Hybrid interventions
Summary
Hybrid treatment of cardiac patients consists in the intentional combination of techniques traditionally reserved to the catheterisation laboratory with techniques traditionally performed in the operating theatre. For multivessel coronary disease the combination of a minimally-invasive internal mammary graft and PCI with drug-eluting stents potentially offers the benefits of both treatments. A similar principle applies to mixed coronary and valvular disease with contemporary percutaneous and minimally-invasive techniques.
Key logistical features include access to a hybrid procedure room with the facilities of both a catheterisation laboratory and an operating theatre. Furthermore, communication and liason between cardiologists and surgeons must be excellent. This chapter focuses on various combinations of minimally invasive cardiac treatments, including percutaneous coronary intervention, valve implantation and endoscopic valve surgery. The goal of combining different techniques is to maximise patient’s comfort without compromising the outcome.
Definition and rationale
Hybrid approaches or strategies in cardiac patients can be defined as the intentional combination of techniques traditionally reserved for the catheterisation laboratory with techniques traditionally performed in the operating theatre. These hybrid approaches necessitate skills and competences classically displayed by both cardiovascular surgeons and interventional cardiologists. Each member of the “Heart Team” should fully understand the advantages and limitations of the various techniques. Ideally, they should be performed in dedicated rooms, namely “hybrid rooms” even though all parts of the hybrid approaches are not necessarily applied simultaneously. In most instances, the different steps of the hybrid strategy will not be performed simultaneously. Therefore, we believe that the term “hybrid strategy” is more appropriate that the term “hybrid intervention”.
In a minority of cases (i.e. very high comorbidity) a hybrid approach is the only possibility to help the patients. However, in general, the goal of combining different techniques is to maximise patient’s comfort without compromising the outcome. Therefore, a truly minimally invasive approach is intrinsic to the concept of hybrid strategies.
The concept of these hybrid strategies is not new but has been made technically possible and clinically meaningful by the recent advances in interventional cardiology and, even more so, by the major progresses made in minimally invasive surgery.
Very little clinical outcome data are available in the literature. It is unlikely that randomised data will be available in the near future, be it only because patients’ heterogeneity is very large. Moreover, the use of such procedures as institutional marketing tools - even though often not truly minimally invasive - further complicates the evaluation of these varied techniques. Therefore, the goal of this chapter is to discuss the possible advantages and drawbacks of the many possible combinations of interventional and minimally invasive surgical techniques.
Hybrid revascularisation in patients with multivessel disease
RESULTS
The rationale of contemplating a hybrid strategy in patients with multivessel coronary artery disease is based on the following reasons: (1) an internal mammary artery (IMA) on the left anterior descending (LAD) coronary artery prolongs survival and has shown outstanding long-term patency., , , , , , These IMA anastomoses can be safely performed by truly minimally invasive surgery, i.e. without sternotomy or extracorporeal circulation, with similar results compared with classic on-pump coronary artery by-pass graft (CABG) surgery,, , , , , while reducing the risk of perioperative complications;, , , , (2) in contrast, the occlusion rate of saphenous venous by-pass grafts (SVG) is higher , , , , , , than the restenosis rate in drug-eluting stents (DES), a procedure which can be considered an “arterial revascularisation”; , , , , , (3) it is commonly admitted that when the anatomy of the LAD stenoses is unfavourable for percutaneous coronary intervention (PCI) (long, calcified lesions, involving the ostial LAD as well as major bifurcations) the clinical outcome is better after IMA implantation than after PCI even in the DES era. , , , , , , Therefore, the clinical outcome after combined implantation of an IMA on the LAD (+/- first diagonal branch, D1) and PCI of the right coronary artery (RCA) and/or the left circumflex (LCx) coronary artery might well be not only as good but even better than after either classical open chest CABG involving venous by-pass grafts or multivessel PCI.
INDICATIONS
The ideal patients, who could benefit from these minimally invasive hybrid strategies, are those with one or more stenoses in the LAD not well suited for PCI and a good distal vascular bed and one or two stenoses in the RCA and/or the LCx amenable for stenting. When a large diagonal branch runs parallel to the LAD or when a large marginal branch runs on the antero-lateral part of the LV, the surgeon will in some cases be able to perform two arterial anastomoses. Additional elements that play a role in patients’ selection for hybrid revascularisation strategies are all (relative) contra-indications for sternotomy or double IMA implantation , , (Table 1).
Table 1
TECHNIQUES
Minimally invasive revascularisation surgery refers to a variety of techniques in which several alternative incisions to sternotomy have been proposed , , , , , . Yet, we believe that for a hybrid strategy to be meaningful, the treatment should be truly minimally invasive. This also implies that the IMA implantation should be performed on beating heart. Two surgical strategies are possible:
The first is the so-called (Robotically Enhanced) minimally invasive direct coronary artery by-pass (MIDCAB) procedure during which the IMA is harvested totally endoscopically (most often robotically assisted). Thereafter the hand-sewn anastomosis is performed through a small (4-6cm) left mini-thoracotomy without rib spreading (only soft tissue retraction). The fact that the ribs are not retracted plays a very important role in avoiding postoperative pain. With the help of a robot both IMA’s can be easily harvested from the left side. In case of anastomosis on the back side of the heart the latter can be performed under femoral extracorporeal circulatory (ECC) support (empty beating heart) to overcome haemodynamic instability when mobilising the heart in a closed chest. A second possible surgical technique is the totally endoscopic coronary artery by-pass (TECAB) with robotic harvesting as well as anastomosis of the IMA in a completely closed chest.
The key requirement in all of these approaches is the need for collaboration between cardiac surgeons and interventional cardiologists to obtain optimal patient outcome.
RESULTS
A number of small sized, single-centre or multicentre, retrospective series of hybrid myocardial revascularisation strategies , , , , , , , , , , , , , , , , , were recently reviewed by Popma et al .
Less than 400 patients have been reported so far. Even though the surgical technique varies widely and can no longer be called “minimally invasive” , the combination of the anastomosis of the IMA on the LAD (+/-D1) and PCI of non-LAD arteries is associated with a very low mortality . In the largest report of 117 patients , two high-risk patients died post operatively and the Kaplan-Meier survival was 92.5% at 1 year and 84.8% at 5 year. There was no death related to the PCI procedures. Follow-up angiography found one bypass occlusion and 5 in-stent restenoses in which re-PCI was performed at the time of planned control angiography. In a pilot series of patients in whom robotically enhanced MIDCAB was combined with PCI of the non-LAD vessels, there was no death and no clinically driven need for repeat-PCI .
TIMING
To be considered “hybrid”, the decision of combining surgical and interventional techniques as well as their respective sequence in time must be taken in advance by the Heart Team. The timing of interventions will depend on clinical, anatomical and logistical considerations. Three general approaches of revascularisation can be considered. The first is to stage the PCI 3 to 7 days after surgery. Dual (oral) antiplatelet therapy can be started after surgery, and the patient can be discharged the following day . This is the most straight-forward sequence and can be applied when the patient is stable or when the patient presents with an unstable coronary syndrome related to the LAD territory. The advantages of this sequence are that the patients are not under dual antiplatelet therapy for surgery and that the IMA can be checked angiographically prior to PCI.
The second option is to perform PCI several weeks in advance of surgery. This should be proposed to patients presenting with an unstable coronary syndrome related to non-LAD lesions. The disadvantage of this sequence is that surgery is performed while on dual antiplatelet therapy , . Alternatively, the thienopyridine derivate should be stopped which increases the risk of stent thrombosis . In our experience, we prefer to perform the MIDCAB intervention while on dual antiplatelet therapy when a DES has been used. When a bare metal stent (BMS) has been placed, surgical revascularisation is delayed by 8-10 weeks and performed after stopping the thienopyridine derivate. In addition, these decisions have to be weighed on a case-by-case basis depending on the amount of myocardium at risk as well as on technical details of the PCI procedure (i.e. total stent length, bifurcation, final result).
The third approach is one in which PCI is performed immediately after the surgical revascularisation, in the same session and in the same “hybrid room” , , . The availability of such a room is a ‘’sine qua non”, moreover the room itself requires not only the characteristics of an operating room and a state-of-the-art imaging equipment (including IVUS and haemodynamic monitoring capability), but also a specialised professional support for both the surgeon and the interventional cardiologist. Dual antiplatelet therapy can be given immediately before the intervention. Even though tempting conceptually, this approach remains logistically cumbersome. Figure 1 shows the example of a hybrid fractional flow reserve (FFR) guided hybrid revascularisation strategy (see figure legend).
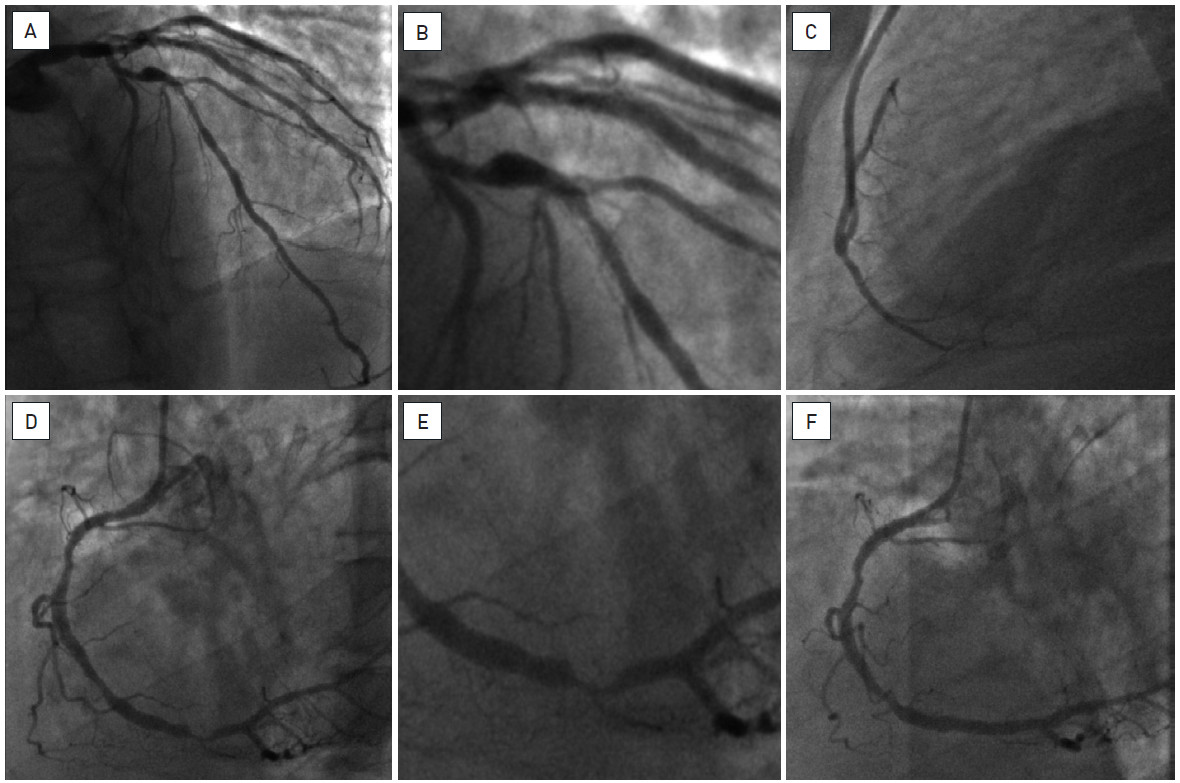
Figure 1
A forty-nine year old man, with previous stenting in the LAD and the LCx, presented with stable angina, Canadian Cardiovascular Society (CCS) class 2. Coronary angiography showed a diffusely diseased LAD (A) with severe in-stent re-stenosis (FFR 0.68) (B); the ostial lesion of the D1 was haemodynamically non-significant (FFR 0.95); there was also a significant (FFR 0.74) lesion of the distal RCA (D, E) while the LCx, although with diffuse atheromatosis, had no significant stenosis (FFR 0.84).
The hybrid therapy consisted in a MIDCAB procedure with LIMA on the LAD (C) followed after one week by PCI and stenting (DES) of the distal RCA (F). The patient had an uneventful clinical evolution and was free of symptoms 6 weeks later.
Combined valvular treatment and revascularisation
PRINCIPLE
Transcatheter aortic valve implantation (TAVI) has emerged as an alternative treatment for aortic stenosis , , .Similarly, Port Access endoscopic surgery has emerged as a minimally invasive but effective approach for mitral and tricuspid valve repair in patients with mitral/tricuspid regurgitation (MR/TR) but also for a variety of other pathologies (mitral valve replacement, subaortic myectomy, atrial septal defect repair, myxoma resection) classically treated by median sternotomy. Yet, in a sizeable proportion of patients, the presence of coronary artery disease (CAD) precludes these patients to benefit from minimally invasive techniques. In these cases the combination of PCI and a minimally invasive valvular procedure allows a minimally invasive treatment of these patients. In contrast we believe that once sternotomy is needed, there is no place for combining valvular surgery and PCI as the minimally invasive aspect would be lost.
COMBINED PCI AND TAVI
The prevalence of CAD is particularly high in elderly patients with an aortic stenosis , , , , , . PARTNER EU study reported an overall incidence of CAD of 60% for 130 patients included with previous CABG in 31.5% and previous PCI in 24.6% . While anecdotal cases have been reported , no sizeable series of patients undergoing simultaneously both TAVI and PCI have been described. Among the exclusion criteria of PARTNER trial were acute myocardial infarction (less than 14 days), unprotected left main disease (>=70%) as well as any therapeutic invasive cardiac procedure other than balloon valvuloplasty within 30 days .
It should be reminded that alleviating the aortic stenosis will theoretically improve coronary haemodynamics by increasing the driving coronary pressure and decreasing the metabolic needs of the myocardium (especially in the case of combined aortic stenosis and regurgitation). Therefore, there is a general consensus to disregard the presence of coronary stenoses in TAVI candidates when (1) angina is not the dominant symptom of the patient, and (2) there is no critical stenosis in the left main (LM), the proximal LAD or in the proximal dominant RCA/LCx. In case a revascularisation procedure is deemed necessary, the latter will be carried out prior to the TAVI intervention, which can be performed under dual antiplatelet therapy. Figure 2 shows a case of staged hybrid approach combining PCI and TAVI (see figure legend).
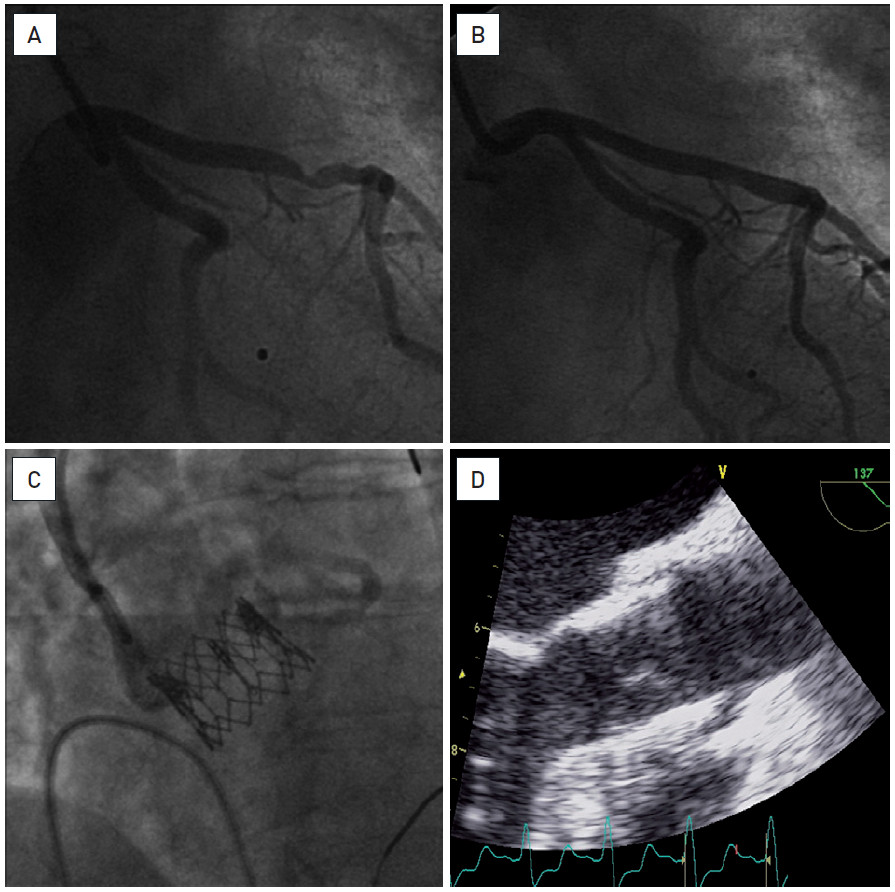
Figure 2
An eighty-eight year old woman admitted for complaints of angina (CCS 3) as well as increasing dyspnoea on exertion, New York Heart Association (NYHA) class 3. A critical aortic stenosis (mean gradient of 56 mmHg, calculated aortic valve area (AVA) of 0.5 cm²) was associated with one-vessel coronary artery disease (significant lesion of the mid-LAD) (A). Six weeks after PCI with stenting (DES) of mid-LAD (B), a TAVI procedure was successfully performed via the trans-femoral approach (26 mm Edwards SAPIEN™ transcatheter heart valve (THV)) (C, D). She had a good early and late post-procedural evolution. At one year follow-up the patient was in NYHA class 1, without angina. The aortic prosthesis had a normal function.
COMBINED PCI AND PORT ACCESS ENDOSCOPIC VALVULAR SURGERY
Albeit lower than in patients with aortic stenosis, the prevalence of significant CAD is not trivial in patients with mitral regurgitation. Between 1997 and October 2010, from the total of 2066 patients in whom Port Access mitral valve plasty/replacement (MVP/MVR) was considered at the OLV Clinic, 199 (9.6%) had CAD. The threshold to treat coronary lesions by PCI in patients undergoing Port Access surgery is lower than in TAVI candidates because (1) these patients are usually markedly younger than those undergoing TAVI; (2) in contrast to TAVI, coronary haemodynamics are not expected to improve after mitral valve repair, and (3) the presence of a critical stenosis might be problematic during the cardioplegia needed to repair the valve.
As for the combination of PCI and MIDCAB (see earlier), three different approaches can be considered: surgery first followed by PCI, PCI first followed by surgery or both techniques in the same session. When the stenosis in the epicardial artery appears to be very tight or when angina was present in daily life, PCI is performed prior to surgery, the latter being postponed by several weeks when possible. In all other cases, it is easier to perform mitral repair first and to plan PCI 3 to 5 days later, the patient being discharged the following day.
So far, the intentional combination of a PCI and port access endoscopic mitral valve repair has been performed in 43 patients in the OLV Clinic. After a mean follow-up of 28.8+/-25 months one non-cardiac death was reported, an endoscopic re-operation for mitral valve replacement was needed and two new PCI were registered, one being target vessel revascularisation. Figure 3 illustrates the case of a combined endoscopic mitral valve repair and PCI of the LAD (see figure legend).
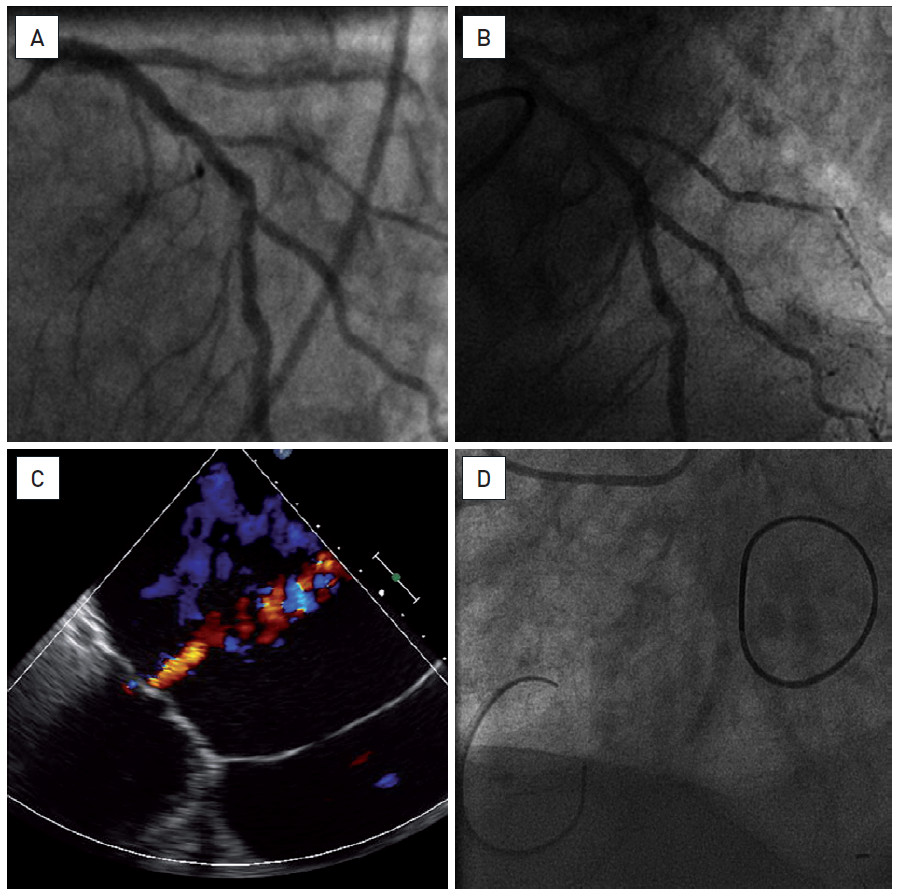
Figure 3
An eighty-three year old man referred for persistent symptoms of heart failure, NYHA class 3. The patient had severe MR, 3+/4 with massively dilated left atrium (more than 10 cm) (C), preserved LVEF and associated severe pulmonary hypertension. Coronary angiography showed a diffuse atherosclerosis with a short, calcified and haemodynamically significant (FFR 0.68) lesion of LAD at the bifurcation with D1 (A). The patient underwent an endoscopic MVP and tricuspid valvuloplasty (TVP) (D), followed, ten days later, by a PCI (DES) of the LAD (B). The clinical evolution was slow but favourable without major complications and he was discharged on day 12.
COMBINED TAVI AND ENDOSCOPIC VALVULAR SURGERY
More complex combinations of surgical and interventional procedures have recently been performed. These approaches are technically not particularly complicated but they illustrate the importance of an outstanding team approach including optimal logistical aspects. Two such examples are presented as follows in Figure 4 and Figure 5 . In the first patient PCI was followed by a TAVI and port access endoscopic mitral repair, all procedures being staged. In the second patients, port access mitral repair and transapical TAVI was performed during the same session. For details see the figure legend.
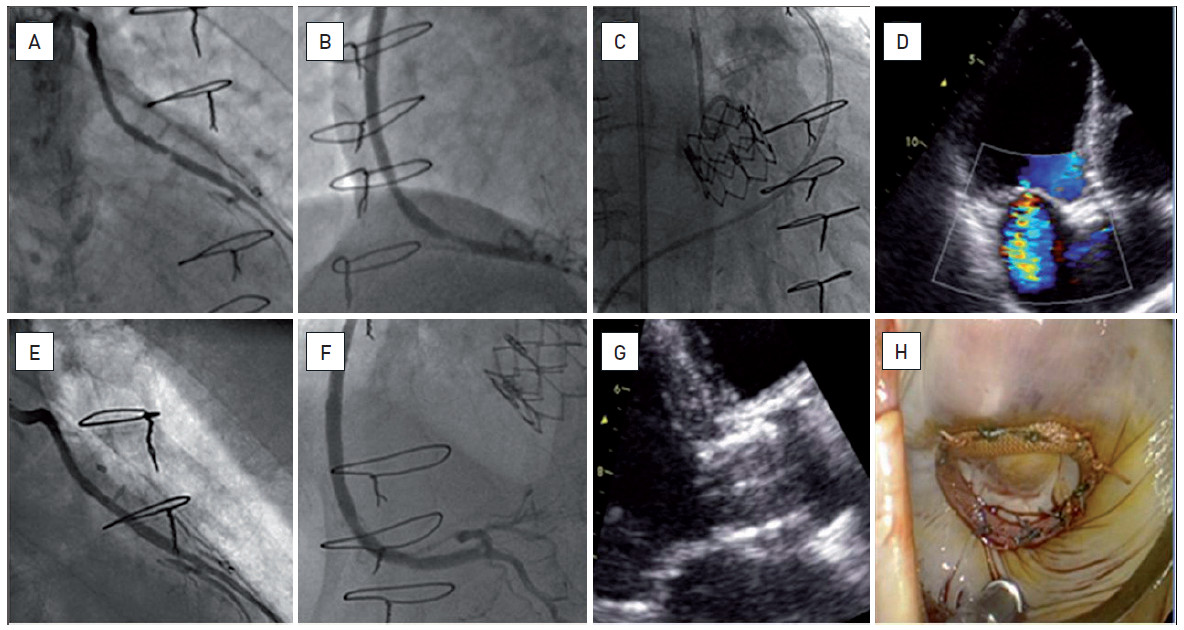
Figure 4
A seventy-five year old man with a long and complex history of coronary artery disease (re-do CABG followed by multiple, recurrent PCIs of the native vessels as well as of the grafts), symptomatic with effort angina and progressively increasing dyspnoea with episodes of acute pulmonary oedema. The presence of bi-valvular disease (severe aortic stenosis, mean gradient 52mmHg, estimated AVA of 0.72cm²; moderate/severe MR, 2-3/4) associated with new and haemodynamically significant lesions of the venous grafts (A, B) led our Heart Team advise a staged hybrid approach: PCI (E, F), followed by a trans-femoral TAVI procedure with implantation of a 26mm Edwards SAPIEN THV (C, G) and then by an endoscopic MVP (D, H). All interventions were completed with excellent functional results.
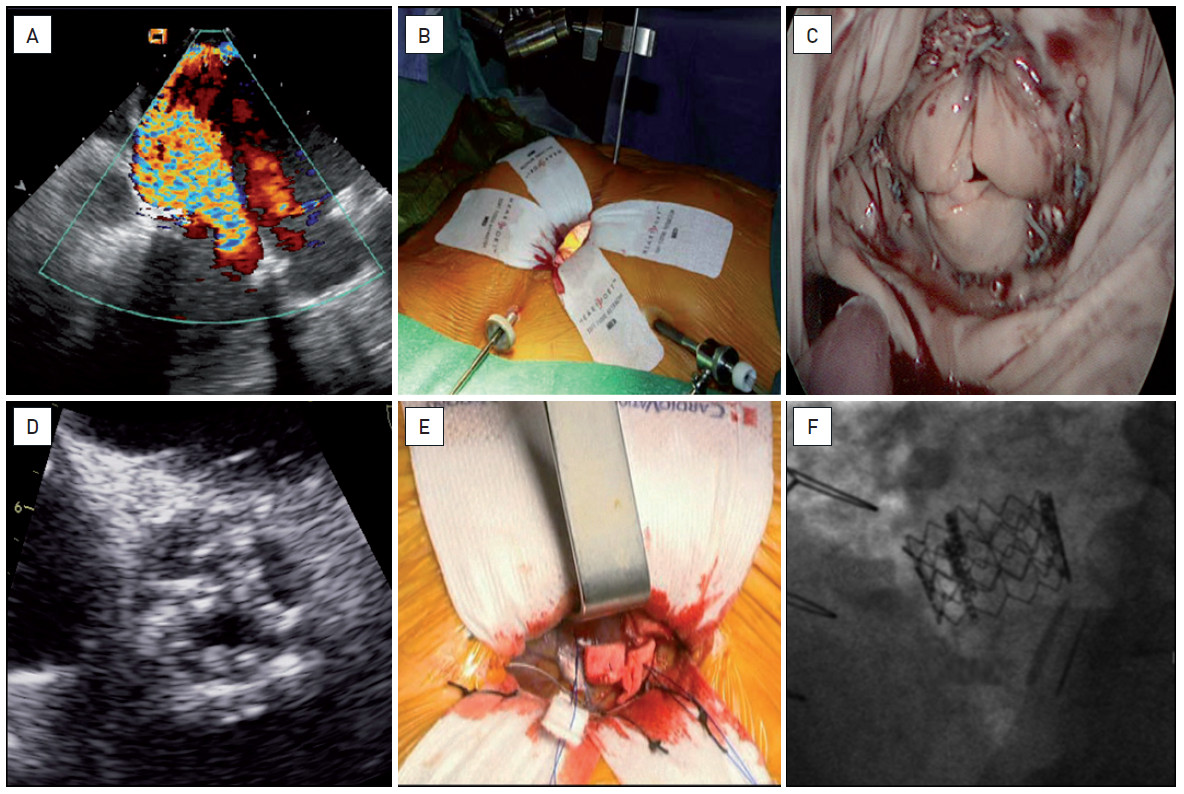
Figure 5
A seventy-seven year old woman with a history of previous cardiac surgery (MVR, TVP and supra-coronary replacement of the ascending aorta) was admitted for persistent symptoms of heart failure, NYHA class 3-4. She presented with complex valvular disease including massive MR (as result of degenerative changes of the mitral bioprosthesis) (A, C), severe TR and low-output low-gradient, though severe, aortic stenosis (D). With multiple comorbidities and a logistic EuroSCORE of 50%, she was referred for hybrid minimally invasive surgery with simultaneous endoscopic MVR/TVP (B) and trans-apical TAVI (E). The clinical evolution was favourable with discharge at day 15. The function of both valves (F) was normal.
Conclusion
Nowadays, a number of patients with coronary artery disease or with combined valvular and coronary disease can realistically be offered minimally invasive treatment strategies. Accurate invasive diagnostic techniques, the improved long-term patency of (drug-eluting) stents, increased success rate in chronic total occlusion treatment and the development of TAVI have increased the “yield” of transcatheter techniques. On the other hand, surgeons have drastically minimised the “invasive” character of their interventions, even though few centres master these technically demanding procedures. The awareness of the need for a Heart Team multidisciplinary decision approach, the improved common teaching at large meetings, as well as the collaboratively conducted research , , has further blurred the demarcation zone between two specialities which have been too often opposed to each other while having to take care of the same patients.
With the increased complexity of patients referred to the catheterisation laboratory and to surgery, a “hybrid thinking” to combine the best available tools of both specialties seems appealing to improve patients comfort and outcome.
Personal Perspective - Bernard De Bruyne
The improvement of techniques traditionally performed in the catheterisation laboratory or in the operation theatre have led to a better recognition of their relative merits, a better definition of their indications, and, finally, a growing awareness of the need for a common decision making process (“Heart teams”, multidisciplinary teams). Practically, these evolutions translate in treatment options intentionally combining surgical and interventional techniques as described in the present chapter. For the patients with complex problems of coronary artery disease and/or valvular heart disease, the hybrid strategies enable treatment in a much less “invasive” manner. A hybrid strategy can only be proposed to the patient if (1) the respective techniques are truly minimally invasive and (2) 'cross-talk' between interventionalists and surgeons is excellent. One has to acknowledge that clinical outcome data are scarce and that it will not be possible to perform randomised controlled trials because the clinical presentation of these patients is extremely varied and complex. The minimal invasiveness cannot justify the strategy on its own and it is our duty to ascertain that these new approaches indeed provide the patient with a satisfactory long term clinical outcome. Therefore, careful registration and analysis of the growing experience is mandatory.
It can be anticipated that departments will distinguish themselves not longer solely on the basis of expertise in techniques but in their possibility of providing combined approaches. Heart teams will have to think hybrid.
- The Task Force on Myocardial Revascularisation of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS), Guidelines on myocardial revascularisation. Eur Heart J. 2010;31:2501–2555.
- Parolari A, Alamanni F, Cannata A, Naliato M, Bonati L, Rubini P, Veglia F, Tremoli E, Biglioli P. Off-pump versus on-pump coronary artery bypass: meta-analysis of currently available randomized trials. Ann Thorac Surg. 2003;76:37-40.
- Serruys PW, Morice MC, Kappetein AP, Colombo A, Holmes DR, Mack MJ, Ståhle E, Feldman TE, van den Brand M, Bass EJ, Van Dyck N, Leadley K, Dawkins KD, and Mohr FW for the SYNTAX Investigators. Percutaneous Coronary Intervention versus Coronary-Artery Bypass Grafting for Severe Coronary Artery Disease. N Engl J Med. 2009;360:961-972.
- Byrne JG, Leacche M, Vaughan DE, Zhao DX. Hybrid cardiovascular procedures. JACC Cardiovasc Interv. 2008;1:459–468.
- Popma JJ, Nathan S, Hagberg RC and Khabbaz KR. Hybrid Myocardial Revascularisation: An Integrated Approach to Coronary Revascularisation. Catheter Cardiovasc Interv. 2010;75: S28–S34.
- Holzhey DM, Jacobs S, Mochalski M, Merk D, Walther T, Mohr FW, Falk V. Minimally invasive hybrid coronary artery revascularisation. Ann Thorac Surg. 2008;86:1856–1860.
- Davidavicius G, Van Praet F, Mansour S, Casselman F, Bartunek J, Degrieck I, Wellens F, De Geest R, Vanermen H, Wijns W, De Bruyne B. Hybrid revascularisation strategy: A pilot study on the association of robotically enhanced minimally invasive direct coronary artery bypass surgery and fractional-flow-reserve-guided percutaneous coronary intervention. Circulation. 2005;112:I317–I322.
- Lefèvre T, Kappetein AP, Wolner E, Nataf P, Thomas M, Schächinger V, De Bruyne B, Eltchaninoff H, Thielmann M, Himbert, Romano M, Serruys P, and Wimmer-Greinecker G on behalf of the PARTNER EU Investigator Group. One year follow-up of the multi-centre European PARTNER transcatheter heart valve study. Eur Heart J. 2011;32:48–157.
- Casselman F, van Slycke S, Wellens F, De Geest r, Degrieck I, Van Praet F, Vanermen H. Mitral valve surgery can now routinely be performed endoscopically. Circulation. 2003;108:II-48-II-54.
- Iung B, Baron G, Butchart E, Delahaye F, Gohlke-Bärwolf C, Levang OW, Tornos P, Vanoverschelde JL, Vermeer F, Boersma E, Ravaud P, Vahanian A. A prospective survey of patients with valvular heart disease in Europe: The Euro-Heart Survey on valvular Disease. Eur Heart J. 2003;24:1231-1243.