Minneapolis Heart Institute and Minneapolis Heart Institute Foundation, Abbott Northwestern Hospital, Minneapolis, MN, USA , Division of Cardiology, VCU Health Pauley Heart Center, Virginia Commonwealth University, Richmond, VA, USA, Director of CTO, Complex and High Risk Angioplasty, New York Presbyterian Hospital, Columbia University Medical Center, New York, NY, USA, Director of Interventional Cardiology, Emory University, Atlanta, GA, USA, Division of Cardiology, Emory Healthcare, Emory University, Atlanta, GA, USA
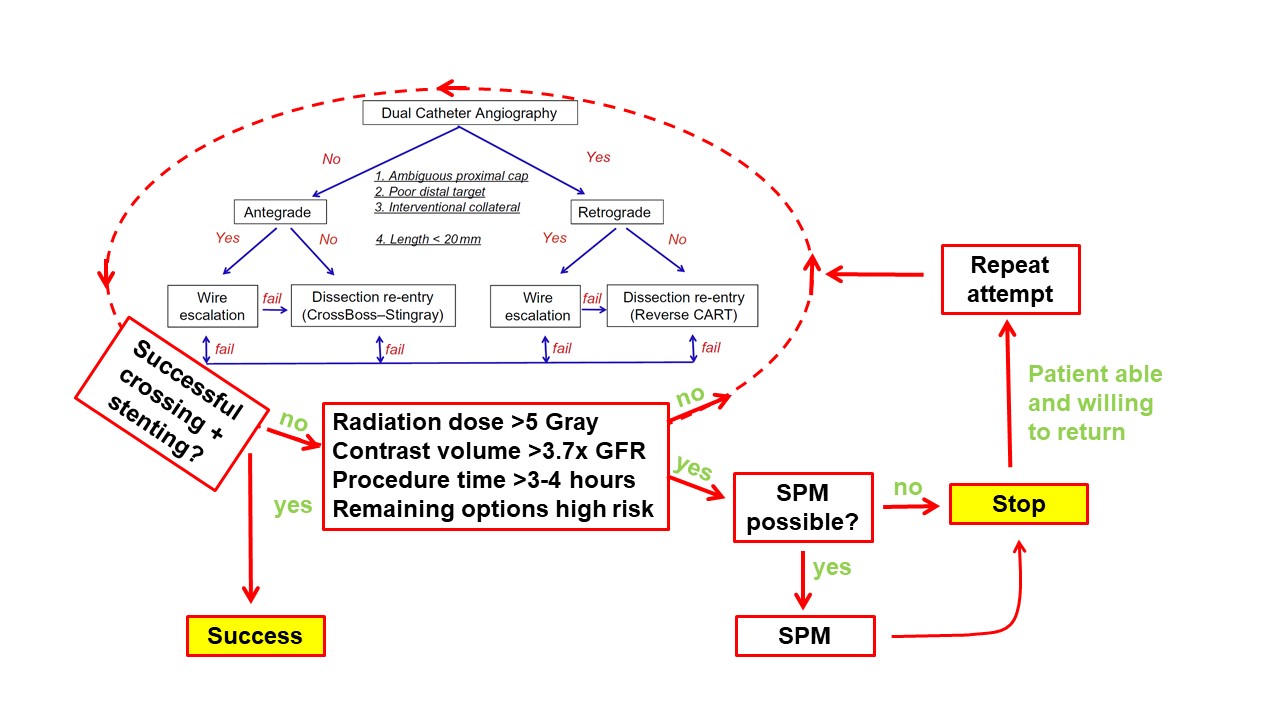
The “hybrid” algorithm for chronic total occlusion (CTO) percutaneous coronary intervention (PCI) was developed to guide selection of the optimal CTO crossing strategy in a stepwise fashion. Dual injection should be performed in nearly all CTO PCI procedures. Four angiographic lesion characteristics are assessed (1) proximal cap ambiguity, (2) quality of the distal vessel, (3) lesion length and (4) presence of collateral vessels suitable for the retrograde approach. Wire escalation is favored for <20 mm long lesions, whereas dissection and re-entry is favored for >20 mm long lesions. The antegrade approach is favored when the proximal cap is clear, and the retrograde approach is favored for lesions with an ambiguous proximal cap and/or diffusely diseased distal vessel, provided that appropriate collateral vessels are present. Early change of crossing strategy is recommended if the initially selected crossing strategy fails.
Rationale for the hybrid algorithm
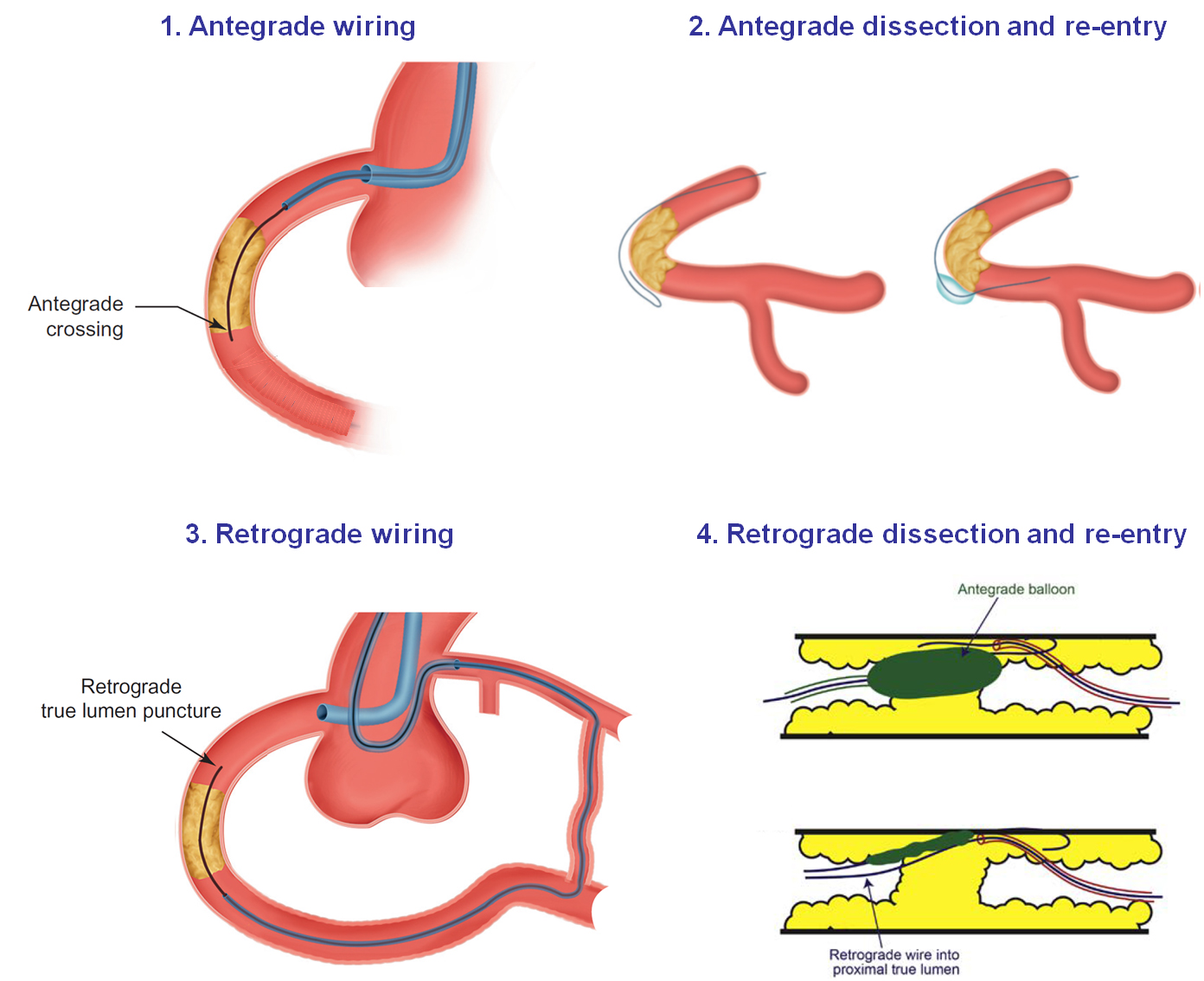
Several techniques have been developed for crossing coronary chronic total occlusions (CTOs). These techniques can be classified according to the direction of wire advancement (antegrade and retrograde) and use of the subintimal space (intraplaque wiring vs. dissection and reentry) (Figure 1) , , 1. Brilakis ES, Grantham JA, Rinfret S, Wyman RM, Burke MN, Karmpaliotis D, Lembo N, Pershad A, Kandzari DE, Buller CE, Demartini T, Lombardi WL and Thompson CA. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-79. Link2. Brilakis ES. Manual of Coronary Chronic Total Occlusion Interventions. A Step-By-Step Approach. 2nd edition: Elsevier; 2017. Link3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link. The CTO-ARC document recommends using the term “intraplaque” (for wire tracking within the occlusive intima-based plaque) and “extraplaque” (for wire tracking outside the plaque but still contained within the adventitial layer when describing the device course within the occluded CTO segment 4. Ybarra LF, Rinfret S, Brilakis ES, Karmpaliotis D, Azzalini L, Grantham JA, Kandzari DE, Mashayekhi K, Spratt JC, Wijeysundera HC, Ali ZA, Buller CE, Carlino M, Cohen DJ, Cutlip DE, De Martini T, Di Mario C, Farb A, Finn AV, Galassi AR, Gibson CM, Hanratty C, Hill JM, Jaffer FA, Krucoff MW, Lombardi WL, Maehara A, Magee PFA, Mehran R, Moses JW, Nicholson WJ, Onuma Y, Sianos G, Sumitsuji S, Tsuchikane E, Virmani R, Walsh SJ, Werner GS, Yamane M, Stone GW, Rinfret S, Stone GW and Chronic Total Occlusion Academic Research C. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation. 2021;143:479-500. Link.
In the antegrade approach the occlusion segment is approached from the proximal CTO cap with the intention of crossing the distal CTO cap into the distal true lumen 4. Ybarra LF, Rinfret S, Brilakis ES, Karmpaliotis D, Azzalini L, Grantham JA, Kandzari DE, Mashayekhi K, Spratt JC, Wijeysundera HC, Ali ZA, Buller CE, Carlino M, Cohen DJ, Cutlip DE, De Martini T, Di Mario C, Farb A, Finn AV, Galassi AR, Gibson CM, Hanratty C, Hill JM, Jaffer FA, Krucoff MW, Lombardi WL, Maehara A, Magee PFA, Mehran R, Moses JW, Nicholson WJ, Onuma Y, Sianos G, Sumitsuji S, Tsuchikane E, Virmani R, Walsh SJ, Werner GS, Yamane M, Stone GW, Rinfret S, Stone GW and Chronic Total Occlusion Academic Research C. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation. 2021;143:479-500. Link. In the retrograde approach the occlusion segment is approached from the distal CTO cap with the intention of accessing the proximal CTO cap into the proximal true lumen 4. Ybarra LF, Rinfret S, Brilakis ES, Karmpaliotis D, Azzalini L, Grantham JA, Kandzari DE, Mashayekhi K, Spratt JC, Wijeysundera HC, Ali ZA, Buller CE, Carlino M, Cohen DJ, Cutlip DE, De Martini T, Di Mario C, Farb A, Finn AV, Galassi AR, Gibson CM, Hanratty C, Hill JM, Jaffer FA, Krucoff MW, Lombardi WL, Maehara A, Magee PFA, Mehran R, Moses JW, Nicholson WJ, Onuma Y, Sianos G, Sumitsuji S, Tsuchikane E, Virmani R, Walsh SJ, Werner GS, Yamane M, Stone GW, Rinfret S, Stone GW and Chronic Total Occlusion Academic Research C. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation. 2021;143:479-500. Link.
Choosing the optimal technique for CTO crossing can be challenging and can be facilitated by an algorithmic approach. 1 The hybrid algorithm (Figure 2) was the first CTO crossing algorithm, developed in 2011 and published in 2012. Its goal has been to open the occluded vessel in the most safe, effective, and efficient way, tailoring all available crossing techniques to each specific case 1. Brilakis ES, Grantham JA, Rinfret S, Wyman RM, Burke MN, Karmpaliotis D, Lembo N, Pershad A, Kandzari DE, Buller CE, Demartini T, Lombardi WL and Thompson CA. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-79. Link. The “hybrid” approach has been used in a large number of cases both in the US , , , , , , , 5. Vo MN, McCabe JM, Lombardi WL, Ducas J, Ravandi A and Brilakis ES. Adoption of the hybrid CTO approach by a single non-CTO operator: procedural and clinical outcomes. J Invasive Cardiol. 2015;27:139-44. Link6. Christopoulos G, Karmpaliotis D, Alaswad K, Yeh RW, Jaffer FA, Wyman RM, Lombardi WL, Menon RV, Grantham JA, Kandzari DE, Lembo N, Moses JW, Kirtane AJ, Parikh M, Green P, Finn M, Garcia S, Doing A, Patel M, Bahadorani J, Tarar MN, Christakopoulos GE, Thompson CA, Banerjee S and Brilakis ES. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228. Link7. Michael TT, Mogabgab O, Fuh E, Patel VG, El Sabbagh A, Alomar ME, Rangan BV, Abdullah SM, Banerjee S and Brilakis ES. Application of the hybrid approach to chronic total occlusion interventions: a detailed procedural analysis. J Interv Cardiol. 2014;27:36-43. Link8. Christopoulos G, Menon RV, Karmpaliotis D, Alaswad K, Lombardi W, Grantham JA, Michael TT, Patel VG, Rangan BV, Kotsia AP, Lembo N, Kandzari DE, Lee J, Kalynych A, Carlson H, Garcia S, Banerjee S, Thompson CA and Brilakis ES. Application of the hybrid approach to chronic total occlusions in patients with previous coronary artery bypass graft surgery (from a Contemporary Multicenter US registry). Am J Cardiol. 2014;113:1990-4. Link9. Christopoulos G, Menon RV, Karmpaliotis D, Alaswad K, Lombardi W, Grantham A, Patel VG, Rangan BV, Kotsia AP, Lembo N, Kandzari D, Carlson H, Garcia S, Banerjee S, Thompson CA and Brilakis ES. The Efficacy and Safety of the Hybrid Approach to Coronary Chronic Total Occlusions: Insights From a Contemporary Multicenter US Registry and Comparison With Prior Studies. J Invasive Cardiol. 2014;26:427-32. Link10. Shammas NW, Shammas GA, Robken J, Harris T, Madison A, Dinklenburg C, Shammas AN, Harb C and Jerin M. The learning curve in treating coronary chronic total occlusion early in the experience of an operator at a tertiary medical center: The role of the hybrid approach. Cardiovasc Revasc Med. 2016;17:15-8. Link11. Pershad A, Eddin M, Girotra S, Cotugno R, Daniels D and Lombardi W. Validation and incremental value of the hybrid algorithm for CTO PCI. Catheter Cardiovasc Interv. 2014;84:654-9. Link12. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S and Brilakis ES. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention: Update From the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11:1325-1335. Link and in Europe , , 13. Wilson WM, Walsh SJ, Yan AT, Hanratty CG, Bagnall AJ, Egred M, Smith E, Oldroyd KG, McEntegart M, Irving J, Strange J, Douglas H and Spratt JC. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486-93. Link14. Maeremans J, Walsh S, Knaapen P, Spratt JC, Avran A, Hanratty CG, Faurie B, Agostoni P, Bressollette E, Kayaert P, Bagnall AJ, Egred M, Smith D, Chase A, McEntegart MB, Smith WH, Harcombe A, Kelly P, Irving J, Smith EJ, Strange JW and Dens J. The Hybrid Algorithm for Treating Chronic Total Occlusions in Europe: The RECHARGE Registry. J Am Coll Cardiol. 2016;68:1958-1970. Link15. Walsh SJ, Hanratty CG, McEntegart M, Strange JW, Rigger J, Henriksen PA, Smith EJ, Wilson SJ, Hill JM, Mehmedbegovic Z, Chevalier B, Morice MC and Spratt JC. Intravascular Healing Is Not Affected by Approaches in Contemporary CTO PCI: The CONSISTENT CTO Study. JACC Cardiovasc Interv. 2020;13:1448-1457. Link with high success rates and is also useful in learning and teaching CTO PCI. Additional algorithms, such as the Asia Pacific algorithm 16. Harding SA, Wu EB, Lo S, Lim ST, Ge L, Chen JY, Quan J, Lee SW, Kao HL and Tsuchikane E. A New Algorithm for Crossing Chronic Total Occlusions From the Asia Pacific Chronic Total Occlusion Club. JACC Cardiovasc Interv. 2017;10:2135-2143. Link and the EuroCTO algorithm 17. Galassi AR, Werner GS, Boukhris M, Azzalini L, Mashayekhi K, Carlino M, Avran A, Konstantinidis NV, Grancini L, Bryniarski L, Garbo R, Bozinovic N, Gershlick AH, Rathore S, Di Mario C, Louvard Y, Reifart N and Sianos G. Percutaneous recanalisation of chronic total occlusions: 2019 consensus document from the EuroCTO Club. EuroIntervention. 2019;15:198-208. Link were subsequently developed, adapting the key concepts of the hybrid algorithm to CTO PCI practices at various geographies. The hybrid algorithm continues to evolve incorporating novel equipment and techniques , 18. Hall AB and Brilakis ES. Hybrid 2.0: Subintimal plaque modification for facilitation of future success in chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. 2019;93:199-201. Link19. Riley RF, Walsh SJ, Kirtane AJ, Michael Wyman R, Nicholson WJ, Azzalini L, Spratt JC, Kalra S, Hanratty CG, Pershad A, DeMartini T, Karmpaliotis D, Lombardi WL and Aaron Grantham J. Algorithmic solutions to common problems encountered during chronic total occlusion angioplasty: The algorithms within the algorithm. Catheter Cardiovasc Interv. 2019;93:286-297. Link.
The first and most important step of CTO PCI is to perform dual coronary injection, in nearly all cases, unless there are no contralateral collaterals. Dual injection allows good visualization of both the proximal and distal vessel, as well as the collateral circulation, allowing selection of the most suitable initial crossing technique 2. Brilakis ES. Manual of Coronary Chronic Total Occlusion Interventions. A Step-By-Step Approach. 2nd edition: Elsevier; 2017. Link. Dual injection also clarifies the location of the guidewire(s) during crossing attempts and can facilitate management of complications, such as perforation 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link. In patients with ipsilateral-only collaterals, selective contrast injection in the collateral donor branch through a microcatheter can reduce contrast administration and reduce the risk of extending antegrade dissections 20. Azzalini L, Agostoni P, Benincasa S, Knaapen P, Schumacher SP, Dens J, Maeremans J, Kraaijeveld AO, Timmers L, Behnes M, Akin I, Toma A, Neumann FJ, Colombo A, Carlino M and Mashayekhi K. Retrograde Chronic Total Occlusion Percutaneous Coronary Intervention Through Ipsilateral Collateral Channels: A Multicenter Registry. JACC Cardiovasc Interv. 2017;10:1489-1497. Link. Since most coronary angiographies performed prior to CTO PCI do not include simultaneous injections, the CTO crossing plan should be re-assessed at the time of the procedure, after obtaining dual injections.
Step 2: Assessment of CTO characteristics
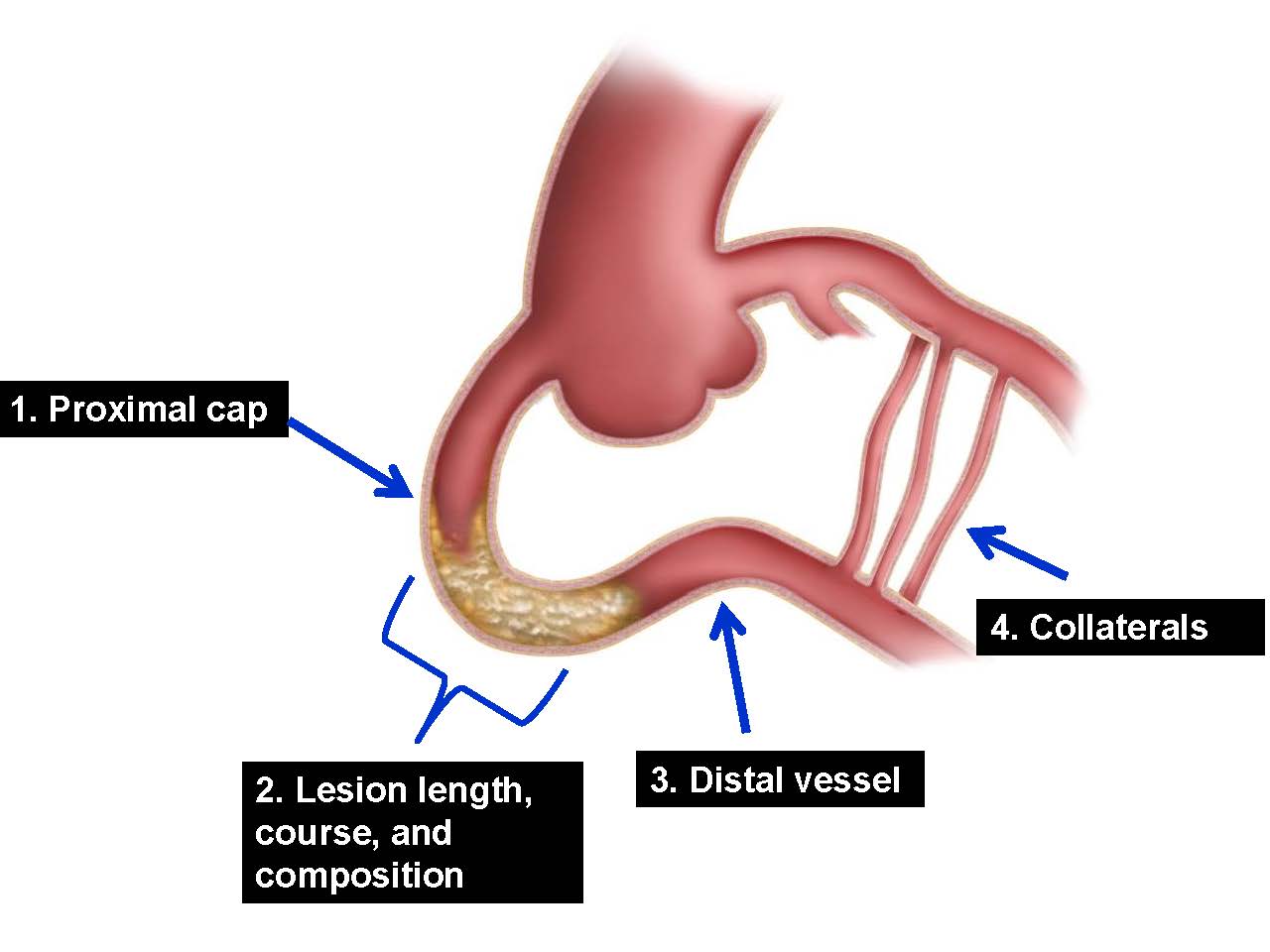
Detailed review of the coronary angiogram (and coronary computed tomography angiography, if available , 21. Ghoshhajra BB, Takx RAP, Stone LL, Girard EE, Brilakis ES, Lombardi WL, Yeh RW and Jaffer FA. Real-time fusion of coronary CT angiography with x-ray fluoroscopy during chronic total occlusion PCI. European radiology. 2017;27:2464-2473. Link22. Xenogiannis I, Jaffer FA, Shah A, Omer M, Megaly M, Vemmou E, Nikolakopoulos I, Rangan B, Garcia S, Lesser J, Cavalcante J, Burke MN and Brilakis ES. Computed Tomography Angiography Co-Registration with Real-Time Fluoroscopy in Chronic Total Occlusion Percutaneous Coronary Interventions. EuroIntervention. 2020. Link forms the basis for crossing strategy selection. Four angiographic parameters are assessed: (a) the morphology of the proximal cap; (b) the length and morphology (tortuosity, calcification, course ambiguity) of the occlusion; (c) the vessel size, quality and presence of bifurcations of the distal vessel; and (d) the location and suitability of collateral channels or bypass grafts for retrograde access (Figure 3) 1. Brilakis ES, Grantham JA, Rinfret S, Wyman RM, Burke MN, Karmpaliotis D, Lembo N, Pershad A, Kandzari DE, Buller CE, Demartini T, Lombardi WL and Thompson CA. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-79. Link:
Figure 3
Review of the coronary angiogram for planning CTO percutaneous coronary intervention.
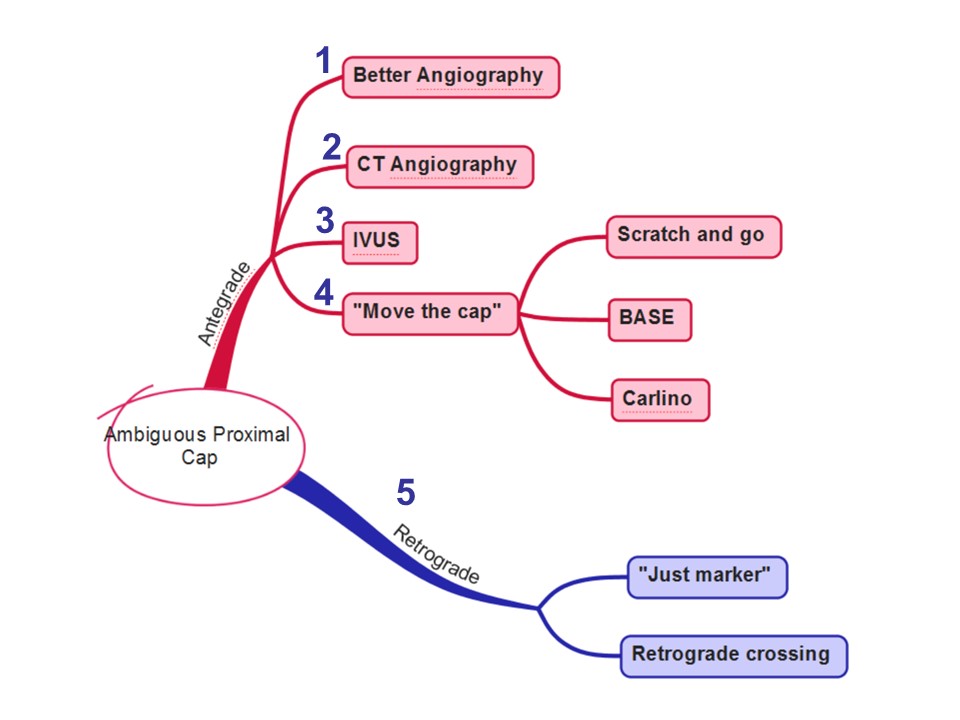
Clearly identifying the entry point to the occlusion is critical for crossing strategy selection, as advancing guidewires and microcatheters through an ambiguous proximal cap can cause perforation. Performing multiple angiographic projections, reviewing prior angiograms, performing intravascular ultrasound (if there is a side branch next the proximal cap) and contrast injection through a microcatheter located just proximal to the occlusion can help clarify the location of the proximal cap (Figure 4). Additional approaches to proximal cap ambiguity include dissection/reentry strategy proximal to the occlusion (“move the cap” techniques 23. Vo MN, Karmpaliotis D and Brilakis ES. Move the cap technique for ambiguous or impenetrable proximal cap of coronary total occlusion. Catheter Cardiovasc Interv. 2016;87:742-8. Link) and retrograde crossing.
Figure 4
Antegrade and retrograde approaches to CTOs with ambiguous proximal cap.
An ambiguous proximal cap increases the complexity of the procedure and decreases the likelihood of success 24. Christopoulos G, Kandzari DE, Yeh RW, Jaffer FA, Karmpaliotis D, Wyman MR, Alaswad K, Lombardi W, Grantham JA, Moses J, Christakopoulos G, Tarar MN, Rangan BV, Lembo N, Garcia S, Cipher D, Thompson CA, Banerjee S and Brilakis ES. Development and Validation of a Novel Scoring System for Predicting Technical Success of Chronic Total Occlusion Percutaneous Coronary Interventions: The PROGRESS CTO (Prospective Global Registry for the Study of Chronic Total Occlusion Intervention) Score. JACC Cardiovasc Interv. 2016;9:1-9. Link. A favorable proximal cap is one that is tapered, as opposed to blunt, and has no bridging collaterals or major side branches that could make engagement of the CTO segment difficult using traditional wire escalation techniques. A particularly challenging anatomic subset is that of flush aorto-ostial occlusions, which often require use of a primary retrograde approach.
2. Lesion length and morphology
Longer occlusions are often harder to cross. CTO lesion length is dichotomized into <20mm and ≥20mm long 25. Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, Ochiai M, Noguchi Y, Kato K, Shibata Y, Hiasa Y, Doi O, Yamashita T, Hinohara T, Tanaka H and Mitsudo K. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4:213-21. Link. Dual injection or coronary computed tomography angiography is needed for accurately assessing the occlusion length, which is usually overestimated when using single coronary injection.
Antegrade or retrograde crossing of short (<20 mm) CTOs is usually done with antegrade or retrograde wiring, whereas in long (≥20 mm) CTOs, dissection/re-entry techniques are often needed, especially for very long and tortuous occlusion segments. Lesion length <20 mm has been associated with faster CTO crossing in the J-CTO (Multicenter CTO Registry in Japan) registry 25. Morino Y, Abe M, Morimoto T, Kimura T, Hayashi Y, Muramatsu T, Ochiai M, Noguchi Y, Kato K, Shibata Y, Hiasa Y, Doi O, Yamashita T, Hinohara T, Tanaka H and Mitsudo K. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4:213-21. Link.
3. Distal vessel
A distal vessel of large caliber (>2.0 mm) that fills well, does not have significant disease and is free from calcification and major branches makes CTO recanalization easier 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link. Conversely, small, diffusely diseased, tortuous and calcified distal vessels are more challenging to recanalize, especially following subintimal guidewire entry. Some distal vessels are small due to hypoperfusion, leading to negative remodeling and often increase in size after recanalization 26. Galassi AR, Tomasello SD, Crea F, Costanzo L, Campisano MB, Marza F and Tamburino C. Transient impairment of vasomotion function after successful chronic total occlusion recanalization. J Am Coll Cardiol. 2012;59:711-8. Link. Distal CTO caps of native coronary artery CTOs in prior CABG patients are often calcified and resistant to guidewire penetration, as they have been exposed to systemic arterial pressure. Distal vessel calcification may hinder wire re-entry in case of subintimal guidewire entry.
4. Collateral circulation
Retrograde access to the distal vessel can be obtained via septal collaterals, epicardial collaterals (called non-septal in the CTO-ARC document 4. Ybarra LF, Rinfret S, Brilakis ES, Karmpaliotis D, Azzalini L, Grantham JA, Kandzari DE, Mashayekhi K, Spratt JC, Wijeysundera HC, Ali ZA, Buller CE, Carlino M, Cohen DJ, Cutlip DE, De Martini T, Di Mario C, Farb A, Finn AV, Galassi AR, Gibson CM, Hanratty C, Hill JM, Jaffer FA, Krucoff MW, Lombardi WL, Maehara A, Magee PFA, Mehran R, Moses JW, Nicholson WJ, Onuma Y, Sianos G, Sumitsuji S, Tsuchikane E, Virmani R, Walsh SJ, Werner GS, Yamane M, Stone GW, Rinfret S, Stone GW and Chronic Total Occlusion Academic Research C. Definitions and Clinical Trial Design Principles for Coronary Artery Chronic Total Occlusion Therapies: CTO-ARC Consensus Recommendations. Circulation. 2021;143:479-500. Link), or (patent or occluded) aortocoronary bypass grafts. Saphenous vein grafts , , 27. Kahn JK and Hartzler GO. Retrograde coronary angioplasty of isolated arterial segments through saphenous vein bypass grafts. Cathet Cardiovasc Diagn. 1990;20:88-93. Link28. Brilakis ES, Banerjee S and Lombardi WL. Retrograde recanalization of native coronary artery chronic occlusions via acutely occluded vein grafts. Catheter Cardiovasc Interv. 2010;75:109-13. Link29. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Potluri S, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Jaber W, Samady H, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Xenogiannis I, Stanberry LI, Rangan BV, Ungi I, Banerjee S and Brilakis ES. In-Hospital Outcomes of Chronic Total Occlusion Percutaneous Coronary Interventions in Patients With Prior Coronary Artery Bypass Graft Surgery. Circ Cardiovasc Interv. 2019;12:e007338. Link and septal collaterals are preferred over epicardial collaterals, as perforation of the latter is more likely to cause tamponade , , 30. Rathore S, Katoh O, Matsuo H, Terashima M, Tanaka N, Kinoshita Y, Kimura M, Tsuchikane E, Nasu K, Ehara M, Asakura K, Asakura Y and Suzuki T. Retrograde percutaneous recanalization of chronic total occlusion of the coronary arteries: procedural outcomes and predictors of success in contemporary practice. Circ Cardiovasc Interv. 2009;2:124-32. Link31. Benincasa S, Azzalini L, Carlino M, Bellini B, Giannini F, Zhao X and Colombo A. Outcomes of the retrograde approach through epicardial versus non-epicardial collaterals in chronic total occlusion percutaneous coronary intervention. Cardiovasc Revasc Med. 2017;18:393-398. Link32. Xenogiannis I, Tajti P, Hall AB, Alaswad K, Rinfret S, Nicholson W, Karmpaliotis D, Mashayekhi K, Furkalo S, Cavalcante JL, Burke MN and Brilakis ES. Update on Cardiac Catheterization in Patients With Prior Coronary Artery Bypass Graft Surgery. JACC Cardiovasc Interv. 2019;12:1635-1649. Link. Retrograde CTO PCI via left internal mammary grafts is sometimes feasible but carries high risk of complications 33. Tajti P, Karatasakis A, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Doing AH, Toma C, Uretsky B, Garcia S, Moses JW, Parikh M, Kirtane A, Ali ZA, Hatem R, Karacsonyi J, Danek BA, Rangan BV, Banerjee S, Ungi I and Brilakis ES. Retrograde CTO-PCI of Native Coronary Arteries Via Left Internal Mammary Artery Grafts: Insights From a Multicenter U.S. Registry. J Invasive Cardiol. 2018;30:89-96. Link. Optimal collateral vessels for retrograde CTO PCI 2. Brilakis ES. Manual of Coronary Chronic Total Occlusion Interventions. A Step-By-Step Approach. 2nd edition: Elsevier; 2017. Link:
Originate from a healthy (or repaired) donor vessel.
Can be easily accessed with wires and microcatheters.
Have minimal tortuosity 34. Huang CC, Lee CK, Meng SW, Hung CS, Chen YH, Lin MS, Yeh CF and Kao HL. Collateral Channel Size and Tortuosity Predict Retrograde Percutaneous Coronary Intervention Success for Chronic Total Occlusion. Circ Cardiovasc Interv. 2018;11:e005124. Link.
Have large caliber. The size of the collaterals is often assessed using the Werner classification (CC0: no continuous connection; CC 1: threadlike connection; CC2: side branch-like connection) 35. Werner GS, Ferrari M, Heinke S, Kuethe F, Surber R, Richartz BM and Figulla HR. Angiographic assessment of collateral connections in comparison with invasively determined collateral function in chronic coronary occlusions. Circulation. 2003;107:1972-7. Link. Crossing invisible septal collateral channels is often possible with the surfing technique, letting the wire find the path of least resistance 36. Dautov R, Urena M, Nguyen CM, Gibrat C and Rinfret S. Safety and effectiveness of the surfing technique to cross septal collateral channels during retrograde chronic total occlusion percutaneous coronary intervention. EuroIntervention. 2017;12:e1859-e1867. Link.
Are not the only (or dominant) source of flow to the CTO segment (which places the patient at risk for intraprocedural ischemia during crossing of the collateral).
Have favorable entry and exit angle, facilitating entry and exit of the guidewire.
Enter the CTO vessel distal to the distal cap.
More favorable collateral circulation characteristics make it easier to use retrograde techniques, both as the initial strategy or as an early crossover strategy. What constitutes an “interventional” collateral (i.e. a collateral that can be wired during a retrograde approach) depends on the experience and skills of the operator. In-depth understanding of the collateral circulation is important during antegrade crossing attempts, because dissection re-entry techniques and the formation of subintimal hematomas may compromise ipsilateral or bridging collaterals, leading to poor visualization of the distal vessel at the re-entry zone and occasionally ischemia.
Step 3: Antegrade Wiring
Antegrade wiring (also called antegrade wire escalation) is the most widely used CTO crossing technique , , , 12. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S and Brilakis ES. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention: Update From the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11:1325-1335. Link13. Wilson WM, Walsh SJ, Yan AT, Hanratty CG, Bagnall AJ, Egred M, Smith E, Oldroyd KG, McEntegart M, Irving J, Strange J, Douglas H and Spratt JC. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486-93. Link14. Maeremans J, Walsh S, Knaapen P, Spratt JC, Avran A, Hanratty CG, Faurie B, Agostoni P, Bressollette E, Kayaert P, Bagnall AJ, Egred M, Smith D, Chase A, McEntegart MB, Smith WH, Harcombe A, Kelly P, Irving J, Smith EJ, Strange JW and Dens J. The Hybrid Algorithm for Treating Chronic Total Occlusions in Europe: The RECHARGE Registry. J Am Coll Cardiol. 2016;68:1958-1970. Link37. Suzuki Y, Tsuchikane E, Katoh O, Muramatsu T, Muto M, Kishi K, Hamazaki Y, Oikawa Y, Kawasaki T and Okamura A. Outcomes of Percutaneous Coronary Interventions for Chronic Total Occlusion Performed by Highly Experienced Japanese Specialists: The First Report From the Japanese CTO-PCI Expert Registry. JACC Cardiovasc Interv. 2017;10:2144-2154. Link. Various guidewires are advanced in the antegrade direction (original direction of blood flow). Guidewire choice depends on the CTO characteristics. If there is a tapered proximal cap, a polymer-jacketed, low penetration force, tapered guidewire is used initially, with subsequent escalation to intermediate and high penetration force guidewires, if needed. If there is a blunt proximal cap, antegrade wiring is usually started with an intermediate penetration force polymer-jacketed guidewire, or a composite core guidewire. Stiff, high penetration force guidewires may be required in highly resistant proximal caps or when areas of resistance are encountered within the body of the occlusion. After crossing 1-2 mm through the proximal cap, de-escalation to less penetrating guidewires should follow before navigating through the CTO segment to minimize the risk of perforation 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link.
Step 4: Antegrade Dissection and Re-Entry
For long lesions approached in the antegrade direction, upfront use of a dissection/re-entry strategy is often recommended, especially in the presence of severe tortuosity or calcification. Dissection can be achieved either by advancing a “knuckle” formed at the tip of a polymer jacketed guidewire (such as the Gladius Mongo, Fielder XT, Bandit, Fighter, or Pilot 200) or by using the CrossBoss catheter (the CrossBoss catheter is currently mainly used for in-stent CTOs) 38. Karacsonyi J, Tajti P, Rangan BV, Halligan SC, Allen RH, Nicholson WJ, Harvey JE, Spaedy AJ, Jaffer FA, Grantham JA, Salisbury A, Hart AJ, Safley DM, Lombardi WL, Hira R, Don C, McCabe JM, Burke MN, Alaswad K, Koenig GC, Sanghvi KA, Ice D, Kovach RC, Varghese V, Murad B, Baran KW, Resendes E, Martinez-Parachini JR, Karatasakis A, Danek BA, Iwnetu R, Roesle M, Khalili H, Banerjee S and Brilakis ES. Randomized Comparison of a CrossBoss First Versus Standard Wire Escalation Strategy for Crossing Coronary Chronic Total Occlusions: The CrossBoss First Trial. JACC Cardiovasc Interv. 2018;11:225-233. Link. Antegrade dissection minimizes the risk for perforation (by the blunt guidewire loop or by the CrossBoss catheter tip) and allows for rapid crossing of long occlusion segments. Reentry into the distal true lumen is currently performed using the Stingray system in most cases, although novel wire-based techniques (such as antegrade fenestration and re-entry 39. Azzalini L, Alaswad K, Uretsky BF, Agostoni P, Galassi AR, Harada Ribeiro M, Filho EM, Morales-Victorino N, Attallah A, Gupta A, Zivelonghi C, Montorfano M, Bellini B and Carlino M. Multicenter experience with the antegrade fenestration and reentry technique for chronic total occlusion recanalization. Catheter Cardiovasc Interv. 2021;97:E40-E50. Link) and novel dual lumen microcatheters (such as the ReCross that has two over-the-wire lumens) can be useful in selected cases. Guidewire advancement distal to the distal cap should be minimized to reduce the risk of subintimal hematoma formation that can hinder reentry into the distal true lumen.
Step 5: The retrograde approach
The retrograde technique differs from the antegrade approach in that the occlusion is approached from the distal vessel with guidewire advancement against the original direction of blood flow , 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link40. Joyal D, Thompson CA, Grantham JA, Buller CEH and Rinfret S. The Retrograde Technique for Recanalization of Chronic Total Occlusions: a Step-by-Step Approach. JACC Cardiovasc Interv. 2012;5:1-11. Link. A guidewire is advanced into the artery distal to the occlusion through a collateral channel or through a bypass graft, followed by placement of a microcatheter at the distal CTO cap. Retrograde CTO crossing is then attempted either with retrograde wiring (usually for short occlusions, especially when the distal cap is tapered 41. Sakakura K, Nakano M, Otsuka F, Yahagi K, Kutys R, Ladich E, Finn AV, Kolodgie FD and Virmani R. Comparison of pathology of chronic total occlusion with and without coronary artery bypass graft. Eur Heart J. 2014;35:1683-93. Link) or using retrograde dissection/reentry techniques, most commonly the reverse controlled antegrade and retrograde tracking (reverse CART) technique. The retrograde wire can also facilitate antegrade wiring, acting as marker of the distal true lumen (“just marker” technique).
The retrograde approach is critical for achieving high success rates, especially in more complex occlusions, , 13. Wilson WM, Walsh SJ, Yan AT, Hanratty CG, Bagnall AJ, Egred M, Smith E, Oldroyd KG, McEntegart M, Irving J, Strange J, Douglas H and Spratt JC. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486-93. Link42. Christopoulos G, Wyman RM, Alaswad K, Karmpaliotis D, Lombardi W, Grantham JA, Yeh RW, Jaffer FA, Cipher DJ, Rangan BV, Christakopoulos GE, Kypreos MA, Lembo N, Kandzari D, Garcia S, Thompson CA, Banerjee S and Brilakis ES. Clinical Utility of the Japan-Chronic Total Occlusion Score in Coronary Chronic Total Occlusion Interventions: Results from a Multicenter Registry. Circ Cardiovasc Interv. 2015;8:e002171. Link however it is also associated with an increased risk of complications, such as myocardial infarction , , , 12. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S and Brilakis ES. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention: Update From the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11:1325-1335. Link43. Werner GS, Coenen A and Tischer KH. Periprocedural ischaemia during recanalisation of chronic total coronary occlusions: the influence of the transcollateral retrograde approach. EuroIntervention. 2014;10:799-805. Link44. Lo N, Michael TT, Moin D, Patel VG, Alomar M, Papayannis A, Cipher D, Abdullah SM, Banerjee S and Brilakis ES. Periprocedural myocardial injury in chronic total occlusion percutaneous interventions: a systematic cardiac biomarker evaluation study. JACC Cardiovasc Interv. 2014;7:47-54. Link45. Stetler J, Karatasakis A, Christakopoulos GE, Tarar MN, Amsavelu S, Patel K, Rangan BV, Roesle M, Resendes E, Grodin J, Abdullah S, Banerjee S and Brilakis ES. Impact of crossing technique on the incidence of periprocedural myocardial infarction during chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. 2016;88:1-6. Link, perforation and donor vessel injury , 46. Karmpaliotis D, Karatasakis A, Alaswad K, Jaffer FA, Yeh RW, Wyman RM, Lombardi WL, Grantham JA, Kandzari DE, Lembo NJ, Doing A, Patel M, Bahadorani JN, Moses JW, Kirtane AJ, Parikh M, Ali ZA, Kalra S, Nguyen-Trong PK, Danek BA, Karacsonyi J, Rangan BV, Roesle MK, Thompson CA, Banerjee S and Brilakis ES. Outcomes With the Use of the Retrograde Approach for Coronary Chronic Total Occlusion Interventions in a Contemporary Multicenter US Registry. Circ Cardiovasc Interv. 2016;9. Link47. El Sabbagh A, Patel VG, Jeroudi OM, Michael TT, Alomar ME, Mogabgab O, Fuh E, Roesle M, Rangan BV, Abdullah S, Hastings JL, Grodin J, Kumbhani DJ, Alexopoulos D, Fasseas P, Banerjee S and Brilakis ES. Angiographic success and procedural complications in patients undergoing retrograde percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 3,482 patients from 26 studies. Int J Cardiol. 2014;174:243-8. Link. Hence, approaching a CTO in the antegrade direction first is preferred in most cases, if feasible.
The retrograde approach can be used either upfront (primary retrograde) or after a failed antegrade crossing attempt , , , , , , , 30. Rathore S, Katoh O, Matsuo H, Terashima M, Tanaka N, Kinoshita Y, Kimura M, Tsuchikane E, Nasu K, Ehara M, Asakura K, Asakura Y and Suzuki T. Retrograde percutaneous recanalization of chronic total occlusion of the coronary arteries: procedural outcomes and predictors of success in contemporary practice. Circ Cardiovasc Interv. 2009;2:124-32. Link46. Karmpaliotis D, Karatasakis A, Alaswad K, Jaffer FA, Yeh RW, Wyman RM, Lombardi WL, Grantham JA, Kandzari DE, Lembo NJ, Doing A, Patel M, Bahadorani JN, Moses JW, Kirtane AJ, Parikh M, Ali ZA, Kalra S, Nguyen-Trong PK, Danek BA, Karacsonyi J, Rangan BV, Roesle MK, Thompson CA, Banerjee S and Brilakis ES. Outcomes With the Use of the Retrograde Approach for Coronary Chronic Total Occlusion Interventions in a Contemporary Multicenter US Registry. Circ Cardiovasc Interv. 2016;9. Link47. El Sabbagh A, Patel VG, Jeroudi OM, Michael TT, Alomar ME, Mogabgab O, Fuh E, Roesle M, Rangan BV, Abdullah S, Hastings JL, Grodin J, Kumbhani DJ, Alexopoulos D, Fasseas P, Banerjee S and Brilakis ES. Angiographic success and procedural complications in patients undergoing retrograde percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 3,482 patients from 26 studies. Int J Cardiol. 2014;174:243-8. Link48. Karmpaliotis D, Michael TT, Brilakis ES, Papayannis AC, Tran DL, Kirkland BL, Lembo N, Kalynych A, Carlson H, Banerjee S, Lombardi W and Kandzari DE. Retrograde coronary chronic total occlusion revascularization: procedural and in-hospital outcomes from a multicenter registry in the United States. JACC Cardiovasc Interv. 2012;5:1273-9. Link49. Tsuchikane E, Yamane M, Mutoh M, Matsubara T, Fujita T, Nakamura S, Muramatsu T, Okamura A, Igarashi Y and Oida A. Japanese multicenter registry evaluating the retrograde approach for chronic coronary total occlusion. Catheter Cardiovasc Interv. 2013;82:E654-61. Link50. Mashayekhi K, Behnes M, Valuckiene Z, Bryniarski L, Akin I, Neuser H, Neumann FJ and Reifart N. Comparison of the ipsi-lateral versus contra-lateral retrograde approach of percutaneous coronary interventions in chronic total occlusions. Catheter Cardiovasc Interv. 2016. Link51. Galassi AR, Sianos G, Werner GS, Escaned J, Tomasello SD, Boukhris M, Castaing M, Buttner JH, Bufe A, Kalnins A, Spratt JC, Garbo R, Hildick-Smith D, Elhadad S, Gagnor A, Lauer B, Bryniarski L, Christiansen EH, Thuesen L, Meyer-Gessner M, Goktekin O, Carlino M, Louvard Y, Lefevre T, Lismanis A, Gelev VL, Serra A, Marza F, Di Mario C, Reifart N and Euro CTOC. Retrograde Recanalization of Chronic Total Occlusions in Europe: Procedural, In-Hospital, and Long-Term Outcomes From the Multicenter ERCTO Registry. J Am Coll Cardiol. 2015;65:2388-400. Link52. Yamane M, Muto M, Matsubara T, Nakamura S, Muramatsu T, Oida A, Igarashi Y, Nozaki Y, Kijima M and Tuschikane E. Contemporary retrograde approach for the recanalisation of coronary chronic total occlusion: on behalf of the Japanese Retrograde Summit Group. EuroIntervention. 2013;9:102-9. Link. Factors that favor a primary retrograde approach include flush aorto-ostial or branch ostial occlusion, ambiguous proximal cap, distal cap at a bifurcation, poor distal vessel quality, good interventional collaterals, and also heavy calcification and chronic kidney disease (as the retrograde approach can often be performed using smaller amounts of contrast).
Step 6: Dynamic change in procedural strategies
Alternating between different crossing strategies enhances the success, safety, and efficiency of CTO PCI. If the initial or subsequent crossing strategy does not achieve progress, small changes (such as modifying the guidewire tip angulation or changing guidewire) or more significant changes (such as converting from antegrade wiring to antegrade dissection/reentry or the retrograde approach) should be made, based on pre-procedural planning and the evolution of the procedure , 1. Brilakis ES, Grantham JA, Rinfret S, Wyman RM, Burke MN, Karmpaliotis D, Lembo N, Pershad A, Kandzari DE, Buller CE, Demartini T, Lombardi WL and Thompson CA. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-79. Link16. Harding SA, Wu EB, Lo S, Lim ST, Ge L, Chen JY, Quan J, Lee SW, Kao HL and Tsuchikane E. A New Algorithm for Crossing Chronic Total Occlusions From the Asia Pacific Chronic Total Occlusion Club. JACC Cardiovasc Interv. 2017;10:2135-2143. Link. The operator should avoid getting “stuck in a failure mode”, in which excessive time, radiation and contrast are expended with little or no progress being made while repeatedly attempting the same technique. This may preclude the use of alternative strategies and increase the risk of complications 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link. Optimal application of the hybrid algorithm requires expertise with all crossing strategies, to minimize impediments to making a change.
Only approximately 50-60% of CTOs are successfully crossed with the initially selected crossing strategy , , , 12. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S and Brilakis ES. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention: Update From the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11:1325-1335. Link14. Maeremans J, Walsh S, Knaapen P, Spratt JC, Avran A, Hanratty CG, Faurie B, Agostoni P, Bressollette E, Kayaert P, Bagnall AJ, Egred M, Smith D, Chase A, McEntegart MB, Smith WH, Harcombe A, Kelly P, Irving J, Smith EJ, Strange JW and Dens J. The Hybrid Algorithm for Treating Chronic Total Occlusions in Europe: The RECHARGE Registry. J Am Coll Cardiol. 2016;68:1958-1970. Link20. Azzalini L, Agostoni P, Benincasa S, Knaapen P, Schumacher SP, Dens J, Maeremans J, Kraaijeveld AO, Timmers L, Behnes M, Akin I, Toma A, Neumann FJ, Colombo A, Carlino M and Mashayekhi K. Retrograde Chronic Total Occlusion Percutaneous Coronary Intervention Through Ipsilateral Collateral Channels: A Multicenter Registry. JACC Cardiovasc Interv. 2017;10:1489-1497. Link53. Xenogiannis I, Alaswad K, Krestyaninov O, Khelimskii D, Khatri JJ, Choi JW, Jaffer FA, Patel M, Mahmud E, Doing AH, Dattilo P, Koutouzis M, Tsiafoutis I, Uretsky B, Jefferson BK, Patel T, Jaber W, Samady H, Sheikh AM, Yeh RW, Tamez H, Elbaruny B, Love MP, Abi Rafeh N, Maalouf A, Fadi AJ, Toma C, Shah AR, Chandwaney RH, Omer M, Megaly MS, Vemmou E, Nikolakopoulos I, Rangan BV, Garcia S, Abdullah S, Banerjee S, Burke MN, Karmpaliotis D and Brilakis ES. Impact of adherence to the hybrid algorithm for initial crossing strategy selection in chronic total occlusion percutaneous coronary intervention. Rev Esp Cardiol (Engl Ed). 2020. Link. The timing and choice of subsequent crossing strategies depends on lesion characteristics, challenges encountered with the original technique, equipment availability and operator expertise , , 1. Brilakis ES, Grantham JA, Rinfret S, Wyman RM, Burke MN, Karmpaliotis D, Lembo N, Pershad A, Kandzari DE, Buller CE, Demartini T, Lombardi WL and Thompson CA. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5:367-79. Link3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link16. Harding SA, Wu EB, Lo S, Lim ST, Ge L, Chen JY, Quan J, Lee SW, Kao HL and Tsuchikane E. A New Algorithm for Crossing Chronic Total Occlusions From the Asia Pacific Chronic Total Occlusion Club. JACC Cardiovasc Interv. 2017;10:2135-2143. Link.
Step 7: When to stop
Reasons to stop a CTO-PCI attempt include:
occurrence of a complication
high radiation dose (usually >5 Gray air kerma dose in the absence of lesion crossing or substantial progress)
large contrast volume administration (>3.7x the estimated creatinine clearance)
exhaustion of crossing options, and
patient or physician fatigue 3. Brilakis ES, Mashayekhi K, Tsuchikane E, Abi Rafeh N, Alaswad K, Araya M, Avran A, Azzalini L, Babunashvili AM, Bayani B, Bhindi R, Boudou N, Boukhris M, Bozinovic NZ, Bryniarski L, Bufe A, Buller CE, Burke MN, Buttner HJ, Cardoso P, Carlino M, Christiansen EH, Colombo A, Croce K, Damas de Los Santos F, De Martini T, Dens J, Di Mario C, Dou K, Egred M, ElGuindy AM, Escaned J, Furkalo S, Gagnor A, Galassi AR, Garbo R, Ge J, Goel PK, Goktekin O, Grancini L, Grantham JA, Hanratty C, Harb S, Harding SA, Henriques JPS, Hill JM, Jaffer FA, Jang Y, Jussila R, Kalnins A, Kalyanasundaram A, Kandzari DE, Kao HL, Karmpaliotis D, Kassem HH, Knaapen P, Kornowski R, Krestyaninov O, Kumar AVG, Laanmets P, Lamelas P, Lee SW, Lefevre T, Li Y, Lim ST, Lo S, Lombardi W, McEntegart M, Munawar M, Navarro Lecaro JA, Ngo HM, Nicholson W, Olivecrona GK, Padilla L, Postu M, Quadros A, Quesada FH, Prakasa Rao VS, Reifart N, Saghatelyan M, Santiago R, Sianos G, Smith E, J CS, Stone GW, Strange JW, Tammam K, Ungi I, Vo M, Vu VH, Walsh S, Werner GS, Wollmuth JR, Wu EB, Wyman RM, Xu B, Yamane M, Ybarra LF, Yeh RW, Zhang Q and Rinfret S. Guiding Principles for Chronic Total Occlusion Percutaneous Coronary Intervention. Circulation. 2019;140:420-433. Link.
Continuous assessment of risk vs. benefit should guide decision-making and choice of strategy during various stages of the procedure. On many occasions, it may be best to fail rather than pursue highly aggressive strategies that may lead to serious complications 12. Tajti P, Karmpaliotis D, Alaswad K, Jaffer FA, Yeh RW, Patel M, Mahmud E, Choi JW, Burke MN, Doing AH, Dattilo P, Toma C, Smith AJC, Uretsky B, Holper E, Wyman RM, Kandzari DE, Garcia S, Krestyaninov O, Khelimskii D, Koutouzis M, Tsiafoutis I, Moses JW, Lembo NJ, Parikh M, Kirtane AJ, Ali ZA, Doshi D, Rangan BV, Ungi I, Banerjee S and Brilakis ES. The Hybrid Approach to Chronic Total Occlusion Percutaneous Coronary Intervention: Update From the PROGRESS CTO Registry. JACC Cardiovasc Interv. 2018;11:1325-1335. Link.
Step 8: CTO modification
CTO modification (often called subintimal plaque modification or “investment procedure”) can sometimes be used when CTO crossing attempts fail (for example due to failure to reenter into the distal true lumen or very distal guidewire reentry). CTO modification is performed by extraplaque balloon angioplasty with or without subintimal tracking and re-entry (STAR). CTO modification can facilitate subsequent CTO crossing attempts by modifying the plaque and creating dissection planes , 54. Hirai T, Grantham JA, Sapontis J, Cohen DJ, Marso SP, Lombardi W, Karmpaliotis D, Moses J, Nicholson WJ, Pershad A, Wyman RM, Spaedy A, Cook S, Doshi P, Federici R, Nugent K, Gosch KL, Spertus JA, Salisbury AC and Group OCS. Impact of subintimal plaque modification procedures on health status after unsuccessful chronic total occlusion angioplasty. Catheter Cardiovasc Interv. 2018;91:1035-1042. Link55. Xenogiannis I, Choi JW, Alaswad K, Khatri JJ, Doing AH, Dattilo P, Jaffer FA, Uretsky B, Krestyaninov O, Khelimskii D, Patel M, Mahmud E, Potluri S, Koutouzis M, Tsiafoutis I, Jaber W, Samady H, Jefferson BK, Patel T, Megaly MS, Hall AB, Vemmou E, Nikolakopoulos I, Rangan BV, Abdullah S, Garcia S, Banerjee S, Burke MN and Brilakis ES. Outcomes of subintimal plaque modification in chronic total occlusion percutaneous coronary intervention. Catheter Cardiovasc Interv. 2020;96:1029-1035. Link. The optimal interval for repeat crossing attempts is unclear at present but most operators wait for 6-8 weeks to allow healing of the dissections.
Conclusion
In summary, a systematic, algorithmic approach to CTO crossing that relies on dual coronary injection and careful angiographic review to select the initial and subsequent crossing strategies along with prompt change of approach when failing to achieve progress can help improve the success and efficiency and reduce the risk of complications of CTO PCI.
Personal perspective
Emmanouil Brilakis
The hybrid algorithm systematized the approach to CTO crossing using a logical step-by-step approach. It also streamlined training in CTO PCI at various practice settings and career stages , , , , , , , 5. Vo MN, McCabe JM, Lombardi WL, Ducas J, Ravandi A and Brilakis ES. Adoption of the hybrid CTO approach by a single non-CTO operator: procedural and clinical outcomes. J Invasive Cardiol. 2015;27:139-44. Link6. Christopoulos G, Karmpaliotis D, Alaswad K, Yeh RW, Jaffer FA, Wyman RM, Lombardi WL, Menon RV, Grantham JA, Kandzari DE, Lembo N, Moses JW, Kirtane AJ, Parikh M, Green P, Finn M, Garcia S, Doing A, Patel M, Bahadorani J, Tarar MN, Christakopoulos GE, Thompson CA, Banerjee S and Brilakis ES. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228. Link7. Michael TT, Mogabgab O, Fuh E, Patel VG, El Sabbagh A, Alomar ME, Rangan BV, Abdullah SM, Banerjee S and Brilakis ES. Application of the hybrid approach to chronic total occlusion interventions: a detailed procedural analysis. J Interv Cardiol. 2014;27:36-43. Link8. Christopoulos G, Menon RV, Karmpaliotis D, Alaswad K, Lombardi W, Grantham JA, Michael TT, Patel VG, Rangan BV, Kotsia AP, Lembo N, Kandzari DE, Lee J, Kalynych A, Carlson H, Garcia S, Banerjee S, Thompson CA and Brilakis ES. Application of the hybrid approach to chronic total occlusions in patients with previous coronary artery bypass graft surgery (from a Contemporary Multicenter US registry). Am J Cardiol. 2014;113:1990-4. Link9. Christopoulos G, Menon RV, Karmpaliotis D, Alaswad K, Lombardi W, Grantham A, Patel VG, Rangan BV, Kotsia AP, Lembo N, Kandzari D, Carlson H, Garcia S, Banerjee S, Thompson CA and Brilakis ES. The Efficacy and Safety of the Hybrid Approach to Coronary Chronic Total Occlusions: Insights From a Contemporary Multicenter US Registry and Comparison With Prior Studies. J Invasive Cardiol. 2014;26:427-32. Link10. Shammas NW, Shammas GA, Robken J, Harris T, Madison A, Dinklenburg C, Shammas AN, Harb C and Jerin M. The learning curve in treating coronary chronic total occlusion early in the experience of an operator at a tertiary medical center: The role of the hybrid approach. Cardiovasc Revasc Med. 2016;17:15-8. Link11. Pershad A, Eddin M, Girotra S, Cotugno R, Daniels D and Lombardi W. Validation and incremental value of the hybrid algorithm for CTO PCI. Catheter Cardiovasc Interv. 2014;84:654-9. Link13. Wilson WM, Walsh SJ, Yan AT, Hanratty CG, Bagnall AJ, Egred M, Smith E, Oldroyd KG, McEntegart M, Irving J, Strange J, Douglas H and Spratt JC. Hybrid approach improves success of chronic total occlusion angioplasty. Heart. 2016;102:1486-93. Link. Procedural success at centers experienced in hybrid CTO PCI is close to 90% with approximately 3% risk for major complications 6. Christopoulos G, Karmpaliotis D, Alaswad K, Yeh RW, Jaffer FA, Wyman RM, Lombardi WL, Menon RV, Grantham JA, Kandzari DE, Lembo N, Moses JW, Kirtane AJ, Parikh M, Green P, Finn M, Garcia S, Doing A, Patel M, Bahadorani J, Tarar MN, Christakopoulos GE, Thompson CA, Banerjee S and Brilakis ES. Application and outcomes of a hybrid approach to chronic total occlusion percutaneous coronary intervention in a contemporary multicenter US registry. Int J Cardiol. 2015;198:222-228. Link.
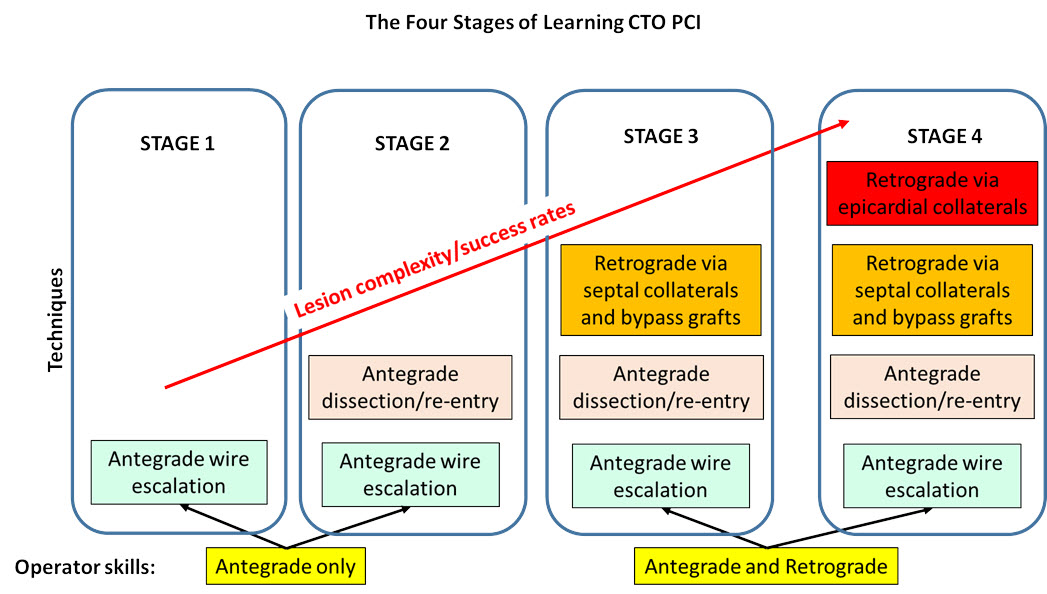
Successful application of the hybrid approach requires expertise in various CTO equipment and techniques. A common training pathway is to start with antegrade wire escalation, followed by antegrade dissection/reentry, retrograde via saphenous vein grafts and septal collaterals, and finally retrograde via epicardial collaterals (Figure 5) 56. Azzalini L and Brilakis ES. Ipsilateral vs. contralateral vs. no collateral (antegrade only) chronic total occlusion percutaneous coronary interventions: What is the right choice for your practice. Catheter Cardiovasc Interv. 2017;89:656-657. Link.
Achieving 100% success is unlikely to be achieved with current equipment and techniques without a significant increase in the incidence of complications 57. Brilakis ES, Xenogiannis I and Burke MN. Chronic total occlusion percutaneous coronary intervention: the road ahead. EuroIntervention. 2019;15:137-139. Link. The operator should continually assess the potential risks and benefits of implementing a new technique vs. continuing with the currently utilized technique. Determining the optimal duration for each step of the procedure depends heavily on operator experience.
There is an ongoing international collaboration for unifying the key principles of the hybrid and newer CTO crossing algorithms into a global algorithm that will further advance performance of CTO PCI and training in CTO PCI around the world.