistic role in the pathogenesis of ST. Based on their efficacy, coronary artery stents have emerged as the preferred tool of PCI and are currently deployed in more than 90% of procedures.
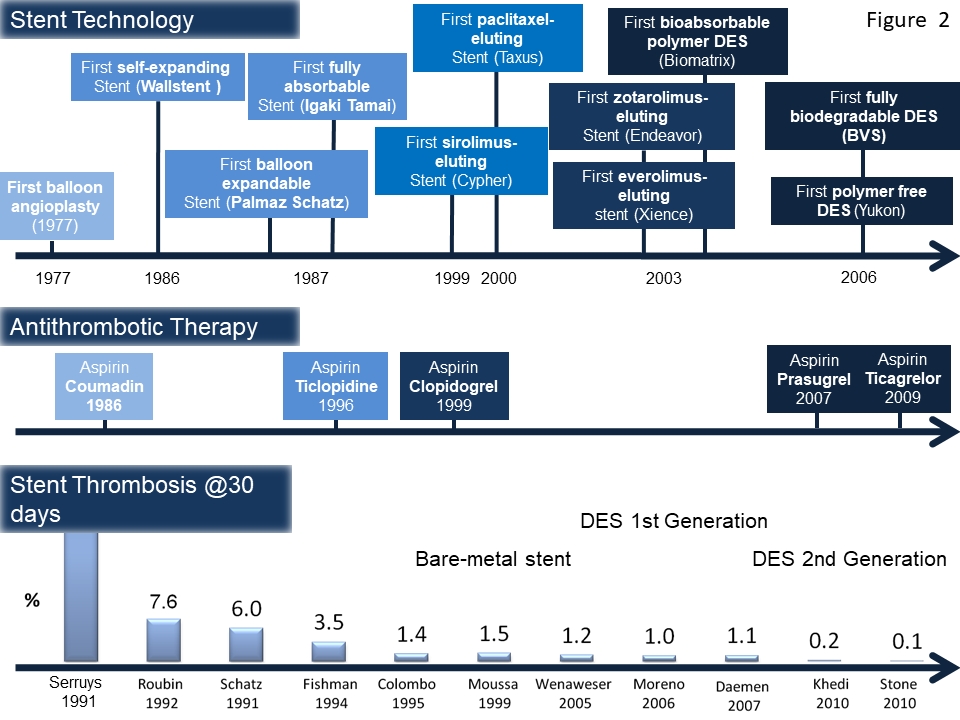
Historical overview of the most prominent advances in stent technology and antithrombotic drug regimens. Both the on-going improvements in coronary stent technology and advances in antithrombotic therapy have improved the safety outcomes as illustrated by the declining 30-day rate of ST in clinical trials in the lower panel.
Drug-eluting stents (DES) have been introduced offering site-specific, controlled delivery of therapeutic agents (Figure 2). Heparin was used initially as a coating material on stents in an attempt to reduce their thrombogenic potential and thus reduce the risk of early ST as confirmed by the results from initial studies. When used in the setting of acute myocardial infarction (AMI), one study showed a reduced rate of ST and recurrent myocardial infarction (MI). Although heparin has proven anti-inflammatory effects in addition to its anticoagulant properties, no benefit was observed in terms of restenosis. Sirolimus-eluting stents (SES) were first implanted in humans in 2001 and subsequently became the first Food and Drug Administration (FDA) approved DES that significantly reduced the risk of restenosis compared with bare metal stents (BMS). This was followed by a polymer-based, paclitaxel-eluting stent (PES), which was also shown to consistently reduce restenosis and the need for repeat revascularization procedures compared with BMS.
BMS were introduced to overcome the limitations of balloon angioplasty by scaffolding the vessel wall and prevention of acute recoil. However, stent mediated arterial injury resulted in neointimal hyperplasia which was more pronounced following BMS implantation than balloon angioplasty alone. This limitation was addressed with the introduction of DES with release of anti-proliferative agents and potent suppression of neointimal hyperplasia. Since both shortcomings, acute recoil and neointimal hyperplasia, are relatively short-lived phenomena, coronary artery stents do not exert any long-term benefit, but may rather be the source of late adverse events including very late ST and elimination of physiological vasomotion. Moreover, coronary artery stents impede subsequent surgical revascularization and impair non-invasive imaging quality. Fully bioresorbable scaffolds have been developed with the aim of the overcoming these drawbacks. An important limitation in the past has been the polymer-mediated occurrence of severe local inflammation.
Figure 3 provides a summary of the structure and composition of drug-eluting bioresorbable vascular scaffolds with Conformité Européenne (CE) mark approval. The first scaffold to receive CE mark, was the biodegradable BVS introduced by Abbott (Santa Clara, CA, USA) consisting of a crystalline poly-L-lactide backbone on top of which everolimus was applied. Unfortunately despite promising early data from first-in-man studies, and the demonstration of non-inferiority compared to conventional DES, contemporary data have not shown any of the anticipated benefits of the device, in particular regarding maintaining vasomotion and reduced ST. Whilst some of these results are due to scaffold design and some a direct consequence of sub-optimal implantation techniques, enough concerns have been raised for the manufacturer to limit use of the BVS to clinical trial work only. Numerous other scaffolds are also undergoing clinical trials including the CE-marked DESolve scaffold (Elixir Medical Corporation, CA, USA) which elutes a mixture of anti-inflammatory myolimus (or novolimus in the revised version) and poly-l-lactic acid, and the Magmaris scaffold (Biotronik, Bülach, Switzerland) which has a backbone made of magnesium and elutes sirolimus. A full discussion of biodegradable stent platforms is found in chapter Calcified coronary lesions.
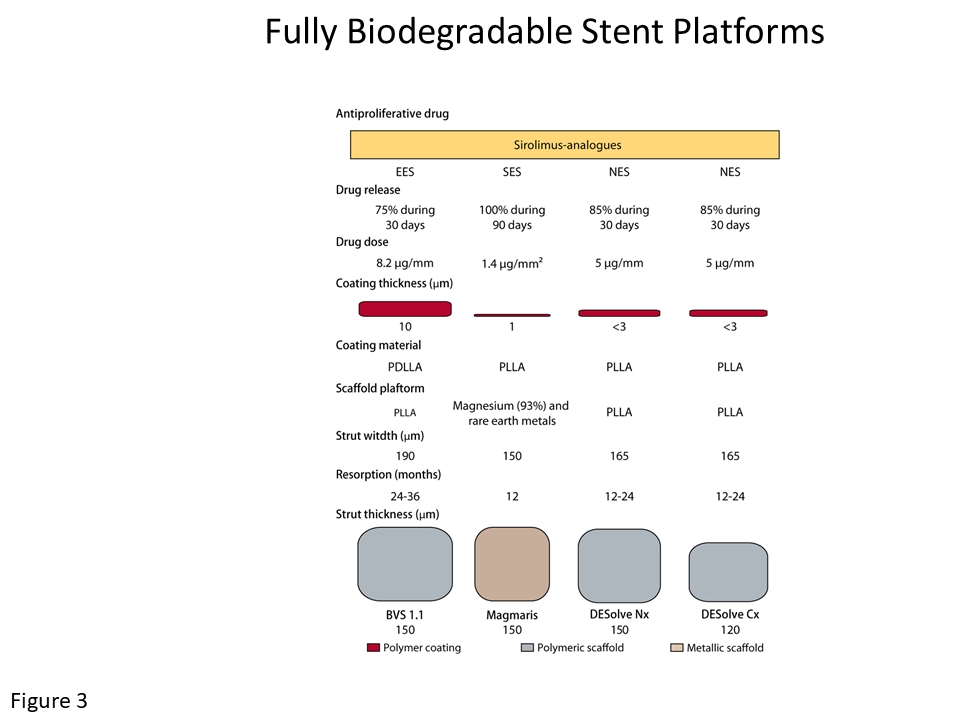
A summary of the structure and composition of the drug-eluting bioresorbable vascular scaffolds with CE mark approval. [Reproduced with permission from ].
The key prerequisites for coronary artery stent platforms are as follows:
Available stents vary in metallic composition, strut design and thickness, delivery system and coating. These different parameters play an important role in deliverability, visibility, scaffolding performance and procedural success. Some of the parameters can also influence the occurrence of adverse events during the hospital stay (peri-procedural myonecrosis, ST) and long-term follow-up (restenosis).
The importance of stent design on acute vascular injury and subsequent vasculo-proliferative response is well established. In animal models, changes in stent design lead to diverse degrees of vascular injury, thrombosis, and neointimal hyperplasia. Furthermore, stents which allow a circular rather than angular vessel lumen lessen neointimal proliferation. Figure 4 illustrates the impact of stent implantation on restenosis and ST. However, only few randomized trials addressed the role of stent design on clinical outcome. Compared with the Palmaz-Schatz stent, the Gianturco-Roubin II stent was found to be inferior for the prevention of restenosis. Several new generation BMS have been directly compared with the Palmaz-Schatz stent in non-complex lesions without showing differences in terms of ST, restenosis, or major adverse cardiac events (MACE). The arrival of newer generations of DESs with improved efficacy and safety and declining cost, has led to a significant fall in the use of BMS, a change supported by contemporary data. The NORSTENT study, which enrolled 9013 patients and is the largest single randomised study comparing outcomes between patients receiving BMS or contemporary DES, reported no significant between-stent differences in the primary composite outcome of all-cause death and non-fatal MI (BMS 17.1% vs. DES 16.6%, p=0.66) at a median of 5 years follow up. Rate of repeat revascularisation (19.8% vs. 16.5%, p<0.001) and definite ST (1.2% vs. 0.8%, p=0.0498) were significantly lower with the use of DES.
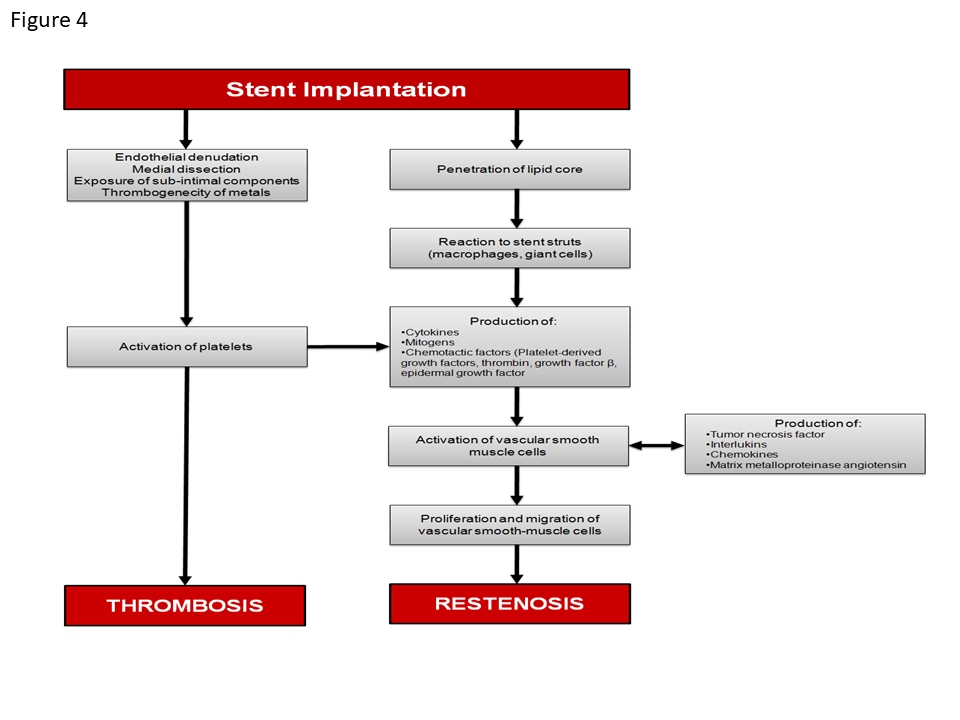
Pathway leading to in-stent restenosis and thrombus formation after stent implantation.
Stainless steel (316L) was, until recently, the most frequently used component of coronary stents due to its excellent processing characteristics, sufficient radial force and low elastic recoil (<5%). As stent material, stainless steel has limitations, including limited radio-opacity, reduced flexibility and a relatively high nickel content which has been linked to an increased risk of restenosis due to allergic reactions. Cobalt chrome (L605 CoCr) alloy has become a more recent alternative and constitutes the most frequently stent material today. L605 CoCr is stronger, more radio-opaque and contains less nickel than 316L stainless steel. Consequently stents manufactured from L605 CoCr have greater radiographic visibility, and thinner struts (with no compromise to radial strength) thereby providing improved deliverability compared with 316L stainless-steel stents. Historical data from stainless steel stents suggest that a reduction in strut thickness may be associated with lower rates of restenosis and repeat revascularization, However, assessment of neointimal hyperplasia by late lumen loss reveals no superiority of CoCr stents. Experimental data suggests that strut thickness is positively correlated with the propensity for thrombus formation and may therefore impact on the risk of ST.
More recently, platinum alloys were introduced, offering several distinct advantages over conventional stent materials. Platinum is two times denser than iron or cobalt, malleable, corrosion resistant, fracture resistant and fully incorporated into the platinum chromium (PtCr) alloy. Consequently, the PtCr stent offers the advantage of increased radio-opacity and thinner stent struts. Importantly, initial benchmark studies indicated that, despite these thinner struts, the PtCr alloy stent had better radial strength, lower acute recoil and better vessel conformability compared to conventional stent platforms. Moreover, the nickel content is reduced when compared with 316L stainless steel thus reducing the risk of allergic reactions. This alloy is however only present in a few available platforms.
The basic characteristics of balloon-expandable (BE) stents are summarized in Figure 5: coil vs. slotted tube designs, closed vs. open cells, number of struts, strut thickness and strut morphology. Currently, most stents have a slotted tube design, which can be further categorized into closed-cell and open-cell design. The main difference between closed versus open-cell design is that in stents with a closed-cell design all deflections between two contiguous hoops are connected, whereas in an open-cell design some of the internal deflection points of the hoops are not connected by bridges or welds. As a result, a closed-cell design provides better coverage of the luminal surface and conveys greater radial strength. Cell size is minimally affected when a closed-cell stent is deployed in a tortuous site. However, it is less flexible and may be more difficult to deliver in tortuous and calcified vessels. In addition, side-branch access may be more challenging. The open-cell design allows for a greater flexibility of the stent and easier access to side branches. Possible drawbacks are a weaker radial strength, changes in cell size in tortuous anatomy, less coverage of the vessel wall particularly on the outer curvature of vessels. In order to further improve flexibility, the number of crowns has been increased accompanied by a decrease in strut length and thickness. Finally, the geometry of the cross-section of the strut has been improved and most of the struts are rounded in order to limit edge dissections and perforation.
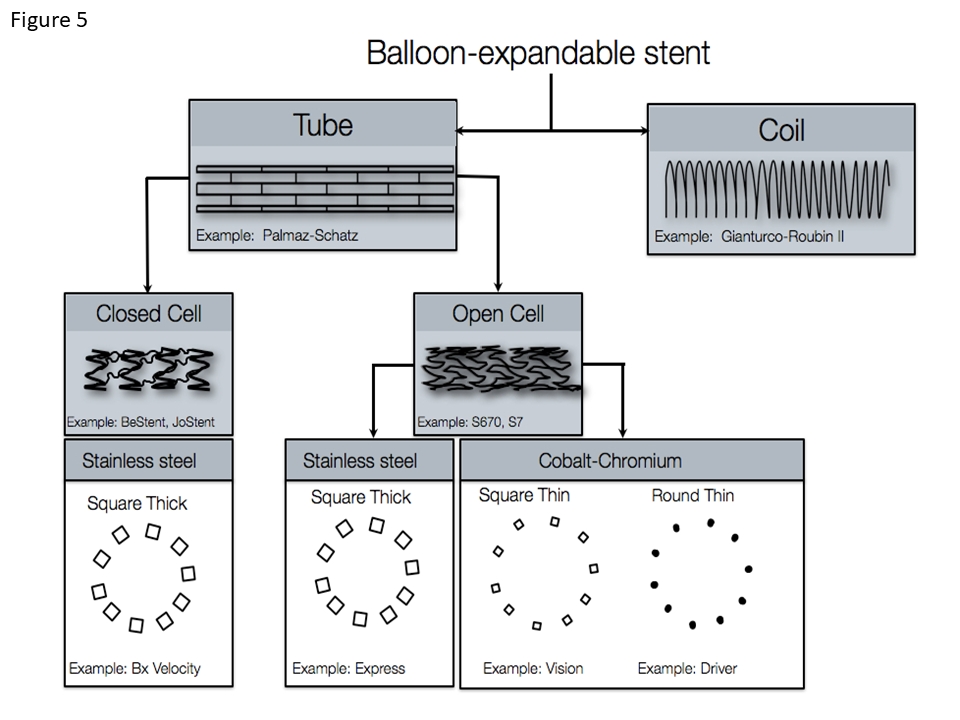
Design characteristics of balloon-expandable coronary stents.
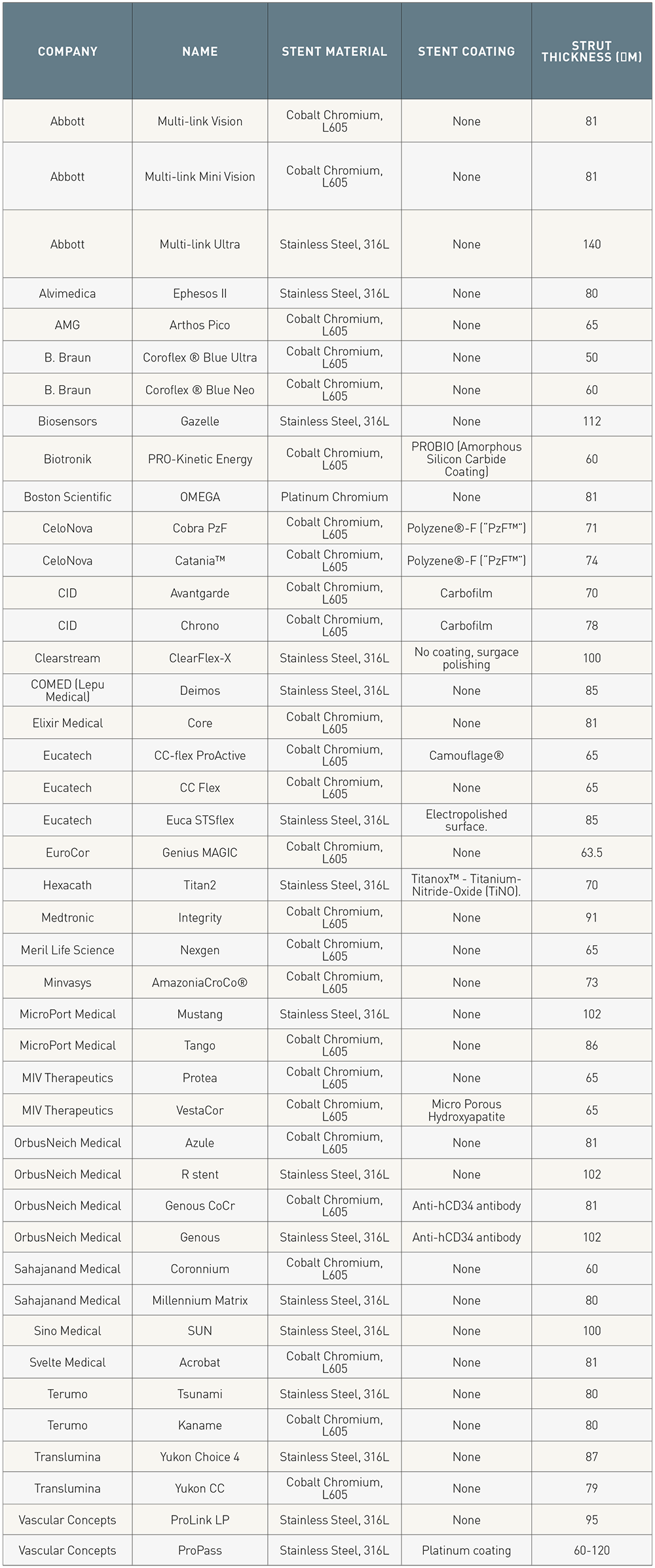
Nowadays, corrugated open-cell and hybrid designs dominate the market (Table 1). Technological refinements pursue the ideal balance between deliverability, strength and biocompatibility. Advances include sophisticated connectors between crowns such as J-links, quadrature-links or double-helical designs; improved coatings with the aim to increase biocompatibility and reduce platelet aggregation such as Probio® (Biotronik) and Carbofilm™ (CID Vascular); and the introduction of endothelial progenitor cells capture technology to accelerate the natural healing process (Genous, OrbusNeich, USA), among others.
Apart from the delivery system and the platform - which are basically the same as for BMS - DES contain two specific parts: the polymer coating and the drug. The components of a DES are summarized in Figure 6. In relation to drug elution, the geometric configuration of the platform is critical to accommodate the required dose of the agent on the drug-carrying units (the struts or reservoirs) and to allow adequate diffusion to ensure optimal drug tissue levels. Stent-strut based drug delivery has been shown to be highly spacing-dependent. Accordingly, an increased strut number has been associated with higher mean arterial wall drug concentrations and inhomogeneous strut placement has been shown to significantly affect local concentrations.
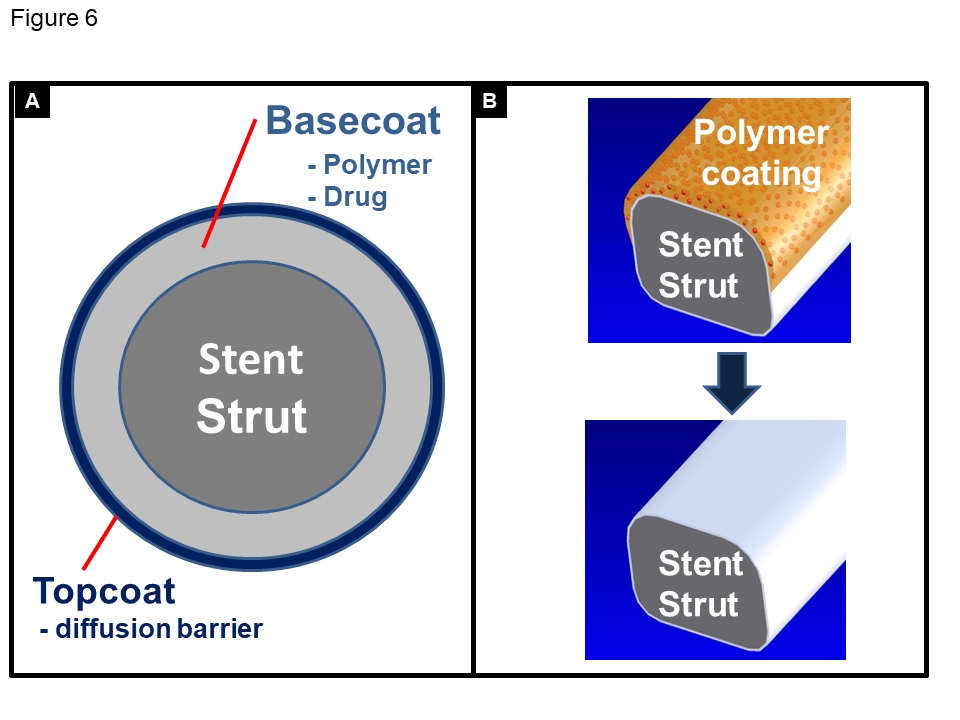
Schematic drawing of the components of a drug-eluting stent with durable polymer (A) and a drug-eluting stent with bioresorbable polymer limited to the abluminal side (B).
The drug aims to limit neointimal proliferation. An ideal profile should be characterized by:
The efficacy of candidate drugs is not only dependent on biological activity in vitro, but is also determined by local pharmacokinetics and physicochemical drug properties. Drug distribution is mediated by stent strut configuration and the balance between convective and diffusive forces. Hydrophilic drugs such as heparin readily permeate into tissue, but are also rapidly cleared. In contrast, lipophilic agents such as paclitaxel or limus analogues are water-insoluble and bind to hydrophobic sites in the arterial wall. Although both hydrophilic and lipophilic drugs show large spatial concentration gradients in the arterial wall, the latter distribute better and more homogenously into the arterial wall than the former. To date, immunosuppressive (limus family) and anti-proliferative (paclitaxel) drugs are used. More recently, asymmetric application of anti-proliferative agents (sirolimus) by means of abluminal stent coating in conjunction with anti-CD34 antibody surface modification has been shown to result in potent suppression of neoinitimal hyperplasia while promoting re-endothelialization more effectively than circumferential stent strut coatings.
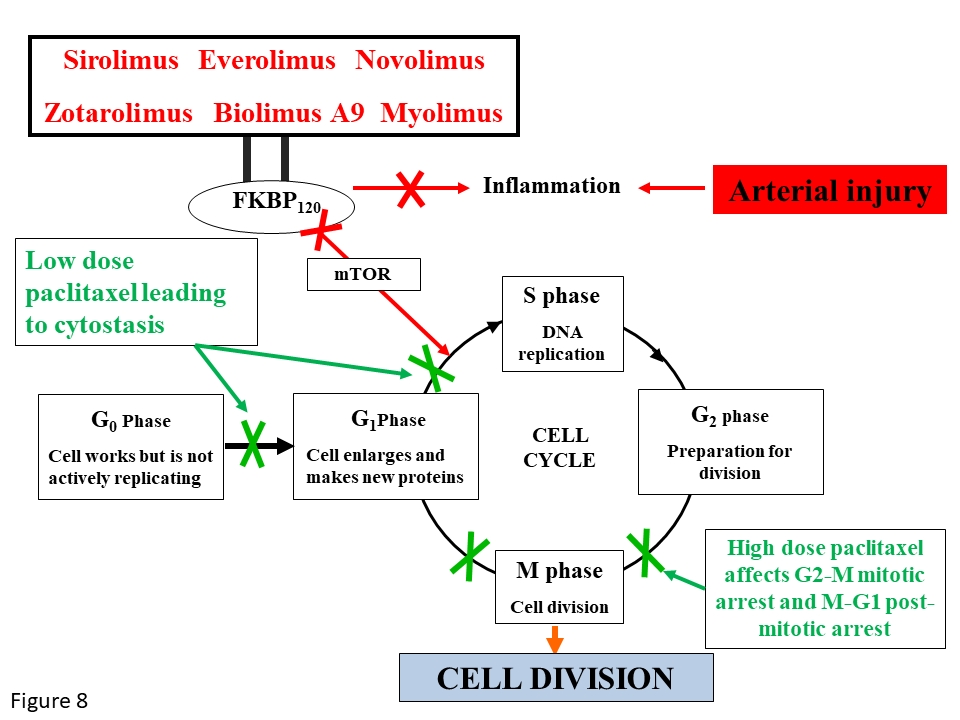
Most of the currently available DES use drugs that are analogues of sirolimus (limus family). The principal therapeutic agents of the limus family encompass: sirolimus, zotarolimus, everolimus, biolimus-A9, novolimus, myolimus, ridaforolimus. (Figure 7). These agents bind to the intracellular receptor FKBP-12 and inhibit a phosphoinositide 3-kinase termed mammalian target of rapamycin (mTOR), thereby reversibly inhibiting the growth factor- and cytokine-stimulated cell proliferation in the G1 phase of the cell cycle (Figure 8). Vascular smooth muscle cells are usually quiescent, proliferate at low indices (<0.05%), and remain in the G0 phase of the cell cycle. However, stimulated by vascular injury or growth factors, vascular smooth muscle cells re-enter the cell cycle at G1 and advance into the S phase. Tacrolimus and pimecrolimus also belong to the limus family but have immunosuppressive rather than anti-proliferative activity. Both drugs bind to FKBP-506 rather than FKBP-12. The tacrolimus/pimecrolimus FKBP506 complex subsequently inhibits the calcineurin receptor, which leads to decreased cytokine expression on the cell surface membrane and results in an inhibition of T-cell activation and lower smooth muscle cell selectivity.
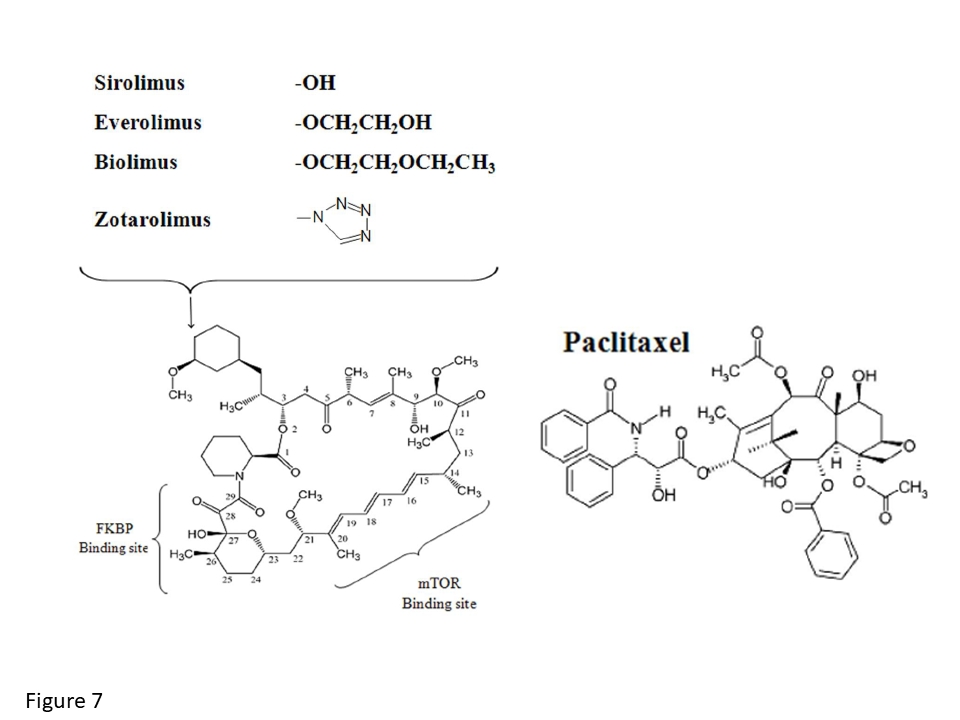
The chemical structure of the macrocyclic lactone group of antiproliferative drugs of the limus family as compared to the chemical structure of paclitaxel.
Mechanism of action of antiproliferative drugs of the limus family and of paclitaxel.
Sirolimus
Sirolimus (C51H79NO13, molecular weight 914 Da), a highly lipophilic drug, was the first member of the limus family to be used for prevention of restenosis following PCI. Following experimental studies showing potent suppression of vascular smooth muscle cell proliferation, local delivery of sirolimus from stents also effectively inhibited neointimal proliferation. The kinetics of drug release from the Cypher® SES (Cordis, Warren, NJ) have been investigated in vivo and indicate that tissue levels are maximal at 14 days and remain substantial up to 28 days.
Everolimus
Everolimus (C53H83NO14, molecular weight 958 Da) is a sirolimus derivative, in which the hydroxyl group at position C40 of sirolimus has been alkylated with a 2-hydroxy-ethyl group. It is slightly more lipophilic than sirolimus, and therefore it is more rapidly absorbed into the arterial wall. Although binding of everolimus to the FKBP-12 domain is 3-fold and immunosuppressive activity in vitro 2 to 5-fold lower than with sirolimus, oral everolimus proved at least as potent as sirolimus in models of autoimmune disease and heart transplantation. In addition, the everolimus-eluting stent (EES) platform is potentially associated with less inflammation than sirolimus- or paclitaxel-eluting stents.
Zotarolimus
Zotarolimus (C52H79N5O12, molecular weight 966 Da) is another sirolimus analogue, in which the C40 position is modified by a tetrazole ring resulting in a shorter circulating half-life of the drug. It is an equipotent analogue of sirolimus in vitro and in vivo. Although the binding affinity to the FKBP 12 domain for zotarolimus and sirolimus is similar and the antiproliferative activities of zotarolimus are also comparable to those of sirolimus, the immunosuppressive activity in vivo is 3 to 4-fold lower. Two stents eluting zotarolimus have been introduced. Both are based on the Driver® stent platform (Medtronic, Inc., Minneapolis, MN) with a strut thickness of 91 µm made of cobalt chromium alloy, and have coatings with both hydrophilic and hydrophobic moieties. On the FDA-approved zotarolimus-eluting Endeavor® stent (E-ZES) zotarolimus is absorbed into a 5 µm-thick phosphorylcholine layer with a concentration of approximately 1.6 µg/mm2 stent surface area. In contrast to the sirolimus-eluting Cypher® stent, which elutes approximately 80% of its drug during the first 30 days, the E-ZES stent releases the same proportion of zotarolimus within only 10 days. The Endeavor Resolute® ZES (R-ZES) uses the BioLinxä polymer system for release of zotarolimus from the Driver® stent platform. BioLinxä consists of three polymers, a hydrophilic C19 polymer, water soluble polyvinyl pyrrolidinone (PVP) and a hydrophobic C10 polymer and allows for a more delayed release of the same zotarolimus concentration as on the original E-ZES, (1.6 µg/mm2 stent surface area) however approximately 50% of drug is released during the first 7 days, and 85% 60 days after stent implantation.
Biolimus A9
Biolimus-A9 is a highly lipophilic, semi-synthetic sirolimus analogue with an alkoxy-alkyl group replacing hydrogen at position 42-O. The drug is immersed at a concentration of 15.6 mg/cm2 into a biodegradable, polylactic acid (PLA) polymer, which is applied solely to the abluminal surface of a stainless steel stent. Based on in vivo studies, PLA is fully converted to lactic acid at 6 months and the polymer is resorbed within 9 months. Biolimus-A9 eluted from PLA has been used as therapeutic agent on several stent platforms:
Novolimus
Novolimus is a macrocyclic lactone, which has been developed by removal of a methyl-group from carbon C16. Notably this differs from the other macrocyclic lactone agents that are used in DES, which have mainly been developed through modifications on the carbon C40 of the macrocyclic ring. Nevertheless in a similar fashion to these other agents, novolimus inhibits mTOR. In vitro studies demonstrate it to have a potency to inhibit human smooth muscle cells (IC50 of 0.5nM) comparable to that of sirolimus. Novolimus is used on two CoCr based stents, which both have a strut thickness of 81 microns, a drug load of 85 micrograms, and a maximum polymer thickness of 3 microns. The difference between the two stents relate to the polymer; whilst the Elixir DESyne™ (Elixir Medical, Sunnyvale, CA, USA) has a durable poly n-butyl methacrylate polymer, which is similar to that found on the Cypher® SES, the Elixir DESyne™ BD (Elixir Medical, Sunnyvale, CA, USA) has a PLA biodegradable polymer. The polymer facilitates controlled release of novolimus, such that 80% of the drug is released over 12 weeks, with elution complete by 6-months (data on file at Elixir medical).
Myolimus
Ridaforolimus, an analog of sirolimus and a small molecule inhibitor of mTOR, has a high therapeutic index is eluted from BioNir stent (Medinol, Tel Aviv, Israel). The 80mm CoCr struts have a uniform dose of ridaforolimus, which is eluted using a durable elastomeric polymeric coating that remains intact post elution.
Paclitaxel stabilizes polymerized microtubules and enhances microtubule assembly, forming numerous unorganized and decentralized microtubules inside the cytoplasm. As a result, cell replication is inhibited and this effect is seen predominantly in the G0/G1 and G2/M phases of the cell cycle (Figure 7). Paclitaxel was shown to effectively inhibit vascular smooth muscle cell migration and proliferation. In addition, it has several favourable characteristics for stent-based local drug-delivery, such as a high degree of lipophilicity and a long-lasting anti-proliferative effect following a single-dose application at low concentrations. In a porcine restenosis model, implantation of stents dip-coated with paclitaxel at increasing doses resulted in a dose-dependent inhibition of neointimal formation at 28 days. However, the beneficial effects of paclitaxel on neointimal formation were associated with local cytotoxic effects that manifested as a decrease in medial wall thickness, focal neointimal and medial wall hemorrhage, and cell necrosis.
The most commonly used devices for stent-based paclitaxel delivery were the TAXUS® Express2® stent (Boston Scientific, Natick, Mass, USA) and TAXUS Liberté™, both made of stainless steel and manufactured with the same polymer and dose of paclitaxel. However, the Liberté™ stent uses a more uniform cell geometry - allowing enhanced and uniform drug delivery, thinner struts (97 µm vs. 132 µm), a smaller profile, and separate stent designs depending on stent diameter. Paclitaxel has lost its role in newer generation DES but is commonly used as the anti-proliferative agent released from drug-coated balloons.
Stent coatings consist of one or several layers (Table 2): The most important layer is the polymer, which accommodates the drug and allows drug elution into the vessel wall by contact transfer. Supplemental layers are found in most drug-eluting stents and consist of either top coatings to delay drug release (for example PBMA) or base coatings to increase polymer adhesion to the stent struts (for example Parylene C). While in the early development durable (non-biodegradable) polymers dominated, new generation stents preferentially use biodegradable polymer carriers. Coatings are typically spray coated or dip coated, and some stent manufacturers use sophisticated auto-pipetting procedures to ensure highly reproducible coatings.
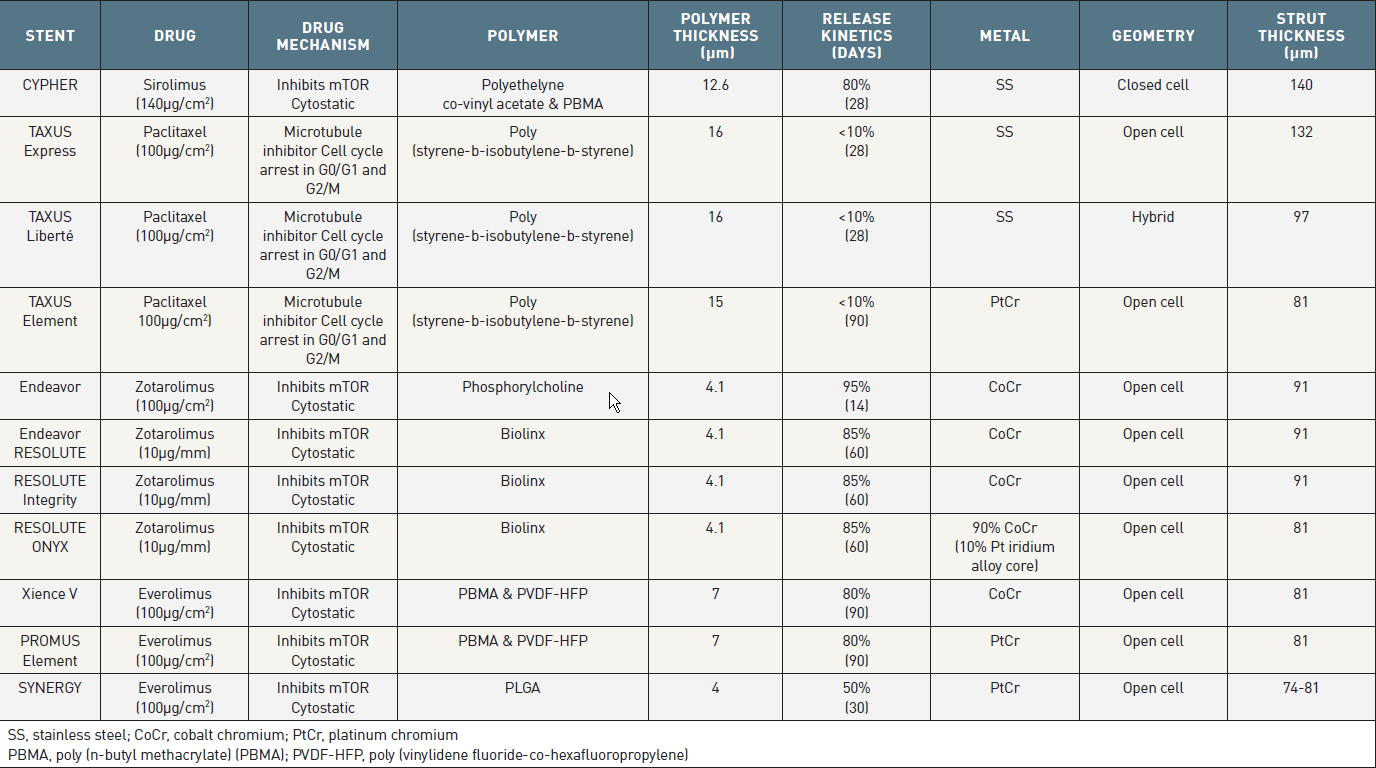
Specificications of the FDA Approved DES
Polymers have been pivotal for the development of local drug delivery and in particular of DES. Polymeric materials act as drug reservoir and allow for controlled drug release over time. The drug may be dissolved either in a reservoir surrounded by a polymer film or within a polymeric matrix. Controlled drug release can occur by diffusion, chemical reaction, or solvent activation. Biodegradable polymers allow drug release by both passive diffusion and matrix degradation, whereas non-degradable polymers enable drug release by particle dissolution. Early efforts to identify suitable polymers for stent coating were characterized by exuberant inflammatory and thrombotic responses resulting in excessive neointimal hyperplasia and vessel occlusion. These adverse effects have been attributed in part to inappropriate polymer degradation and molecular weight of the compounds as well as solvents and catalyst by-products. More recently, a wide variety of biocompatible polymers, some of them triggering no or minimal inflammatory response, have been developed as carriers for DESs. Furthermore, some stents have only an abluminal polymer coating (asymmetric coating) (Figure 6). In the investigation of new drugs for local delivery it is therefore mandatory to address not only the drug itself, but also the biocompatibility of the polymeric carrier.
Another solution for drug release is modification of stent designs providing laser cut reservoirs within stent struts, the so-called reservoir technology (RES). Each strut may contain several reservoirs, which can be located abluminally or luminally, or feature an entire hole (Figure 9). This concept theoretically reduces the polymer tissue contact surface while maintaining controlled drug release and provides flexible drug delivery of one or more drugs into a single, dual or bidirectional release. The reservoir technology was first utilized with the CoStar™ stent platform (Conor MedSystems, Menlo Park, CA, USA) and established the pharmacokinetic profile of paclitaxel release from a biodegradable polymer. Inferior outcomes as compared with the durable polymer based TAXUS® (Boston Scientific, Natick, MA, USA) stent in the CoStar II trial were related to a more delayed release pattern of paclitaxel beyond the period of maximal smooth muscle cell proliferation. The reservoir technology was then used on NEVO™ stent (Cordis, Warren, NJ, USA) which had a CoCr platform and released sirolimus from a biodegradable PLGA polymer. Unfortunately, despite promising initial results, further evaluations of this stent were stopped prematurely due to stent dislodgement problems.
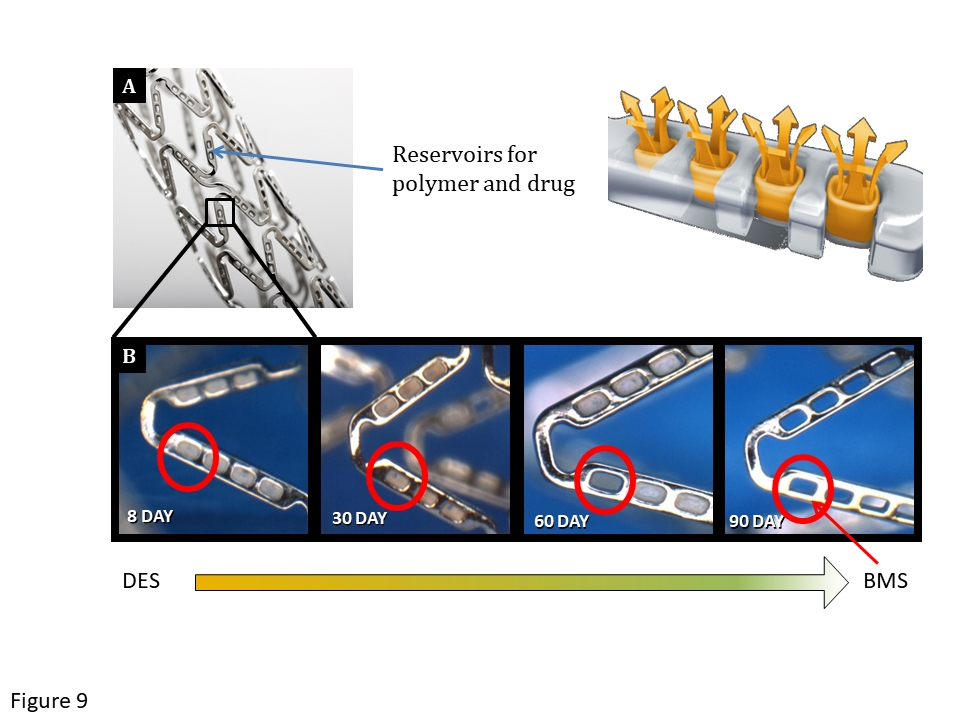
The NEVO™ cobalt chromium stent, which has an open-cell design and reservoirs which contain a biodegradable polymer and sirolimus. After 90 days, the reservoirs are depleted as the polymer has undergone complete biodegradation.
Attempts to eliminate the polymer as a potential source of adverse events have led to the development of polymer-free drug carrier systems (Figure 10). Non-polymeric stents offer the potential advantages of avoiding the long-term adverse effects of a polymer, thereby improving healing and maintaining the integrity of the stent’s surface owing to the absence of a polymer cracking, webbing and peeling off. Several different techniques are available to enable drug elution from stents in the absence of a polymer:
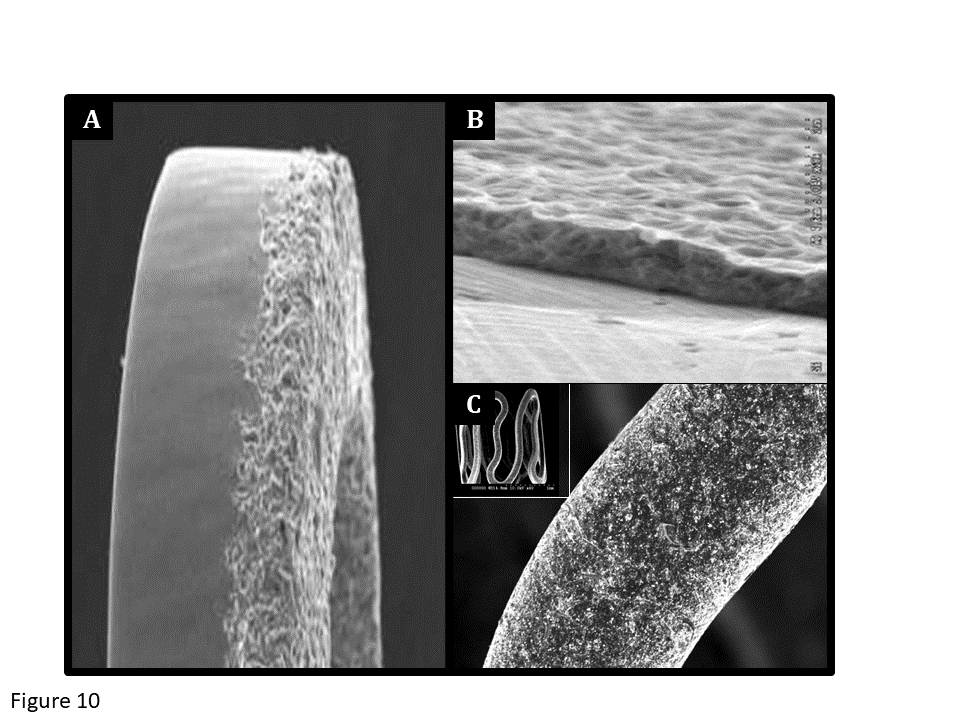
Scanning electron microscopy of the surface of three different polymer-free stents. The BioFreedom™ stent (A) is a polymer-free biolimus-eluting stent made of stainless steel and a micro-structured, polymer-free surface alteration at the abluminal stent side. The VESTAsync™ stent (B) has a nano-thin, microporous, hydroxyapatite surface coating impregnated with sirolimus. The Yukon stent (C) has a microporous surface, with pores which are 2 μm deep and impregnated with sirolimus.
Mainly the first approach has been evaluated in clinical investigations and will be discussed later in this text
The first SES was the Cypher stent, developed by Cordis Corporation, Warren, NJ. It consisted of sirolimus in a concentration of 140 µg/cm2, incorporated in an amalgam of two biostable polymers, with the polymer/drug matrix then applied onto the tubular 316L stainless steel BX Velocity stent (Table 3).,
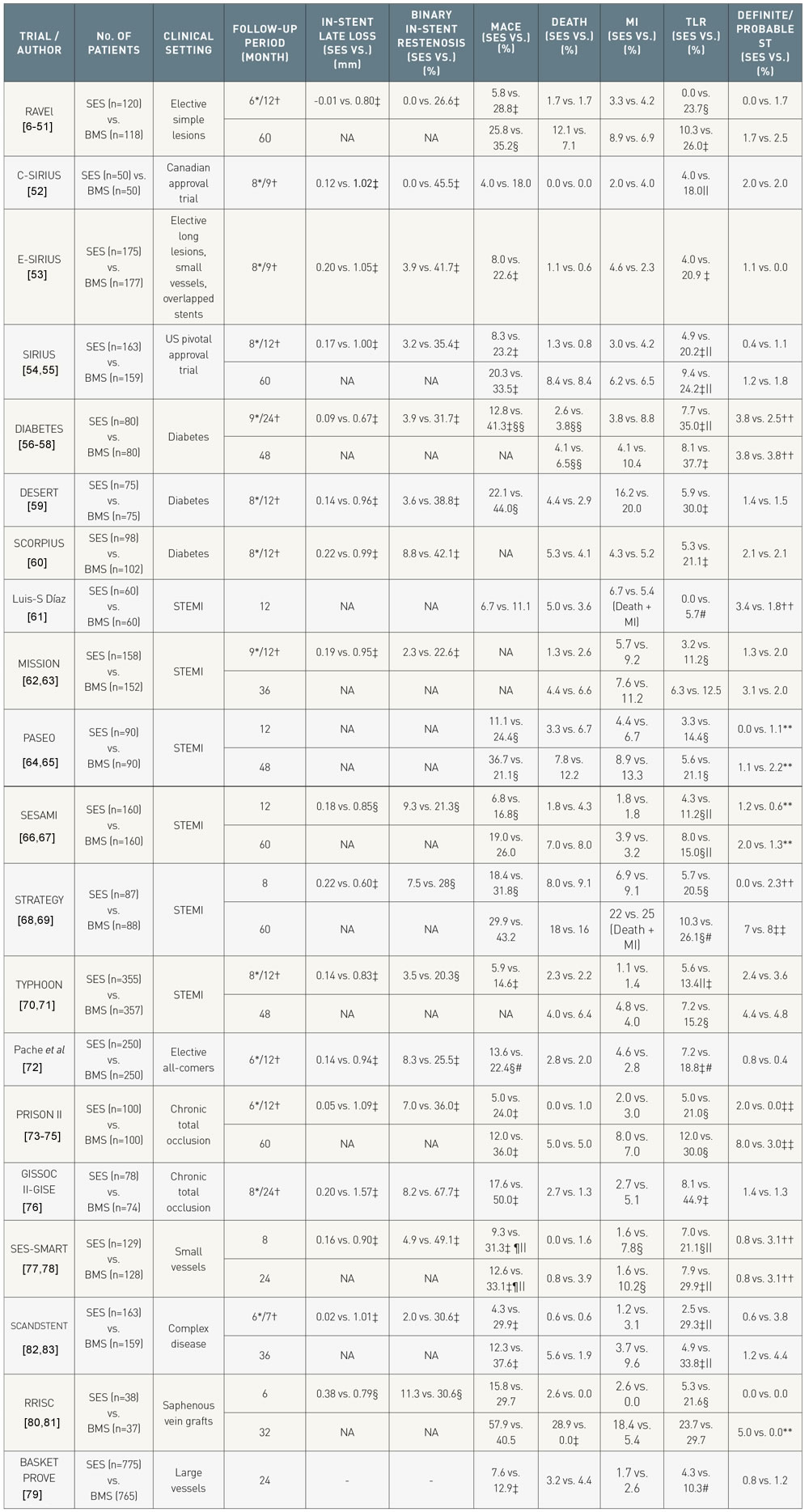
Summary of major randomized trials of the sirolimus eluting stent versus bare metal stents in different clinical settings.
Differences are non-significant unless indicated. Stent thrombosis defined per ARC definitions, unless indicated.
*Angiographic follow-up
†Clinical follow-up
‡ P<0.001
§ P<0.05
¦Ischemia driven
¶ Major Adverse Cardiovascular and Cerebrovascular events
# Target vessel revascularization
** Definite ST only
†† Protocol defined ST
‡‡ Definite, probable and possible
§§ Cardiac
STEMI, ST-elevation MI; ST, stent thrombosis; MACE, major adverse cardiovascular events (a composite of death, MI and target lesion revascularization); BMS, bare metal stent; SES, sirolimus-eluting stent; NA, not available;
Both fast release stents with drug release in < 15 days and slow release stents with ≥ 28 day drug release were developed and tested in the FIM study in 1999 in Sao Paulo, Brazil and Rotterdam, the Netherlands. Angiographic and IVUS results from the 45 patients who were studied showed remarkable suppression of in-stent neointimal hyperplasia, which continued out to 4 years of follow-up.
The pivotal RAVEL study (RAndomised study with the sirolimus-eluting VElocity balloon-expandable stent in the treatment of patients with de novo native coronary artery Lesions) evaluated the Cypher SES by randomizing 238 patients with relatively low risk lesions to treatment with SES or BMS. At 1-year follow-up the rate of binary stenosis was 0.0% and 26.6% for patients treated with Cypher SES and BMS, respectively. These results were subsequently confirmed in the larger SIRIUS trial (SIRolImUS-coated Bx Velocity balloon-expandable stent in the treatment of patients with de novo coronary artery lesions) that enrolled 1058 patients with more complex lesions than were seen in RAVEL. Significantly lower rates of target lesion revascularization (TLR) and MACE following treatment with the Cypher SES were demonstrated when compared to BMS controls at 9-months, 2-years and 5-year follow-up. The Cypher stent was thus the first DES to receive CE-mark in April 2002 and was subsequently approved by the FDA in 2003. A meta-analysis of data from four double-blind studies with 1,784 patients found that TLR was reduced from 23.6% with BMS to 7.8% with SES (hazard ratio [HR] 0.29, 95% CI 0.22-0.39, p < 0.001) at four years (Table 4). Although rates of death or MI were similar for both BMS and SES, the latter showed a somewhat higher propensity for late ST (5 vs. 0 events) between 1 and 4 years; efficacy remained superior with SES out to 5 years (TLR: SES 15% vs 30.1%; p < 0.0001).
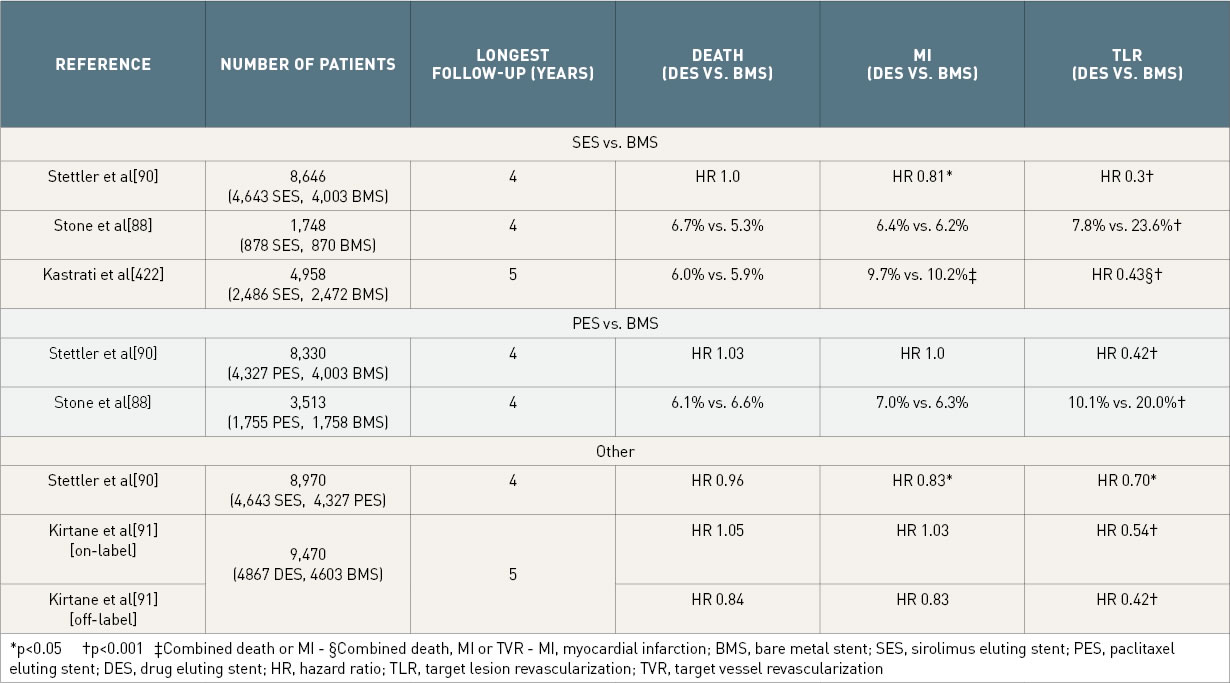
Rates of death, myocardial infarction and target lesion revascularization from recent meta-analyses of drug eluting stents compared to bare metal stents. Differences non-significant unless indicated.
*p<0.05 †p<0.001
‡Combined death or MI
§Combined death, MI or TVR
MI, myocardial infarction; BMS, bare metal stent; SES, sirolimus eluting stent; PES, paclitaxel eluting stent; DES, drug eluting stent; HR, hazard ratio; TLR, target lesion revascularization; TVR, target vessel revascularization
Performance of the Cypher SES has been assessed in ‘off label’ settings and specific subgroups of patients such as diabetics, and those presenting with AMI, In addition it has been assessed in patients with different lesion types including chronic total occlusions, SVGs, lesions in small coronary vessels, and complex lesions. Irrespective of clinical situation, when compared with BMS, the use of SES results in significant reductions in angiographic in-stent late loss, in-stent angiographic stenosis, and repeat revascularization at both short and long-term 5-year follow-up, with results consistent across numerous different patient and lesion types (Table 3 and Figure 11).
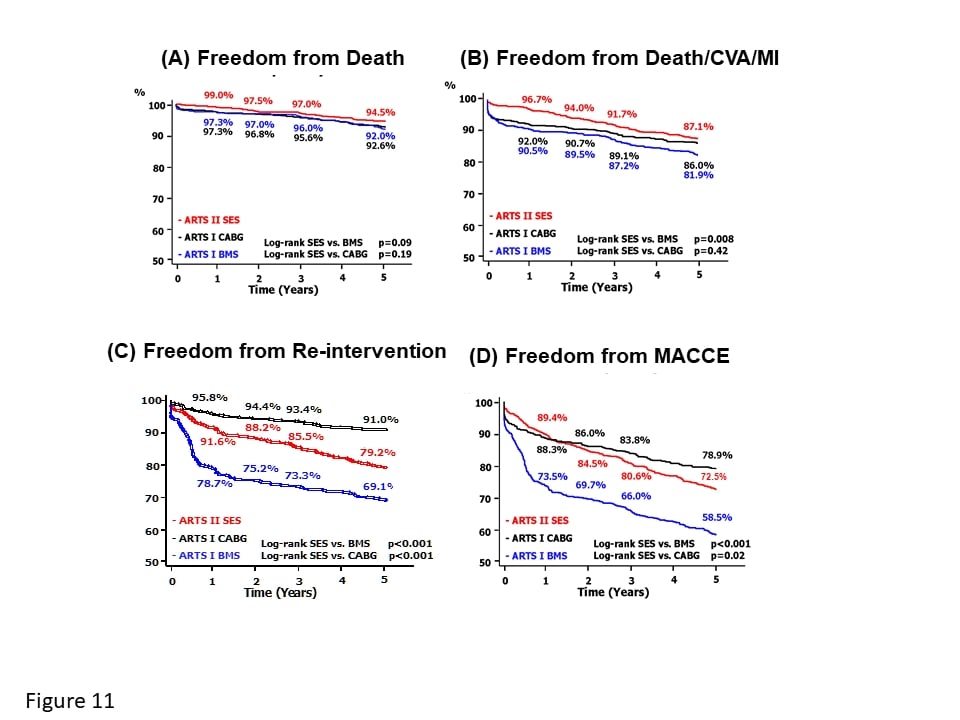
Long-term clincal outcomes of patients treated with SES (in red), BMS (in blue), and CABG (in black) in the ARTS (Arterial Revascularisation Therapy Studies) I and II Kaplan-Meier estimates for freedom from (A) death, (B) death, cerebrovascular accident (CVA) and myocardial infarction (MI), (C) repeat revascularisation, and (D) overall major adverse cardiovascular and cerebrovascular events (MACCE). [Reproduced with permission from ].
Despite the wealth of data confirming the efficacy of the Cypher stent, the manufacturer ceased production at the end of 2011.
The first TAXUS PES (Boston Scientific, Natick, MA) consisted of paclitaxel contained within a polyolefin derivative biostable polymer coated on the stainless steel NIR platform. A slow release (SR) formulation with an 18 µm thick coat, a moderate release (MR) with a 7 µm coat and a fast release with 4 µm coat shed 8%, 22% and 50% of the paclitaxel within 30 days respectively (Table 2). The difference in release was achieved by changing the polymer to drug ratio while maintaining the same paclitaxel concentration (1µg/mm2). The TAXUS PES has been evaluated in the TAXUS series of trials which have enrolled different patient and lesion types (Table 5): , ,
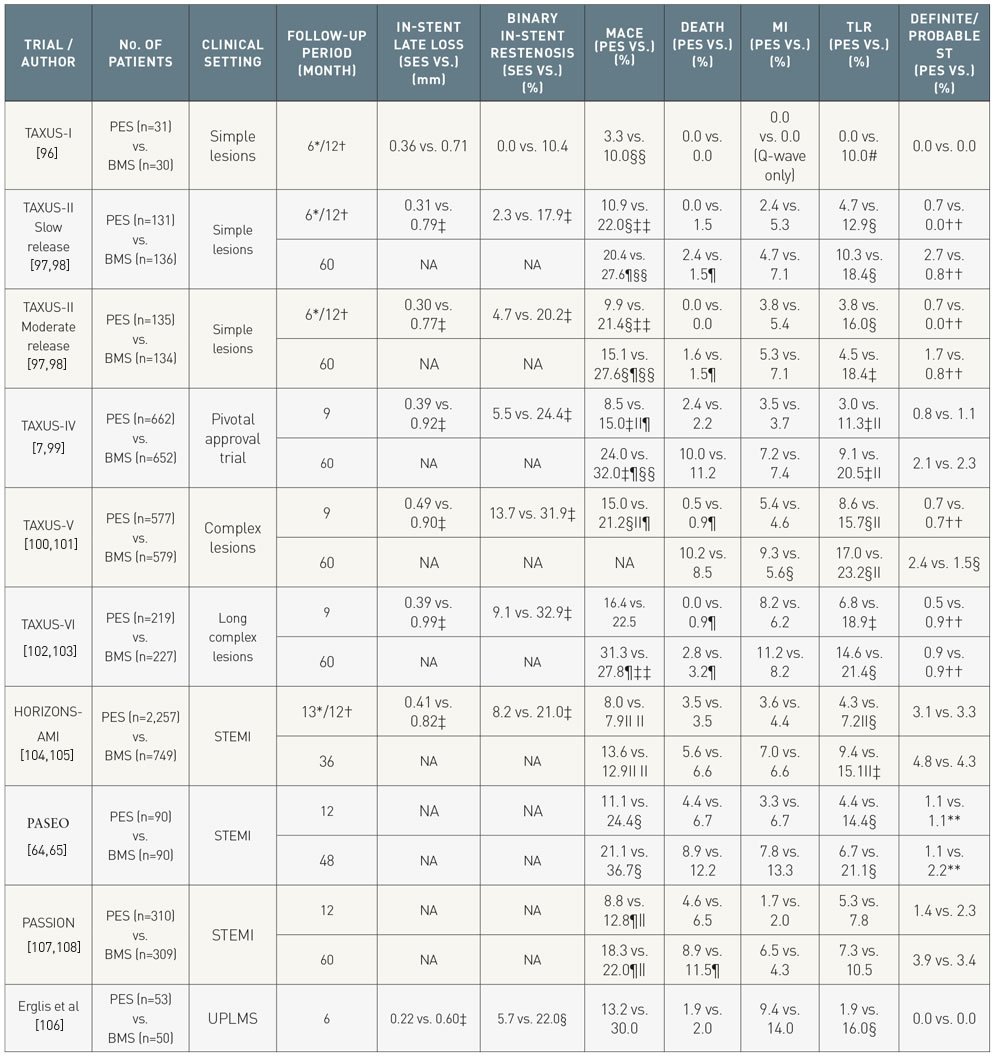
Summary of major randomized trials of paclitaxel eluting stent versus bare metal stents in different clinical settings. Differences are non-significant unless stated.
Stent thrombosis as per ARC definition, unless indicated.
*Angiographic follow-up
†Clinical follow-up
‡ P<0.001
§ P<0.05
¦Ischemia driven
¶ Cardiac death
#Percutaneous revascularization only
**Definite ST only
††Protocol defined ST
‡‡ Major adverse cardiovascular events a composite of death, MI and target vessel revascularization
§§ Major adverse cardiovascular events a composite of death, MI, target vessel revascularization and stent thrombosis
¦¦Major adverse cardiovascular events a composite of death, MI, stroke and stent thrombosis
UPLMS, unprotected left main stem; STEMI, ST-elevation MI; ST, stent thrombosis; MACE, major adverse cardiovascular events (a composite of death, MI and target lesion revascularization) BMS, bare metal stent; PES, paclitaxel-eluting stent; NA, not available; TVR, target vessel revascularization
Patient level meta-analysis of the initial PES approval trials have confirmed the comparable safety and superior efficacy of PES, compared to BMS out to 4-year follow-up (Table 4). A meta-analysis of five double-blind trials in 3,513 patients also revealed that TLR decreased from 20.0% with BMS to 10.1% with PES at 4 years (HR 0.46, 95% CI 0.38-0.55, p < 0.001). Rates of death and MI were balanced among patients treated with PES and BMS at 4 years of follow up. The incidence of ST was low owing to the non-complex underlying disease and not different between PES and BMS at one year. Between 1 and 4 years, however, there was an increase in those treated with PES (0.7% vs. 0.2%, 95% CI 0.98-21.03). TAXUS II is the first trial reporting 5-year outcome data comparing PES with BMS in patients with non-complex coronary artery disease. In this analysis, both slow- and moderate-release polymer based PES were more effective than BMS to reduce TLR (PES-MR: 4.5%; PES-SR: 10.3%, BMS: 18.4%, p < 0.001).
A third iteration of the TAXUS stent is the TAXUS Element stent (Ion, Boston Scientific, Natick, MA) which has a PtCr platform coated with a poly(styrene-b-isobutylene-b-styrene) polymer, which facilitates controlled elution of paclitaxel (concentration 1µg/mm2) in an identical pattern to that seen on the stainless steel TAXUS Liberté and Express stent (Table 2). The device was evaluated in the PERSEUS (A Prospective Evaluation in a Randomised Trial of the Safety and Efficacy of the use of the TAXUS Element Paclitaxel Eluting Coronary Stent System for the Treatment of De Novo Coronary Artery Lesions) clinical trial program, which includes:
Several randomized studies, which are summarized in Table 6 have directly compared outcomes between patients treated with SES or PES in: (I) unselected patients populations; (II) specific patient groups such as diabetics or those with STEMI; and (III) specific lesion types such as unprotected left main stem lesions, long lesions or lesions in small vessels. Results at short-term angiographic follow-up consistently demonstrate superior reductions in late loss with the use of SES, however long-term angiographic follow-up, indicates a greater delayed late loss with SES, such that at 5-years there was no longer a significant difference in late loss between SES and PES. In terms of clinical outcomes, a meta-analysis of 16 randomized trials of SES versus PES, which included 8,695 patients and where possible patient level data, reported significant reductions in TLR (HR:0.74, 95% CI:0.63-0.87, p < 0.001) and ST (HR 0.66, 95% CI:0.46-0.94, p = 0.02) with SES, whilst no significant differences in death (HR 0.92, 95%: CI:0.74-1.13, p = 0.43), or MI (HR 0.84, 95% CI:0.69-1.03, p = 0.10) were noted at a median of 2-year follow-up. The SORT-OUT II and SIRTAX studies have both reported long-term outcomes and failed to show any between-stent differences in MACE, cardiac death, MI, clinically-indicated TLR and ST at 10-year follow-up, with attenuation of the differences in MACE noted beyond 1-year.
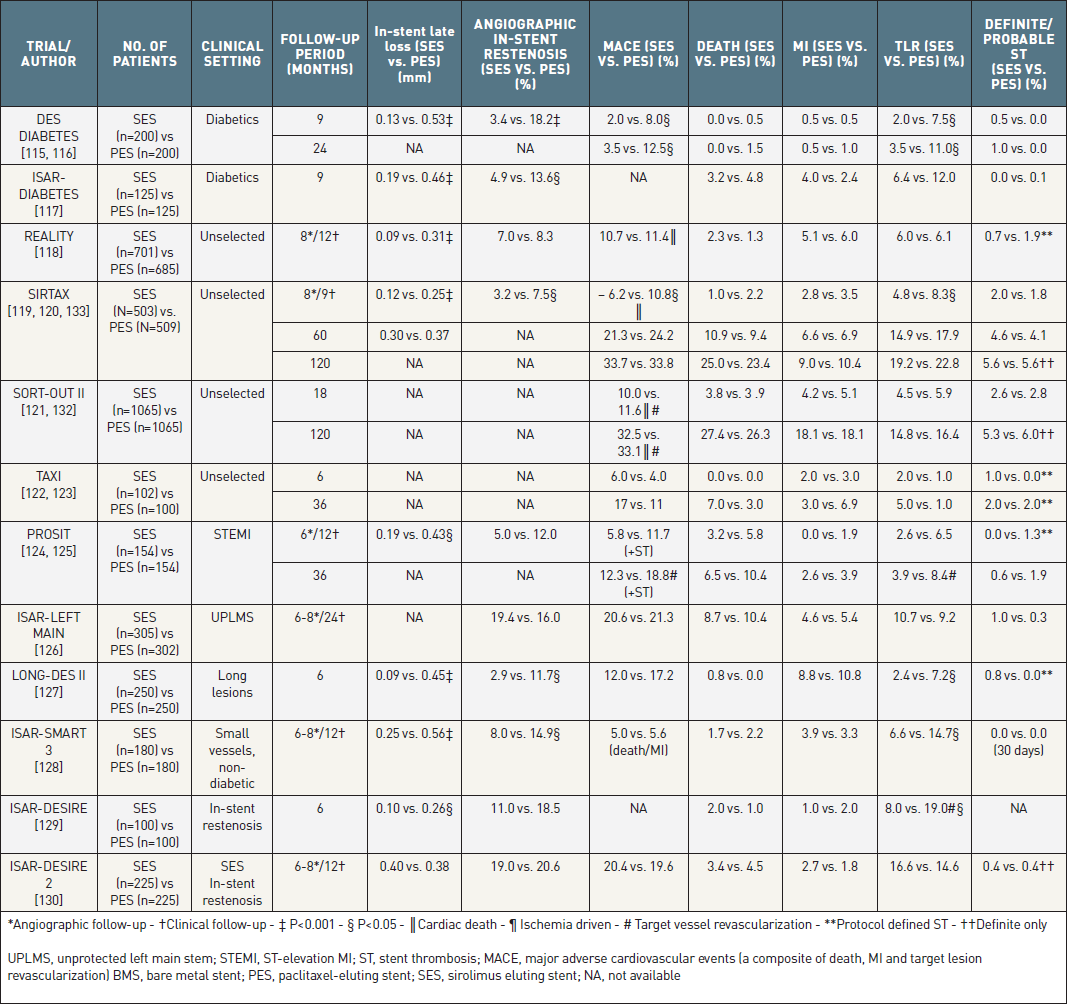
Summary of major randomized trials (>100 patients in each group) comparing the sirolimus-eluting stent to the paclitaxel eluting stents in different clinical settings. Differences are non-significant unless indicated. Stent thrombosis ARC definition unless indicated.
XIENCE V® (Abbott Vascular, Santa Clara, CA, USA), PROMUS™ (Boston Scientific, Natick, MA, USA)
The cobalt chromium EES stent has a strut thickness of 81µm, and is coated with a 7.6 µm thick, non-erodable, co-polymer of poly vinylidene fluoride co-hexafluoropropylene (PVDF-HFP), and poly n-butyl methacrylate (PBMA), which facilitates elution of everolimus over 120-days (Table 2). The feasibility of using everolimus on a DES was first assessed in the FUTURE I and FUTURE II studies. Numerous randomised studies have compared the performance of EES to BMS, PES, SES, R-ZES and most recently stents with biodegradable polymers. This stent was also commercially available until 2012 as the Promus™ (Boston Scientific, Natick, MA) stent.
XIENCE PRIME™ (Abbott Vascular, Santa Clara, CA, USA)
The Xience PRIME EES, represents a newer iteration of the Xience® V stent. This modified EES has a CoCr platform; however, this is mounted on a new enhanced stent delivery system that enables the stent to be more flexible and deliverable and offers longer stent lengths. Furthermore, the stent balloon has higher rate burst pressures (18 atm vs. 16 atm), and shorter balloon tapers (1-2 mm vs. 3-5 mm) to minimize the risk of edge dissections. The stent’s efficacy and safety has been demonstrated in the 510 patient SPIRIT PRIME clinical trial which met its primary endpoint of TLF at 1-year with statistical significance when compared to pre-specified performance goals derived from previous EES trials. Furthermore, the safety and effectiveness profile of the Xience PRIME EES was also similar and consistent to that of the Xience EES. On the basis of the SPIRIT PRIME clinical data the FDA approved the stent for use in the US in late 2011.
EES vs. BMS
The SPIRIT FIRST study enrolled 56 patients (EES = 27, BMS = 29) and demonstrated superior performance of EES with respect to 6-month in-stent late lumen loss (0.10 mm vs. 0.87 mm, p < 0.001), and angiographic binary restenosis (0.0 vs. 25.9, p < 0.05) (Table 7). Similarly, clinical follow-up through to 5-years demonstrated significantly lower rates of TLR with the use of EES, with comparable rates of mortality, MI and overall MACE.
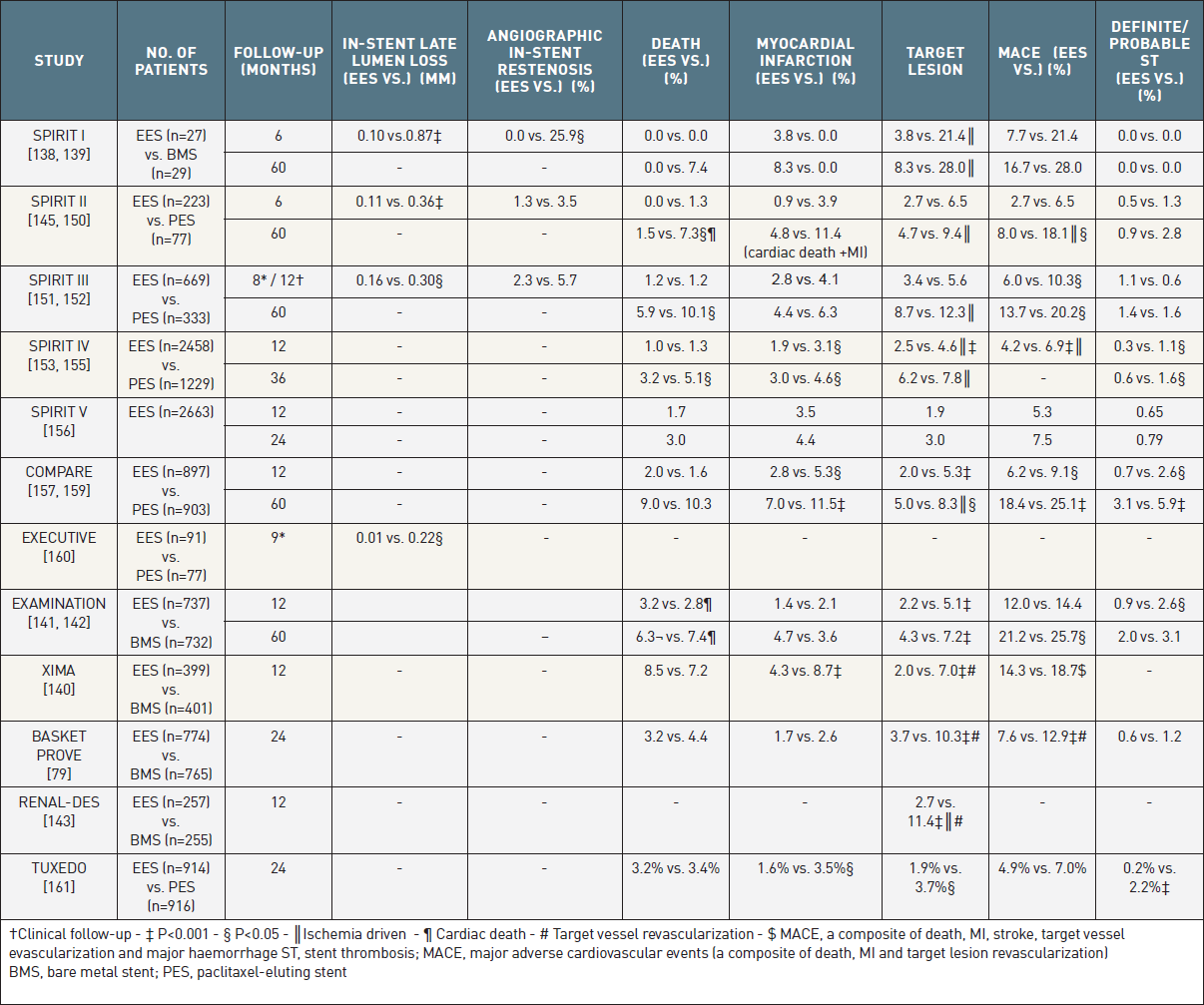
The most prominent randomized trials comparing the 2nd generation everolimus-eluting stent to the bare-metal stent and to the paclitaxel-eluting stent. Differences non-significant unless indicated.
Contemporary studies of EES versus BMS have been conducted in specific patient groups including patients with stable angina over 80 years of age (XIMA), patients undergoing primary PCI for AMI (EXAMINATION), patients requiring stents greater than 3mm in diameter (BASKET PROVE) and patients with chronic kidney disease (RENAL-DES). Results (Table 7) show superior efficacy with EES compared with BMS, and comparable safety. [79, 140-143] A meta-analysis of these studies (excluding RENAL-DES) by Valgimigli et al, which included 4896 patients followed-up for a median of 720 days, reaffirmed that compared to BMS, EES lowered MI and ST as well as cardiovascular mortality.
EES vs. PES
Six randomised trials have compared EES to PES in 8,819 patients with increasingly complex lesions ranging from those with up to two relatively simple de novo lesions in the SPIRIT II study, to the unrestricted all-comers population in the COMPARE study (Table 7). Irrespective of patient complexity or follow-up period, angiographic and clinical outcomes have consistently demonstrated superior outcomes in those treated with EES. Specifically in the SPIRIT II (0.11 mm vs. 0.36 mm) and SPIRIT III (0.16 mm vs. 0.30 mm) study in-stent late loss at 6- and 8-months, respectively were significantly lower with EES (Figure 12). Consistent with these results are findings of the EXECUTIVE study, which enrolled patients with multivessel disease, and reported in-stent late lumen losses at 9-months follow-up of 0.08 mm (95% CI: -0.01, 0.16) and 0.22 mm (95% CI: -0.13, 0.31) (p = 0.018) amongst patients randomised to EES and PES, respectively. Longer angiographic follow-up is only available from the SPIRIT II study, and this demonstrated evidence of catch up in late loss with EES, such that the significant difference in in-stent late loss between EES and PES which was observed at 6-months was no longer present at 2-years. Nevertheless, clinical outcomes at 3-, 4- and 5-year follow-up in the SPIRIT II study remain consistent with those seen at 6-months and 1-year (Figure 12). Similarly, at 5-year follow-up in the SPIRIT III study, treatment with EES led to significantly lower rates of MACE. More extensive assessment of EES took place in the SPIRIT IV trial, which randomized 3,690 patients (EES = 2,458, PES = 1,229), and the all-comers COMPARE study, which recruited 1,800 patients (EES = 897, PES = 903).[153-155, 157-159, 162] At 3- (SPIRT IV) and 5-year (COMPARE) follow-up both studies reported superior efficacy and safety with EES compared to PES. Notably rates of definite/probable ST were significantly lower with EES in both at final follow-up (SPIRIT IV 0.6% vs. 1.6%, p=0.003 and COMPARE 3.1% vs. 5.9%, p=0.005). The TUXEDO trial compared EES vs. PES among 1830 diabetic patients. At 2-year follow-up, EES was associated with a significant reduction in the risk of TVF (4.3% vs. 6.6%, p=0.03), mainly driven by a reduction in the risk of MI, TLR, and ST.
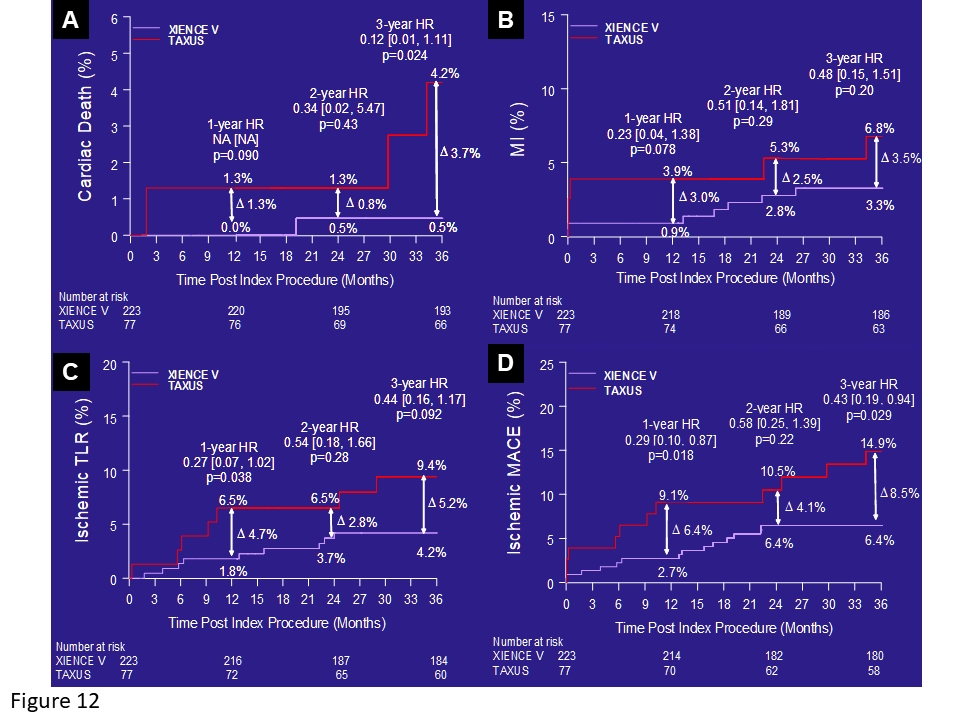
Clinical outcomes in the SPIRIT II trial up to three years. Cardiac death (A), myocardial infarction (B), ischaemic target lesion revascularisation (TLR) (C), and ischaemic MACE (D) are shown. EES in white, PES in red. [Reproduced with permission of ].
A patient-level pooled analysis of the 6,789 patients enrolled in the SPIRIT-II, -III, -IV and COMPARE studies has confirmed the superior performance of EES compared with PES. At 12-months follow-up whilst there were no between-stent differences in mortality or cardiac death, there were significantly lower rates of MI (2.1% vs. 4.0%, p < 0.001), ischaemic TLR (2.3% vs. 4.7%, p < 0.001), MACE (4.4% vs. 7.6%), definite ST (0.4% vs. 1.2%, p < 0.001) and definite/probable ST (0.5% vs. 1.5%, p < 0.001) with EES. Results were maintained even after adjustment of confounding factors. Following on from this, meta-analysis of the SPIRIT studies at 3-year follow-up have shown the emergence of a clear safety advantage with the use of EES compared to PES. Amongst 4,989 patients, who were prospectively randomised to EES (n=3350) or PES (n=1639), significantly lower rates of all endpoints including all-cause mortality (HR 0.65, p=0.003), MI (HR 0.64, p=0.02), TLR (HR 0.72, p=0.004), MACE (HR 0.71, p=0.0002) and definite/probable ST (HR 0.45, p=0.003) were seen with EES.
EES vs. SES
Several studies have reported the results from the comparison of EES with SES, which has been regarded as the most efficacious first generation DES (Table 8).,
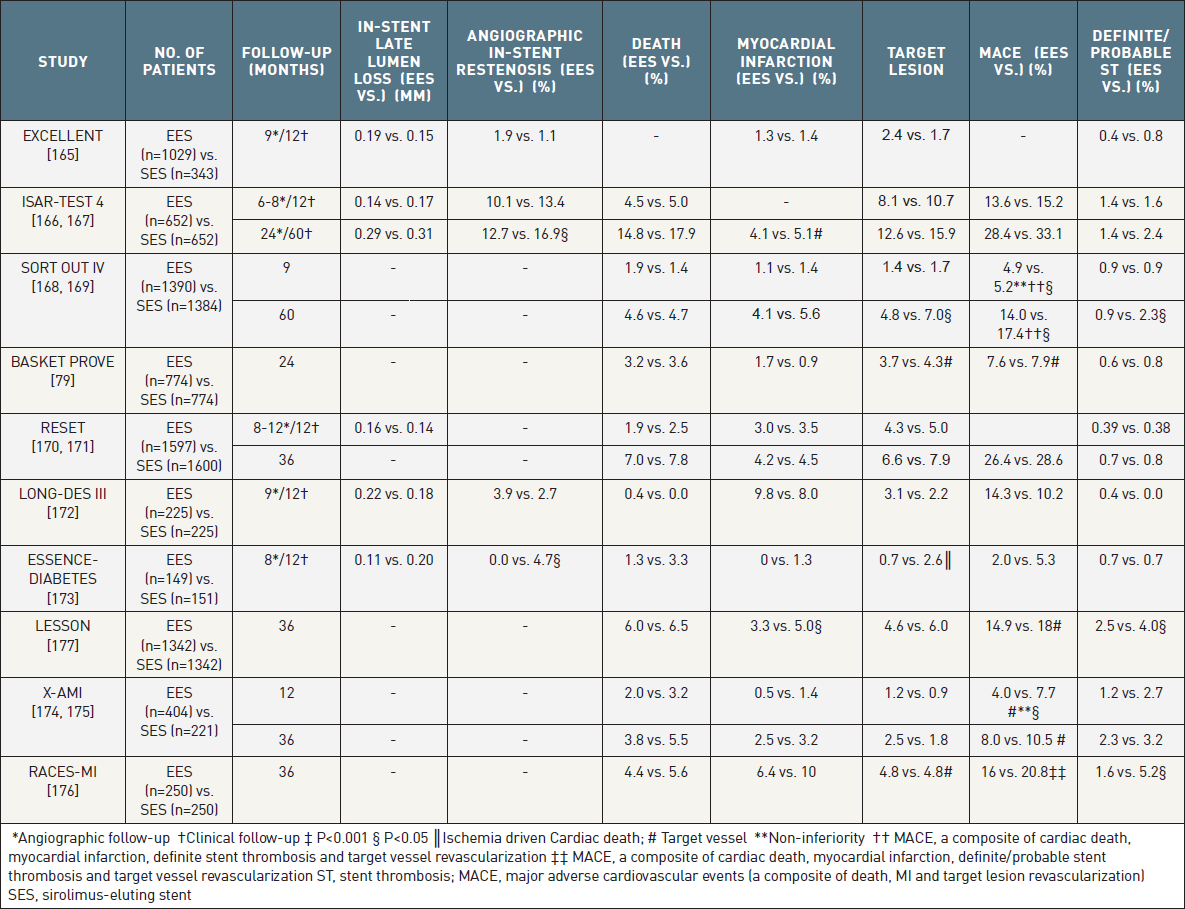
The most prominent randomized trials and registries comparing the 2nd generation everolimus eluting stent to the sirolimus-eluting stent. Differences non-significant unless indicated.
The EXCELLENT study enrolled 1,372 patients randomised 3:1 to EES (n = 1029) and SES (n = 343). The study achieved its pre-specified non-inferiority primary endpoint of in-segment late lumen loss at 9-months (EES 0.10 mm vs. SES 0.05 mm, Pnon-inferoirty = 0.023). At 12-months clinical follow-up there were no significant differences in rates of MI, TLR, and the composites of mortality/MI and MACE. Rates of ST were lower with EES (0.4% vs. 0.8%, p = 0.028).
In a sub-study of the ISAR-TEST 4 trial, late loss at 6-8 months amongst the 1,304 patients randomised to treatment with EES and SES was 0.14 mm versus 0.17 mm respectively (p = NS). At 2 years of follow-up with repeat angiography performed, the investigators observed a trend towards lower TLR (9.9% vs. 13.5%, HR=0.73, 0.52-1.01, p = 0.06) and a significant reduction of binary restenosis (12.7% vs. 16.9%, p = 0.03) in favour of EES in the absence of differences for safety endpoints. At 5-year clinical follow-up both efficacy and safety remained numerically lower with EES (p > 0.05 for all).
SORT OUT IV reported non-inferior outcomes with EES compared with SES in terms of MACE (4.9% vs. 5.2%, HR 0.94, 0.67-1.31) and TLR (1.4% vs. 1.7%, HR 0.87, 0.48-1.58) at 9 months among 2,774 patients randomly assigned treatment with EES or SES. Differential outcomes occurred after the first year, and at 5-years significantly lower rates of MACE were seen in those treated with EES (14.0% vs. 17.4%, HR 0.80, p=0.02), which was larger the result of significantly lower rates of definite ST with EES (0.4% vs. 2.0%, HR 0.18).
The largest randomised study of EES and SES is the RESET study which randomised 3197 all-comers patients and achieved its pre-specified non-inferiority primary clinical endpoint with rates of TLR at 12-months of 4.3% and 5.0% with EES and SES, respectively (Pnon-inferority<0.001). Other safety and efficacy endpoints were comparable between the stents with similar results observed at 3-years. Of note, significant between-stent differences in favour of EES were seen in the secondary composite endpoints of TLF, TVF, MACE, and the device-orientated endpoint.
BASKET PROVE randomly assigned 2,314 patients undergoing stent implantation of large vessels (stent diameter > 3.0 mm) to receive SES, EES or BMS. At 2 years of follow-up, TVR was lower with both EES (3.7%) and SES (4.3%) as compared with BMS (10.3%, p = 0.005 vs SES, p = 0.002 vs EES), however, the event rates were similar for EES and SES (3.7% vs 4.3%, p = 0.85).
LONG-DES III assessed outcomes in 500 patients randomised to EES and SES who had a coronary lesion which required at least 28 mm of stent. The study failed to meet its non-inferiority primary endpoint of in-segment late loss at 9-months follow-up (EES 0.17 mm vs. SES 0.09 mm, Pnon-inferiority = 0.96, Psuperiority = 0.04). Furthermore, in-segment binary angiographic restenosis was also significantly lower with SES (EES 7.3% vs. SES 2.7%, p = 0.046). Despite these angiographic outcomes, there were no significant between-stent differences in clinical outcomes.
ESSENCE-DIABETES study showed a similar trend in the assessment of EES versus SES in patients with diabetes. Specifically the study demonstrated that EES was non-inferior to SES in terms of in-segment late loss and angiographic restenosis at 8-months, with similar clinical outcomes being seen at 12-months follow-up.
The X-AMI study randomised 625 patients undergoing primary PCI for acute MI in a 2:1 ratio (EES n=404, SES n=221). The study met its non-inferiority primary endpoint of MACE, a composite of cardiac death, non-fatal MI and TVR at 1-year (EES 4.0% vs. SES 7.7%, Pnon-inferority=0.048); no individual endpoints were significantly different. Rates of ST were low considering the population, and no between-stent differences were observed. A further analysis at 3-years reported low overall events rates without identifying any significant differences between patients treated with EES or SES.
The RACES-MI study also compared the performance of EES and SES in the setting of primary PCI for AMI randomising 500 patients in a 1:1 fashion (EES n=250, SES n=250). The study was powered for a primary endpoint of MACE, a composite of cardiac death, reinfarction, definite or probable ST and TVR at 3-year follow-up. Results showed comparable outcomes for MACE and its components apart from ST, which was significantly lower in patients receiving EES (EES 1.6% vs. SES 5.2%, p = 0.035).
A meta-analysis of the 7,370 patients (EES = 4044, SES = 3326) enrolled in BASKET–PROVE, ESSENCE-DIABETES, EXCELLENT, SORT OUT IV and ISAR-TEST 4 has confirmed the comparable performance of EES compared with SES in terms of efficacy and safety. At a median of 13.3 months follow-up rates of MACE (7.2% vs. 8.8%, p = 0.28), cardiac death (2.2% vs. 2.6%, p = 0.92), MI (1.7% vs. 1.9%, p = 0.76), repeat revascularization (3.8% vs. 4.8%, p = 0.16), and the composite of definite and probable ST (0.8% vs. 1.0%, p = 0.33) were not significantly different between EES and SES. However, this analysis did not include the most recent trial reports and therefore requires an update to include longer-term follow-up data.
A larger meta-analysis by Park et al which included 11 randomised trials and just under 13,000 patients followed-up for a median of 23.8 months, also confirmed comparable safety outcomes between EES and SES. In contrast to the previous meta-analysis this study was able to demonstrate significantly lower rates of repeat revascularization (OR 0.85, p=0.047) and definite ST (OR 0.44, p=0.007) with EES.
EES vs. Non-EES DES Durable Polymer DES
A meta-analysis of 13 randomised trials enrolling a total of 17101 patients treated with either EES (n = 9764) or non-EES DES (n = 7337) has confirmed a consistent benefit with the use EES out to a mean follow-up of 21.7 months. Specifically use of EES was associated with similar cardiac mortality (1.6% vs. 1.9%, p = 0.38) and significant reductions in rates of MI (2.9% vs. 3.9%, p = 0.02), TVR (5.7% vs. 7.7%, p = 0.004) and definite/probable ST (0.7% vs. 1.5%, p = 0.001), when compared to patients receiving non-EES DES.
Consistent with this are the results of a larger comprehensive network meta-analysis of 51 randomised studies by Palmerini et al which included just over 51,000 patients, and demonstrated that:
Other analyses include a mixed-treatment comparison analysis of DES (SES, PES, EES, E-ZES and R-ZES) versus BMS with 117,762 patient-years of follow-up, which reported similar findings, and concluded that EES was overall the stent with the most advantageous safety profile.
A similar analysis in patients with diabetes treated with either SES, PES, EES, E-ZES, R-ZES or BMS by Bangalore et al also concluded that EES was the safest and most efficacious stent through 22,844 patient years of follow-up. A smaller meta-analysis which only included studies using EES also reported significant reductions in ST with EES out to 2-years follow-up.
Several factors that have been suggested to be behind the consistent superior performance of EES including the fact that everolimus is slightly more lipophilic than sirolimus, and therefore more rapidly absorbed into the arterial wall. In addition, pre-clinical data have suggested that the combination non-erodible, co-polymer of PVDF-HFP and PBMA, is potentially associated with less inflammation than seen with the polymers on SES and PES. Finally, the fluoro-polymer has been shown to have thrombo-resistant properties, which when combined with thin-struts, and the reduced polymer and drug load may contribute to the low rates of ST with EES.
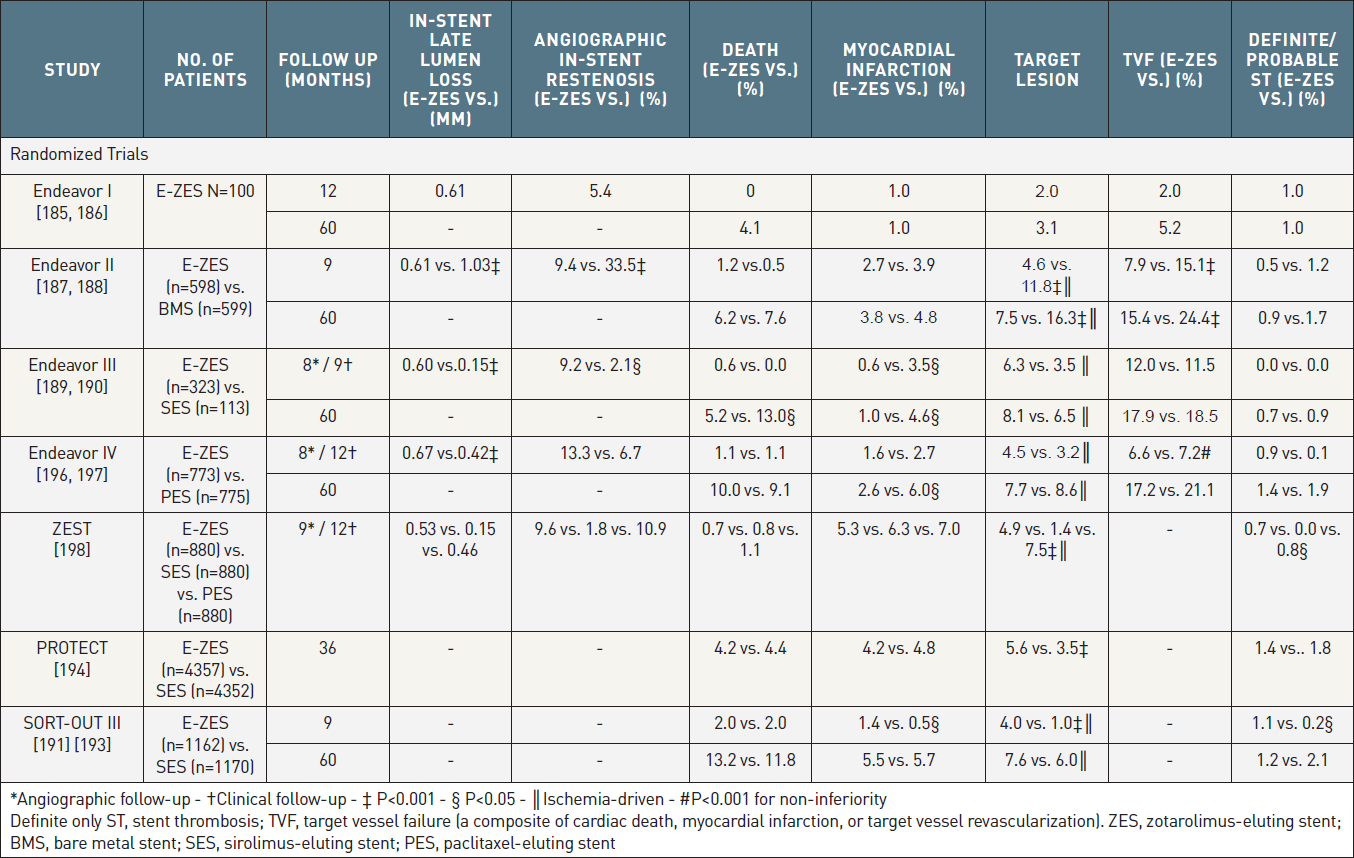
The first clinical assessment of E-ZES took place in the 100 patient single arm ENDEAVOR I study, which reported a 12-months in-stent late loss and binary restenosis rate of 0.61 ± 0.44 mm and 5.4%, respectively. Clinic event rates were low, with 2 TLRs, 1 MI and 1 definite/probable ST at 1-year, and only one further TLR and no addition MIs or ST events reported out to 5-year follow-up.
E-ZES vs. BMS
The ENDEAVOR II trial enrolled 1197 patients (ZES = 598, BMS = 599) and demonstrated significantly lower rates of in-stent late loss (0.61 ± 0.46 mm vs. 1.03 ± 0.58 mm, p < 0.001), binary in-stent restenosis (9.4% vs. 33.5%, p < 0.001), TLR (4.6% vs. 11.8%, p < 0.001) and TVF, a composite of cardiac death, MI attributable to the target vessel, and clinically-driven TLR, (7.9% vs. 15.1%, p < 0.001) at 9-months follow-up, with additional clinical follow-up at 5-years indicating a sustained benefit in favour of E-ZES with respect to TLR and TVF. Mortality and rates of MI and ST were comparable at all time points (Table 9).
The most prominent randomized trials and registries of the 2nd generation Endeavor zotarolimus eluting stent. Differences non- significant unless indicated.
E-ZES vs. SES
The comparison of E-ZES and SES has taken place in three randomised studies - ENDEAVOR III, SORT-OUT III and PROTECT. ENDEAVOR III compared E-ZES with SES in a non-inferiority trial with a primary angiographic endpoint (N = 436 patients). E-ZES was found inferior to SES regarding late loss (in-stent: 0.60 ± 0.48 mm vs. 0.15 ± 0.34 mm, p < 0.001) (Figure 13) and binary restenosis (in-segment: 11.7% vs. 4.3%, p = 0.04). Conversely, the incidence of late acquired stent malapposition as assessed by IVUS was lower with E-ZES than SES (0.5% vs. 5.9%, p = 0.02). E-ZES had a lower rate of MI than SES (SES: 3.5% vs. E-ZES: 0.6%, RR = 0.18, 95% CI 0.03-0.96, p = 0.04) at 9 months, which was mainly due to a lower incidence of peri-procedural myonecrosis. There were no significant differences in rates of death, cardiac death, ST, repeat revascularization, MACE, and TVF. At 5-years the absolute difference in TLR between E-ZES and SES was small 1.6% at 5-years (E-ZES 8.1% vs. SES 6.5%). Rates of ST remained similar between both groups throughout follow-up, although the study was not powered for this endpoint.
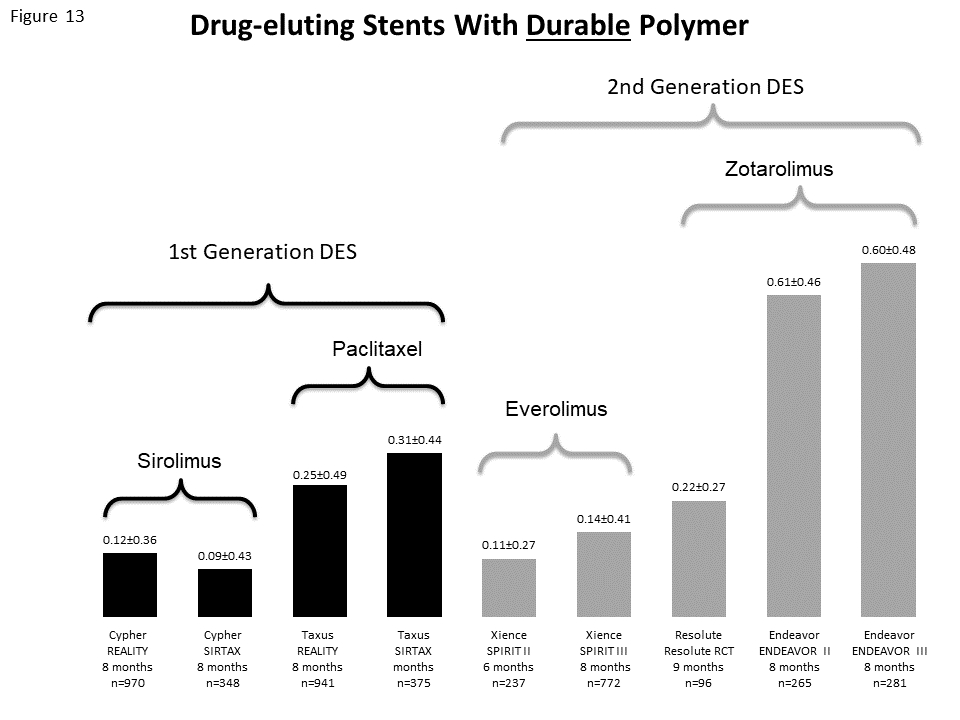
Late lumen loss of early and newer-generation DES platforms with durable polymers.
In contrast, SORT-OUT III enrolled 2332 patients (E-ZES = 1162, SES = 1170) and reported significant differences in favour of SES with respect to MI, TLR and ST at both 9- and 18-months follow-up. At 3-years, rates of MI (E-ZES 3.8% vs. SES 3.3%, p = 0.44) and ST (1.1% vs. 1.4%, p = 0.61) were comparable between E-ZES and SES, whilst TLR remained significantly lower with SES (6.8% vs. 3.9%, p = 0.002). This significant difference in TLR was no longer present at final 5-year follow-up (7.6% vs. 6.0%, p=0.15); similarly no between-stent differences in death, MI or ST was seen. Landmark analyses showed significantly lower rates of definite ST (0.1% vs. 1.8%, p=0.003), TLR (2.4% vs. 4.8%, p=0.003) and TVR (4.1% vs. 7.0%, p=0.003) with E-ZES compared with SES between 1- and 5-years, thereby reversing the significantly higher rates of these respective endpoints with E-ZES at 1-year follow-up (definite ST 1.1% vs. 0.3%, p=0.04; TLR 5.3% vs. 1.4%, p<0.001; TVR 6.7% vs. 2.8%, p<0.001).
The much larger PROTECT study recruited 8709 all-comers patients who were randomised to treatment with SES and E-ZES.30 Uniquely the study was powered to detect a 1% difference in definite/probable ST at 3-years follow-up, however consequent to event rates in the SES arm (1.8%) being lower than anticipated in the power calculation (2.5%), even this large study was somewhat underpowered. The study failed to identify any significant differences between E-ZES and SES with regards the primary endpoint of definite/probable ST (E-ZES 1.4% vs. SES 1.8%, HR:0.81) and secondary clinical safety endpoints such as death and MI at 3 years. However, in the pre-specified 4-year of follow-up there was an increase in the absolute between-stent difference in definite/probable ST from 0.4% at 3-years to 1.0%, such that rates were significantly lower with E-ZES at 4-years (1.6% vs. 2.6%, p=0.003). with resultant lower rates of MI as per the extended historical definition (E-ZES 4.6% vs. SES 5.8%, p=0.02). Whilst TVR was comparable at 4-years follow-up (9.0% vs. 8.6%), TLR remained significantly higher with E-ZES (5.9% vs. 4.5%, p=0.002), however there was a fall in the absolute between-stent difference (2.1% at 3-years vs. 1.4% at 4-years).
Overall these three studies confirm differential clinical outcomes over time amongst these two DES with differing abilities to suppress neointimal hyperplasia. During early follow-up E-ZES is associated with inferior outcomes compared to SES, however these differences appear to disappear or even reverse with long-term follow-up. Importantly, these contrasting short- and long-term results have implications for clinical trial design reiterating the need for long-term follow-up to fully evaluate the efficacy and safety of DES.
E-ZES vs. PES
ENDEAVOR IV compared E-ZES with PES in a non-inferiority, randomized trial enrolling 1,548 patients with a primary clinical endpoint of TVF (Table 9). In the angiographic arm of the trial, E-ZES did not achieve the pre-specified secondary endpoint of in-segment late loss (0.36 ± 47 mm vs. 0.23 ± 0.45 mm, p = 0.023). However, E-ZES met its primary clinical endpoint of non-inferiority on TVF at 9 months (E-ZES: 6.6% vs. PES: 7.2%, p = 0.685). While the rate of MI was lower at 30 days (0.8% vs. 2.3%, p = 0.02) largely related to fewer side-branch occlusions, there were no significant differences in rates of death, cardiac death, or MI at 9 and 12 months. The 5 year clinical follow-up results of ENDEAVOR IV revealed an increasing safety benefit of E-ZES over PES with a lower rate of the composite of cardiac death and MI (E-ZES=6.4%, vs. PES=9.1%, p = 0.048). Rates of definite and probable ST were no different at 9 months (E-ZES=0.8% vs. PES=0.1%, P=0.12) or 5 years (E-ZES=1.4% vs. PES=1.9%, p=0.42). Of note, the incidence of very late ARC definite and probable ST between one and five years was significantly reduced in favor of patients treated with E-ZES (E-ZES=0.4% vs. PES=1.8%, p = 0.012). In terms of efficacy, differences in rates of TLR remained unchanged among E-ZES (7.7%) and PES (8.6%, p = 0.70) treated patients.
E-ZES vs. SES vs. PES
The ZEST trial compared outcomes amongst 2640 patients randomised to E-ZES (n = 880), PES (n = 880) and SES (n = 880). The primary endpoint was MACE at 12-months, with the comparison of E-ZES with SES analysed as a non-inferiority analysis, whilst the comparison between E-ZES and PES was a superiority analysis (Table 9). At 12 months, MACE rates were non-inferior between E-ZES and SES (10.2% vs. 8.3%, Pnon-inferiority = 0.01, Psuperiority = 0.17) and significantly lower with E-ZES compared with PES (10.2% vs. 14.1%, p=0.01). The incidence of death or MI was similar (E-ZES 5.8% vs. SES 6.9% vs. PES 7.6%, p = 0.31), whilst the incidence of ST was significantly lower in the SES group (E-ZES 0.7% vs. SES 0.0% vs. PES 0.8%, respectively, p = 0.02). Overall at 12-months follow-up the use of E-ZES resulted in similar rates of MACE compared with SES and fewer MACE events compared with PES.
The R-ZES is the second iteration of the E-ZES (Table 2). The first R-ZES consisted of the Driver CoCr stent platform, and a Biolinx polymer - a blend of 3 different polymers: the hydrophobic C10 polymer to control drug release; the biocompatible and hydrophilic C19 polymer; and polyvinyl pyrrolidone to allow an early burst of drug release. The polymer allows delayed drug release, such that at least 85% of the zotarolimus is released within 60 days, with the remainder being released within 180 days (Figure 14).
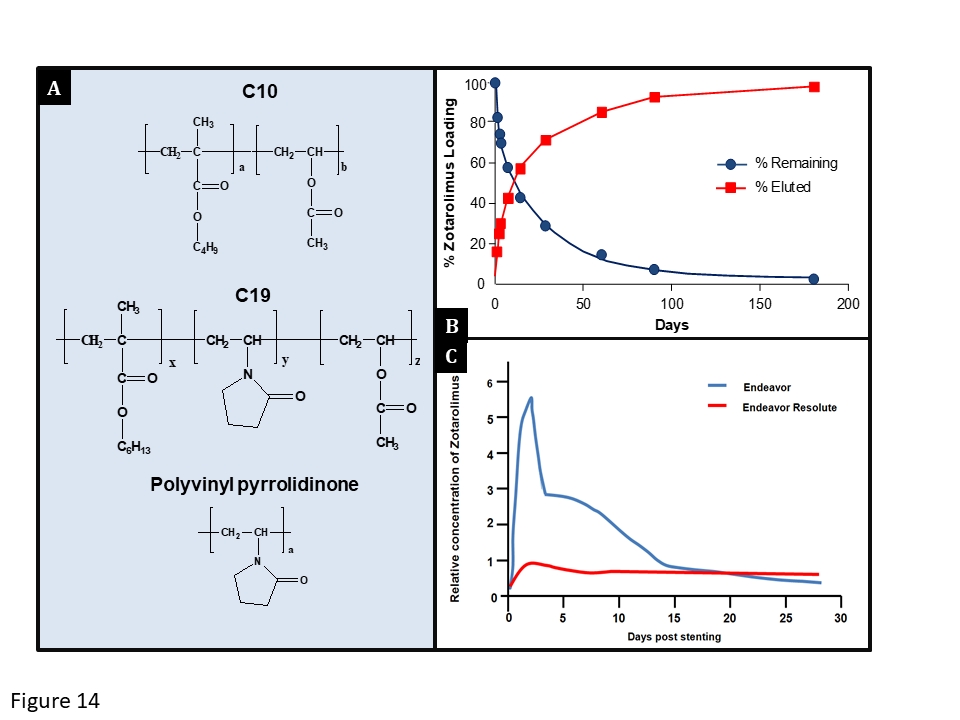
The Endeavor® Resolute stent. (A) The chemical structure of the three components of the BioLinx™ polymer system. The hydrophobic C10 polymer is based on hydrophobic butyl methacrylate to provide adequate hydrophobicity for zotarolimus. The hydrophilic C19 polymer is manufactured from a mixture of hydrophobic hexyl methacrylate, and hydrophilic vinyl pyrrolidinone and vinyl acetate monomers, to provide enhanced biocompatibility. The hydrophilic polyvinyl pyrrolidinone increases the initial drug burst and enhances biocompatibility. (B) The drug release pattern of zotarolimus: >85% is released within the first 60 days, with drug elution complete by 180 days. (C) A comparison of the relative arterial concentrations of zotarolimus in the porcine coronary artery model at various times post implantation of the Endeavor® and Endeavor® Resolute stents. The Endeavor® stent maintains effective drug levels through the initial loading of arterial tissue with zotarolimus during the first two weeks of elution. Conversely, the Endeavor® Resolute stent sustains an effective drug level in the tissue through continued, sustained elution. (B) and (C) are reproduced with permission from and Udipi et al EuroIntervention. 2007;3:137-9 respectively.
The second version of R-ZES was called the Resolute Integrity ZES, which only differed from its predecessor by being manufactured using continuous sinusoid technology. This method of stent manufacturing molds one single strand of wire into a sinusoidal wave which is then wrapped into a helical pattern and laser-fused at certain points, making the stent comparable to a flexible spring enhancing deliverability and conformability to the vessel wall. The latest iteration of the R-ZES stent is called the Resolute Onyx ZES, which this differs from the Resolute Integrity by its stent platform being made from core wire technology. Consequently the Onyx R-ZES has a denser core metal wrapped in a cobalt alloy outer layer, which enables thinner and stronger stent struts that enhance deliverability, improve conformability and increase radiopacity with no compromise to radial and longitudinal strength.
The initial evaluation of R-ZES took place in the 139 patient multi-centre, non-randomized, FIM RESOLUTE study which demonstrated an angiographic in-stent late loss of 0.22 mm at 9-months follow-up (Figure 13) and respective rates of MACE, TLR and any definite/probable ST of 16.5%, 3.1% and 0.0% at 12-months follow-up, and 14.0%, 2.3% and 0.0% at 5-year follow-up.
Several studies have evaluated the performance of R-ZES as summarized in Table 10:
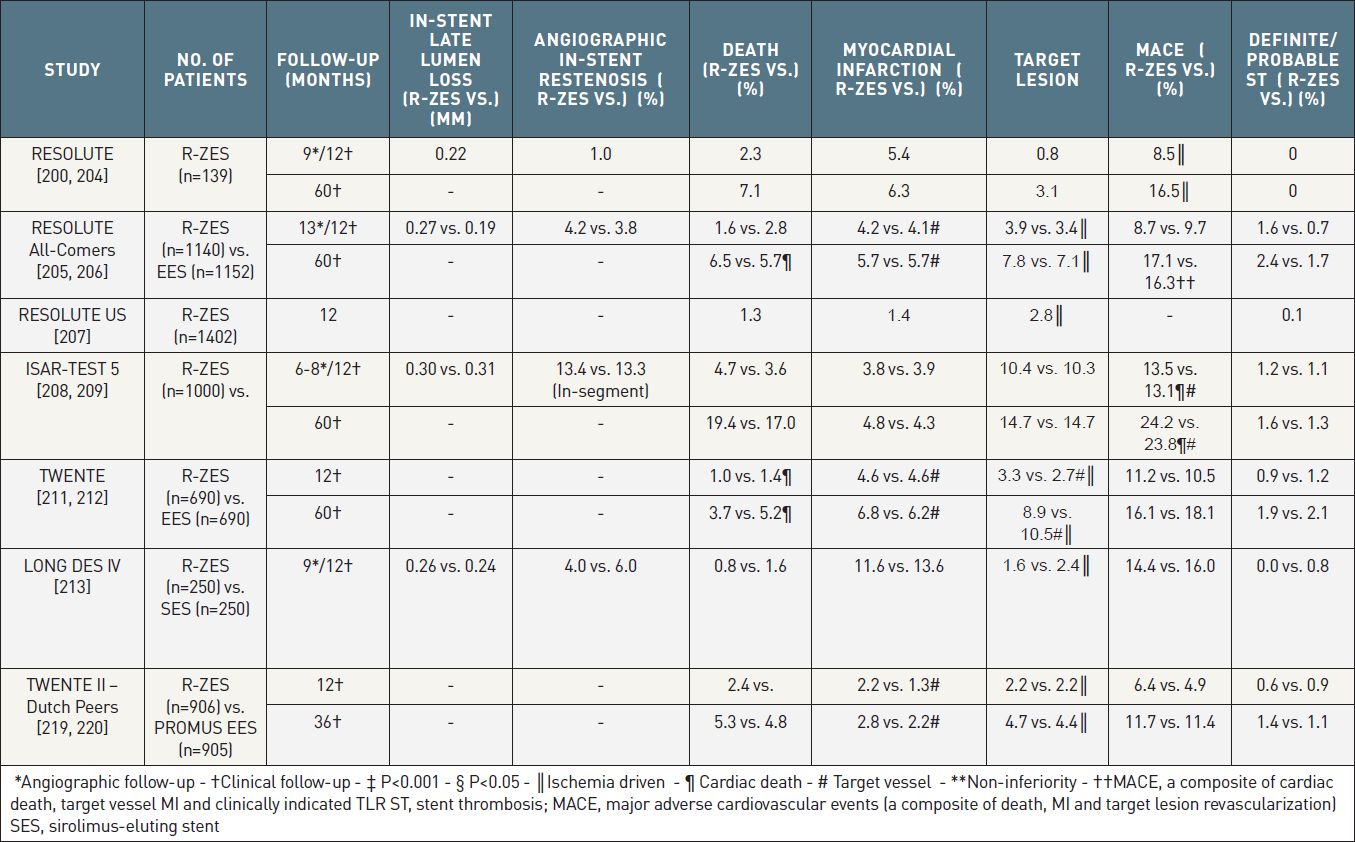
The most prominent randomized trials and registries of the 2nd generation RESOLUTE zotarolimus-eluting stent. Differences non-significant unless indicated.
The RESOLUTE All-Comers trial, which was the first randomised assessment of two new generation DES, enrolled 2,300 patients, who were randomized in a 1:1 ratio to treatment with either the R-ZES or the Xience™ V EES. At 12-months clinical follow-up in a predominantly off-label population, the R-ZES was found to be non-inferior to EES with respect to the primary clinical endpoint of TLF, a composite of cardiac death, target vessel MI and clinically indicated TLR (R-ZES 8.2% vs. EES 8.3%, Pnon-inferiority < 0.001). In addition, in a sub-group of patients who were randomised to 13-month angiographic follow-up, R-ZES was found to be non-inferior to EES with respect to the powered angiographic secondary endpoint of in-stent diameter stenosis (R-ZES 21.65 ± 14.42% versus EES 19.76 ± 14.64%, Pnon-inferiority=0.04). Considering the complex patient population, the overall rate of definite or probable ST was low at 2.3% and 1.5% for R-ZES and EES respectively (P= 0.17). Five-year results mirrored the trends seen at 1-year with no significant between-stent differences in TLR (R-ZES 17.1% vs. EES 16.3%, P=0.65) or its individual safety and efficacy components. Only 10% of patients remained on DAPT at 5-years, however despite this rates of ST were low, with very late definite/probable ST rates of only 0.84% and 1.03% (p=0.66) for R-ZES and EES, respectively.
The ISAR-TEST 5 study enrolled 3002 patients who were randomized to treatment with the R-ZES (n = 1000) and a polymer-free rapamycin/probucol dual DES (n = 2002). At 12-months follow-up the study achieved its non-inferiority primary endpoint following MACE rates of 13.1% for both stents (P=0.83, Pnon-inferiority = 0.012). The two stents were also comparable with respect to other clinical endpoints such as mortality, TLR and ST, and the angiographic endpoints in-stent late loss and binary angiographic restenosis. Rates of MACE (23.8% vs. 24.2%, p=0.80), its individual components and definite/probable ST (1.3% vs. 1.6%, p=0.64) remained similar out to 5-years follow-up. Parallel results were seen in the cohort of AMI patients.
The single centre TWENTE study randomly allocated in a 1:1 fashion 1,380 patients presenting with stable angina or non-ST elevation MI to treatment with EES or R-ZES. The primary endpoint of this non-inferiority trial included cardiac death, target vessel related-MI and clinically-driven TVR and occurred with a similar frequency for both devices (EES 8.1% vs. ZES 8.2 %, Pnon-inferiority = 0.001). Similar to RESOLUTE All-comers, rates of definite or probable ST were low and of similar magnitude between groups (R-ZES 0.86% vs. EES 1.16%, Pnon-inferiority = 0.12). The safety and efficacy of both stents remained comparable at 5-year follow-up.
The LONG DES IV study randomised 500 patients with coronary lesions ≥ 25mm in length to treatment with either R-ZES (n = 250) or SES (n = 250). The study achieved its primary endpoint by demonstrating the non-inferior performance of R-ZES compared to SES for angiographic in-segment late lumen loss at 9-month follow-up (R-ZES 0.14 ± 0.38 vs. SES 0.12 ± 0.43, Pnon-inferiority = 0.03, Psuperiority = 0.6). Both stent platforms were associated with comparably low clinical events rates.
The PROMUS Element stent has a PtCr platform, a PBMA primer coating, a PVDF-HFP polymer and is loaded with 1 µg/mm2 of everolimus, 80% of which is eluted within 90-days of stent implantation (Table 2). Initial assessment of the stent took place in the PLATINUM clinical trial programme comprising of:
The PROMUS element stent platform design has undergone a small important modification; this second iteration, called the PROMUS Premier stent, has two additional proximal connectors designed to improve longitudinal strength in the area where distortion is most common.
Two all-comers randomised non-inferiority studies have reported outcomes comparing treatment with the Promus EES and R-ZES.
The DUTCH PEERS study enrolled 1811 patients in a 1:1 ratio (EES 905 vs. R-ZES 906) and met its non-inferiority endpoint of TVF, a composite of cardiac death, target-vessel MI, and TVR (EES 5% vs. R-ZES 6%, Pnon-inferiority=0.006). All components of the primary endpoint were also comparable. Definite ST rates were low (EES 0.7% vs. R-ZES 0.3%, p=0.34). Longitudinal stent deformation was identified in 9 out of 1591 implanted EES stents, with no deformed R-ZES stents; reassuringly these deformed stents were not associated with any adverse clinical outcomes. No significant between-stent differences emerged out to 3-years of clinical follow-up.
The larger HOST-ASSURE study randomised 3755 patients in a 2:1 ratio to treatment with Promus EES (n=2503) or R-ZES (n=1252). The primary endpoint, which was TLF, a composite of cardiac death, target vessel MI and TLR occurred in 2.9% of patients treated with EES and R-ZES, achieving the pre-specific margin of non-inferiority (Psuperiority=0.006, Pnon-inferiority=0.0025). There were no differences in the components of the primary endpoint, the patient-orientated composite endpoint or definite/probable ST. As in the DUTCH PEERS study there were no stent deformations in the R-ZES arm, however 7 out of the 3500 Promus EES stents deployed were deformed with no resultant clinical sequela.
Two all-comers randomised non-inferiority studies have reported outcomes comparing treatment with the Promus EES and R-ZES.
The DUTCH PEERS205 study enrolled 1811 patients in a 1:1 ratio (EES 905 vs. R-ZES 906) and met its non-inferiority endpoint of target vessel failure, a composite of cardiac death, target-vessel MI, and TVR (EES 5% vs. R-ZES 6%, Pnon-inferiority=0.006). All components of the primary endpoint were also comparable. Definite ST rates were low (EES 0.7% vs. R-ZES 0.3%, p=0.34). Longitudinal stent deformation was identified in 9 out of 1591 implanted EES stents, with no deformed R-ZES stents; reassuringly these deformed stents were not associated with any adverse clinical outcomes.
The larger HOST-ASSURE study randomised 3755 patients in a 2:1 ratio to treatment with Promus EES (n=2503) or R-ZES (n=1252). The primary endpoint, which was TLF, a composite of cardiac death, target vessel MI and TLR occurred in 2.9% of patients treated with EES and R-ZES, achieving the pre-specific margin of non-inferiority (Psuperiority=0.006, Pnon-inferiority=0.0025). There were no differences in the components of the primary endpoint, the patient-orientated composite endpoint or definite/probable ST. As in the DUTCH PEERS study there were no stent deformations in the R-ZES arm, however 7 out of the 3500 Promus EES stents deployed were deformed with no resultant clinical sequelae.
The Elixir DESyne permanent polymer novolimus eluting stent (NES) was first assessed in the 15-patient FIM EXCELLA study, which reported an angiographic in-stent late loss of 0.31 ± 0.25 mm, and a percent volume obstruction on IVUS of 6.0 ± 4.4% at 8-months follow-up, together with no MACE through 12 months, and one MACE event at 24 months (Table 11).
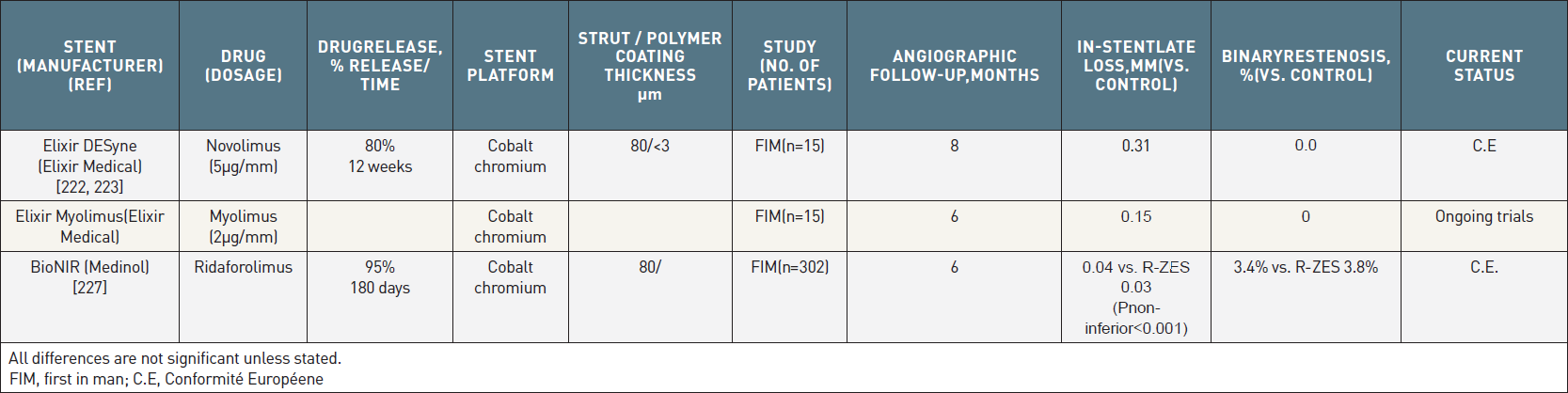
New metallic stents with durable polymers which are either currently available outside the USA, or undergoing clinical evaluation.
Further assessment of the NES has been performed in the single-blind, prospective EXCELLA-II study, which randomised 210 patients to treatment with either NES (n = 139) or E-ZES (n = 71). At 9-month follow-up, the primary endpoint of angiographic in-stent late loss was measured at 0.11 ± 0.32 mm, and to 0.63 ± 0.42 mm in patients treated with NES and ZES, respectively (Pnon-inferiority < 0.0001, Psuperiority < 0.0001). At 12-months clinical follow-up there were no significant differences between stent groups in the device orientated composite endpoint (NES 2.9% vs. E-ZES 5.6%, p = 0.45) or its individual components. The rate of ST was comparable between both groups. At 5-year follow-up, patients in the NES group had significantly lower rates of the patient-oriented (HR 0.53, 95% CI: 0.32-0.87, p=0.013) and device-oriented (HR 0.38, 95% CI: 0.17-0.83, p=0.011) composite endpoints. Rates of cardiac death and definite/probable stent thrombosis were similar between the two groups; however, there was a trend towards reduction in MI and repeat revascularisation in the NES group.
The FIM study of the myolimus-eluting stent enrolled 15-patients, and at 6-months angiographic follow-up in-stent late lumen loss, binary restenosis and percent neointimal volume obstruction were 0.15 ± 0.11mm, 0.0% and 1.4%, respectively (Table 11). Clinical events out to 9-months comprised of one MI; there was no death, TLR or ST.
The BioNIR stent (Medinol, Israel) elutes ridafolimus using a bio-permanent elastomeric durable polymer, which is resistant to bending, bonding, cracking, peeling and distortions unlike other contemporary DES. The stent platform is made from CoCr and is characterised by a variable strut size and width, which ensures that drug distribution is in a more even and gradual pattern compared to other contemporary DES. The stent’s manufacturing process is also distinctive as the stents are made from a thin sheet of cobalt alloy that is laser cut, spray and coated with drug and rolled into a cylinder and laser welded. This process allows for greater efficiencies, which may lead to lower production costs compared to other DES.
The stent was first evaluated in the NIREUS FIM non-inferiority study, which randomised 302 patients in a 2:1 ratio to BioNIR (n=201) and R-ZES (n=101). The study met its primary endpoint of in-stent late lumen loss at 6-months (BioNIR 0.04mm vs. R-ZES 0.03, Pnon-inferiority<0.001). Clinical event rates were low and compared between the stents.
Further assessment has taken place in the BIONICS multi-centre randomized trial BIONICS study which randomised 1,919 patients to BioNIR (n=958) or R-ZES (n=961). The primary endpoint was TLF at 12-months follow-up and rates were identical for both devices (5.3%), achieving the pre-specified criterion for non-inferiority (Pnon-inferiority=0.0012). No significant differences in the individual components of TLF and rates of ST were seen.
Durable polymer coatings have proven to be a successful method for drug loading and release, the key determinants of DES efficacy in clinical practice. However, an important limitation of durable coatings is their undetermined effect on arterial healing. Several animal and human studies have identified durable polymer coatings of early generation DES as a possible stimulus for hypersensitivity reactions and nidus for chronic inflammation. These patho-mechanisms may play an important role in the predisposition for very late ST and delayed restenosis. Several newer generation DES platforms utilize biodegradable as opposed to durable polymers and are reviewed here. In theory immediately after implantation these devices function similar to conventional DES, however after polymer breakdown, they speculatively may offer the safety benefits of a BMS. Short-term results from these stents have been encouraging, whilst recent long-term data have provided some evidence that these stents may lead to the perceived improvements in clinical safety.
There are many challenges remaining for this polymer technology, which include amongst others, establishing the optimal biocompatibility, composition, formulation, and degradation time of the polymer. In addition attention must be paid to the pharmacokinetics of the anti-proliferative agent released by the degradation of the polymer, and the variation in polymer degradation time which can be affected by production factors such as the use of long polymer chains, decreased polymer hydrophobicity and greater polymer crystallinity; together with physical and biological environmental factors. Evidence indicates that polymer breakdown can be associated with a significant inflammatory reaction which at times can create an acidic environment; moreover, complications may also occur as a result of a persistent immune response to monomer breakdown products. These uncertainties reiterate the need for continued research, with clinical outcomes assessed at long-term follow-up.
The currently available biodegradable polymer stents, together with those under investigation are summarized in Table 12. An overview of most commonly used biodegradable polymer DES is provided in Figure 15. The first generations of biodegradable polymer devices (BioMatrix BES, Biosensors, Morges, Switzerland and Nobori BES, Terumo, Japan) have been in use for a decade, and have now been joined by a heterogeneous group of second-generation biodegradable polymer devices which use a platform of CoCr or PtCr instead of stainless steel; elute other macrocyclic lactone inhibitors such as sirolimus, everolimus, novolimus, and myolimus instead of biolimus; have struts which are between 61-80mm thick compared to 120-125mm and have polymers with a thickness of 2-15mm instead of 10-20mm (Table 12).
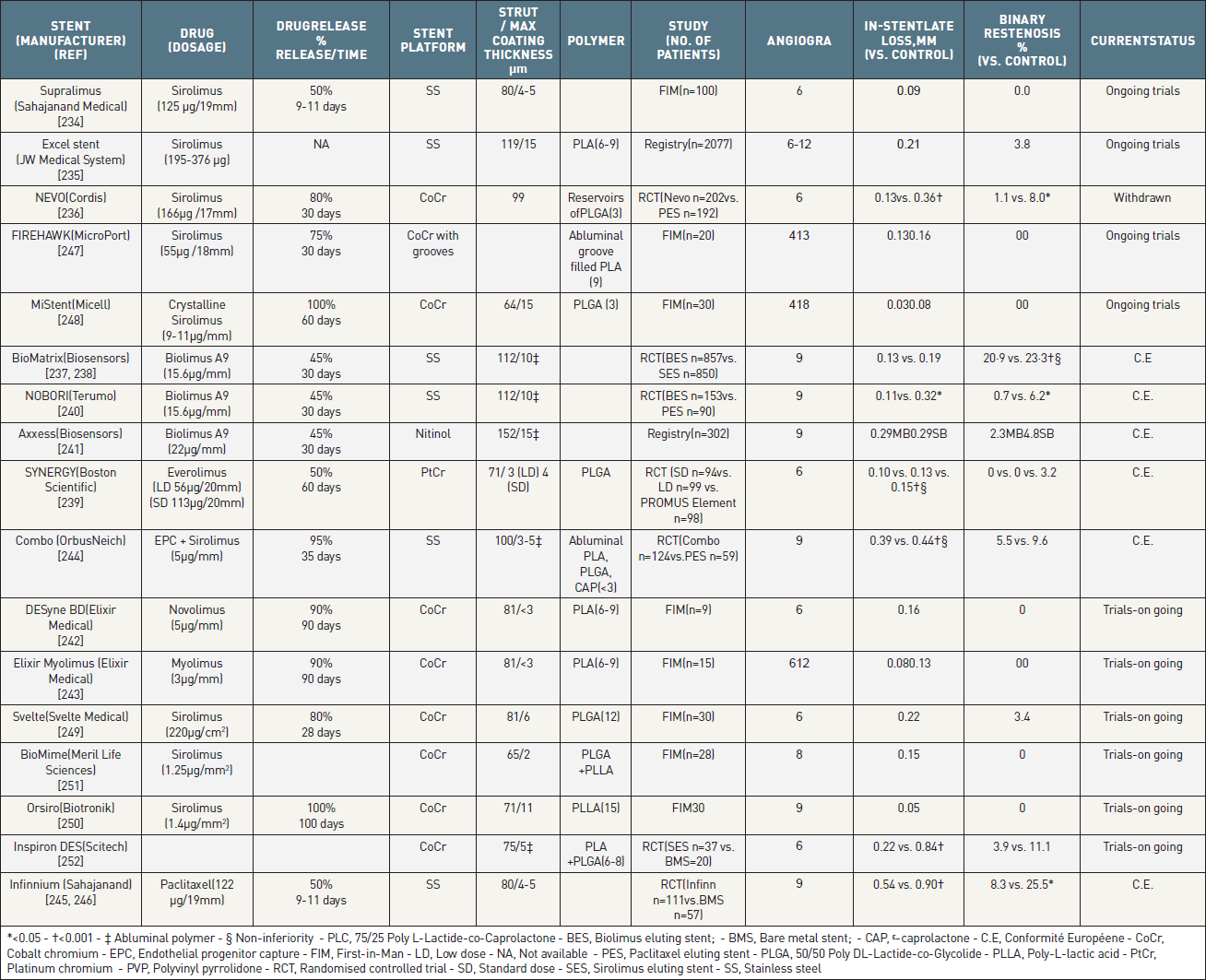
Metallic stents with a biodegradable polymer which are either currently available outside the USA, or undergoing clinical evaluation.
All differences are not significant unless stated.
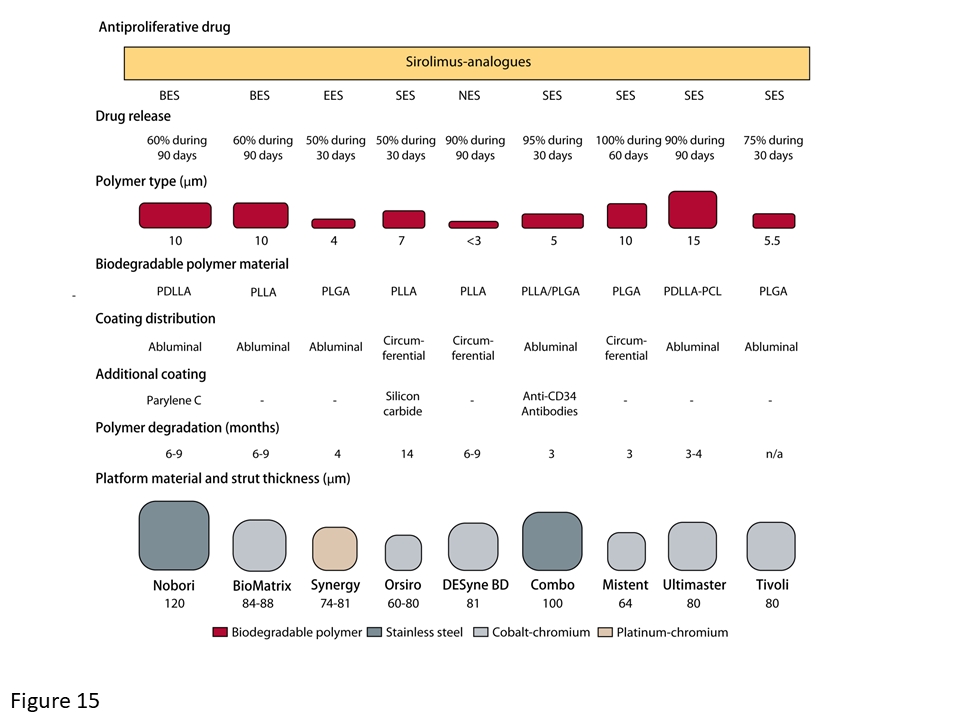
Overview of most commonly used biodegradable polymer DES in clinical practice. [Reproduced with permission from ].
Two stent platforms utilize the combination of a biodegradable PLA polymer and the elution of biolimus A9:
Biomatrix™ stent (Biosensors International PTE LTD, Singapore)
The BioMatrix stent platform has undergone several modifications since it was first developed in 2008. The original device was made of stainless steel with 125mm struts, and these have now been replaced with 84-88mm struts made of CoCr on the latest iteration, the BioMatrix Alpha stent.
The angiographic efficacy of BES was first demonstrated in the randomized STEALTH-I study which reported significantly lower in-stent late lumen loss (0.26mm vs. 0.74mm, p<0.001) and percent neointimal volume (3.2% vs. 32%, p<0.001) with BES compared to BMS at 6-months follow-up. In the angiographic follow-up group of the LEADERS study (described below), BES was non-inferior to SES for the principal angiographic endpoint of in-stent percent diameter stenosis (BES: 20.9% vs. SES: 23.3%, difference -2.2%, 95%-CI -6.0 to 1.6, Pnon-inferiority = 0.001, Psuperiority = 0.26) with no significant difference in any other angiographic endpoint. Comparisons with more contemporary devices took place in the EVERBIO II study, which randomised 238 patients 1:1:1 to BES, EES or Absorb BVS, and showed comparable rates of in-stent, and in-segment late lumen loss at 9-months angiographic follow-up for all three devices.
In the LEADERS study, the BioMatrix Flex BES (Figure 16) was compared against SES in 1,707 all comer patients undergoing PCI. BES was found non-inferior to SES for the primary clinical endpoint, a composite of cardiac death, MI, and TVR (BES: 9.2% vs. SES: 10.5%, rate ratio 0.88, 95%-CI 0.64 to 1.19, Pnon-inferiority = 0.003, Psuperiority = 0.39) (Table 12). There were no significant differences for any individual safety or efficacy endpoints between the two stents. As above, BES was also non-inferior to SES for the principal angiographic endpoint of in-stent percent diameter stenosis. Five-year follow-up data showed similar rates of MACE (BES: 22.3% vs. SES: 26.1%, HR=0.83, 95% CI 0.69-1.02, Pnon-inferiority < 0.001, Psuperiority = 0.07). Beyond one year, an increasing difference in very late definite ST emerged with an annual incidence of definite ST amounting to 0.17% in BES and 0.63% in SES treated patients. This resulted in a significant relative risk reduction of 74% (HR 0.26, CI 0.10 – 0.68, p = 0.003) in favour of BES between year one and five. The reduction in very late ST translated into a lower incidence of clinical events associated with definite ST, whereas there was no reduction in clinical events not associated with ST. The long-term findings of improved clinical outcomes as well as the interaction of treatment effect with time, namely the absence of treatment effect within the first year and an emerging differential beyond one year, provide a proof of concept with respect to the long-term advantage of a stent using the biodegradable polymer technology.
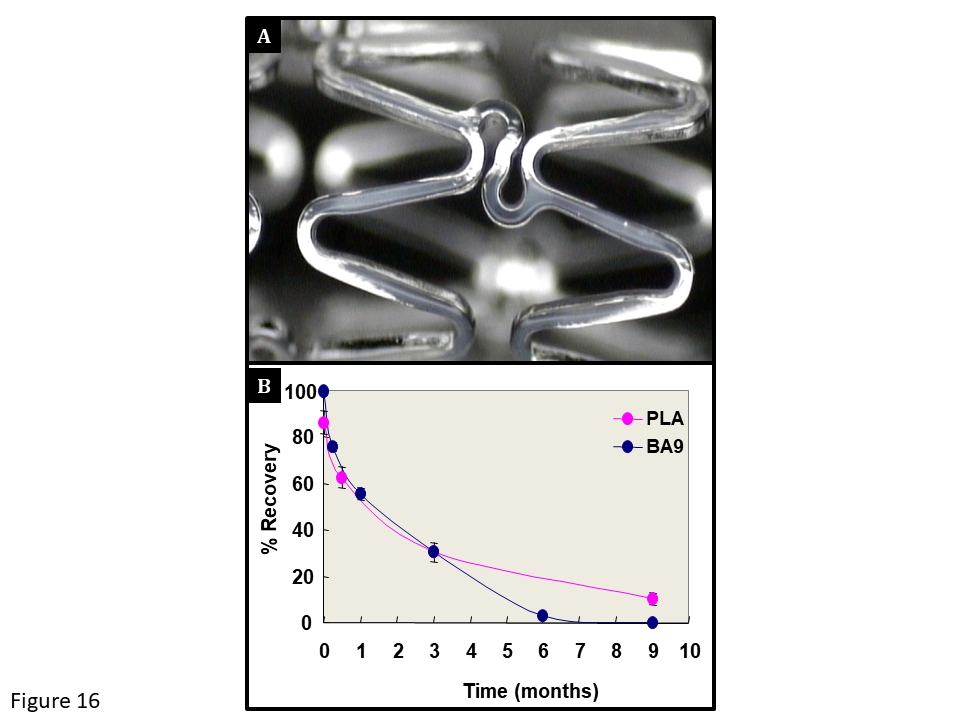
(A) The stainless steel BioMatrix™ stent. (B) The elution pattern of Biolimus A9™ (BA9) and the corresponding biodegradation pattern of the polylactic acid (PLA) polymer. (Courtesy of Biosensors SA, Morges, Switzerland).
In the COMFORTABLE study, 1161 patients undergoing primary PCI for a AMI were randomised to receive either BES (n=575) or BMS (n=582). Data out to 1-year demonstrated comparable rates of cardiac death and ST, whilst use of BES lead to significantly lower rates of MACE (4.3% vs. 8.7%, p=0.004). The benefit of BES over BMS in terms of MACE continued to accrue at out to 5 years (8.6 % vs. 14.9%, p=0.001) with clinical differences mainly driven by a significantly reduced risk for target vessel re-infarction (BES 2.2% vs. BMS 5.0%, p=0.02) and ischaemia-driven TLR (4.4% vs. 10.4%, p<0.001). Although approximately 10% of patients discontinued DAPT after 1 year and >80% at 2-years, comparable rates of very late ST were reported for BES and BMS.
The all-comers SORT-OUT VI study randomised 2,999 patients to BES (n=1497) or R-ZES (n=1502). The study met its non-inferiority primary endpoint of MACE, a composite of cardiac death, target vessel MI, and ischaemia-driven TLR with rates of 5.3% and 5.0% for R-ZES and BES, respectively (Pnon-inferiority =0.004). There were no significant differences in rates of efficacy or safety, including ST. No between-stent differences emerged out to 3-year follow-up.
Nobori™ stent (Terumo, Japan)
The Nobori™ stent uses the same PLA polymer and anti-proliferative agent as the aforementioned BioMatrix stent, however, the Nobori stent uses the S-Stent platform, which was only used on the first iteration of the BioMatrix stent. Other differences relate to the delivery system, delivery balloon, and the stent coating process. The BioMatrix stent is coated by an automated autopipette proprietary technology, whilst the Nobori stent is not. The Nobori stent has been compared with the Cypher SES, TAXUS PES and EES.
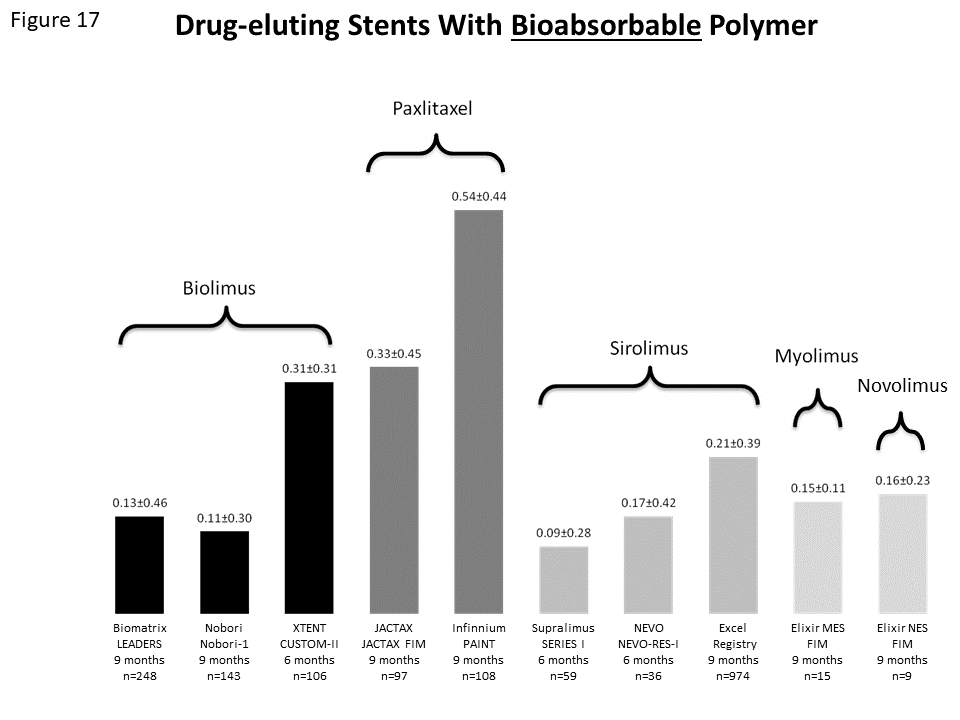
Late lumen loss of different stent platforms using bioresorbable polymers as drug carrier.
The FIM study of the Elixir DESyne BD biodegradable polymer NES enrolled 9-patients, and reported an in-stent late lumen loss of 0.16 ± 0.23 mm together with no binary restenosis at 6-months, and no MACE events through to 9-months (Figure 17). In the follow-on randomized EXCELLA II BD trial 146 patients were randomised 3:1 to the Elixir DESyne BD (n=115) or the E-ZES (n=31). The study achieved its primary endpoint by demonstrating non-inferiority of the Elixir DESyn BD compared to the control stent with respect to in-stent late loss (0.12 ± 0.15 mm vs. 0.67 ± 0.47 mm, Pnon-inferiority < 0.001, Psuperiority<0.001). In addition significantly lower rates of binary angiographic stenosis (0.0% vs. 7.9%, p = 0.003) were seen in the Elixir DESyn group. Clinical events remained low through to 5 years and clinically indicated TLR was lower in the DEsyne BD group compared with the E- ZES (4.5% vs. 9.7%, p=0.11). No ST was reported at 60 months.
The FIM study of the myolimus-eluting stent recruited 30 patients half of whom had angiographic follow-up at 6-months, whilst the remaining returned at 12-months. Late lumen loss and percent neointimal volume obstruction were 0.08±0.16mm and 3.2%, and 0.13 ± 0.27 mm and 5.4% at 6- and 12-months, respectively; there was no binary restenosis. Clinical events, assessed at 12-months, demonstrated no mortality or ST; there were however two MIs and two TLRs.
NEVO™ Stent (Cordis, Warren, NJ, USA)
The NEVO™ stent was an open-cell, cobalt chromium stent, with a PLGA biodegradable polymer which facilitated elution of sirolimus. The stent was unique in its design as the polymer and sirolimus were contained within reservoirs, which eliminate the need for a surface polymer coating, and subsequently reduce tissue-polymer contact by over 75%. This stent design was previously used on the durable polymer, paclitaxel-eluting CoStar stent (Conor MedSystems, Palo Alto, CA). Unfortunately despite promising initial results, the CoStar stent failed to develop following disappointing results from the CoStar II study, where it was shown not to be non-inferior to the TAXUS PES with respect to MACE, (CoStar 11.0% vs. PES 6.9%, p=0.005) and angiographic outcomes such as in-stent late loss (CoStar 0.49 mm vs. PES 0.18 mm, p < 0.0001).
The stent was evaluated in the NEVO-RES I study, which was a randomized, multi-center, non-inferiority study comparing the NEVO™ stent to the TAXUS™ Liberté PES stent in 394 patients with single de novo coronary artery lesions. The sirolimus-eluting NEVO stent was found not only to be non-inferior but also superior to PES for the endpoint in-stent late loss (0.13 ± 0.31 vs 0.36 ± 0.46, Pnon-inferiority < 0.001 and Psuperiority < 0.001) and a trend towards lower in-segment binary restenosis (3.9% vs 8.6%, p = 0.08) at 6 month of follow-up (Figure 17, Table 12).
Despite these promising initial results, two factors have led to the withdrawal of the NEVO stent. Firstly stent dislodgements were observed in three patients (all in the NEVO group) during the early phase of ‘all-comers’ NEVO-II study, resulting in the study being stopped. Secondly, and perhaps more importantly, the stent manufacturer, Cordis (Warren, NJ), decided to withdraw from the coronary stent industry at the end of 2011. It seems unlikely that this stent technology will develop further.
The Combo Stent Platform (OrbusNeich, Fort Lauderdale, FL, USA)
The Combo stent is a 100µm thick stainless steel stent covered abluminally with a biodegradable polymer matrix allowing a controlled release of sirolimus. An additional circumferential layer of anti-CD34 antibodies is applied on the stent struts on top of the polymer aiming to accelerate endothelial coverage. Data from histology and OCT at 28 days follow-up in the porcine model indicates that this combination promotes endothelialization, while also reducing neointimal formation and inflammation when compared to the standard SES and Genous EPC stent. Overall, the Combo Stent offers the potential to improve vascular healing whilst still maintaining effective control over neointimal proliferation. The polymer is predictably degraded within 90 days and sirolimus is applied at a dosage of 5µg/mm stent length, which corresponds to approximately half the dose of the Cypher stent platform. The resolution profile however is very similar to the one of the Cypher stent platform. The Combo stent was tested in the REMEDEE trial, an angiographic non-inferiority trial, comparing the in-stent late loss at 6 month between the Combo stent and the Taxus Liberté PES in a total of 183 patients (2:1 randomization). The primary endpoint was met with an in-stent late loss amounting to 0.39 ± 0.45 mm in the Combo as compared to 0.44 ± 0.56 mm in the Taxus Liberté stent group (p non-inferiority= 0.0012). These findings were corroborated in an IVUS sub study. Clinical event rates were low, and no ST was seen out to 5-years. Evaluation of the device in an all-comers population took place in the 1000 patient REMEDEE registry, which report low event rates out to 1-year follow-up. A recent propensity matched analysis between outcomes in patients receiving the Combo stent in the REMEDEE registry, and Promus EES or R-ZES from the Dutch Peers study, showed comparable clinical outcomes out to 2-years.
The EGO-COMBO reported a 9-month late lumen loss of 0.23 ± 0.36 in 61 patients and neointimal regression at OCT follow-up from 9 to 24 months. The rate of MACE beyond 36 months was low (3.28%) and no definite ST occurred.
Results from the randomised HARMONEE study, of the Combo stent versus EES and the REDUCE trial, of 3 versus 12 months of DAPT post Combo stent insertion in ACS patients, are awaited.
The ISAR TEST 4 stent platform
A custom-made stent platform consisting of a mixture of a microporous stainless steel stent coated with sirolimus, a biodegradable polymer and a biocompatible resin widely used in the coating of medical tablets (n=1299) has been compared against two durable polymer DES platforms, the Cypher SES and the Xience V EES (n = 1304) in the ISAR-TEST-4 non-inferiority trial. At 1-year the biodegradable polymer SES was found to be non-inferior for the primary endpoint, a composite of cardiac death, MI, and TLR (13.8% vs. 14.4%, RR 0.96, 95% CI 0.78-1.17, Pnon-inferiority = 0.005, Psuperiority = 0.29). Likewise, there were no differences with respect to cardiac death or MI (6.3% vs 6.2%, p = 0.94), TLR (8.8% vs 9.4%, p = 0.58), and ARC definite or probable ST (1.0% vs 1.5%, p = 0.58). Similar trends were observed at 5-year follow-up with the primary endpoint occurring in 20.5% and 19.5% of patients treated with biodegradable polymer and permanent polymer DES, respectively (p=0.71). Rates of ST were similar with the BP SES and EES but numerically higher with Cypher-SES compared with EES (2.4% vs. 1.4%, p=0.22).
FIREHAWK™ Stent (MicroPort, Shanghai, China)
The FIREHAWK stent is a CoCr stent with abluminal grooves containing a PLA bioabsorbable polymer which releases sirolimus. The safety and feasibility of the stent was confirmed in the TARGET FIM which enrolled 21 patients and showed in-stent late lumen losses of 0.13 ± 0.18 mm and 0.16 ± 0.07 mm at 4- and 13-month respectively. Furthermore, a primary OCT endpoint showed that 96.2% of struts were fully covered at 4-months, whilst low clinical events rates were seen out to 12-months. Following this in the TARGET I study 458 patients were randomised to the FIREHAWK SES (n = 227) or EES (n = 231). The study achieved its primary endpoint of non-inferiority between the FIREHAWK SES and EES with respect to in-stent late loss at 9-month follow-up (0.13 vs. 0.13, Pnon-inferiority < 0.001). Clinical event rates remained low and comparable between both groups with no definite/probable ST events with the FIREHAWK out to 60-months. The 730 patient TARGET II registry also reported low event rates out to 60-months follow-up. The ongoing TARGET All Comers trial (NCT01196819) will test non-inferiority and subsequently superiority of the FIREHAWK SES compared with EES stents in 1656 all-comer patients for the primary endpoint of TLF at 12 months.
MiStent (Micell Technologies, Durham, NC, USA)
The MiStent is a cobalt chromium stent, coated in a PLGA bioabsorbable polymer which degrades over 45-60 days, and elutes sirolimus which is present in a crystalline formulation to facilitate modified release such that the stent’s anti-restenotic drug last three times longer than its polymer. The stent’s FIM study is the DESSOLVE I study which enrolled 30 patients and had a primary endpoint of in-stent late lumen loss. Angiographic and IVUS follow-up demonstrated the stent’s efficacy with an in-stent late lumen loss of 0.08 mm, and a neointimal percentage obstruction of 11.2% at 18-months. No binary restenosis or TLR was seen out to 18-months. Safety has been demonstrated on OCT with a mean strut coverage of >85%, and clinically at 5-years, with low MACE rates and no reported TLF or ST. Further evaluation took place in the DESSOLVE II study, which enrolled 184 patients who were randomised 2:1 between the MiStent (n = 121) and the E- ZES (n = 60). The primary endpoint of the study was met with a significantly lower in-stent late loss at 9-months with the MiStent compared with E-ZES (0.27 mm vs. 0.58 mm, p < 0.001). OCT performed in a selected group of patients showed a very low proportion of uncovered struts in both arms and mean neointimal thickness significantly lower in patients treated with the MiStent. Clinical event rates and ST were low and similar up to 5-year follow-up.
The most robust evaluation of the device took place in multi-centre all-comers DESSOLVE III study which enrolled 1398 patients who were randomised 1:1 to the MiStent (n=703) or Xience EES (n=695). The study met its non-inferiority primary endpoint, a composite of cardiac death, target vessel MI and clinical indicated TLR at 12-months follow-up, with rates of 5.8% for MiStent and 6.5% EES (Pnon-inferiority<0.001). No significant differences were observed in rates of the individual clinical endpoints, including ST.
Svelte (Svelte Medical Systems, New Providence, NJ, USA)
The Svelte is a sirolimus-eluting cobalt chromium stent, which has a combined PLGA and amino acid based coating which is highly biocompatible, non-thrombogenic, non-inflammatory and fully bioresorbable over 12-months. Data confirm that tissue concentrations are similar to the Cypher SES, with the drug elution pattern comparable to both Cypher SES and Xience EES. The stent has been designed to reduce procedural time and overall costs. This is achieved by the stent being designed for direct stenting owing to it being pre-mounted on a 0.012-inch flexible coil guidewire; hence no additional guidewire is required. The stent balloon also has distinct features including two balloon control bands located on the proximal and distal balloon shoulders which are designed to facilitate smooth stent delivery; focus pressure under the stent for controlled stent deployment; and minimise longitudinal balloon growth and contact with the vessel wall. The balloons also have a lower compliance enabling higher-pressure inflations, which is important given the inability to pre-dilate the lesion.
The first clinical assessment of the stent took place in the DIRECT FIM study, which enrolled 30 patients and had a primary safety endpoint of angiographic TVF, and a primary efficacy endpoint of in-stent late loss. There was one device failure. Angiographic, IVUS and OCT follow-up reported an in-stent late lumen loss of 0.22 mm; a neointimal percentage obstruction of 2.7%; and 97.9% strut coverage at 6-months, respectively. There was one binary restenosis, one angiographically driven TLR and no reported cardiac death, MI or ST at 60-months.
The DIRECT II trial randomised 159 patients 2:1 to Svelte or R-ZES the 6-month lumen loss showed non-inferiority of the Svelte stent to the R-ZES stent (0.09mm vs. 0.13mm, Pnon-inferiority<0.0001). Similar clinical outcomes were reported for both groups and no ST occurred.
Orsiro stent (Biotronik, Germany)
The Orsiro SES is a cobalt chromium stent with ultrathin struts (60 or 80 µm) whose surface is fully coated with a layer of an amorphous hydrogen-rich silicon carbide, which acts as a diffusion barrier sealing the underlying bare metal surface and reducing ion release by up to 96%. The components of this silicon carbide include: silicon carbide, a ceramic material, carbon and a chemical compound of silicon. Overlying this is a PLLA polymer that elutes sirolimus over a period of approximately 100 days. The polymer matrix has an asymmetric design that allows for the release of a greater drug dose on the abluminal than luminal side. The clinical trial program has been robust comparing this second-generation biodegradable polymer DES with second-generation durable polymer DESs, and more recently, in the first of its kind, with other biodegradable polymer DESs.
The FIM study was the BIOFLOW-I which enrolled 30 patients, and reported a primary endpoint of in-stent late loss of 0.05 mm at 9-months. The 12-month MACE rate was 10% owing to one cardiac death, and two ischaemia driven TLRs. Further assessment took place in the multi-center BIOFLOW-II study, which randomised 452 stable patients to treatment with the Orsiro stent (n = 298) and Xience EES (n = 154). The study achieved its non-inferiority primary endpoint of in-stent late loss at 9-months (0.10±0.32mm vs. 0.11±0.29mm, Pnon-inferiority < 0.0001). Clinical event rates were low and comparable between both devices at one year: rates of the device-oriented endpoint, TLF, were 6.5% in the Orsiro arm vs. 8.0% in patients treated with XIENCE (p=0.58). These findings were confirmed at 24 months in the overall population and also in diabetic and small vessel cohorts. Neointimal thickness assessed by OCT in a subgroup of patients was similar without differences in terms of uncovered or malapposed struts were recorded. The potent inhibitory effect on neointimal hyperplasia did not appear to affect arterial healing as no case of ST occurred in either group at one year whilst only one patient in the XIENCE arm experienced a possible very late ST.
In the randomized ORIENT study the Orsiro SES was shown to be non-inferior in terms of in-stent late lumen loss at 9-months compared to R-ZES (median 0.06 mm vs. 0.12 mm; Pnon-inferiority<0.001; Psuperiority=0.21). Angiographic restenosis was significantly lower with Orsiro (15% vs. 20%, p=0.002), whilst adverse clinical outcomes were low in both groups.
In the BIOSCIENCE trial 2119 patients with minimal exclusion criteria, were randomly assigned to receive the Orsiro stent (n=1063) or the XIENCE EES (n=1056). At 12 months, the comparable rate of the combined safety and efficacy primary endpoint proved the non-inferiority of the Orsiro stent compared with XIENCE. No significant differences were reported in rates of ST. Clinical outcomes continued to be similar between groups at 2-years follow-up in the full cohort and the pre-specified diabetic sub-group. Randomisation was stratified according to patients presenting with or without an ST-elevation MI, and results from this sub-group identified a significant interaction between the device and the treatment effect.
The all-comers SORT OUT VII study was the first randomised study to compare the performance of two biodegradable polymer DES–Orsiro SES (n=1261) and Nobori-BES (n=1264). At 1-year the primary endpoint of TLF occurred in 3.8% and 4.6% of patients treated with Orsiro and Nobori, respectively, achieving the pre-specific criterion for non-inferiority (Pnon-inferiority<0.001). Overall clinical event rates were low with no between-stent differences in any clinical endpoints other than definite ST, which was significantly lower with Orsiro (0.4% vs. 1.2%, p=0.034) and driven by lower rates of sub-acute definite ST (0.1% vs. 0.6%, p=0.05). The study was not powered for ST and therefore the variances in ST should only be regarding as hypothesis generating. Notwithstanding this, these differences may be result of the different stent designs between these two generations of biodegradable polymer DES which includes, amongst others, their differing strut thickness and polymer degradation time.
The all-comers BIO-RESORT (TWENTE III) trial was a multicentre double-blinded trial, which randomised 3,514 patients to Orsiro (n=1,169), Synergy EES (Boston Scientific, Natick, MA, n=1,172) and R-ZES (n=1,173). The study’s two independent hypotheses were that Orsiro and Synergy would have non-inferior rates of TVF, a composite of cardiac death, target vessel MI and clinically indicated TVR at 12-months, when compared separately with R-ZES. Despite >70% of study population having acute coronary syndromes the event rate was lower than expected. At 12-months the primary endpoint of TVF occurred in 4.7% and 5.4% of patients receiving Orsiro and R-ZES, respectively (HR 0.87, Pnon-inferiority<0.001). There were no significant differences in the components of TVF or ST.
The BIOFLOW V randomized in a 2:1 ratio a total of 1334 patients to undergo PCI with the Orsiro SES or the Xience EES. The primary endpoint of TLF was significantly reduced among patients allocated to the Orsiro SES (6% vs. 10%, p=0.0399) due mainly to a lower occurrence of target-vessel MI in the experimental arm (5% vs. 8%, p=0.0155).
Ultimaster stent (Terumo Corporation, Tokyo, Japan)
The Ultimaster stent is made of a cobalt-chromium bare metal platform with thin struts (80 µm) and open cell design and a biodegradable polymer (poly-DL-lactic acid –PDLLA- and polycaprolactone co-polymer) applied to the abluminal side only. The polymer elutes sirolimus drug (3.9 µg/mm stent length) and degrades during a period of 3-4 months. A peculiar aspect of this device is a gradient coating consisting of a lack of drug polymer on the stent areas experiencing the highest physical stress with the aim to reduce the risk of polymer cracking and delamination. In the randomized CENTURY II trial, it showed a safety and efficacy profile similar to a DP EES (Xience). In a population of 1123 patients with broad inclusion criteria, freedom from TLF (a composite of cardiac death, target vessel MI and TLR) was 95.6% in the BP-SES group and 95.1% in the DP-EES group (Pnon-inferiority<0.0001) at 9-month follow-up. A comparable short-term safety profile was also noted with non-significant differences in rates of cardiac death, MI and ST. At 3 years follow up from CENTURY II, there was no difference between the Ultimaster and Xience in clinical outcomes and ST.
Tivoli stent (EssenTech, Beijing, China)
The Tivoli stent is an open cell, balloon expandable, cobalt-chromium stent (80 µm) coated with a biodegradable polymer (PLGA) containing sirolimus at a dose of 8 µg per mm of stent length. Most of the drug (75%) is released in 28 days. It proved to be non-inferior for the occurrence of efficacy primary endpoint at 12 months compared with a DP sirolimus-eluting stent sharing the same cobalt-chromium platform, the FIREBIRD 2 stent (MicroPort, Shanghai, China) in the randomized I-LOVE-IT-2 trial.
BioMime stent (Meril Life Sciences, Gujarat India)
The BioMime SES stent has a cobalt chromium ultra-thin (65 µ) platform and a hybrid cell design that is coated in a combined PLGA and PLLA biodegradable polymer. The initial clinical assessment took place in the Merit-I study, which enrolled 28 patients, and reported an in-stent late loss of 0.15mm at 8-months angiographic follow-up. There were no clinical events out to 2-years. Following this was the Merit-2 study, which recruited 242 more complex patients, who had an in-stent late loss of 0.13 mm at 8-months. The rate of MACE was 6.2% at 1-year as a result of 2 cardiac deaths, 3 non-fatal MIs and 10 clinically-driven TLRs. Furthermore 3 STs were seen.. Randomized comparisons with EES are ongoing (meriT4, meriT5, merit China).
Inspiron stent (Scitech, Sao Paulo, Brazil)
The Inspiron has a cobalt chromium platform coated in an abluminal PLA and PLGA polymer and elutes a low dose of sirolimus (56µg). Initial clinical evaluation took place in the INSPIRON I trial, which randomised 58 patients 2:1 to treatment with the Inspiron stent (n = 39) or a BMS control (n = 19) The study achieved its primary endpoint with a significantly lower in-segment late loss with the Inspiron stent compared to the controls (0.19 vs. 0.58, p <0.001). In-stent late loss and percent neointimal obstruction were also both significantly lower with the Inspiron SES. MACE rates at 12-motnhs were comparable, whilst no TLR was seen with the SES out to a median of 878 days. In the multi-center DESTINY trial including 170 patients, the Inspiron stent was non-inferior to the Biomatrix Flex stent for the 9-months in stent lumen loss (0.20 vs. 0.15, Pnon-inferiority <0.001). IVUS and OCT findings showed a slightly higher neointimal hyperplasia and strut coverage compared with the Biomatrix stent, respectively.inspiro
SYNERGY stent (Boston Scientific, Natick, MA, USA)
The SYNERGY stent utilises the same PtCr alloy and stent design as the Element stent platform, however the stent is coated in an abluminal ultrathin rollcoat bioerodable polylactic-co-glycolic acid polymer that elutes everolimus. Drug release profiles and tissue concentrations are similar to the PROMUS Element stent. The safety and performance of the stent was assessed in the single-blind randomised, non-inferiority EVOLVE trial, which enrolled 291 patients in 29 sites in Europe, Australia, and New Zealand. The trial compared two doses of everolimus (PROMUS-like, 113 µg/20 mm stent; and half-PROMUS, 56 µg/20 mm stent) on the SYNERGY stent to the Promus EES stent in patients with a single de novo native coronary artery lesion. At 6-months both SYNERGY stents were shown to be non-inferior to the Promus EES with respect to the primary angiographic endpoint of late loss (Standard dose 0.10 mm vs. Low dose 0.13 mm vs. EES 0.15, Pnon-inferiority < 0.001). In addition, rates of the primary clinical endpoint of TLF, a composite of cardiac death, MI, and TLR at 30 days were comparable between stents (1.1% vs. 3.1% vs. 0.0%, p = NS), with results maintained out to 60-months.
In the EVOLVE II trial, 1684 patients scheduled for PCI due to stable CAD or Non-ST segment elevation MI were randomly assigned to receive either the SYNERGY stent or the PROMUS EES. Comparable rates of the primary composite endpoint, TLF at 12-month (6.7% vs. 6.5%, p=0.83 for difference) demonstrated the non-inferiority of the SYNERGY stent (Pnon-inferiority =0.0005). Rates of the individual components of TLF were similar for both study arms: cardiac death (0.5% vs. 0.9%, p= 0.34), MI (5.4% vs. 5.0%, p= 0.68), clinically indicated TLR (2.6% vs. 1.7%, p= 0.21). Comparable clinical safety was established in view of a similar rate of ST (0.4% vs. 0.6%, p= 0.50). At 2 years, rates of TLF were 9.4% in the SYNERGY groups vs 8.5% in the PROMUS EES (p=0.57). Three-year follow up data support long term safety and efficacy of the SYNERGY stent with a 0.2% probable ST rate in the SYNERGY group versus 0.7% in the PROMUS EES (p=0.15). On the basis of the results from this study, the SYNERGY stent received FDA approval, and became the first biodegradable polymer DES available in the US.
As mentioned previously two arms of the BIO-RESORT (TWENTE III) trial included patients randomised to Synergy EES (n=1,172) or R-ZES (n=1,173), and at 12-months, as with Orsiro, the Synergy EES was shown to be non-inferior to R-ZES for TVF (Synergy 4.7% vs. R-ZES 5.4%, HR 0.87, Pnon-inferiority<0.001). As in the other arm of the study there were no significant differences in the components of TVF or ST.
Stefanini et al reported a patient level meta-analysis of three randomised studies (LEADERS, ISAR TEST 3, ISAR TEST 4) of biodegradable polymer stents (n = 2358) versus early-generation - SES (n=1704). At 4-years rates of TLR (HR 0.82, p = 0.03), and definite ST (HR 0.56, p = 0.02) were significantly lower in the biodegradable polymer group compared with the durable polymer group. Therefore, biodegradable polymer DES provide better efficacy and safety outcomes when compared with early-generation DES. Collectively, data from randomised trials suggest similar efficacy and safety outcomes between biodegradable and durable polymer new-generation DES. However, a direct comparison in the SORT OUT VII indicated that biodegradable polymer DES with thinner struts may be associated with a lower risk of ST compared with relatively thicker biodegradable polymer DES during the early period after PCI. This finding has been also confirmed by a large network meta-analysis accounting also for indirect evidence.
Non-polymeric DES offer the potential advantages of avoiding the long-term adverse effects of a polymer, improved healing, and an improvement to the integrity of the stent’s surface. The physical properties of these polymer-free stents and angiographic follow-up results from FIM studies or randomized trials are summarized in Table 13, , and late loss figures are provided in Figure 18. Overall robust clinical studies that confirm the improvements in clinical safety hypothesised by their design are currently lacking.
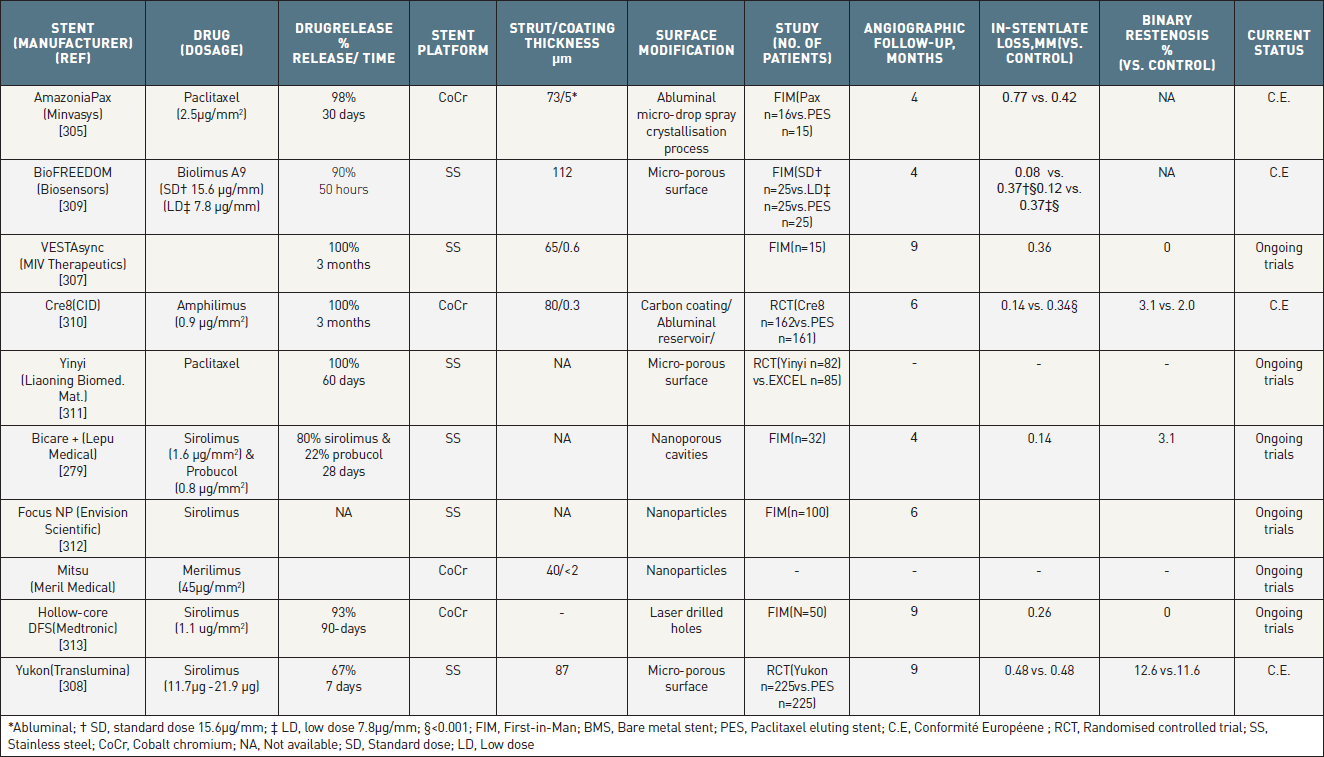
Polymer Free Metallic stents which are either currently available outside the USA, or undergoing clinical evaluation.
All differences are not significant unless stated.
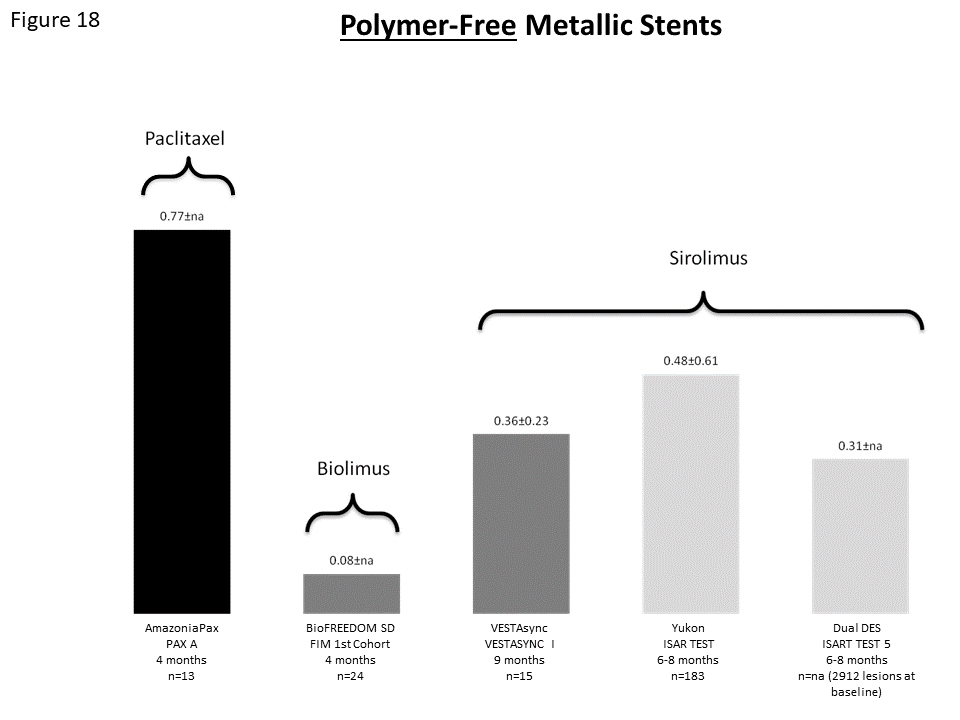
Late lumen loss of different polymer-free stent platforms.
The stainless steel YUKON SES (Translumina, Germany) was the first and the most extensively studied polymer-free DES. The stent has a micro-porous surface, with pores that are 2 µm deep and effectively function as a drug reservoir removing the need for a polymer. Uniquely the dose of sirolimus is customized in the cath lab, just prior to stent implantation, in a coating process taking approximately eight minutes (Figure 19). Initial studies have established that the optimal concentration of rapamycin to prevent restenosis is 2%.
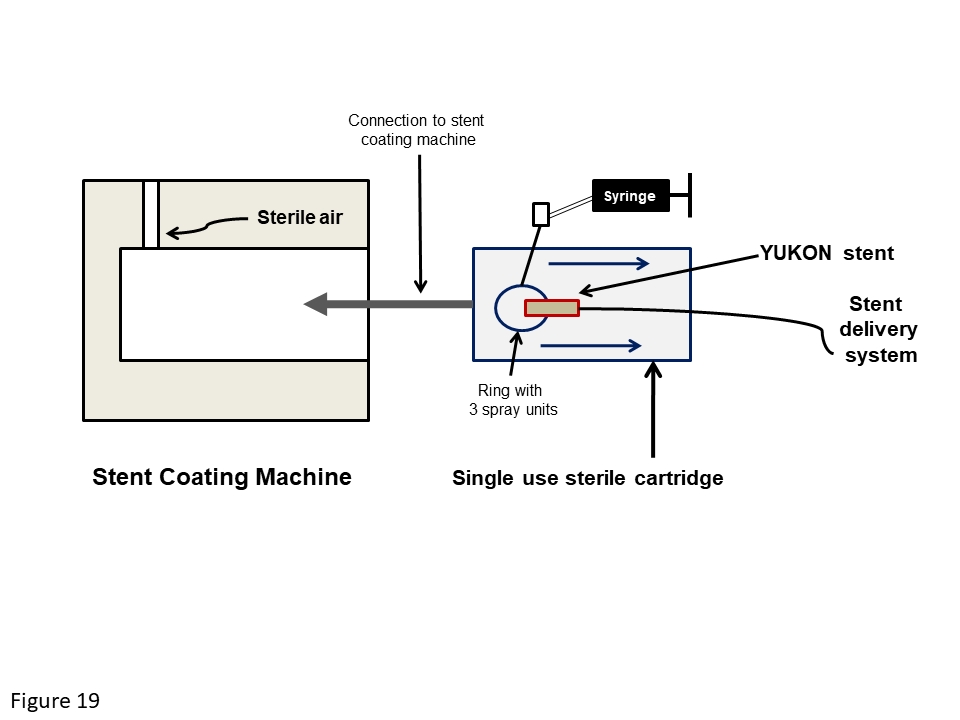
Schematic diagram of the YUKON stent coating machine. The stent is inserted into a sterile single-use cartridge which is placed in the stent coating machine. The syringe is used to inject the antiproliferative drug, which is sprayed uniformly over the stent using 3 spray units. Following the spray coating, the stent is dried using sterile pressurized air.
After complete drug release the remaining micro-porous surface appears to favour the adhesion of endothelial cells, a hypothesis initially suggested by angiographic follow-up data, and subsequently confirmed by OCT, which has demonstrated significantly greater neointimal thickening, and stent strut coverage with the YUKON stent compared to SES at 3-months follow-up. Clinical studies including both registry and randomized data demonstrate non-inferiority of a YUKON stent eluting 2% rapamycin when compared with PES out to 1-year follow-up (Figure 18, Table 13). In the randomised ISAR-TEST study comparable rates of TLR (YUKON 16.5% vs. PES 16.4%, p = 0.89), death/MI (16.6% vs. 20.0%, p = 0.52), MACE (27.3% vs. 31.7%, p = 0.40) and ST have been seen (0.5% vs. 1.6%, p = 0.32) out to 5-year follow-up.
Observational data extending out to 2-year follow-up have indicated that the YUKON stent may be less susceptible to delayed restenosis when compared to conventional DES. Byrne et al reported a significantly lower change in late loss between 6-8 months and 2 years for the YUKON stent, when compared with durable polymer based SES and PES (YUKON 0.01±0.42 mm, SES 0.17 ± 0.50 mm, and PES 0.13 ± 0.50mm, p < 0.001). This finding has also been observed during similar 2-year follow-up of the ISAR-TEST 2 and ISAR-TEST 3 studies, both of which randomized patients to treatment with polymer free SESs, or either conventional polymer or biodegradable polymer DES. Collectively these results suggest that polymer-free DES may not be subject to the “late-catch” phenomena which have been reported with durable polymer DES, and appears to be worse in those stents eluting macrocylic lactone derived anti-proliferative coatings.
The polymer-free biolimus-eluting BioFreedom stent (BES-PF, Biosensors International PTE LTD, Singapore) is made of stainless steel with a strut thickness of 112 µm and a micro-structured, polymer-free abluminal surface (Figure 6). The investigation of drug release kinetics revealed that >90% of drug is released within 50 hours with biolimus detectable in neointima and myocardium surrounding stent struts at 28 days. Pre-clinical studies of BES-PF provide support for the concept of polymer-free DES. In a porcine model Tada et al demonstrated comparable early, and more durable long-term, efficacy between BES-PF and a durable polymer SES. Furthermore, at 180-days compared with SES, BES-PF use was associated with decreased fibirn, and less inflammation suggesting superior arterial healing.
Clinical assessment of this BES-PF has taken place in the BioFreedom FIM study which randomised patients to treatment with either BES-PF with standard dose biolimus (15.6 µg/mm stent length), BES-PF with low dose biolimus (7.8 µg/mm stent length) or Taxus Liberté PES. In total 182 patients were enrolled, 75 into the first cohort which had a primary endpoint of in-stent late loss at 4-months; with the remaining 107 patients entering into the second cohort which had a primary endpoint of in-stent late loss at 12-months. The first cohort achieved its primary endpoint with late loss significantly reduced in both BES-PF with standard dose (late loss 0.08 mm) and BES-PF with low dose (late loss 0.12 mm) at 4 months compared with Taxus Liberté (0.37 mm, both p < 0.001) (Figure 20, Table 13). The IVUS results confirmed the angiographic findings with a lower neointimal volume obstruction in the BES-PF standard dose (1.3%) compared to both BES-PF low dose (5.5%, p = 0.003) and PES (6.6%, p = 0.0003).
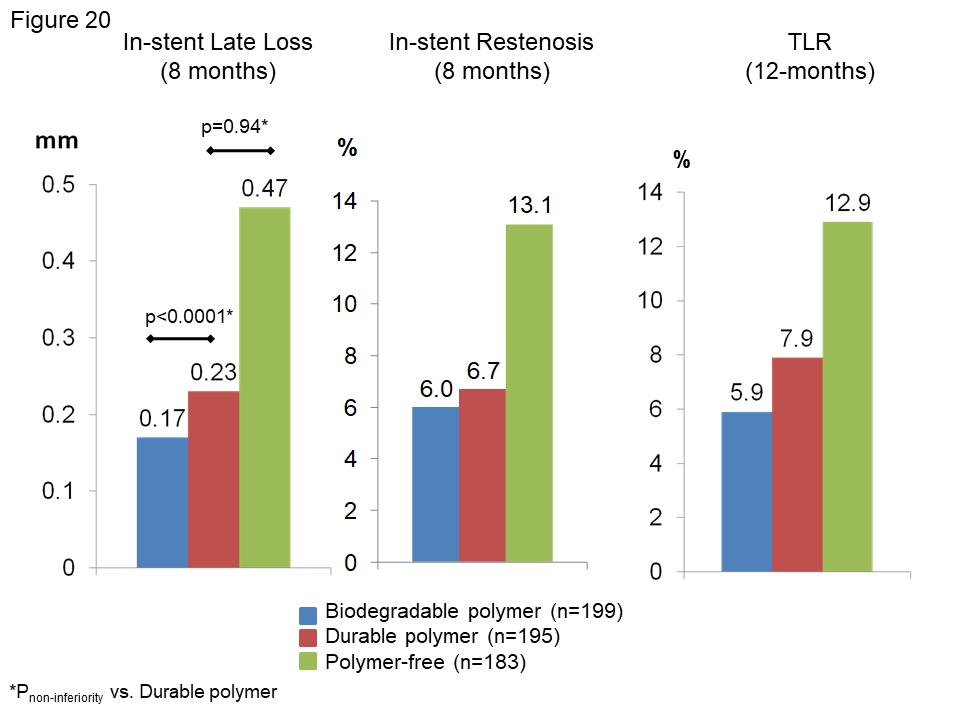
Results of the ISAR-TEST 3 study. Patients were treated with three different sirolimus-eluting stent platforms: the durable polymer (red), biodegradable polymer (blue) or polymer-free (green).
Similarly, the second cohort also achieved its primary endpoint of non-inferiority for in-stent late loss with respective median late loss values for the standard dose BES-PF, low dose BES-PF, and TAXUS PES of 0.17mm, 0.22mm, and 0.35mm (standard dose vs. TAXUS Pnon-inferiority < 0.001 and Psuperoirty = 0.11, low dose vs. TAXUS Pnon-inferiority < 0.21). At 5 years, clinical event rates were similar, with no ST observed in any group.
Further evaluation of the BES-PF took place in the LEADERS FREE study, a randomised double blind study, which aimed to assess whether the rapid elution of biolimus in the absence of a polymer would offer a safety advantage over BMS in those patients requiring the efficacy of a DES, but who were unable to take prolonged DAPT. The LEADERS FREE study enrolled 2466 patients, who due to co-morbidity, or a high-risk of bleeding (including age >75 in 64% patients), were unable to take DAPT beyond one-month, and randomised them to receive either the BES-BF or a BMS. The study had two 1-year primary endpoints: a non-inferior safety composite of cardiac death, MI and ST; and a superiority efficacy endpoint of clinically driven TLR. The primary safety endpoint occurred in 112 patients (9.4%) in the BES-PF group and in 154 patients (12.9%) in the BMS group (Pnon-inferiority < 0.001 and Psuperiority=0.005) at 390 days. Clinically driven TVR occurred in 59 patients (5.1%) in the drug coated stent group and in 113 patients (9.8%) in the BES-PF and BMS groups, respectively (p< 0.001). Results at 2-years showed that BES-PF continued to remain both significantly safer and more effective than BMS in high bleeding risk patients treated with a one month only DAPT course.
Observation data assessing the efficacy and safety of the stent in an all-comer’s population are available from the 1103 patients enrolled in the RUDI-FREE registry. Clinical outcomes at 12 months confirmed device safety and efficacy, with as expected, significantly higher event rates in patients with high as opposed to non-high bleeding risk. Notably, the device’s performance in high-bleeding risk patients was comparable to those reported in the LEADERS-FREE study, whilst its performance in non-high bleeding risk patients was comparable to contemporary DES.
The VESTAsyn SES (MIV Therapeutics, Atlanta, GA) is a polymer free stainless stent which has a nano-thin, micro-porous, hydroxyapatite surface coating impregnated with 55µg dose of sirolimus. Sirolimus is eluted over 90-days, whilst the hydroxyapatite remains stable over the first 4-months, before completely dissolving around 9-12 months after stent implantation. Pre-clinical studies indicate that the low dose of sirolimus, which is made possible by the hydroxyapatite platform, results in reduced signs of delayed vascular healing, suggesting less local toxicity, and a faster healing response.
Primary evaluation of the stent took place in the 15 patients VESTAsync I FIM study (Figure 18, Table 13). At 4- and 9-months angiographic follow-up effective reductions in late loss and intimal hyperplasia were observed, with no evidence of ‘late-catch’ seen on quantitative coronary angiography (QCA) or IVUS. Out to three year follow-up the only clinic event was a single TLR.
Further assessment is on-going in the VESTAsyncII study which has randomised 75 patients in a 2:1 ration to either the VESTAsyn SES (n = 50) or the Gen X stent, a control BMS with a microporous hydroxyapatite surface coating. The in-stent late loss at 8-months follow-up was 0.39±0.20mm and 0.74±0.52mm in VESTAsyn SES and BMS respectively (p=0.03), such the study achieved its primary endpoint. In addition, IVUS demonstrated significantly less neointimal hyperplasia with the VESTAsynSES stent (15.4mm3 vs. 29.4mm3, p=0.01). Clinical event rates out to 2-years were low, with 3 and 5 MACE events in the VESTAsyn SES group (1 death, 1 MI, 1 TLR) and BMS (2 deaths, 1 MI and 2 TLRs) respectively; there were no ST events.
The Amazonia Pax (Minvasys, Genevilliers, France) stent is the only polymer free stent that is made of cobalt chromium, and elutes paclitaxel. The stent has an open cell design, with 73µm thick struts, which are coated with a 5µm thick abluminal coating of polymer free paclitaxel at a dose of 2.5 µg/mm2. The pure paclitaxel is applied using a micro-drop spray crystallization process. This consistent coating ensures that 98% of the drug is eluted within 30 days, and ensures that by 45 days all that remains is a bare metal cobalt chromium stent.
The multicenter Pax A study randomized 30 patients to treatment with either the Amazonia stent or the TAXUS PES (Figure 18, Table 13). At 4-months the respective in-stent late lumen loss and %neointimal volume obstruction for the Amazonia and PES were 0.77mm versus 0.42mm (p = 0.20), and 19% versus 6% (p = 0.08). OCT analysis demonstrated significantly more stent strut coverage with the Amazonia stent compared with PES. Clinically at 2-years there were no deaths or ST events; however four patients treated with PES had a TLR, whilst two patient in the Amazonia arm had an MI, and two had a TLR.
The Cre8 stent is a polymer free stent which releases sirolimus through the use of abluminal reservoir technology such that drug elution is completed in 90 days. The stent uses an Amphilimus formulation –sirolimus formulated with a mixture of long chain fatty acids which enhances drug stability, facilitates sustained drug elution timing and modulates drug bioavailability. Uniquely the bare metal stent struts are coated in a second generation pure carbon coating which has a crystalline structure close to diamonds and provides excellent bio- and haemo-compatibiltity. Pre-clinical data indicate the absence of a chronic inflammatory response with the Cre8 stent as evidenced by reduced inflammatory scores and neointimal thickness in porcine models when compared to controls comprising of the same stent platform without the carbon coating and the Cypher SES. Consistent with this are the results from the Demonstr8 OCT study which reported that strut coverage was non-inferior between the Cre8 stent at 3-months and a BMS at 1-month.
The first clinical study was the multicentre prospective NEXT trial which randomised 323 patients to Cre8 stent (n = 162) and the TAXUS PES (n = 161). The study achieved its primary endpoint by demonstrating non-inferiority of the Cre8 stent with regards to in-stent late loss at 6-months (Cre8 0.14±0.36mm vs. PES 0.34±0.40mm, Pnon-inferiority < 0.0001, Psuperiority < 0.0001). The occurrence of MACE (cardiac death, all MI, all TLR) was similar in both groups (8.3% vs. 10.1%, p=0.59)
The multi-centre, all-comer’s pARTicip8 registry enrolled 1186 patients treated with Cre8 stent and reported low rates of ST, device-oriented MACE and TLR at 1-year follow-up in the entire population, and a pre-specified diabetic sub-group. The latter group also underwent 6-month angiographic follow-up, with a reported late lumen loss of 0.16mm. Specific assessment of the Cre8 stent’s performance in diabetic patient took place in the RESERVOIR study, which randomised 112 patients to the Cre8 stent (n=56) or EES (n=56). The study met its primary endpoint of %neointimal volume obstruction as assessed by OCT at 9-month follow up (Cre8 11.97+/- 5.94% vs. EES 16.11 +/- 18.18%, Pnon-inferiority=0.0003, Psuperority=0.22).
The ASTUTE registry has suggested that the Cre8 stent can be used safely in patients needing a short duration of DAPT (<3 months). The study reported comparable rates of 1-year TVF between the 106 patients receiving <3 months DAPT (5.7%) and the 1102 patients receiving >6 months (5.1%). BARC defined major bleeding was significantly higher in the short DAPT group (3.4% vs. 0.2%, p=0.007), however this difference was not observed following a landmark analysis at 90-days (0% vs. 0.3%).
Further trials of the Cre8 stent are on-going and include the EFFICACY study in diabetic patients, and the ReCre8 study which will randomise 1530 all-comers patients to Cre8 stent or R-ZES with DAPT given for 1-month (stable angina) or 12-months (ACS).
The FOCUS np DES system (Envision Scientific, Surat, India) is a DES using nanotechnology. The potential benefits of using this concept on a DES is to enhance long-term safety, improve stent efficacy, and reduce the long-term requirement for DAPT. These stents have a standard stent platform, with a nanomatrix coating, made up of nano-particles of an anti-proliferative drug combined with one or more stabilising excipients; this matrix functions as a substitute for the polymer. There are many advantages of using nanoparticles for drug-delivery: (i) they enable controlled and reproducible drug release kinetics; (ii) they increase drug stability in vivo because of the encapsulation process; (iii) they are able to penetrate deeper into the vessel wall thereby improving efficacy; (iv) they facilitate rapid release of drug into the tissue, with a drug depot or reservoir effect, which enables the stent to become drug-free in a short period of time, leading to more rapid healing; (v) they allow increased intra-cellular uptake of drug, with a prolonged residence time at site; (vi) they permit a lower overall drug dosage; and (viii) they increase bio-availability at the target site.
The FOCUS np polymer-free stent has a cobalt chromium stent platform, and is coated with nano-particles containing sirolimus within two excipients, which were selected to create a two phase programmed drug release. The first phase is a burst release from the top layer of nano-particles occurring within 60 seconds of stent deployment; whilst the second phase is a programmed release from the bottom layer. Drug delivery is completed in 28-days. Uniquely the stent balloon shoulders are also coated in the nanomatrix to allow delivery of drug at edges of the stent to avoid edge restenosis. Following successful pre-clinical studies, the Nano ActiveFIM- IN study has completed enrolment of 83 patients divided in cohort A (n= 55, simple lesions) and B (n=28, real world scenario). Data from 6-month and 1-year follow-up are expected.
These novel polymer-free DES have 81mm struts made from a tri-layer wire:
Sirolimus is released through an average of six laser-drilled holes on the abluminal side of each stent, each with a minimal bore diameter of 20μm (∼1,800 holes for an 18 mm stent) Drug elution commences on stent deployment and is controlled and sustained through natural diffusions via direct interaction with the vessel wall. Pre-clinical data show 68% and 93% of the sirolimus is released by 28- and 90-days respectively, with histology confirming that this drug release is effective at suppressing neointimal hyperplasia compared to BMS controls (P<0.001), with minimal inflammation. The FIM RevElution clinical trial is currently being conducted, and 9-month results from the first cohort of 50 patients are encouraging with a late loss of 0.26mm which is non-inferior to R-ZES historical controls (Pnon-inferior<0.001), a 0% binary restenosis rate, and signs of rapid early healing with >98% stent strut coverage and 0% late incomplete malapposition. At 12-months clinical follow-up, two patients had had experienced a cardiovascular event leading to a target vessel non-Q-wave MI, and a TLR; no ST was seen.
The ISAR-TEST 3 trial is currently the only comparison of three stents with different types of polymer and the same anti-proliferative drug - sirolimus. This non-inferiority study randomized 605 patients to SES with either a durable polymer (202 patients), a biodegradable polymer (202 patients), or a stent that was polymer free (201 patients). At 6-8 months angiographic follow-up the biodegradable polymer stent met its pre-specified criterion for non-inferiority in terms of in-stent late lumen loss (0.23 mm vs. durable polymer 0.17 mm, Pnon-inferiority < 0.001); whilst the polymer free stent failed to achieve non-inferiority (0.47 mm vs. 0.17 mm, Pnon-inferiority = 0.94) (Figure 20). Despite these results, clinical outcomes at 1-year demonstrated a similar safety profile for the three stents; however, efficacy appeared numerically inferior with the polymer free stent, and comparable between the biodegradable and durable polymer stents. At 2-years follow-up, clinical outcomes remained comparable in terms of rates of mortality, MI, and ST. The rate of TLR was also comparable between all three stents, however the absolute increase in TLR between 1- and 2-year follow-up was notably higher with the biodegradable polymer and durable polymer stents, when compared to the polymer free stent (∆2.5% vs. ∆2.5% vs. 0.5%). Paired angiographic follow-up was available in 69% of patients, and demonstrated a delayed in-stent late lumen loss of 0.17 mm, 0.16 mm and -0.01 mm for biodegradable polymer, durable polymer and polymer-free stents, respectively (p < 0.001). Importantly, these results indicate that not only are biodegradable polymer stents still susceptible to the delayed restenosis observed previously with durable polymer stents, but they also indicate that polymer free stents are potentially less prone to this unwanted long-term phenomenon. This observation is consistent with that previously reported by Byrne et al, and warrants additional investigation.
The failure of polymer-free stents to demonstrate non-inferiority compared to durable polymer stents in the ISAR-TEST 3 study prompted interest in dual drug-eluting polymer-free (Dual-PF) stents. This approach, which aims at improving the anti-restenotic performance of polymer-free stents through the use of a second anti-proliferative agent which targets a different part of the cell-cycle, was evaluated in the ISAR-TEST 2 and ISAR-TEST 5 study.
The ISAR-TEST 2 study randomized 1007 patients to treatment with SES (n = 335), ZES (n = 339) or a Dual-PF stent (n = 333), that eluted sirolimus and the anti-oxidant probucol which has previously been shown to reduce neointimal hyperplasia. The rate of the primary endpoint of binary restenosis at 6-8months follow-up was Dual-PF 11.0%, ZES 19.3% (p < 0.001 vs. Dual-PF), and SES 12.0% (p = 0.68 vs. Dual PF). Clinical outcomes at 1-year follow-up demonstrated comparable safety in terms of mortality, MI and ST between the three stents, however rates of TLR were significantly lower with the Dual-PF compared to ZES (Dual-PF 6.8% vs. ZES 13.6%, p = 0.001), and comparable with SES (Dual-PF 6.8% vs. SES 7.2%, p = 0.83).
At 2-years follow-up, safety clinical outcomes remained comparable amongst the three groups. Similar to the 1-year results, rates of TLR were significantly lower with Dual-PF compared to ZES (p = 0.006), and comparable between Dual-PF and SES. Moreover, as seen in the ISAR-TEST 3, the absolute increase in TLR between 1- and 2-year follow-up was notably higher with the durable polymer SES compared to the Dual-PF SES (∆3.5% vs. ∆0.9%, p = 0.009). Likewise paired angiographic follow-up demonstrated a significantly greater increase in in-stent binary restenosis with the durable SES compared to the Dual-PF SES (∆6.6% vs. ∆2.9%, p = 0.002). Overall this study demonstrated that Dual-PF DES offer a reduction in delayed restenosis compared to 1st generation DES, whilst maintaining a comparable safety profile. Importantly this reduction in delayed restenosis with the polymer free stent, is consistent with other studies such as ISAR-TEST, and ISAR-TEST 3, suggesting these stents may hold promise for the future.
Similarly, and as described earlier, the ISAR-TEST 5 study also demonstrated that the polymer-free sirolimus and probucol-eluting stent was non-inferior to R-ZES out to 12-months.
The physical properties of these stents with novel coatings, together with angiographic follow-up results from FIM studies or randomized trials are summarized in Table 14.
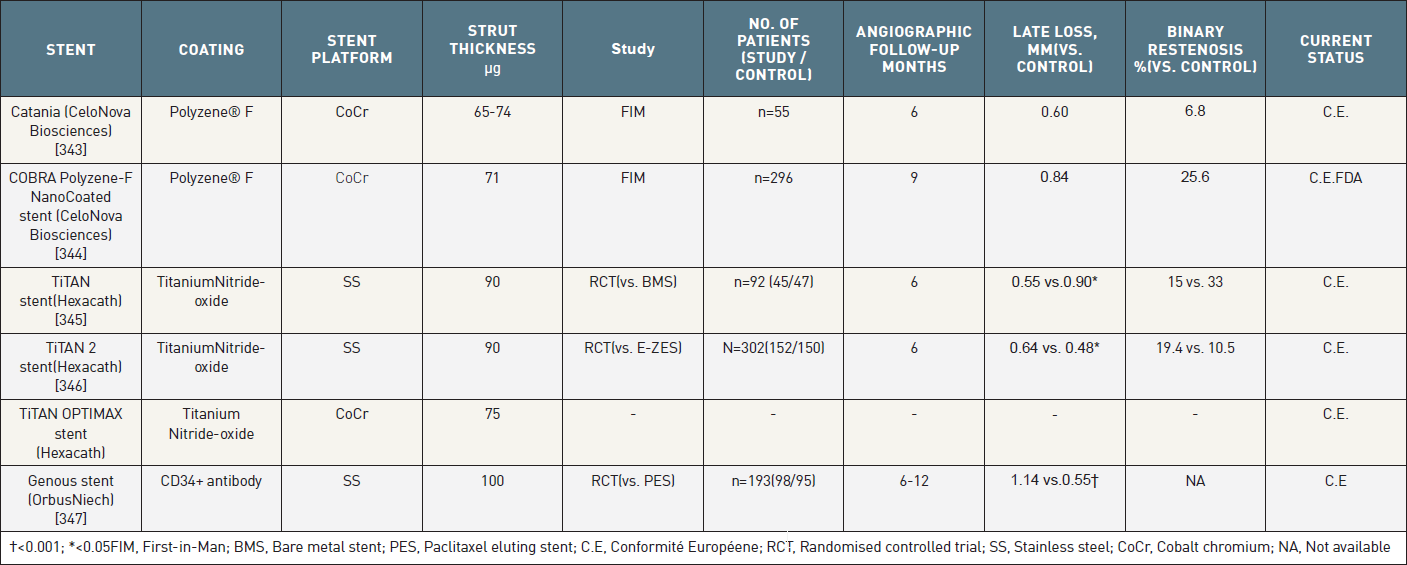
Metallic stents with novel coatings which are either currently available outside the USA, or undergoing clinical evaluation.
All differences are not significant unless stated.
Polyzene F is a biocompatible, biostatic, proprietary formulation of poly[bis(trifluoro-ethoxy)phosphazene], which has anti-inflammatory, bacteria-resistant and pro-healing qualities. Its application onto a stent was therefore proposed as a method of creating very low surface thrombogenecity, thereby potentially reducing the risk of ST. Pre-clinical studies have demonstrated reduced inflammation, neointimal hyperplasia, and thrombogenicity with stents coated with Polyzene F compared to uncoated stents. Subsequently two commercial stents have been developed by applying a 40nm thick layer of Polyzene F onto the surface of cobalt chromium struts creating the Catania stent (CeloNova BioSciences, Tx, US), and its newer iteration the Cobra stent (CeloNova BioSciences, Tx, US).
The FIM ATLANTA study reported a 6-month late lumen loss of 0.60±0.48mm, whilst at 12-months follow-up there were no reported deaths or MI, and a clinically driven TLR rate of 3.6% in the 55 patients treated with the Catania stent. No ST was observed, despite DAPT being given for only 30-days. In addition OCT, which was performed in 15 patients, showed that 99.5% of struts were fully covered at 6-months. Registry data have also demonstrated the absence of ST events at 6-months follow-up amongst 94 patients with ACS who were treated with the Catania stent, and received only 30-days of DAPT. A broader, more real world cohort were enrolled in the follow-up ATLANTA-II registry, which enrolled 300 patients, 14% of whom presented with ST-elevation MI. At 1-year follow-up, the cumulative rate of MACE was 8.8%, with individual rates of cardiac death, MI and TLR of 2.5%, 0.7% and 6.5%, respectively. DAPT was again given for only 30-days, and the rate of ST was 0.7% due to two cases of sub-acute ST.
The Cobra stent has been evaluated in the non-randomised 296 patient PzF SHIELD study, whose favourable results enabled the device to receive FDA approval in March 2017. The study achieved its primary endpoint with a rate of TVF, a composite of cardiac death, MI and clinically driven TLR at 9-months follow-up, of 11.5% which met the pre-specified performance goal of 19.62%, that had been derived from historical meta-analyses of BMS. The study also met its powered secondary endpoint with a late lumen loss of 0.84mm, compared with the performance goal of 1.1mm). There were no ST events. Further studies are on-going including the all-comers e-COBRA registry and the COBRA Reduce trial, which will assess the stent’s performance in patients, treated with oral anti-coagulation, who receive only 14-days of DAPT post PCI.
Titanium-nitride oxide (Figure 21), has been shown to inhibit platelet aggregation, minimize fibrin deposition, reduce inflammation, and promote healing, and consequently has been utilised as a coating on the three iterations of the TiTAN coronary stent (Hexacath, France). The first two versions (TiTAN and TiTAN-2) had a platform of stainless steel, whilst the newest iteration, the TiTAN Optimax, uses cobalt chromium, which offers greater radio-opacity and enables the struts to be 20% thinner. The TiNOX study randomized 92 patients to treatment with either a BMS, or a BMS coated with titanium-nitride oxide and reported a significant reduction in late loss (0.55 ± 0.63 mm vs. 0.90 ± 0.76 mm, p = 0.03) at 6-months follow-up. Clinical evaluation demonstrated significantly reduced MACE, which was driven primarily by a reduction in TLR, with the titanium-coated stent at 6-months follow-up, with results indicating preservation of this out to 5-year follow-up.

Additional studies include the TiTAX-AMI trial, which randomized 425 patients with ST-elevation MI to treatment with either the TiTAN stent or the TAXUS PES. At 12-months there were no significant differences in the primary endpoint (p=0.5), however the TiTAN stent had significantly lower rates of ST (0.9% vs. 4.3%, p=0.03). At 5-years, use of the TiTAN stent lead to a significantly lower incidence of MACE, cardiac death, re-infarction, and ST. Furthermore, despite the absence of an anti-proliferative drug, the rate of TLR was comparable.
In contrast, the TiTAN-2 stent failed to demonstrate non-inferiority when compared to the E-ZES in the randomized 300 patient TIDE study. At 6-months angiographic follow-up, in-stent late lumen loss was 0.64 ± 0.61 mm and 0.47 ± 0.48 mm for the TiTAN-2 stent and E-ZES, respectively (Pnon-inferiority = 0.54). Of note, differences in late lumen loss were more pronounced in patients with diabetes, small vessel disease and patients over 65. Clinical outcomes assessed up to five years of follow-up were comparable. The majority of events occurred within the first year after PCI and were mostly related to clinically-indicated TVR.
Further assessment took place in the BASE-ACS trial, which enrolled 827 patients with ACS who were randomised to either the TiTAN-2 stent (n=417) or EES (n=410). At 1-year the study met its primary non-inferior endpoint of MACE, a composite of cardiac death, non-fatal MI or ischaemia-driven TLR (9.6% vs. EES 9.0%, Pnon-inferiority <0.001). A 5-years follow-up the TiTAN-2 stent remained non-inferior in terms of MACE; whilst its use was associated with significantly lower rates of non-fatal MI (5.9% vs. 9.7%, p=0.03), and comparable rates of cardiac death and TLR.
A more contemporary study in ACS patients is the TIDES ACS trial, which randomised 1500 ACS patients in a 2:1 ratio to the TiTAN Optimax (n=1000) or Synergy EES (n=500). The study’s main hypotheses are that the Optimax will be non-inferior to Synergy for MACE at 12-months follow-up and superior for hard endpoints (cardiac death, MI and major bleeding) at 18-months follow up. Preliminary results from the first 1451 patients who have reached 6-months follow-up show comparable rates of MACE (4.6% vs. 4.5%, p=0.94). Full results are expect in 2018.
This bare metal stainless steel stent is unique by containing on its luminal surface immobile CD34 antibodies (Figure 22). In pre-clinical and clinical studies these antibodies are able to bind to endothelial progenitor cells (EPC), resulting in a rapidly formed, functional endothelial covering of the stent’s struts, which ultimately has the potential to reduce ST and restenosis. Unfortunately, the CD34+ markers that are used to phenotype EPCs are non-specific, and are shared by other hematopoietic stem cells. Therefore, it is possible for the EPC capture stent to sequester other bone marrow cell lines such as smooth muscle progenitor cells, which in turn can lead to neointimal proliferation. This is reflected in published clinical studies that have shown low rates of ST despite only one month of DAPT, however late-loss at 6-month follow-up has repeated been above 0.6mm. Data from the TRIAS HR study, which is the only randomized trial published so far, reported a late loss as high as 1.14±0.64 mm, and an overall higher target vessel failure with the Genous stent compared to the TAXUS PES. Encouragingly, preliminary data at two-year follow-up demonstrated a lower absolute increase in TLR between 1 and 2 years in those treated with EPC stent compared to PES. This may reflect regression of late loss with the EPC stent, as was previously observed in the HEALING II study where late loss fell by 16.9% between 6- and 18-months, and/or late catch-up with PES. Additional data comes from the 5000 patients enrolled in e-HEALING registry, which reported rates of MACE, MI and ST at 1-year follow-up of 7.7%, 1.7% and 1.0% respectively.
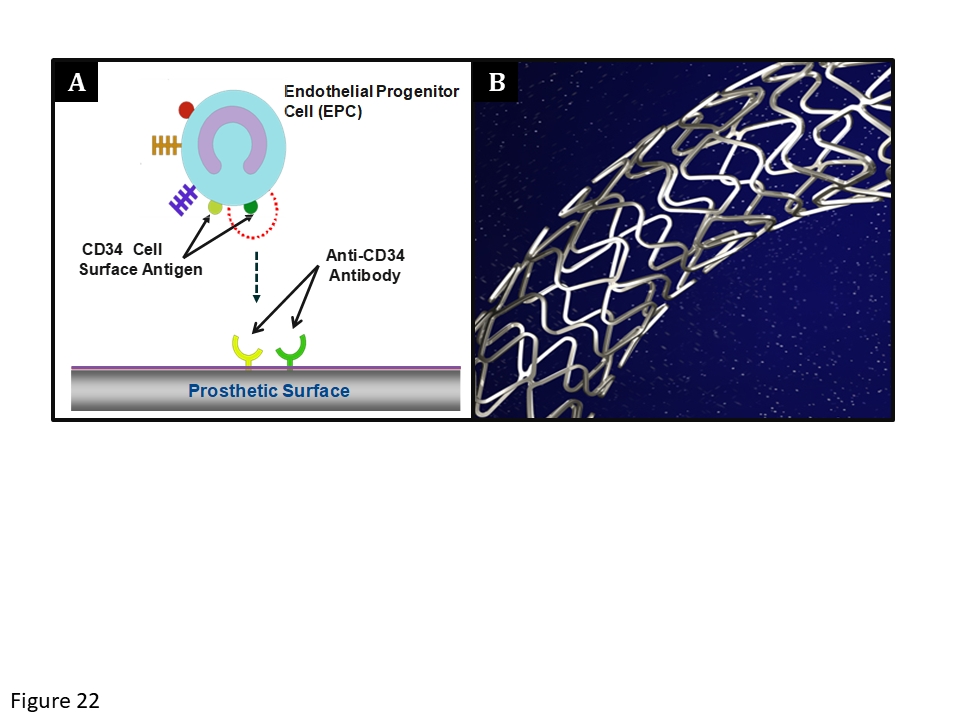
The Genous stent. (A) Schematic representation of the endothelial progenitor cell (EPC) capture technology. The CD-34 antigens on the surface of the EPCs attach to the anti-CD-34 antibodies on the stent’s surface with the aim of promoting endothelialisation. (B) The stainless steel Genous™ stent; (courtesy of OrbusNeich).
A new application of the EPC capture technology has been to combine it with DES technology in a Combo Stent, as described previously.
The use of polytetrafluoroethylene (PTFE)-covered stents has been evaluated in saphenous vein graft interventions. The rationale is that a covered stent may be able to entrap friable degenerated material, decrease the probability of distal embolization, and reduce neointimal hyperplasia. However, a randomized trial of 400 patients undergoing PCI of saphenous vein grafts (SVG) yielded disappointing results, showing no benefit in terms of restenosis or MACE over BMS. In the coronary circulation, the use of covered stents is confined to the emergency treatment of coronary perforations and for the exclusion of giant coronary aneurysms. Unfortunately due to their rigid structure, deliverability can be challenging; and once deployed, they are associated with higher rates of adverse events compared to conventional stents which is possibly due to delayed endothelialisation and an increased susceptibility for thrombus formation. One study reported 6-months rates of sub-acute ST and angiographic restenosis with Jostent of 5.7% and 31.6%, respectively. Recently, PTFE has been replaced with equine pericardium in the Aneugraft™ stent (ITGI Medical, Or Akiva, Israel) consisting of a single, thin-strut, 316L stainless steel, laser-cut, balloon-expandable stent upon which a single layer of equine pericardium is mounted; this approach enables higher deliverability and trackability, and offers an ideal platform for endothelial regrowth and vessel healing.
A stainless steel stent covered with a ultrathin (20 µm) polyethylene terephthalate flexible micronet (MGuard, InspireMD, Israel) has been developed to immobilize thrombus and atheroma between the micronet and the vessel wall during stent expansion mitigating distal embolization. Among STEMI patients undergoing primary PCI, this device significantly increased the primary endpoint of complete (>70%) ST-segment resolution (57.8% vs. 44.7%, p=0.008) and improved TIMI 3 flow (91.7% vs. 82.9%, p=0.006) compared with standard BMS and DES in a randomized clinical trial. Clinical and angiographic 1-year follow-up showed higher rate of MACE with the MGuard, driven by greater ischemia-driven TLR (8.6% vs. 0.9%, p=0.0003) and a trend toward higher rate of definite ST (2.3% vs. 0.5%, p=0.10). Although the study was not powered for this endpoint, lower all-cause and cardiac mortality were recorded at 30 days and 1 year in the MGuard group.The MASTER II trial (N=1100) which was designed to compare the efficacy (ST segment resolution at 60-90 min and infarct size at 2-7 days) and safety (death or reinfarction at 30 days) of the MGuard device with BMS and DES among STEMI patients undergoing primary PCI was terminated due to poor enrolment.
Self-expanding (SE) stents were the first stents to be implanted in coronary arteries, being quickly followed by BE stents, such that both technologies were used with similar frequency in the early days of coronary stenting. SE stents are made from nitinol, an alloy of nickel and titanium, which is uniquely suited for this purpose given its shape memory, biocompatibility, fatigue resistance, and super-elastic qualities which allow it to withstand large amounts of recoverable strain.
In addition to comparable outcomes, SE stents offer distinct advantages over BE stents such as a lower incidence of edge dissections, reduced rates of side branch occlusion and no-reflow, and positive remodelling. Furthermore, animal data suggest that SE stents offer the ability to prevent immediate vessel wall injury, which may eventually translate into a reduction in neointimal hyperplasia, and a larger lumen area. Some of the drawbacks associated with their use are related to their mechanical properties, for example precisely matching stent size to vessel size is hindered by the continued outward radial force that SE stents exert after deployment, leading to negative chronic recoil, and a subsequently larger vessel at follow-up. In addition, SE stents are housed within a delivery catheter that ensures stent security, however, these catheters can be cumbersome to use, and have an associated learning curve. Importantly the delivery profile of these stents is dictated by strut dimensions, as opposed to the balloon profile (as in BE stents). Finally placement accuracy of SE stents is complicated by stent foreshortening on expansion, and/or forward spring movements of the stent from the delivery system once deployment commences.
The advent of DES largely led to a considerable loss of interest in pursuing the development of SE stents, and they were largely abandoned for coronary use. Recently, however there has been a resurgence of interest in this technology for niche coronary settings following new stent designs that have incorporated thinner struts, drug coatings, and improved delivery systems.
At present SE stents are being investigated for use in patients with:
Nitinol SE-dedicated bifurcation stents, which include the Axxess™ (Biosensors International Pte Ltd, Singapore), Stentys™ (Stentys S.A., Paris, France) and Cappella Sideguard™ (Cappella, Inc., Auburndale, MA, USA), have been suggested to improve outcomes in the treatment of bifurcation lesions, owing to their ability to conform the angulated anatomy more optimally than a conventional BE stent (Figure 23). For a more detailed discussion on the indications for these devices please refer to Chapter Bifurcation lesions (old).
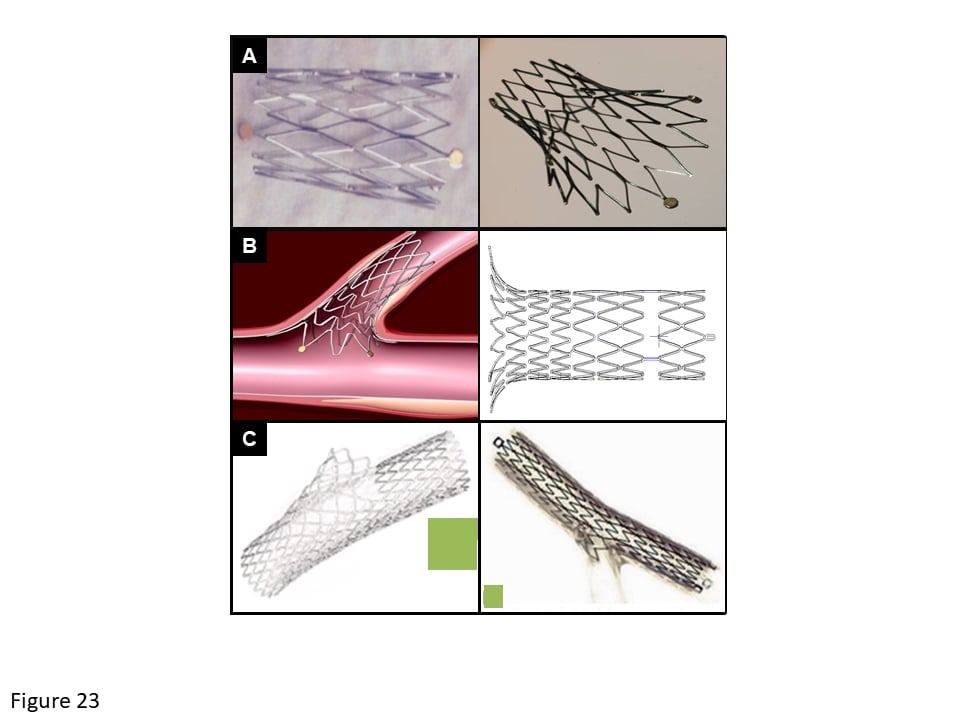
Self-expanding dedicated bifurcation stents
(A) Axxess™, (B) Sideguard®, (C) Stentys™.
Acute MI commonly results from disruption of thin-cap fibroatheromas (TCFAs). It follows that pre-emptive treatment of these lesions involves preventing cap rupture, and promoting endothelialization. Understandably, BE stents are not well suited to these delicate lesions owing to the high radial forces required for their deployment, potentially causing plaque rupture, distal embolization and no-reflow. Conversely, SE stents offer the theoretical advantage of minimizing vessel injury during implantation, thereby reducing the risk of embolising necrotic material and thrombus distally. In the long-term the lack of strut penetration into the necrotic core may theoretically reduce the risk of ST, which may occur through the substantially delayed arterial healing that occurs when struts penetrate into it.
The STENTYS™ stent was assessed in patients having primary PCI for ST-elevation MI in the APPOSITION I study. The trial enrolled 25 AMI patients and reported technical, device and procedural success rates of 100%, 96% and 96%, respectively. Notably, IVUS evaluation three days post stenting demonstrated a significant 18% increase in stent expansion, such that the stent was completely apposed to the vessel wall. At 6-months follow-up, rates of in-stent late lumen loss, binary restenosis and ischaemia-driven TLR were respectively 0.71 ± 0.71 mm, 25% and 12%. Overall the study confirmed the safety and feasibility of the use of STENTYS in AMI and resulted in its C.E. mark for this indication. Following this, the APPOSITION II study randomised 80 patients with AMI to STENTYS (n=43) or a conventional BMS (n = 37), with the aim of assessing strut malapposition 3 days after stent deployment using OCT. As anticipated, results showed significantly lower rates of malapposed struts with STENTYS (0.58% vs. 5.46%, p < 0.001). Clinical event rates at 6-months were comparable.
The APPOSITION III study used a sirolimus-eluting version of the device and reported low rates of MACE (11.2%) at 24-months amongst 1000 acute MI patients treated with STENTYS. In the APPOSITION IV study 152 patients with AMI were randomised 3:2 to either a sirolimus-eluting STENTYS (n=90) or R-ZES (n=62). Angiographic outcomes showed lower late lumen loss at 4- and 9-months with the STENTYs device compared to R-ZES, whilst OCT demonstrated that STENTYS SES was associated with fewer malapposed struts and covered struts that R-ZES. Clinical outcomes were low and comparable between groups.
The vProtect® Luminal Shield (Prescient Medical, Inc., Doylestown, PA, USA) SE stent has been shown in animal studies to promote vascular healing, and importantly, to achieve complete endothelialization of the stented vessel segment within 7 days. Data from the FIM study have demonstrated that the ‘shield’ can induce plaque remodelling and has a positive vascular healing profile, as demonstrated on IVUS. A subsequent study in 29 patients with intermediate de novo coronary lesions treated with the device showed, at 6-months follow-up, a late loss of 0.50 ± 0.30 mm, and a binary restenosis rate of 10.3%. There was no stent malapposition. The rate of MACE was 10.3% related to three TLRs.
Further evaluation of the stent took place in the prospective randomized SECRITT I pilot study, which evaluated the safety and feasibility of stenting a vulnerable plaque with the vProtect® Luminal Shield (n = 13) compared with a medically treated, non-stented (control) group (n = 10). There were no device related complications or MACE events out to 6-months. The study was underpowered to detect differences in clinical events, however it did suggest that sealing these vulnerable plaques was feasible and safe, although the clinical benefit remains to be established.
The use of BE stents in vessels with small diameters is inherently associated with a risk of edge dissection, owing to the high pressures required for optimal stent implantation. Inadequate stent strut apposition and stent underexpansion add risk for ST and restenosis. For lesions located in small-sized vessels, the use of SE stents, which can minimise baro-trauma and the risk of edge dissections, offers distinct advantages. The Cardiomind Sparrow™ (previously Cardiomind Inc, Sunnyvale, CA, USA, now Biosensors, Morges, Switzerland) is a small profile nitinol SE stent that is designed specifically for lesions in small diameter vessels (2.00-2.75mm). The stent, which has a strut thickness of 61µm, is pre-loaded on an 0.014” guidewire, with 2-3 cm of radio-opaque guidewire at the distal end, enabling positioning within the vessel. The stent is deployed through a dedicated Sparrow™ delivery system, which facilitates electrolysis of mechanical latches holding down each end of the stent. The electric current required for release of each latch is less than 0.2 mA, and release occurs within 20 seconds. The CARE I feasibility study was performed in 21 patients with de novo lesions in vessels of 2.0-2.5 mm diameter. At 6-month follow-up, a 13% rise in stent volume index was observed together with a binary restenosis rate of 20%. There was no ST at 30-days, and 2 MACE events up to 24-months follow-up.
The next-generation Sparrow™ stent has a strut thickness of 67 µm, and is coated with a 4 µm-thick layer of sirolimus at a dose of 6 µg/mm and an 8 µm-thick biodegradable PLA/PGLA polymer. It was assessed in the CARE-II study that was designed to randomise 220 patients, with lesions ≤ 20mm in length, in vessels between 2.00-2.75 mm in diameter, to treatment with the bare metal Cardiomind Sparrow™, the sirolimus-eluting Cardiomind Sparrow™ or a BMS. Interim results at 8-months follow-up after enrolment of the first 100 patients (36 Cardiomind BMS, 36 Cardiomind SES and 30 BMS) demonstrated numerically lower in-stent late lumen loss with the drug coated Cardiomind stent, such that the primary endpoint of the study was met (Cardiomind SES 0.29 mm vs. Cardiomind BMS 0.86 mm [p = 0.0001] vs. BMS 0.94mm [p < 0.0001]) and enrolment was stopped. Clinical outcomes were also superior with the drug-eluting Cardiomind stent compared to the other two stents.
In general terms, a delivery system consists of a catheter which carries a stent on its distal end portion. The stent is held in place around the catheter prior to and during percutaneous delivery by means of a sheath (SE stents), or the stent may be crimped to hold it in place (BE stents). The stent must be able to securely maintain its axial position on the delivery catheter without translocating proximally or distally and especially without becoming separated from the catheter. In order to safely and effectively advance a stent delivery catheter through the tortuous and narrow confines of the vessels, it is desirable to have a stent delivery system with a reduced profile (diameter) prior to delivery of the stent.
Nitinol SE stents must be maintained under positive external pressure in order to maintain their reduced diameter configuration during delivery of the stent to its deployment site. Once in position, they spring after being liberated from the sheath. BE stents are pre-mounted over a balloon positioned between the stent and the delivery catheter, at the distal portion of the latter, and crimped to reduce their diameter. These stents are manoeuvred to the deployment site and manually expanded to the vessel diameter by fluid inflation of the balloon.
In order to remove the catheter from the body and minimize damage to any bodily vessels through which the catheter may be drawn, it is also desirable to provide a stent delivery system with a reduced profile subsequent to stent delivery. To provide the balloon with a reduced profile subsequent to stent delivery, stent delivery systems rely on deflation of the balloon, by simply drawing inflation fluid from the catheter until it is effectively collapses.
Better angiographic results correlate with improved clinical outcome. Uncovered dissections (Figure 24) and intramural hematoma are associated with abrupt vessel closure. Stent under-expansion is associated with both restenosis and ST after BMS and DES implantation. Stent under-expansion typically occurs in insufficiently prepared calcified lesions. Strategies that can be attempted to adequately prepare the lesion include balloon pre-dilation (with semi-compliant or non-compliant balloons), atheroablation (rotablator), and atherotomy by means of cutting balloons. Along with improvements in stent design, observations made by IVUS led to changes in deployment strategy, emphasizing the importance of complete apposition of stent struts to the vessel wall. IVUS guidance in DES implantation is associated with a significant reduction in MACE in patients with complex lesions, bifurcation lesions and left main disease. A minimal stent area of >5 mm2 is usually considered satisfactory. Omission of long stented segments and stent overlap should be considered. For bifurcation lesions, the strategy of provisional side-branch stenting is preferred and techniques using two stents with excessive stent overlap like the "crush" or "culotte" techniques should be avoided.
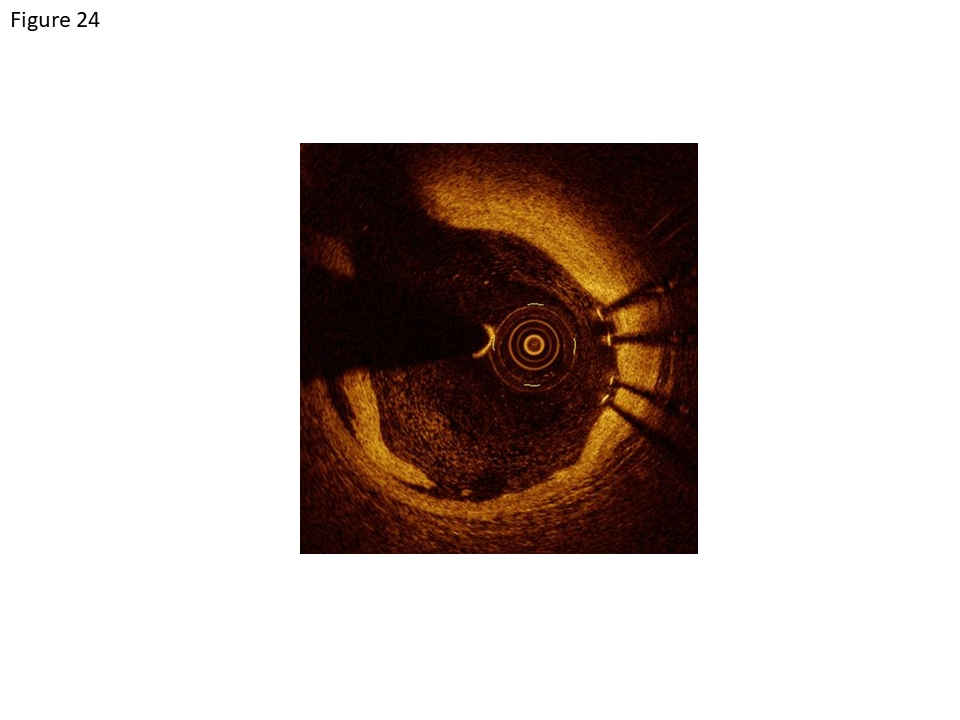
OCT image of an intimal dissection at the proximal stent border with the dissection flap at 7 o’clock and stent struts at 3 o’clock [C7, Lightlab, St.Jude Medical Company].
Refer to 118
Abrupt vessel closure, complicating 6-8% of balloon angioplasty procedures, was associated with considerable rates of mortality and MI, and frequently (40%) resulted in emergency CABG. Stents exert their greatest therapeutic potential in the setting of abrupt vessel closure by nearly eliminating the need for emergency CABG and reducing mortality and MI in this setting. The initial approval of coronary stents for this “bailout” indication was based on a multicenter registry of patients with angioplasty complications who were treated with the Gianturco-Roubin II stent. Contemporary new-generation DES are indicated in all patient and lesion subsets, and there is no formal restriction to their use in clinical practice.
Advances in techniques, equipment, stents and adjuvant therapy have established PCI as a routine and safe procedure in patients with SCAD and suitable coronary anatomy. The mortality risk associated with the procedure in SCAD is <0.5%.
The efficacy of PCI in SCAD in comparison to medical therapy and CABG has been the subject of extensive evaluation. DES are recommended for all lesion sub-sets in SCAD patients. Although direct randomised trials have not demonstrated a survival benefit from PCI over medical therapy in SCAD patients, a network meta-analysis of 100 randomised trials in 93,553 patients suggested that PCI with new-generation DES reduces the risk of all-cause mortality compared with medical therapy and affords rivalling outcomes to CABG.
Primary PCI is the recommended reperfusion therapy over fibrinolysis in ST-elevation MI, if performed by an experienced team within 120 min of first medical contact. Stenting is recommended (over balloon angioplasty alone) for primary PCI. In patients without persistent ST-segment elevation myocardial infarction an invasive strategy (within 72 h after first presentation) is indicated. Urgent coronary angiography (<2 h) is recommended in patients at very high ischaemic risk (refractory angina, with associated heart failure, life-threatening ventricular arrhythmias, or haemodynamic instability). An early invasive strategy (<24 h) is recommended in patients with a GRACE score >140 or with at least one primary high-risk criterion. Non-invasive documentation of inducible ischaemia is recommended in low-risk patients without recurrent symptoms before deciding for invasive evaluation. The revascularization strategy (ad-hoc culprit lesion PCI/ multivessel PCI/CABG) should be based on the clinical status as well as the disease severity, i.e. distribution and angiographic lesion characteristics (e.g. SYNTAX score), according to the local ‘Heart Team’ protocol. New generation DES have proved more effective and potentially safer than BMS among patients undergoing primary PCI throughout 5-year follow-up. No particular safety concerns have been observed in trials including patients with non-ST elevation ACS, and as a consequence, new-generation DES are indicated as default option over BMS in ACS patients.
“On-label” indications for DES use, as approved by the FDA are limited to simple lesions: for SES, de novo lesions ≤30 mm in length in native coronary arteries with reference vessel diameters of 2.5-3.5mm, and for PES de novo lesions ≤28 mm in native coronary arteries 2.5-3.75mm in diameter. If follows that, “off-label” indications represent a higher-risk population with more complex lesion morphologies and unstable clinical presentations.
One of the criticisms of early DES trials was that they enrolled stable patients treated with DES for ‘on-label’ indications. For example, the meta-analyses by Stettler et al, Stone et al, Spaulding et al, Kastrati et al and Mauri et al included patients who were treated for essentially stable de novo lesions, which had a mean lesion length of 23-24 mm, a mean vessel diameter of 2.7 mm, and were treated with an average of 1.2-1.4 stents. There were concerns that the comparative results between DES and BMS seen in these studies did not reflect real-world practice in which 70-75% of DESs are implanted for ‘off-label’ indications.
Unfortunately, the lack of any dedicated trials comparing ‘off-label’ DES and BMS added to these concerns, such that the FDA circulatory system devices advisory panel which met in December 2006, concluded that there was a need for a comprehensive assessment of the safety and efficacy of ‘off-label’ DES use. This prompted numerous studies, many of which were observational, and ultimately demonstrated that the use of DESs for ‘off-label’ indications was associated with poorer clinical outcomes in terms of death, MI and repeat revascularization when compared to DES use for ‘on-label’ indications. [408, 411-413] Of equal importance are the results from registries and randomized controlled trials which suggest that ‘off-label’ use of a DES is no worse than the use of BMS,[91, 320, 414-416] with some studies, such as the Medicare and STENT registry actually demonstrating significantly improved outcomes with the use of a DES. These findings suggest that the overall poor outcome with off-label use is most likely related to patient or lesion characteristics, rather than to specific shortcomings of DES.
The advent of coronary artery stents has transformed PCI into a safe and reproducible revascularization procedure. The most important benefit of stents was the effective treatment of abrupt or threatened vessel closure following balloon angioplasty. Whereas abrupt closure in the balloon angioplasty era was associated with an increased risk of death (5%), MI (40%) and need of emergency CABG (40%), Schömig et al. reported a significant reduction of these adverse events with the use of stents (death: 1.3%, MI: 4.0%, emergency coronary artery bypass grafting: 1.0%) (Figure 25). The ACC/National Cardiovascular Data Registry analyzed data from 558,273 percutaneous coronary interventions performed between 2001 and 2004 and observed an in-hospital mortality of 0.7%, a rate of MI of 1.1%, and the need of emergency CABG in 0.6% of patients. Mortality is not only related to the procedure but also the clinical condition of the patient at baseline. Accordingly, several clinical and angiographic variables have been identified which are associated with an increased mortality risk including advanced age, female gender, diabetes, renal dysfunction, cardiogenic shock, a large area of myocardium at risk, impaired left ventricular function and an urgent procedure. In addition, PCI performed in the setting of STEMI (primary PCI) is associated with a higher death rate than is observed among patients undergoing elective PCI. The risk of stroke is low ranging from 0.1% to 0.3% in the ACC/NCDR registry during the in-hospital period.
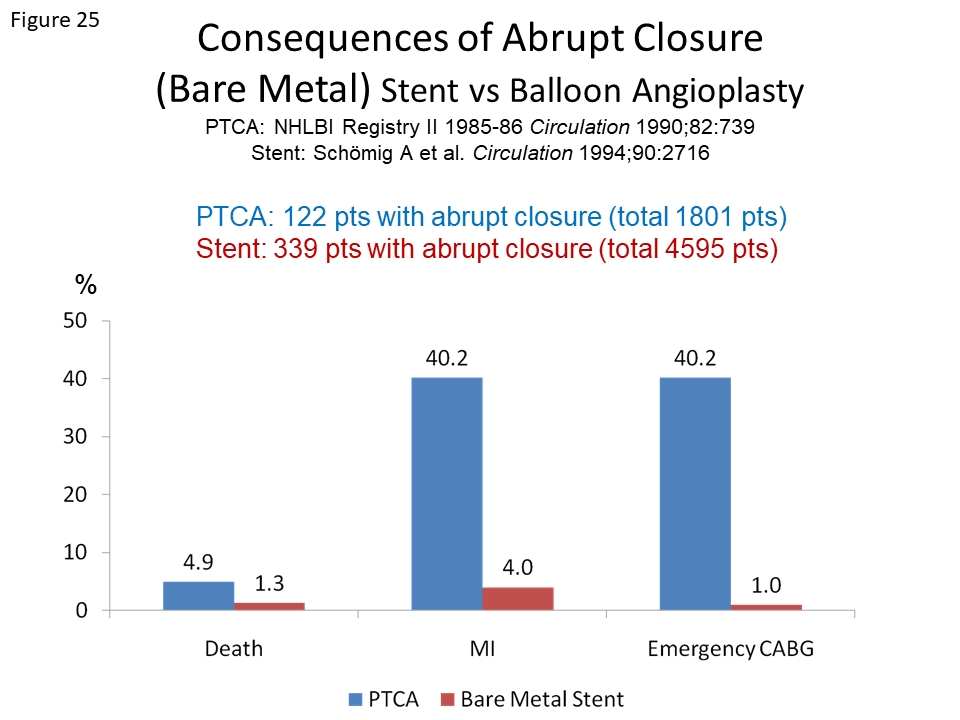
Clinical consequences of abrupt closure following BMS implantation (in red) as compared with ballon angioplasty treatment (in blue).
Balloon inflation during a procedure almost always results in ischemia even if not accompanied by ST-T wave changes. The aetiology of peri-procedural myonecrosis is multifactorial and includes among others side branch occlusion and distal embolisation. Any increase in CK-MB after PCI is associated with a small, but statistically and clinically significant increase in the subsequent risk of death.11 An analysis of 6,755 SES treated patients demonstrated that irrespective of lesion complexity, mortality at 6 month follow-up was highest among those who incurred a peri-procedural MI (4.3%), followed by those who developed any troponin elevation (2.5%) and was significantly lower among those who remained free of these events (1.3%). In a subgroup analysis of the TAXUS V trial among patients requiring multiple overlapping stents13, PES use was associated with an increased incidence of MI at 30 days (8.3% vs. 3.3%; P = 0.047) compared with the otherwise identical BMS, most of which were non–Q-wave infarctions. The rate of MI was numerically increased with both planned (6.3% vs. 2.9%) and unplanned (14.0% vs. 4.2%) use of multiple PES. Blinded core laboratory angiographic analysis in the multiple stent cohort demonstrated more frequent occurrence of progressive side-branch narrowing to more than 70% diameter stenosis or to total occlusion with PES (42.6% vs. 30.6%; P = 0.03) than BMS and a greater likelihood of reduced side branch TIMI flow (41.9% vs. 28.6%; P = 0.02). No differences were present in main vessel TIMI flow, acute occlusion, ST, distal embolization, or other angiographic complications compared to the BMS counter-part. Reductions in rates of clinical and angiographic restenosis were present at 9 months in patients who received multiple stents and who had been assigned to PES rather than BMS, with similar rates of cardiac death, MI, and ST.
In the ENDEAVOR IV Trial14, ZES resulted in a significantly lower rate of MI at 30 days compared to PES (0.8% vs. 2.3%; P = 0.02). A subgroup analysis, which focused specifically on the incidence of side branch occlusion immediately after stent implantation as a possible explanation for the higher rates of post-procedural MI, demonstrated a significantly higher rate of side branch occlusion with PES than ZES (4.0% vs. 2.2%; P = 0.03). Similar findings were evidenced in the SPIRIT III trial15 comparing EES with PES: at 30 days there tended to be fewer MI among the patients randomized to receive EES compared with PES (7/667 patients [1.0%] vs. 9/330 [2.7%], respectively; relative risk, 0.38 [95% CI, 0.14 to 1.02]; P=0.06), with comparable rates of cardiac death (0% in both groups) and TLR (3/667 patients [0.4%] vs. 1/330 [0.3%], respectively; relative risk, 1.48 [95% CI, 0.15 to 14.21]; P>0.99). These results underline the central role of the distinct mechanical features of each individual device on clinical outcome. Newer generation DES appear to be associated with a lower rate of peri-procedural myonecrosis most likely related to improved stent design with less side branch compromise.
In balancing the risks and benefits of PCI with the use of different technologies from a patient’s perspective, the assessment of safety end points such as overall mortality and MI are most important. A meta-analysis of 29 trials in 9,918 patients comparing balloon angioplasty with BMS observed a similar risk of death and MI during follow-up (5.4% versus 4.8%, OR=0.9, CI 0.72-1.11). After their extensive use, concerns were raised that improved efficacy with early generation DES was offset by a higher rate of very late adverse events such as ST, resulting in the need for long-term DAPT. In the aftermath of these studies, which caused widespread concern, several patient based meta-analysis were performed which reassuringly demonstrated the overall comparable outcomes between DES and BMS in terms of death and MI, at both short and long term follow-up (Table 4). The largest of these studies by Stettler et al reported a similar risk of death between patients treated with SES, PES and BMS; the risk of MI although comparable between PES and BMS (p=0.99), was significantly lower with SES compared to BMS (p=0.03). Additional meta-analyses performed at a similar time by Stone et al, Spaulding et al, Kastrati et al, Mauri et al and Kirtane et al all reiterated the safety of DES, by demonstrating the absence of any significant increased risk of death and/or MI with the use of early generation DES compared to BMS. [88, 91, 422-424]
More contemporary meta-analyses have also dispelled the earlier concerns by consistently showing no increased risk of mortality with the use of DES compared to BMS., A meta-analysis by Kang et al, which included 90,584 patients from 113 trials, reported comparable mortality between DES (SES, PES, E-ZES, R-ZES, EES, Promus EES and BES) and BMS. Furthermore, all DES, apart from PES, were shown to significantly reduce the risk of MI compared to BMS with hazard ratios between 0.42 and 0.85. A larger network meta-analysis by Bangalore et al, which included data from 126 trials and 258,544 patient years of follow-up, showed similar performance in terms of comparable all-cause mortality for all DES apart from EES, which was shown to significantly reduce mortality (HR 0.72, 95% CI 0.58-0.90). Rates of MI were significantly lower compared to BMS for all DES apart from PES.
A smaller meta-analysis by Valgimigli et al which only included patients receiving EES or BMS in 4896 patients, followed up for 720 days reported findings consistent with the previous mega studies, with significant reductions in cardiovascular mortality (HR 0.67, p=0.01) and MI (HR 0.71, p<0.01) with EES. Amongst patients receiving BES, Palmerini et al showed significant reductions compared with BMS in cardiac death and MI at 1-year follow-up amongst 85,490 patients, with similar results seen at longer follow-up in over 50,000 patients. In STEMI patients, Sabate et al showed no adverse risk of all-cause mortality (HR 0.98, 95% CI 0.60-1.35) with the use of EES or BES compared to BMS at 1-year and a significant reduction in target vessel re-infarction (HR 0.36, 95% CI 0.14-0.91).
Restenosis, defined as greater than 50% diameter stenosis at follow-up angiography, was the most important limitation of balloon angioplasty with an incidence of 30-50% and a need for target vessel revascularisation in 20-30% of patients. The mechanism of restenosis following balloon angioplasty is multifactorial, nevertheless roughly two thirds is mediated by pathologic arterial remodelling with shrinkage of the dilated segment, whilst one third is mediated by neointimal proliferation. Coronary artery stents have been found to be beneficial as anti-restenosis devices by eliminating arterial shrinkage due their radial force.
The STRESS and the BENESTENT trials compared elective stenting with angioplasty alone in native coronary arteries with short (<15 mm in length) de novo lesions and showed a 25-30% reduction in restenosis rate. Subsequent stent trials confirmed reduced rates of restenosis and TLR in patients undergoing stent implantation of SVG, lesions located in the proximal left anterior descending artery, restenotic lesions and patients presenting with acute STEMI. A meta-analysis of 29 trials in 9,918 patients comparing balloon angioplasty with BMS implantation confirmed a significant reduction in restenosis (odds ratio: 0.52. 95% CI [0.37 to 0.69]) and the need of repeat PCI (odd ratio: 0.59. 95% CI [0.50 to 0.68]).
The clinical consequences of restenosis depend on the degree of restenosis, area at risk subtended by the restenosed target lesion, amount of recruitable collaterals, and lesion location. Restenosis impacts on clinical outcome in different ways: first, repeat revascularization procedures influence patient’s quality of life. In the Optimal Angioplasty versus Primary Stenting (OPUS) I trial, a randomized comparison of routine and provisional BMS implantation that prospectively assessed quality of life parameters, patients without restenosis had less frequent angina (17% vs 22%, P = 0.03), fewer limitations in physical activities (21% vs 27%, P < 0.004), and better quality of life (25% vs 21%, P = 0.003). Secondly, restenosis is associated with a risk of MI; several studies report a 2-19% rate of restenosis-related MI. In addition, the treatment of restenosis itself is also associated with a small but finite procedural risk of mortality or MI. Finally, observational studies suggest a potential negative impact of restenosis on prognosis. The outcome of 3,363 patients treated with balloon angioplasty and repeat angiography was analysed according to the presence (1,570 patients) or absence (1,793 patients) of restenosis. Although survival at 6 years was similar in both groups (95% vs 93%, P = 0.16), patients with restenosis had an increased rate of MI (15% vs 12%, P = 0.0001). A study of 603 patients with diabetes who underwent balloon angioplasty observed a higher 10-year mortality in patients with, as opposed to without, restenosis (24% without restenosis, 35% with non-occlusive restenosis, and 59% with occlusive restenosis) (Figure 26). Notably, occlusive restenosis was an independent predictor of mortality in multivariate analysis. A series of 2,272 consecutive patients treated with BMS between 1992 and 1996 reported a mortality rate of 6.0% at 4 years in patients without and 8.8% in patients with restenosis (P = 0.02) (Figure 27). Another large analysis including 10,004 patients with 15,004 treated patients found that restenosis at angiographic follow-up was associated with a small but significant increase in the risk of mortality at 4-year follow-up (adjusted HR 1.23, 95%CI 1.03-1.46). While these data raise the question as whether surveillance angiography should be part of the routine follow-up after PCI, recent randomized evidence does not support a benefit from follow-up angiography in terms of clinical outcomes.
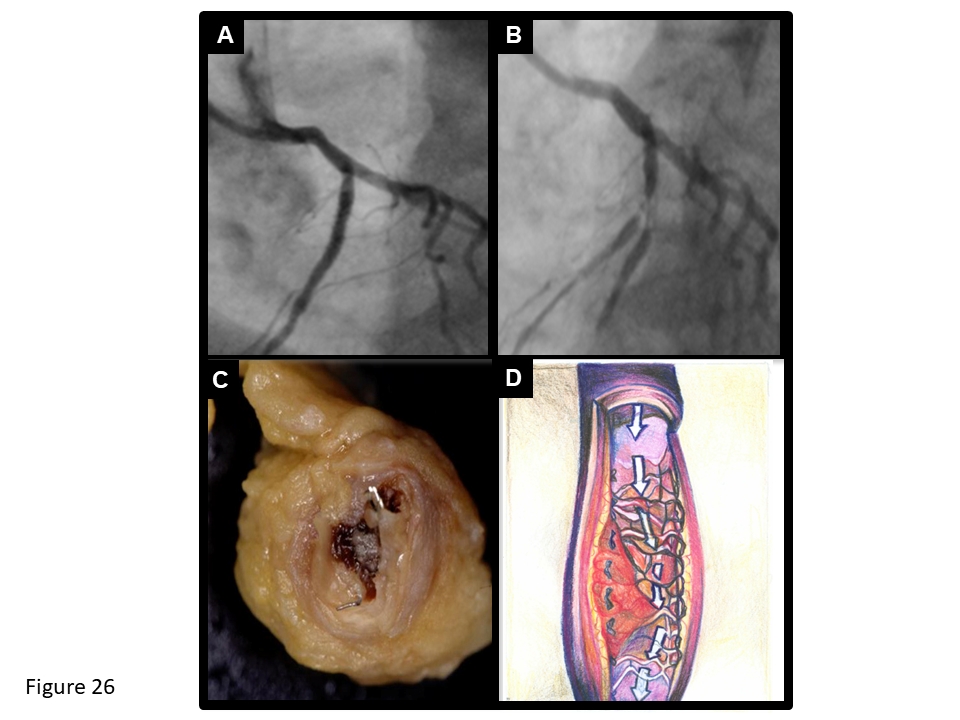
Angiographic, autopsy and schematic drawing of ST. Drug-eluting stent implantation of the proximal left anterior descending artery (A) complicated by ST (B) occuring 7 months later, shortly after discontinuation of DAPT. Gross pathological example of ST (C) and schematic drawing of underlying mechanisms including uncovered and malapposed struts (D).
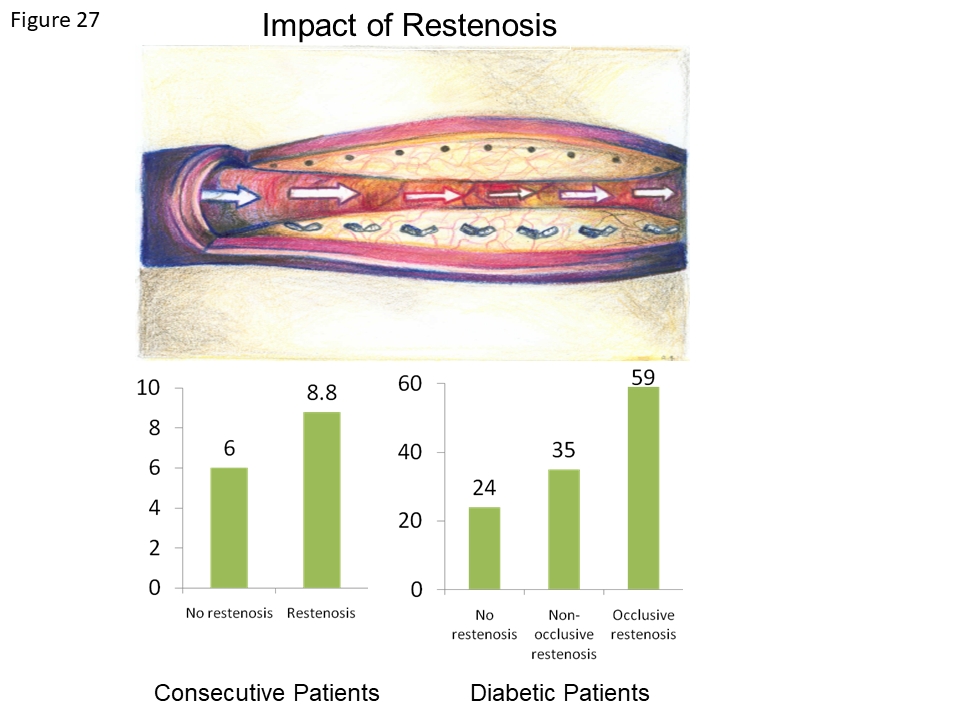
Clincal impact of restenosis during long-term follow-up in observational studies. On the left side, the 4-year mortality is shown in patients with versus without restenosis following BMS implantation showing an increase in overall mortality in patients with restenosis. On the right side, the 10-year mortality of diabetic patients with no versus non-occlusive versus occlusive restenosis is shown. Mortality is lowest among diabetic patients without restenosis and highest among diabetic patients with occlusive restenosis.
Numerous randomized clinical trials and meta-analyses attest that DES reduce rates of restenosis and repeat TLR compared with BMS., , , , In a collaborative network meta-analysis of 38 randomized trials involving 18,023 patients the rate of TLR was reduced by 70% with the use of SES and by 58% with the use of PES compared to BMS at 4 years. For the comparison of SES versus BMS, this benefit translated into a number needed to treat to prevent one revascularization event of 7 patients; for PES versus BMS the figure was 8 patients. More contemporary meta-analyses show a consistent marked reduction in TLR with DES compared to BMS., Kang et al reported reductions in TLR of 81% with BES versus BMS (HR 0.19, 95% CI 0.12-0.29) and 80% with EES versus BMS (HR 0.20, 95% CI 0.14-0.28) at 1-year. Bangalore et al reported slightly lower reductions in TLR compared to BMS, however hazard ratios still ranged from 0.30 with EES to 0.57 with E-ZES. Of note, DES are superior to BMS in all lesion and patient subsets studied to date including small vessels, large vessels, long lesions, diabetic patients and those with acute MI. Although the greatest benefits of DES over BMS regarding TLR reduction are seen during the first year after implantation, all long-term analyses indicate that the benefit is sustained long-term.
ST is a rare but devastating adverse event following PCI, which results in abrupt closure of the treated artery with the incumbent risk of sudden death or MI (Figure 26). The impact of ST is influenced by the myocardial area at risk, its viability, the degree of instantly recruitable collaterals, and the speed of reperfusion therapy. Mortality rates of ST vary across studies depending on its definition even though the Academic Research Consortium criteria have been used in most contemporary trials. In an analysis from the ADAPT-DES study, which included 8,582 patients treated with a DES, 1 in 5 non-procedural MIs were due to a ST event during 2 years follow-up. Similarly, very late ST was the underlying cause of MI in a fifth of the 4,184 patients with SCAD included in the CORONOR registry and, importantly, the mortality rate in those patients was substantially higher than that related to MIs due to other aetiologies (18% per year vs. 7% per year).
In light of the potential devastating consequences of ST, risk stratification and identification of patients at highest risk for ST is of great importance. Multiple factors have been identified to portend an increased risk for ST following DES implantation and include: 1. patient related factors, 2. procedural characteristics, 3. lesion properties, 4. factors related to the implanted device (Figure 28). Studies using OCT have shown that uncovered struts, malapposition, under-expansion, and edge dissection are dominant findings of early ST, whereas malapposition, neoatherosclerosis, uncovered struts, and under-expansion are principal correlates of very late ST.
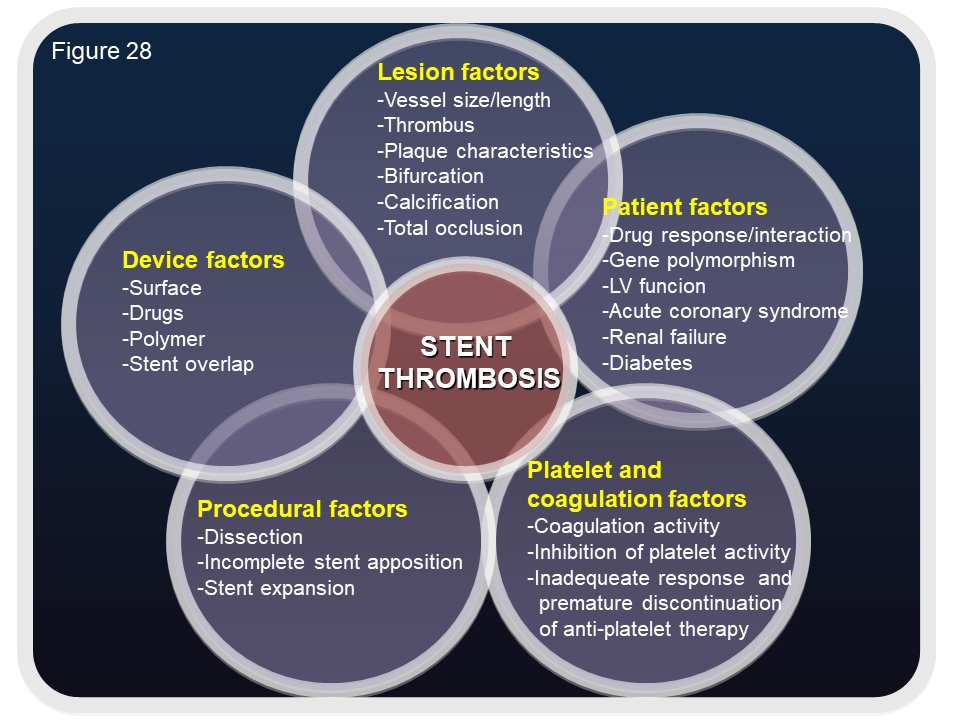
Multiple factors have been identified to portend an increased risk of ST following drug-eluting stent implantation including patient-related factors, procedural characteristics, lesion properties, device factors and antiplatelet and coagulation factors.
Meta-analyses have shown that the thin-strut, fluoropolymer coated EES is associated with lower rates of definite ST than other DES, and unexpectedly, even lower than BMS.[425-427, 454] Furthermore, data from the large SCAAR (Swedish Coronary Angiography and Angioplasty Registry) registry, showed a similar risk of very late ST in patients undergoing primary PCI treated with new generation DES and BMS. In a larger network meta-analysis including 147 randomised trials in 126,526 patients, the risk of definite or probable ST at 1-year was significantly lower with PtCr-EES, R-ZES, and Orsiro SES when compared against BMS. The notion of new-generation DES being safer than BMS represents a paradigm shift in the evolution of PCI.
Stent fracture remains an uncommon late complication of DES implantation, whose true incidence amongst early generation DES remains unknown, however rates of 1-2%, 1-8% and up to 29% have been reported in randomised, observational and autopsy studies, respectively. Notably the majority of stent fractures have been reported with the Cypher SES, whereas stent fractures with TAXUS PES and BMS have been seen very rarely. This difference may be related to the increased radio-opacity of the Cypher SES, its closed cell design, and/or the greater neointimal coverage seen with the PES and BMS that may strengthen and stabilize the struts to withstand the mechanical forces that result in stent fracture. Overall stent fractures can range from a single strut fracture (Grade I) to multiple strut fractures (Grade V) (Figure 29).
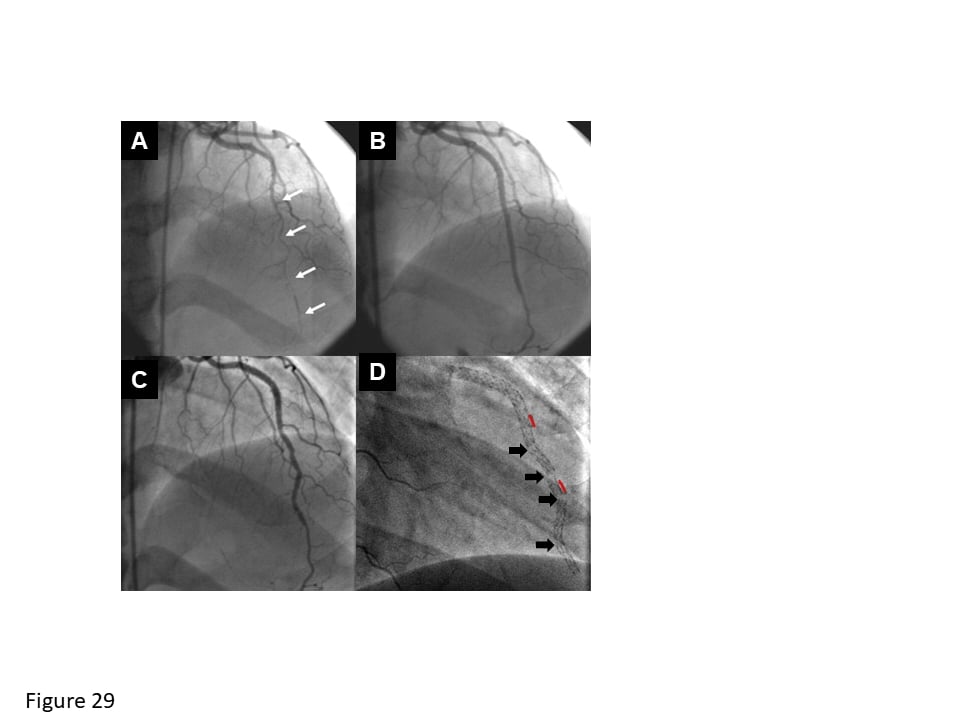
Stent fracture. (A) long, diffusely diseased left anterior descending artery was treated with 3 SES (white arrows). (B) The initial angiographic result is excellent, however, at (C) 3-months’ follow-up, an irregular appearance is seen, and is the result of (D) 4 stent fractures (black arrows) occuring adjacent to regions of stent overlap (red lines).
There are several causes for stent fractures which include both mechanical and lesion based factors: a) Mechanical factors: Stent fracture may be the consequence of an excessive mechanical vessel wall stress that occurs from extreme repetitive contraction and flexion of the vessel. Of note this may actually be a protective mechanism for stress relief within the vessel. b) Lesion factors: Predictors for stent fractures have included lesions located in the right coronary artery, and/or lesions in very tortuous/severely calcified vessels. Additional factors increasing the risk of stent fracture include implantation of long and/or overlapping stents, underlying diffuse disease, saphenous vein graphs, and treatment of chronic total occlusions., In a recent autopsy study longer stent length, use of the Cypher stent and longer stent duration were all identified as independent predictors of stent fracture.
Patients with stent fractures may remain asymptomatic, however they may present with ACS, ST, or recurrent angina due to clinical restenosis; overall 70-80% of those patients with a stent fracture will present with in-stent restenosis or ST. The extent of symptoms appears to be related to the grade of the stent fracture with few symptoms occurring as a result of Grade I-IV stent factures, whilst Grade V stent fractures are associated with the most adverse clinical events.
There are no data on definitive treatment, however repeat PCI, which is the current preferred strategy, appears to provide prompt symptom relief. Some suggest treatment using a short stent, together with extending DAPT beyond 12-months.
Coronary artery aneurysms are a rare complication of stenting, whose true incidence, clinical course and treatment are largely unknown (Figure 30). Nevertheless, studies report an incidence of between 0.3-6.0% after DES and BMS implantation. There are a number of postulated causes for these coronary artery aneurysms, some of which are specific for DES. In general, mechanical causes include the use of oversized balloons or stents, high-pressure balloon inflations and atherectomy all of which can cause residual dissection and deep arterial wall injury eventually leading to aneurysm formation. Of note for DES, the elution of anti-proliferative drugs and/or presence of a polymer can lead to delayed re-endothelialization, inflammatory changes in the medial wall, ISA, and hypersensitivity reactions all of which can result in coronary artery aneurysm formation. Data on coronary aneurysms are mainly derived from case reports, which indicate a variable clinical course, which is similar irrespective of whether the aneurysm is post BMS or DES implantation. In particular aneurysms have been detected from as earlier as 3-days post DES implantation, and as late as 9-year following BMS implantation.
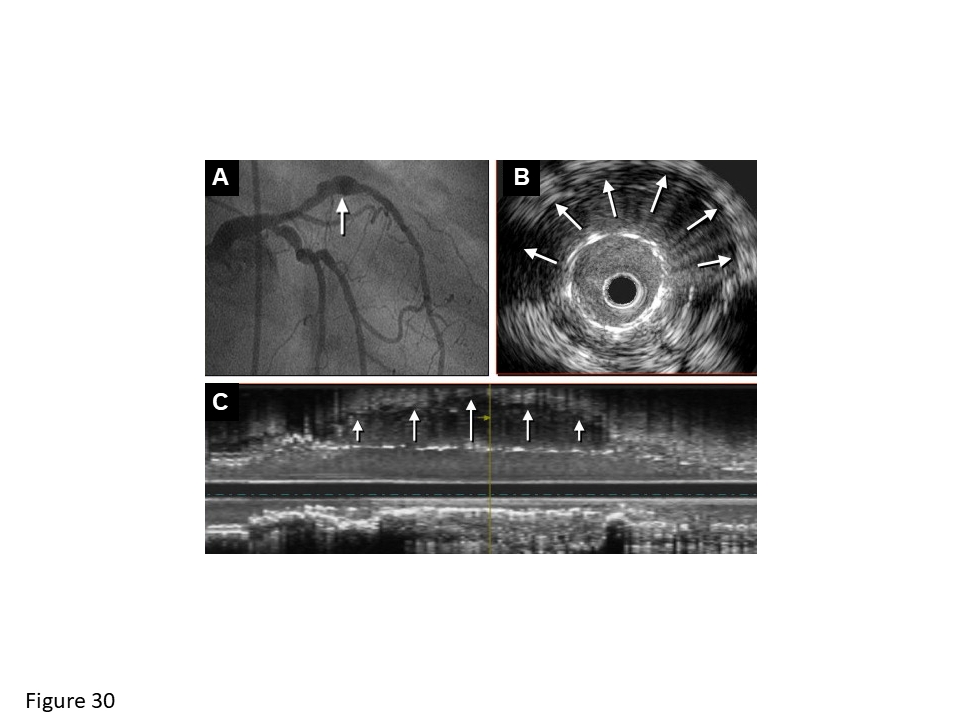
Coronary artery aneurysm. A coronary aneurysm (white arrows) is seen on (A) coronary angiography and on (B) cross-sectional and (C) longitudinal intravascular ultrasound. The aneurysm has led to extensive stent malapposition (B and C).
Two post-stenting coronary phenomena linked to coronary aneurysms have been recently described: a) Coronary evaginations detected by means of OCT and suspected whenever the luminal vessel contour extends in a pouchlike fashion beyond the line connecting all stent struts (stent contour). Theses were more common among SES- than PES-treated lesions (17 vs. 7 per 100 cross sections, p = 0.003) in the SIRTAX Late Study. Combined with a high degree of malapposition and protrusion, they were associated to 2 cases of very late ST during a extended clinical follow-up of the aforementioned trial. b) Peri-stent contrast staining (PSS) which is defined as contrast staining outside the stent contour extending to ≥ 20% of the stent diameter, measured by quantitative coronary angiography. Severe PSS is defined as contrast staining outside the stent contour extending to ≥ 50% of the stent diameter. Lesions with PSS within 12 months after SES implantation were associated with higher rates of subsequent TLR as well as very late ST compared with lesions without PSS.
Coronary artery aneurysms can be associated with restenosis, whilst turbulent and sluggish blood flow in the area of the aneurysm, coupled with a metallic stent can predispose patients to the risk of ST and/or distal embolization. Currently there are no definitive data on the best management of patients with coronary artery aneurysms, treatment of which is complicated by some aneurysms resolving spontaneously, whilst others lead to life-threatening complications. Besides the use of long-term DAPT to minimise the risks of ST, therapeutic options that can be considered include the use of coils, and cardiac surgery.
Coronary stenting is the standard of care for flow-limiting atherosclerotic disease in a wide variety of lesions and patients subsets. Complexity of both has been associated with worse long-term results. Notwithstanding, continued research and technological advances have contributed to improved outcomes. Such subsets include
A small, randomized trial (n = 500) comparing SES with thin-strut BMS showed significantly lower angiographic restenosis (8.3% vs 25.5%, respectively; RR 0.33, 95% CI 0.19-0.56, P <0.001) and TVR (7.2% vs 18.8%; RR 0.38, 95% CI 0.22-0.66, P <0.001) with the DES. The benefit was, however, largely restricted to patients with small vessel disease (reference vessel diameter <2.8 mm; restenosis of SES 7.0% vs 34.2% for BMS; P <0.001). In contrast, binary restenosis was similar in vessels with a reference vessel diameter of 2.8 mm or more (mean RVD 3.1 mm; SES 10% vs BMS 13%; P = 0.52). Another randomized trial comparing newer generation DES with BMS in 826 patients without routine angiographic follow-up observed lower rates of TVR at 18 months (7.5% vs 11.6%, respectively; P = 0.05). A stratified subgroup analysis of this trial indicated that the benefit was limited to patients who received at least one small stent (<3.0 mm diameter; TVR HR 0.44 in favour of DES; P = 0.02), whereas no difference was observed in patients who received only large stents (≥3 mm). The Ontario propensity score matched comparison of DES and BMS showed that DES were particularly beneficial in patients with small vessels (<3 mm) and long lesions (≥20 mm). The number needed to treat in patients with small vessels ranged from 0 to 12 in patients with diabetes, to 27 to 83 in non-diabetic patients. Similarly, the number needed to treat in patients with long lesions ranged from 10 to 23 in patients with diabetes, to 27 to 53 in non-diabetic patients. Accordingly, DES seem particularly useful in vessels with a reference vessel diameter of 3 mm or less and long lesions.
Data from studies of newer generation DES have failed to show any influence of vessel diameter on stent performance. One-year data from the XIENCE V USA study showed comparable performance of EES in terms of MACE, TLR and ST amongst patients receiving a single EES <=2.5mm (n=838) or >2.5mm (n=2015) in diameter. Two-year outcomes of patients enrolled in five R-ZES studies demonstrated comparable performance in terms of TLF (10.1% vs. 8.7%, P=0.54) when R-ZES was used in vessels with a reference vessel diameter below (n=1956) and above 2.5mm (n=3174). In contrast, in the LEADERS study TLR (9.6% vs. 2.6%, p=0.001) and MACE (12.1% vs. 7.1%, p=0.04) were significantly higher in patients treated with BES for vessels less than- or more than 2.75mm in diameter. Amongst those patients with a small vessel diameter, there was no difference in performance of SES versus BES. Similarly no between-stent difference was observed in a propensity matched analysis of 1302 patients treated for acute MI in the KAMIR registry who had vessels <=2.75mm in diameter and received either EES to R-ZES. In the PLATINUM SV study, PROMUS EES had significantly lower rates of TLF (2.4% vs. 21.1%, P<0.001) when compared to historical controls receiving TAXUS PES in vessels between 2.25 and 2.5mm in diameter.
Likewise, in the PLATINUM LL, the PROMUS EES was used to treat lesions between 24 and 34 mm with outcomes compared to historical controls receiving TAXUS PES. At 1-year TLF was significantly lower with PROMUS EES (3.2% vs. 19.4%, P<0.001). Non-inferior angiographic and clinical outcomes have been reported in studies comparing EES to SES, R-ZES to SES and Nobori BES to Promus EES in patients with lesions longer than 24mm.
BASKET PROVE prospectively addressed the question whether DES are beneficial among patients with large vessels as compared to BMS and randomly assigned treatment of 774 patients with EES, 775 patient with SES and 765 patients with BMS. During a median follow-up of 745 days, the investigators noted no difference in terms of death (EES 3.2%, SES 3.6%, BMS 4.4%), MI (EES 1.7%, SES 0.9%, BMS 2.6%) and definite or probable ST (EES 0.6%, SES 0.6%, BMS 1.2%). However, rates of target revascularization were significantly lower for both EES (3.7%, PEES vs BMS = 0.002) and SES (4.3%, PSES vs BMS = 0.005) compared with BMS suggesting that the use of DES is safe and more effective than BMS in patients undergoing PCI for lesions in large vessels.
The role of biodegradable-polymer DES in large vessel stenting has been assessed by the randomized BASKET-PROVE II trial that showed similar performance of a BP BES compared with the durable- polymer EES. Both DES showed a superior efficacy profile over BMS but without evidence for better safety.
Stent overlap occurs in up to 30% of patients undergoing PCI in contemporary clinical practice for a variety of reasons including excessive target lesion length, incomplete lesion coverage, edge dissections and residual thrombus. The use of overlapping BMS is associated with inferior clinical outcomes compared to patients treated with a single BMS or overlapping DES, mainly due to higher rates of TLR.
In the largest study to date addressing long-term clinical outcomes among patients treated with the unrestricted use of early-generation overlapping DES, patients with DES overlap had a higher incidence of MACE (cardiac death, MI, ischaemia-driven TLR) and impaired angiographic results as compared with non-overlapping or single DES control groups.
Contemporary data from a prospective, unrestricted DES registry, continued to show that patients with DES overlap have a higher incidence of ischemic events as compared with non-overlapping DES controls during three-year follow-up. However, this finding was driven primarily by a higher incidence of such events in the early-generation SES overlap patient cohort when compared with non-overlapping SES controls. Conversely, among patients treated with the newer-generation EES, rates of the composite primary endpoint were similar among patients with and without overlap.
Coronary artery stents constitute the most important advance in the field of percutaneous coronary intervention since the introduction of balloon angioplasty. Stents are used in more than 90% of procedures today and have enabled the technique to become one of the most frequently performed therapeutic interventions in medicine. The most important benefit of coronary artery stents has been the effective treatment of abrupt or threatened vessel closure eliminating the need of emergency bypass surgery required in 5-8% of patients in the balloon angioplasty era. In addition, the technique of coronary artery stenting has allowed reproducible results and resulted in a short procedure requiring only minutes in uncomplicated cases. Moreover, the ease and predictable outcome in the context of excellent peri-procedural safety as well as cost considerations contribute to the justification for ad hoc procedures as the preferred approach for patient care. Controlled release of anti-proliferative drugs from polymer coatings immobilized on the stent surface were realized in the form of drug-eluting stents. These devices effectively reduced restenosis and lowered the need of repeat revascularization of the target lesion to below 5%. Of note, newer generation DES have overcome the limitation of first generation DES – the problem of very late ST thus combining improved efficacy while maintaining an excellent safety profile.
Francesco Prati, Flavio Giuseppe Biccirè
Updated on May 13, 2021
Soo-Teik Lim, Tian-Hai Koh
Updated on February 1, 2018
Kai Ninomiya, Scot Garg, Alexandre A. Abizaid, Ron Waksman, Ashok Seth, Joanna Wykrzykowska, John A. Ormiston, Patrick W. Serruys, Yoshinobu Onuma
Updated on September 30, 2022
Bruno Scheller
Updated on May 13, 2021