Medizinische Klinik Ill, Universitatsklinikum Heidelberg, Germany, Kerckhoff Heart and Thorax Center - Bad Nauheim, Germany, UKGM Giessen - Giessen, Germany, Medizinische Klinik Ill, Universitatsklinikum Heidelberg, Germany
In this chapter
Summary
Measurement of serological biomarkers before, during and after percutaneous coronary interventions for stable or acute coronary artery disease allows for insight into various complex pathophysiological processes which are involved in the progression of atherosclerosis and complications of percutaneous coronary interventions. Key to the proper use of biomarkers is an understanding of the fundamental principles of atherosclerosis and the mechanisms potentially involved in the transition from stable disease to spontaneous plaque disruption, as well as the mechanisms behind mechanically induced vessel wall trauma after balloon angioplasty and coronary stenting.
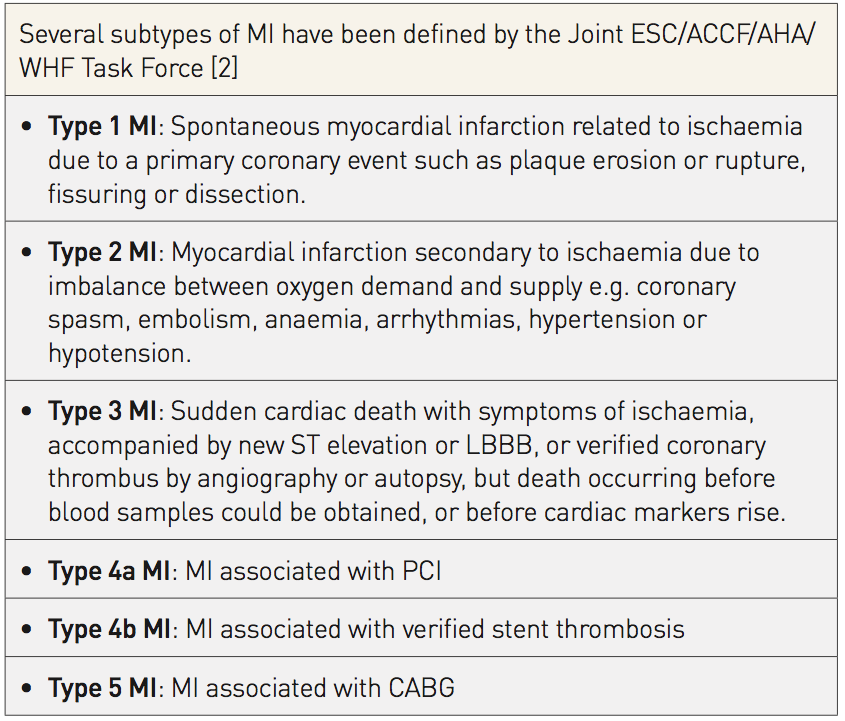
Cardiac troponins are recommended for the diagnosis of spontaneous MI and subtypes of MI, including type 4 MI (post-PCI) and type 5 MI (post-CABG), although there is still controversy regarding the magnitude of concentration rise that is prognostically relevant. New and more sensitive assay generations have been introduced to facilitate earlier and more accurate diagnosis of non-STEMI. These high sensitive cardiac troponin (hs-cTn) assays raise the question whether additional markers of early necrosis, such as myoglobin, ischaemia-modified albumin or heart-type fatty acid binding protein may be omitted. These biomarkers might confer independent information or add to the diagnostic and prognostic information already provided by cardiac troponins.
Biomarkers in acs
PATHOPHYSIOLOGY OF ACS
The aetiology of acute coronary syndromes (ACS) is complex and consists of multiple inter-related mechanisms, many of which are not yet fully understood. Our current understanding is that a plaque may rupture or erode in response to inflammation, leading to local occlusive or non-occlusive thrombus 1. Braunwald E. Unstable angina: an etiologic approach to management. Circulation. 1998; 98: 2219–22. Link.
Depending on the degree and reversibility of this dynamic obstruction, the clinical manifestations of ACS comprise a continuous spectrum of risk that progresses from unstable angina (UA) to non-ST-elevation myocardial infarction (non-STEMI) and ST-elevation myocardial infarction (STEMI). Non-STEMI is distinguished from UA by ischaemia sufficiently severe in intensity and duration to cause myocyte necrosis, which is recognised by the detection of troponin. This molecule is considered the preferred biomarker for detection of myocardial infarction due to its absolute cardiospecificity and superior sensitivity compared to cardiac enzymes or protein mass of CKMB.
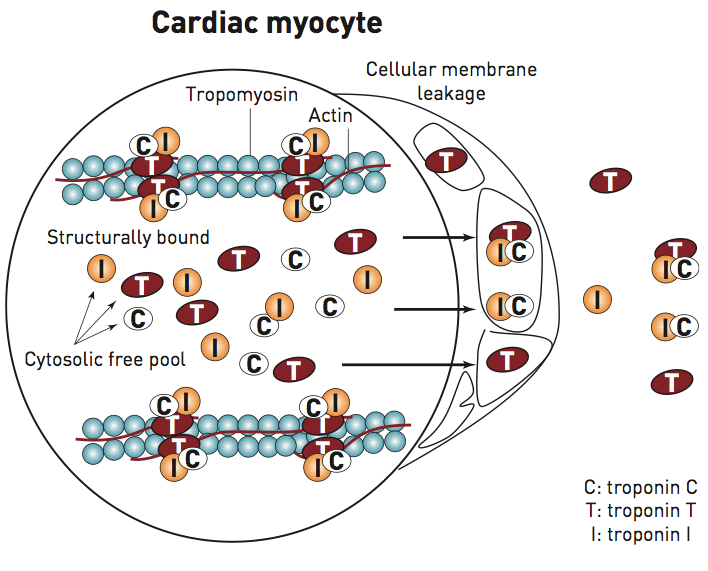
Cardiac troponin is composed of three subunits: T, I, and C, which are the products of different genes 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link. The total mass of the troponin complex is minuscule as compared to the protein mass of other myofibrillar proteins like actin and myosin. However, both troponin T and I are ideally suited for the detection of myocardial damage as they are expressed as cardio-specific isoforms, which are encoded by separate cardiac troponin T and I genes. The vast majority of the troponin complex is immobilised in the sarcomere of striated muscle and only a minor fraction exists as a soluble pool, which eventually represents a precursor pool of sarcomere assembly.
In patients with myocardial infarction distinct release kinetics have been described, with a rapidly appearing first peak resulting from the loosely bound troponin pool and a second long lasting elevation due to degradation of the contractile apparatus 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link. A biphasic pattern has been observed for cTnT whereas a monophasic release has been demonstrated for cTnI 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link. The exact reason for this difference in release kinetics remains elusive. cTnT differs from cTnI with respect to higher molecular weight, with a higher fraction of unbound cTnT and less degradation, whereas cTnI is more frequently found as binary or tertiary complexes in blood (Figure 1). There is evidence that the early appearing pool may give information on the quality of micro-vascular reperfusion, while the concentration of cTn on day 3 or 4 reflects myocardial infarct size 3. Giannitsis E, Steen H, Kurz K, Ivandic B, Simon AC, Futterer S, Schild C, Isfort P, Jaffe AS, Katus HA. Cardiac magnetic resonance imaging study for quantification of infarct size comparing directly serial versus single time-point measurements of cardiac troponin T. J Am Coll Cardiol. 2008; 51:307-14. Link. Experimental data strongly suggest that troponin leaks out of the cell only after membrane disruption following myocardial cell death 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link. The detection of a brief rise and subsequent fall of troponin concentration during marathon running 4. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002; 106:2871-2. Link and a rise after inducible myocardial ischaemia 4. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002; 106:2871-2. Link has cast some doubts on the hypothesis that troponin is released only upon irreversible damage. However, at this time there are neither consistent experimental nor clinical data providing proof of this concept.
Figure 1
Release of cardiac troponin from the structurally bound and the soluble pool after irreversible myocyte damage
Novel biomarkers of inflammation, activation of coagulation, myocyte necrosis, vascular damage and haemodynamic stress have the potential to enable a more differentiated characterisation of the individual components as well as their contribution at different stages of the disease, giving insights into the local consequences of percutaneous interventions in acute and stable coronary artery disease.
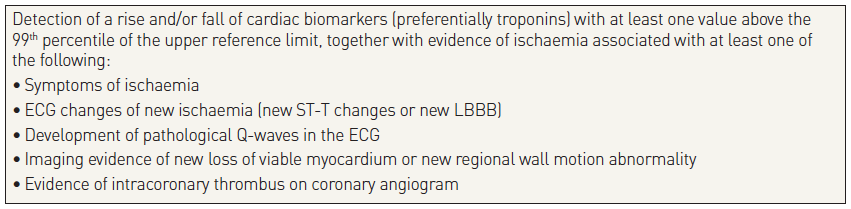
According to the 4th version of the Joint ESC/ACCF/AHA/WHF Task Force universal infarct definition 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link, the diagnosis of MI is based on the presence of:
an elevated cardiac troponin, which is considered the preferred biomarker indicating myocyte necrosis,
a dynamic change of biomarker concentration suggesting an acute rather than a chronic myocardial damage, and
the clinical context of acute myocardial ischaemia.
When troponin is not available, detection of a rise and/or fall of CKMB mass with at least one value above the 99th percentile of the upper reference limit measured with a coefficient of variation of < 10% is recommended.
There is a recent consensus recommendation 6. Thygesen K, Mair J, Giannitsis E, Mueller C, Lindahl B, Blankenberg S, Huber K, Plebani M, Biasucci LM, Tubaro M, Collinson P, Venge P, Hasin Y, Galvani M, Koenig W, Hamm C, Alpert JS, Katus H, Jaffe AS; Consensus Study Group on Biomarkers in Cardiology of ESC Working Group on Acute Cardiac Care. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur Heart J. 2012; 33: 2252-7. Link on the magnitude that defines a relevant rise and/or fall. If the baseline cTn is still below the upper limit of normal, i.e. the 99th percentile value of a healthy reference population, an acute myocardial injury can be assumed if the second troponin value exceeds the ULN and there is a change of 50% or more of the upper limit of normal. If the baseline value is already above the ULN a change of 20% or more from the baseline value is sufficient to diagnose an acute myocardial injury. The latter recommendation is based on a recommendation from the National Academy of Clinical Biochemistry (NACB) for patients with end-stage renal disease (ESRD) patients, and for all patients who may have baseline elevations of cTn, presenting with possible ACS, dynamic changes in the cTn values of 20% or more should be used to define AMI 7. Morrow DA, Cannon CP, Jesse RL, et al, Academy of Clinical Biochemistry laboratory medicine practice guidelines: clinical characteristics and utilization of biochemical markers in acute coronary syndromes. Clin Chem. 2007; 53: 552-574. Link. Implementation of serial concentration changes is paramount to distinguish acute from stable cTn level. Recent observations, however, have suggested that absolute changes may have greater diagnostic utility 8. Reichlin T, Irfan A, Twerenbold R, Reiter M, Hochholzer W, Burkhalter H, Bassetti S, Steuer S, Winkler K, Peter F, Meissner J, Haaf P, Potocki M, Drexler B, Osswald S and Mueller C. Utility of Absolute and Relative Changes in Cardiac Troponin Concentrations in the Early Diagnosis of Acute Myocardial InfarctionCirculation. 2011; 124: 136-145. Link. The increasing use of cardiac troponin assays with high sensitivity designation has facilitated more accurate and faster diagnosis. The 2020 ESC Guidelines 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link on NSTE-ACS recommend an ESC0/1 hour protocol over a 0/3 hour protocol if a hs-cTn assay is routinely available that has been validated in a clinical trial.
Spontaneous MI versus type 2 MI/MINOCA
While patients may fulfill the diagnostic criteria for MI, a substantial proportion does not show a plaque rupture with intracoronary thrombus causing obstruction of blood flow but disclose stenotic lesions without rupture or thrombus, coronary spasm, or normal coronary arteries. In particular, type 2 myocardial infarcts with luminal obstruction of 50% or less are labelled as myocardial infarction without obstructive coronary arteries (MINOCA). Long-term prognosis of type 2 MI is similarly adverse as type 1 MI and frequently driven by comorbidities or missed underlying pathologies. Therefore, additional diagnostic workup including contrast-enhanced magnetic resonance imaging is recommended to identify the most probable etiology including myocarditis, Tako Tsubo (stress) cardiomyopathy, cardioembolic reason, vasospastic angina or microvascular dysfunction 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link.
NON-ACS RELATED TROPONIN ELEVATION
Troponin is released following irreversible myocardial damage and not solely due to myocardial ischaemia. Thus, cardiac troponins (cTn) are tissue specific, indicating myocyte death, but not specific for ACS. Other frequent mechanisms of cardiac troponin release include tachy- and bradyarrhythmia, pulmonary embolism, inflammatory processes such as myocarditis, toxic agents or mechanical trauma (Table 2). A typical reason for chronically elevated cardiac troponin in asymptomatic patients is end-stage renal failure , 4. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002; 106:2871-2. Link5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link.
Patients with elevated cTn values should be followed closely since an elevated cTn indicates an adverse prognosis in almost all non-ACS pathologies. Some of these pathologies may also show a rising and/or falling pattern of cTn values which might hamper the interpretation of results. Patients without a changing pattern should not be diagnosed as having AMI or other acute reasons for the elevation. Some patients with stable CAD, chronic renal failure, chronic heart failure, and severe left ventricular hypertrophy can have chronic elevations of cTn which may or may not change markedly in the short term.
The introduction of more sensitive cardiac troponins (hsTn) has the advantage of detecting MI earlier and to identify a higher number of MI at decreasing numbers of unstable angina 13. Giannitsis E, Kurz K, Hallermayer K, et al. The new high sensitive cardiac troponin T assay. Clin Chem. 2010; 56: 254-6. Link. However, the most relevant obstacle for clinicians is that clinical specificity decreases as sensitivity increases 14. Giannitsis E, Katus HA. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol. 2013 Nov;10(11):623-34. Link. This phenomenon leads to an increased prevalence of troponin-positive patients. In this scenario, the clinical challenge is to discriminate ACS from a wide range of differential diagnoses associated with acute or chronic myocardial damage, particularly in the symptomatic patient.
CONVENTIONAL cTn ASSAYS
There are several cTnI assays but, due to patent limitations, there is only one cTnT assay (Roche Diagnostics) available on the market today. All available cTnI assays vary with respect to the epitope against which the detecting antibody is directed. In addition, there are several differences regarding the molecular weight, the predominant form of release and molecule stability at room temperature and after freezing. For conventional assays true false positives are very rare in the absence of heterophilic antibodies or severe haemolysis which may interfere with the troponin assay to cause either overestimation or underestimation of the true troponin concentration , 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link6. Thygesen K, Mair J, Giannitsis E, Mueller C, Lindahl B, Blankenberg S, Huber K, Plebani M, Biasucci LM, Tubaro M, Collinson P, Venge P, Hasin Y, Galvani M, Koenig W, Hamm C, Alpert JS, Katus H, Jaffe AS; Consensus Study Group on Biomarkers in Cardiology of ESC Working Group on Acute Cardiac Care. How to use high-sensitivity cardiac troponins in acute cardiac care. Eur Heart J. 2012; 33: 2252-7. Link. In contrast to cTnT, cardiac troponin I is susceptible to oxidation, reduction and phosphorylation which may affect epitope recognition and thus blood concentrations. In addition, prevalence of cTnT is considerably higher among patients with endstage renal failure than cTnI. In clinical routine, the diagnostic and prognostic performance of cTnT and cTnI are comparable, provided the test quality of the particular cTnI assay complies with quality specifications and has been validated in clinical trials. Among patients with ESRD, cTnT gives stronger prognostic information on outcomes than cTnI and should be preferred for this purpose. Despite enormous efforts to establish a reference material, a major obstacle in clinical routine using cTnI is the lack of standardisation between assays 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link.
The method of choice is quantitative measurement of cTn in the central laboratory. However, if results for cTn cannot be reported within 45 to 60 minutes after blood draw, the use of a quantitative point-of-care (POC) test is recommended for rule-in. Unfortunately, most POC test systems lack adequate analytical sensitivity and precision at the low end of the concentration range and bear the potential to miss a considerable number of small infarcts.
Recently, POC tests that meet high sensitivity designation have entered the market and allow the utilization of validated fast protocols 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link.
HIGH-SENSITIVITY CARDIAC TROPONINS
For many years, none of the commercially available cTn formulations used in the central laboratory met the precision requirements of the ESC/AHA infarct definition or the universal MI definition that mandated a total imprecision of 10% or less at the 99th percentile cut-off. Therefore, more sensitive, high-sensitive and ultrasensitive cTn assay generations were developed which are characterised by higher analytical sensitivity and improved analytical precision 13. Giannitsis E, Kurz K, Hallermayer K, et al. The new high sensitive cardiac troponin T assay. Clin Chem. 2010; 56: 254-6. Link. These novel cTn assays now allow detection of manifold lower cTn concentrations and meet the precision criteria. A scorecard system has been proposed to grade more sensitive assays into assays that only meet the precision criteria and truly sensitive assays that differ in the percentage of detectable troponin concentrations in healthy reference populations 15. Apple FS.A new season for cardiac troponin assays: it’s time to keep a scorecard. Clin Chem. 2009;55:1303-6. Link.
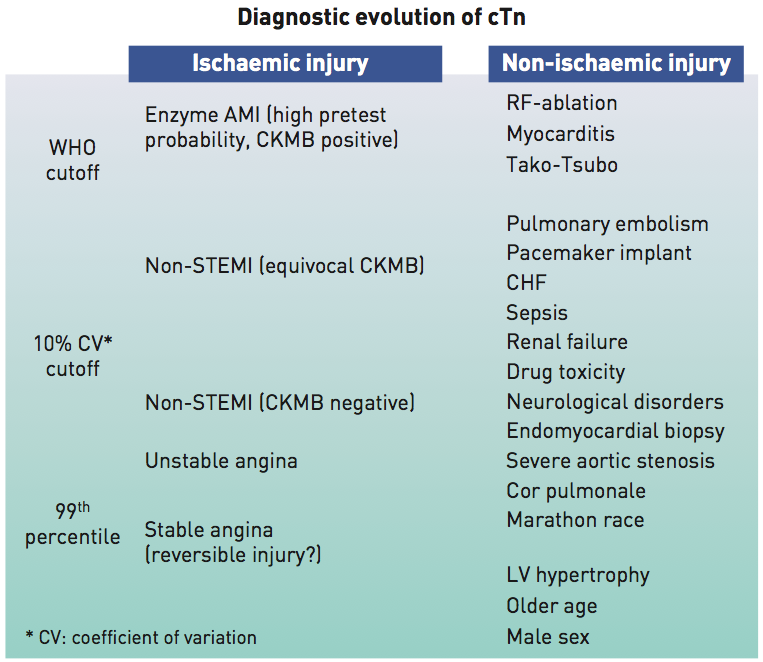
The magnitude of cTn may give some indirect information on the cause of elevation (Figure 2). Accordingly, small elevations may be seen with numerous cardiac and extra-cardiac pathologies, whereas very high concentrations are less likely with conditions other than myocardial infarction , , 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link4. Hamm CW, Giannitsis E, Katus HA. Cardiac troponin elevations in patients without acute coronary syndrome. Circulation. 2002; 106:2871-2. Link14. Giannitsis E, Katus HA. Cardiac troponin level elevations not related to acute coronary syndromes. Nat Rev Cardiol. 2013 Nov;10(11):623-34. Link.
Figure 2
Association between diagnostic threshold and detectable cardiovascular pathology
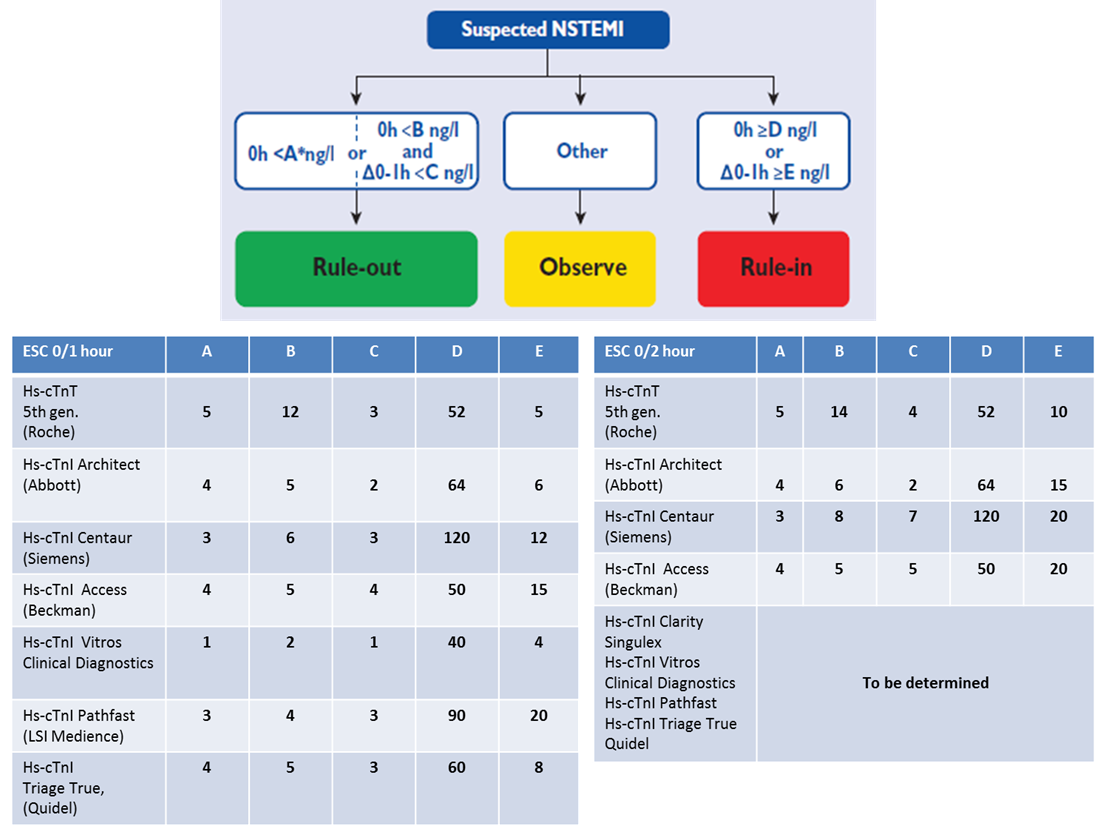
Use of more sensitive cTn assays at lower decision cut-offs has been found to reduce the time for the next blood draw from the recommended 6 to 9 hours after presentation to 1-3 hours 16. Chiang CH, Chiang CH, Pickering JW, Stoyanov KM, Chew DP, Neumann JT, Ojeda F, Sörensen NA, Su KY, Kavsak P, Worster A, Inoue K, Johannessen TR, Atar D, Amann M, Hochholzer W, Mokhtari A, Ekelund U, Twerenbold R, Mueller C, Bahrmann P, Buttinger N, Dooley M, Ruangsomboon O, Nowak RM, DeFilippi CR, Peacock WF, Neilan TG, Liu MA, Hsu WT, Lee GH, Tang PU, Ma KS, Westermann D, Blankenberg S, Giannitsis E, Than MP, Lee CC. Performance of the European Society of Cardiology 0/1-Hour, 0/2-Hour, and 0/3-Hour Algorithms for Rapid Triage of Acute Myocardial Infarction : An International Collaborative Meta-analysis. Ann Intern Med. 2022 Jan;175(1):101-113. Link. The ESC 0/1 hour and ESC 0/2 hour protocols demonstrate advantages over the 0/3 hour algorithm and should be preferred 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link. The use of the ESC 0/1 and ESC 0/2 hour algorithms have been optimized for sensitivity and specificity and triage patients into a “rule-out”, a “rule-in” zone and an “observational” zone, if neither criteria for rule-in or rule-out apply (Figure 3, upper panel). Of note, the protocols are specific for hs-cTnT and for each hs-cTnI assay. The 2020 ESC guidelines provide a table showing an overview on recommended and validated assays (Figure 3, lower panel). If patients present later than 3 hours after onset of symptoms, rule-out can be based on a single low hs-cTn below the limit of detection or a low troponin close to the limit of quantitation as proposed by the High-STEACS protocols 17. Shah AS, Anand A, Sandoval Y, Lee KK, Smith SW, Adamson PD, Chapman AR, Langdon T, Sandeman D, Vaswani A, Strachan FE, Ferry A, Stirzaker AG, Reid A, Gray AJ, Collinson PO, McAllister DA, Apple FS, Newby DE, Mills NL; High-STEACS investigators. High-sensitivity cardiac troponin I at presentation in patients with suspected acute coronary syndrome: a cohort study. Lancet. 2015 Dec 19;386(10012):2481-8. Link.
Figure 3
0 h/1 h rule-out and rule-in algorithm using high-sensitivity cardiac troponin assays in patients presenting with suspected non-ST-segment elevation acute coronary syndrome to the emergency department. Cut-offs are assay specific. The asterics denotes that a rule-out based on a single hs-cTn below the limit of detection (LoD) requires that the time from chest pain onset to the baseline blood draw exceeds 3 hours. Otherwise, the use of a serial protocol is mandated.
OTHER BIOMARKERS FOR EARLIER RULE-IN OR RULE-OUT OF MI (EARLY ISCHAEMIA MARKERS, COPEPTIN
The 2020 ESC Guidelines on the Management of NSTE-ACS do not recommend the use of additional biomarker for diagnosis of MI, provided a hs-cTn assay is routinely used. Copeptin, the C-terminal part of the vasopressin prohormone may represent an exception as more recently several investigators could demonstrate that copeptin improved the rapid ruling out of MI when tested together with cTn on presentation , 21. Maisel A, Mueller C, Neath SX, Christenson RH, Morgenthaler NG, McCord J, Nowak RM, Vilke G, Daniels LB, Hollander JE, Apple FS, Cannon C, Nagurney JT, Schreiber D, deFilippi C, Hogan C, Diercks DB, Stein JC, Headden G, Limkakeng ATJr, AnandI, Wu AH, Papassotiriou J, Hartmann O, Ebmeyer S, Clopton P, Jaffe AS, PeacockWF. Copeptin helps in the early detection of patients with acute myocardial infarction: primary results of the CHOPIN trial (Copeptin helps in the early detection of patients with acute myocardial infarction). J Am Coll Cardiol. 2013; 62: 150-60. Link22. Lipinski MJ, Escárcega RO, D’Ascenzo F, Magalhães MA, Baker NC, Torguson R, Chen F, Epstein SE, Miró O, Llorens P, Giannitsis E, Lotze U, Lefebvre S, Sebbane M, Cristol JP, Chenevier-Gobeaux C, Meune C, Eggers KM, Charpentier S, Twerenbold R, Mueller C, Biondi-Zoccai G, Waksman R. A systematic review and collaborative meta-analysis to determine the incremental value of copeptin for rapid rule-out of acute myocardial infarction. Am J Cardiol. 2014 May 1;113(9):1581-91. Link. A negative test result of copeptin in a patient with a negative cTn on presentation ruled-out MI with a NPV of 97.3%. The reason for the strikingly different performance of copeptin as compared to biomarkers of myocardial ischaemia is still unsettled. It has been hypothezised that copeptin reflects endogenous, life-threatening stress and haemodynamic changes as copeptin is secreted from the neurohypophysis in response to endogenous stress, different states of shock, and very early after the onset of myocardial ischaemia. However, due to the lack of cardiac specificity, copeptin has to be measured in addition to a cardio-specific troponin. Importantly, the Biomarkers-in-Cardiology 8 (BIC-8) study, a multicentre trial on 902 patients found that cTn negative patients at presentation randomized to an experimental copeptin arm could be safely discharged earlier, with rates of follow-up events comparable with the reference diagnostic protocol that requires repeat testing of cTn after 6 hours 18. Möckel M, Searle J, Hamm C, Slagman A, Blankenberg S, Huber K, Katus H, Liebetrau C, Müller C, Muller R, Peitsmeyer P, von Recum J, Tajsic M, Vollert JO, Giannitsis E. Early discharge using single cardiac troponin and copeptin testing in patients with suspected acute coronary syndrome (ACS): a randomized, controlled clinical process study. Eur Heart J. 2015 Feb 7;36(6):369-76. Link. In support of this randomized intervention trial, the ProCore registry conferred supportive evidence on the safety of early discharge from the ED in the real world setting among low-to-intermediate risk patients after instant rule-out of MI 19. Giannitsis E, Clifford P, Slagman A, Ruedelstein R, Liebetrau C, Hamm C, Honnart D, Huber K, Vollert JO, Simonelli C, Schröder M, Wiemer JC, Mueller-Hennessen M, Schroer H, Kastner K, Möckel M. Multicentre cross-sectional observational registry to monitor the safety of early discharge after rule-out of acute myocardial infarction by copeptin and troponin: the Pro-Core registry. BMJ Open. 2019 Jul 23;9(7):e028311. Link. Consistently, a pooled analysis added incremental evidence supporting the usefulness of a dual marker strategy, even when a normal hs-cTn is used in combination with a normal Copeptin 23. Giannitsis E, Slagman A, Hamm CW, Gehrig S, Vollert JO, Huber K. Copeptin combined with either non-high sensitivity or high sensitivity cardiac troponin for instant rule-out of suspected non-ST segment elevation myocardial infarction. Biomarkers. 2020 Dec;25(8):649-658. Link.
Compared to the ESC 0 hour pathway, the DMS strategy shows comparable diagnostic and prognostic performance but provides a 2.4-fold higher efficacy in terms of proportion of eligible patients eligible for the protocol 20. Giannitsis E, Huber K, Hamm CW, Möckel M. Instant rule-out of suspected non-ST-segment elevation myocardial infarction using high-sensitivity cardiac troponin T with Copeptin versus a single low high-sensitivity cardiac troponin T: findings from a large pooled individual data analysis on 10,329 patients. Clin Res Cardiol. 2021 Feb;110(2):194-199. Link.
At present, although there is still controversy regarding the added value of a normal Copeptin in combination with a hs-cTn 24. Giannitsis E, Blankenberg S, Christenson RH, Frey N, von Haehling S, Hamm CW, Inoue K, Katus HA, Lee CC, McCord J, Möckel M, Chieh JTW, Tubaro M, Wollert KC, Huber K. Critical appraisal of the 2020 ESC guideline recommendations on diagnosis and risk assessment in patients with suspected non-ST-segment elevation acute coronary syndrome. Clin Res Cardiol. 2021 Sep;110(9):1353-1368. Link, ESC guidelines recommend that Copeptin should be considered if a hs-cTn assay is not available 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link.
There are other biomarker that are of potential interest to be used as an adjunct to hs-cTn including myosin binding protein C, however, evidence is sparse and broader validation is required before routine use can be recommended.
BIOMARKERS FOR DETECTION OF COMPLICATIONS OF MI (REINFARCTION, MVO, INFARCT SIZE
Reinfarction
In patients in whom recurrent myocardial infarction is suspected from clinical signs or symptoms following the initial infarction, an immediate measurement of cardiac troponin is recommended. A second sample should be obtained 3 to 6 hours later. Recurrent infarction is diagnosed if there is a 20% or more increase in the value in the second sample 2. Thygesen K, Mair J, Katus H, Plebani M, Venge P, Collinson P, Lindahl B,Giannitsis E, Hasin Y, Galvani M, Tubaro M, Alpert JS, Biasucci LM, Koenig W, Mueller C, Huber K, Hamm C, Jaffe AS; Study Group on Biomarkers in Cardiology of the ESC Working Group on Acute Cardiac Care. Recommendations for the use of cardiac troponin measurement in acute cardiac care. Eur Heart J. 2010;31:2197-204. Link. This value should also exceed the 99th percentile for a control group. The usefulness of serial troponin measurements for detection of early reinfarction, particularly beyond the initial 48 hours has been demonstrated. The measurement of CKMB mass for detection of early reinfarction has recently been discouraged by expert consensus 25. Jaffe AS, Lindahl B, Giannitsis E, Mueller C, Cullen L, Hammarsten O, Mockel M, Mair J, Krychtiuk KA, Huber K, Mills NL, Thygesen K. ESC Study Group on Cardiac Biomarkers of the Association for Acute CardioVascular Care: A fond farewell at the retirement of CKMB. Eur Heart J. 2021 Jun 14;42(23):2260-2264. Link.
Microvascular obstruction
Microvascular obstruction (MVO) is thought to be related to peripheral embolisation of platelet microaggregates, intimal oedema, vasoconstriction, and/or leukocyte sticking. Irrespective of cause, experimental and clinical studies clearly demonstrate that MVO is associated with a greater degree of myocardial damage, more severely depressed LV function and a higher mortality 26. Wu KC, Zerhouni EA, Judd RM, Lugo-Olivieri CH, Barouch LA, Schulman SP, Blumenthal RS, Lima JA.Prognostic significance of microvascular obstruction by magnetic resonanceimaging in patients with acute myocardial infarction. Circulation. 1998; 97:765-72. Link. Accordingly, significantly higher concentrations of cardiac cTn have been found in the presence of MVO, and the levels of early cTn release correlate with transmurality of infarction, infarct size and magnitude of MVO 27. Neizel M, Futterer S, Steen H, Giannitsis E, Reinhardt L, Lossnitzer D, Lehrke S, Jaffe AS, Katus HA. Predicting microvascular obstruction with cardiac troponin T after acute myocardial infarction: a correlative study with contrast-enhanced magnetic resonance imaging. Clin Res Cardiol. 2009; 98: 555-62. Link. However, there is not enough evidence to recommend measurement of cardiac troponin for identification of microvascular obstruction, at present.
Infarct size
Animal experiments and human studies using thallium SPECT and contrast-enhanced MRI demonstrated an excellent correlation between infarct size and cTn concentrations. Any single cTn measurement between 24 and 96 hours after the onset of symptoms may be used to estimate infarct size , , 3. Giannitsis E, Steen H, Kurz K, Ivandic B, Simon AC, Futterer S, Schild C, Isfort P, Jaffe AS, Katus HA. Cardiac magnetic resonance imaging study for quantification of infarct size comparing directly serial versus single time-point measurements of cardiac troponin T. J Am Coll Cardiol. 2008; 51:307-14. Link28. Vogel B, Claessen BE, Arnold SV, Chan D, Cohen DJ, Giannitsis E, Gibson CM, Goto S, Katus HA, Kerneis M, Kimura T, Kunadian V, Pinto DS, Shiomi H, Spertus JA, Steg PG, Mehran R. ST-segment elevation myocardial infarction. Nat Rev Dis Primers. 2019 Jun 6;5(1):39. Link29. Steen H, Giannitsis E, Futterer S, Merten C, Juenger C, Katus HA. Cardiac troponin T at 96 hours after acute myocardial infarction correlates with infarct size and cardiac function. J AmCollCardiol. 2006; 48:2192-4. Link. However, it should be noted that correlation between infarct size and level of cTnT or cTnI is excellent for large STEMI but is less impressive for the heterogeneous group of non-STEMI and for small infarcts 3. Giannitsis E, Steen H, Kurz K, Ivandic B, Simon AC, Futterer S, Schild C, Isfort P, Jaffe AS, Katus HA. Cardiac magnetic resonance imaging study for quantification of infarct size comparing directly serial versus single time-point measurements of cardiac troponin T. J Am Coll Cardiol. 2008; 51:307-14. Link. Although serial measurements performed as effective as single one point protocols, the latter may have a better acceptance for clinical practice as a simple algorithm is more convenient and more cost-effective than serial measurements.
PROGNOSIS
The role of cardiac troponins for risk assessment in suspected ACS is well established. The presence of elevated cardiac troponin in blood indicates the antecedent occurrence of plaque rupture with subsequent embolisation of platelet micro- or macro-aggregates from the ruptured plaque to the periphery causing obstruction of the capillaries with ensuing myocardial necrosis. As a mirror of platelet activation and representative for a pro-thrombotic milieu, an elevated troponin predicts a higher acute (thrombotic) risk for (re-)infarction and death. In addition, the presence of elevated cTn has been linked to more severe atherosclerotic disease, more prevalent triple coronary artery disease, left main disease, and more severely depressed left ventricular function 30. Frey N, Dietz A, Kurowski V, Giannitsis E, Tölg R, Wiegand U, Richardt G, Katus HA. Angiographic correlates of a positive troponin T test in patients with unstable angina. Crit Care Med. 2001; 29:1130-6. Link. Therefore, the prognostic significance of a cTn elevation during the index event persists for years reflecting the persistence of vulnerable plaque.
Other biomarkers which indicate persistence of a chronic underlying inflammatory process such as fibrinogen and C-reactive protein have also been found to predict an adverse long-term outcome. These markers confer additive and independent prognostic information to cardiac troponin 31. Armstrong EJ, Morrow DA, Sabatine MS. Inflammatory biomarkers in acute coronary syndromes: part I: introduction and cytokines. Circulation. 2006;113: e72-5. Link.
A large body of evidence has also confirmed that concentrations of natriuretic peptides (BNP, NT-proBNP) are elevated across the entire spectrum of ACS and that the magnitude of this increase closely correlates with outcomes 32. James SK, Lindbäck J, Tilly J, Siegbahn A, Venge P, Armstrong P, Califf R, Simoons ML, Wallentin L, Lindahl B. Troponin-T and N-terminal pro-B-type natriuretic peptide predict mortality benefit from coronary revascularization in acute coronary syndromes: a GUSTO-IV substudy. J Am Coll Cardiol. 2006; 48: 1146-54. Link. The reasons for natriuretic peptides increase following ACS are multiple, including haemodynamic stress and volume overload due to acute heart failure. However, there is also evidence from experimental studies showing that expression of B-type natriuretic peptides (BNP and NT-proBNP) may be stimulated directly or indirectly by myocardial ischaemia 33. Goetze JP, Gore A, Moller CH, Steinbruchel DA, Rehfeld JF, Nielsen LB. Acute myocardial hypoxia increases BNP gene expression. FASEB J. 2004; 18: 1928-30. Link.
Natriuretic peptides were found to predict adverse outcomes independently and add prognostic information to established risk predictors such as renal function, levels of C-reactive protein and cTn 34. Wollert KC, Kempf T, Peter T, Olofsson S, James S, Johnston N, Lindahl B, Horn-Wichmann R, Brabant G, Simoons ML, Armstrong PW, Califf RM, Drexler H, Wallentin L. Prognostic value of growth-differentiation factor-15 in patients with non-ST-elevation acute coronary syndrome. Circulation. 2007; 115: 962-71. Link. Eventually, the combination of NT-pro BNP and creatinine clearance was found to be the strongest predictor of 1-year mortality. The measurement of natriuretic peptides appears meaningful in a multi-marker strategy as natriuretic peptides may refine risk particularly among patients negative for cTn.
Impaired renal function is associated with higher mortality in patients with ACS 35. Herzog CA, Ma JZ, Collins AJ. Poor long-term survival after acute myocardial infarction among patients on long-term dialysis. N Engl J Med. 1998; 339: 799-805. Link. It is believed that creatinine clearance indicates the cumulative extent of vascular damage caused by hypertension, dyslipidaemia, and diabetes. The knowledge of renal function is important for risk assessment and for dose adjustment of anticoagulation and antiplatelet therapies, as patients with renal failure are prone to excess bleeding due to overdosing. Glomerular filtration rate (GFR) estimates based on creatinine levels can be an unreliable indicator of renal function, as creatinine serum concentrations may be affected by tubular secretion, age, sex, muscle mass, physical activity, and diet. There is accumulating evidence that plasma cystatin C level is an accurate marker of renal function and an independent predictor of mortality in patients with coronary artery disease (CAD), but only few studies have evaluated the prognostic role of cystatin C specifically in patients with ACS. In a study on 726 patients with suspected ACS, cystatin C had better discrimination power than creatinine clearance or creatinine and this suggests that its measurement can improve early risk stratification 36. Jernberg T, Lindahl B, James S, Larsson A, Hansson LO, Wallentin L. Cystatin C: a novel predictor of outcome in suspected or confirmed non-ST-elevation acute coronary syndrome. Circulation. 2004; 110:2342-2348. Link.
OTHER BIOMARKERS
For every stage in the evolution of atherosclerosis, and for the transition of a vulnerable plaque into plaque rupture or erosion, numerous representative biomarkers are currently under investigation. Some of them have already provided promising results regarding prognostication of plaque rupture and adverse outcomes. A list of potential candidates is presented in Table 3. Biomarker of special interest include GDF-15, heart type fatty acid binding protein, Lipoprotein-associated phospholipase A2 (Lp-PLA2), and Myeloperoxidase (MPO). However, none of these biomarkers has provided sufficient evidence for implementation into routine use. 2020 ESC Guidelines on NSTE-ACS recommend to measure hs-cTn serially for the estimation of prognosis 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link. The measurement of BNP or NT-pro BNP should be considered to gain prognostic information, whereas other biomarkers including C-reactive protein, mid-regional pro-adrenomedullin, GDF-15, FABP or Copeptin are not recommended for routine risk or prognostic assessment.
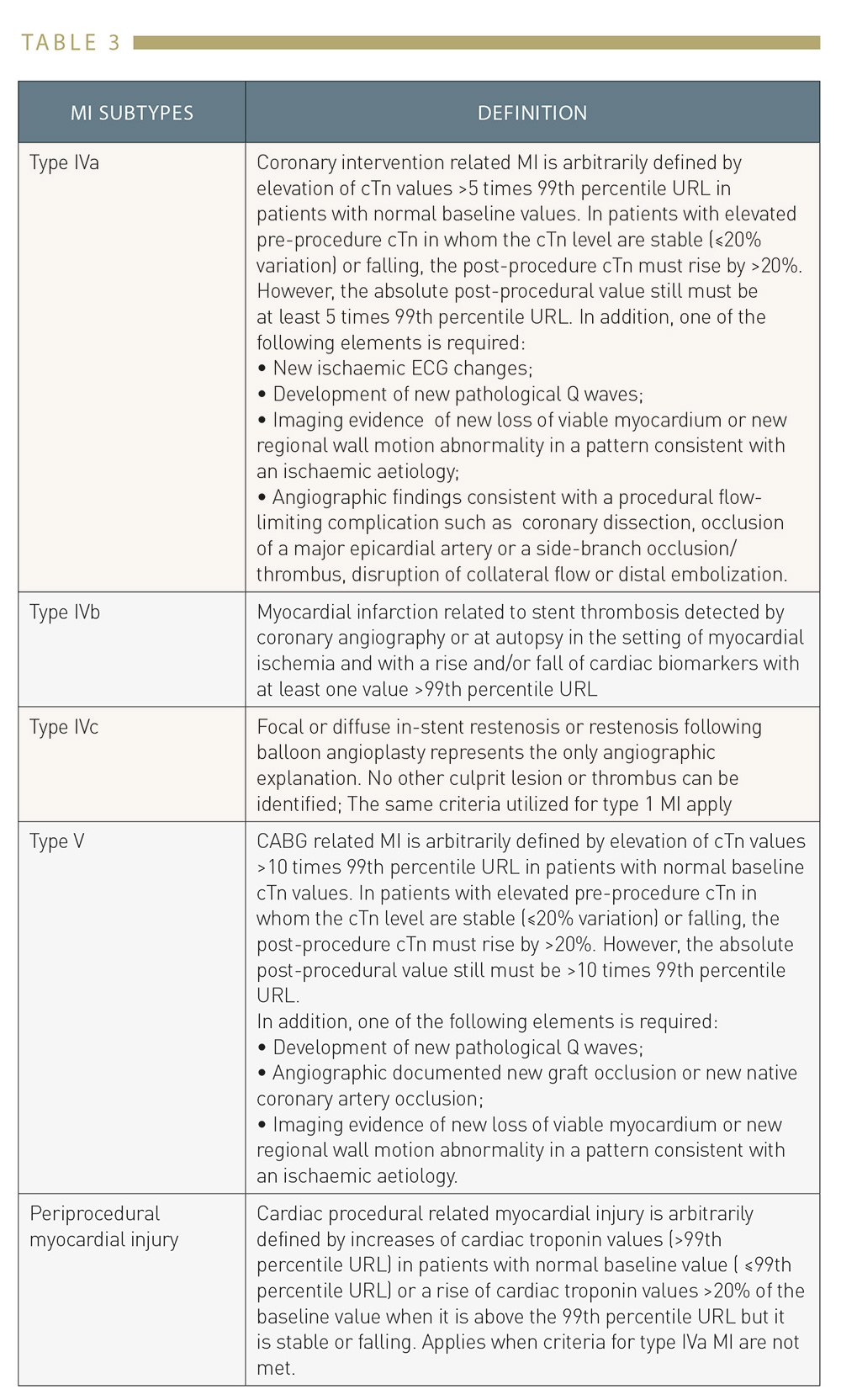
Table 3
Subtypes of prodedure-related MI and periprocedural myocardial injury
Several biomarkers were found to confer independent and incremental information to standard risk assessment and cTn testing.
However, 2020 ESC Guidelines 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link judged evidence not strong enough for a recommendation into clinical routine.
Guidance of therapy
Benefits of adjunctive pharmacological therapy
It has been shown consistently that cardiac troponin may be used for objective guidance of more aggressive anticoagulation with dalteparin or enoxaparin , 37. Lindahl B, Venge P, Wallentin L. Troponin T identifies patients with unstable coronary artery disease who benefit from long-term antithrombotic protection. Fragmin in Unstable Coronary Artery Disease (FRISC) Study Group. J Am Coll Cardiol. 1997; 29: 43–8. Link38. Morrow DA, Antman EM, Tanasijevic M, et al. Cardiac troponin I for stratification of early outcomes and the efficacy of enoxaparin in unstable angina a TIMI-11B substudy. J Am CollCardiol. 2000; 36: 1812-1817. Link, and antiplatelet therapies with abciximab, tirofiban, lamifiban , , 39. Morrow DA, Cannon CP, Rifai N, Frey MJ, Vicari R, Lakkis N, Robertson DH, Hille DA, DeLucca PT, DiBattiste PM, Demopoulos LA, Weintraub WS, Braunwald E; TACTICS-TIMI 18 Investigators. Ability of minor elevations of troponins I and T to predict benefit from an early invasive strategy in patients with unstable angina and non-ST elevation myocardial infarction: results from a randomized trial. JAMA. 2001; 286: 2405-12. Link40. Hamm CW, Heeschen C, Goldmann B, et al. Benefit of abciximab in patients with refractory unstable angina in relation to serum troponin T levels. c7E3 Fab AntiPlatelet Therapy in Unstable Refractory angina (CAPTURE) study investigators. N Engl J Med. 1999; 340: 1623–1629. Link41. Morrow DA, Antman EM, Snapinn SM, McCabe CH, Theroux P, Braunwald E. International, randomized, controlled trial of lamifiban (a platelet glycoprotein IIb/IIIa inhibitor), heparin, or both in unstable angina. The PARAGON investigators. Platelet IIb/IIIa Antagonism for the Reduction of Acute coronary syndrome events in a Global Organization Network. Circulation. 1998; 97: 2386–2395. Link, or triple antiplatelet therapy 42. Kastrati A, Mehilli J, Neumann FJ, Dotzer F, ten Berg J, Bollwein H, Graf I,Ibrahim M, Pache J, Seyfarth M, Schühlen H, Dirschinger J, Berger PB, Schömig A; Intracoronary Stenting and Antithrombotic: Regimen Rapid Early Action for Coronary Treatment 2 (ISAR-REACT 2) Trial Investigators. Abciximab in patients with acute coronary syndromes undergoing percutaneous coronary intervention after clopidogrel pretreatment: the ISAR-REACT 2 randomized trial. JAMA. 2006; 295: 1531-8. Link followed by early coronary intervention were mostly restricted to patients with elevated troponins.
The 2020 ESC guidelines 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link recommend a staged approach to the decision and the timing of coronary angiography. An immediate invasive approach within 120 minutes after initial presentation is recommended in patients at very high risk including hemodynamic instability, cardiogenic shock, acute heart failure related to NSTE-ACS, recurrent or refractory chest pain despite medical treatment, life-threatening arrhythmias, mechanical complications, or ST-segment depression > 1mm in 6 leads plus ST segment elevation in lead aVr or V1. 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link.
An early invasive strategy within 24 hours is indicated for individuals who carry a higher acute risk for death or MI including patients with an established NSTEMI, a GRACE score > 140 points, dynamic new or presumably new contiguous ST-segment changes, resuscitated cardiac arrest without ST segment elevation or cardiogenic shock. All other cases where features of very high or high risk are absent are regarded as low risk. The therapeutic strategy in low risk cases is selective invasive depending on findings from functional stress imaging or non-invasive imaging of coronary anatomy Distinct to previous 2015 ESC Guidelines on NSTE-ACS 43. Roffi M, Patrono C, Collet JP, Mueller C, Valgimigli M, Andreotti F, Bax JJ, Borger MA, Brotons C, Chew DP, Gencer B, Hasenfuss G, Kjeldsen K, Lancellotti P, Landmesser U, Mehilli J, Mukherjee D, Storey RF, Windecker S, Baumgartner H, Gaemperli O, Achenbach S, Agewall S, Badimon L, Baigent C, Bueno H, Bugiardini R, Carerj S, Casselman F, Cuisset T, Erol Ç, Fitzsimons D, Halle M, Hamm C, Hildick-Smith D, Huber K, Iliodromitis E, James S, Lewis BS, Lip GY, Piepoli MF, Richter D, Rosemann T, Sechtem U, Steg PG, Vrints C, Luis Zamorano J; 2015 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation: Task Force for the Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology (ESC). Management of Acute Coronary Syndromes in Patients Presenting without Persistent ST-Segment Elevation of the European Society of Cardiology. Eur Heart J. 2016;37(3):267-315. Link an intermediate risk cohort was omitted and patients with previous MI, previous PCI or CABG, intermediate GRACE score (108-140 points) reduced LVEF, chronic kidney disease (GFR< 60 ml/min) were shifted into the low risk category. In parallel, routine pre-treatment with any P2Y12 inhibitor in patients with planned early PCI was discouraged.
A debate was stimulated 44. Crea F, Thiele H, Sibbing D, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Siontis GCM, Barbato E, Collet JP, Giannitsis E, Hamm CW, Böhm M, Cornel JH, Ferreiro JL, Frey N, Huber K, Kubica J, Navarese EP, Mehran R, Morais J, Storey RF, Valgimigli M, Vranckx P, James S. Debate: Prasugrel rather than ticagrelor is the preferred treatment for NSTE-ACS patients who proceed to PCI and pretreatment should not be performed in patients planned for an early invasive strategy. Eur Heart J. 2021 Aug 17;42(31):2973-2985. Link after this recommendation indicating insufficient evidence to back such a recommendation, in particular to extend findings generated with Prasugrel to all P2Y12 receptor inhibitors. In addition, guidelines disregard current practice where the majority of patients with established NSTEMI receives angiography and revascularization between 24-72 hours 45. https://www.ucr.uu.se/swedeheart/dokument-sh/arsrapporter-sh Link. In favor of early pre-treatment, the EARLY trial 46. Lemesle G, Laine M, Pankert M, Boueri Z, Motreff P, Paganelli F, Baumstarck K, Roch A, Kerbaul F, Puymirat E, Bonello L. Optimal Timing of Intervention in NSTE-ACS Without Pre-Treatment: The EARLY Randomized Trial. JACC Cardiovasc Interv. 2020 Apr 27;13(8):907-917. Link randomized NSTE-ACS patients with high or intermediate risk without P2Y12 ADP receptor antagonist pre-treatment into an immediate and a delayed invasive arm. It emerged that the risk for cardiovascular death or recurrent ischemic event was almost fivefold higher if patients were assigned to the delayed invasive strategy between 12-72 hours without pre-treatment as compared to an immediate invasive strategy within 2 hours.
Biomarkers following elective PCI
In the setting of PCI, biomarkers may be helpful for prediction of procedural success and complications such as PMI. The assessment of the relative contribution of underlying CAD and the additional impact of PCI is almost impossible as the pathophysiology is too complex and the reasons for concentration changes of biomarkers are multifactorial. Generally, PCI leads to mechanical injury of the endothelial layer and plaque and may cause acute release of chemokines, reactive oxygen species, pro-inflammatory and pro-coagulant molecules, and may instigate a pro-inflammatory milieu that may promote adverse vascular remodeling and lead to restenosis, subacute or late stent thrombosis and poor outcomes. Biomarkers that mirror specific pathophysiological aspects may be helpful to identify patients at risk or to develop drugs alleviating adverse sequelae of PCI. In addition, increase of biomarkers before PCI may give information on the presence of vulnerable plaque and hence help to identify patients who require more intense adjunctive treatment during PCI and optimal secondary prevention. Unfortunately, neither 2018 ESC Guidelines on Myocardial Revascularization 47. Neumann FJ, Sousa-Uva M, Ahlsson A, Alfonso F, Banning AP, Benedetto U, Byrne RA, Collet JP, Falk V, Head SJ, Jüni P, Kastrati A, Koller A, Kristensen SD, Niebauer J, Richter DJ, Seferovic PM, Sibbing D, Stefanini GG, Windecker S, Yadav R, Zembala MO; ESC Scientific Document Group. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019 Jan 7;40(2):87-165. Linknor 2021ACC/AHA/SCAI Guideline for Coronary Artery Revascularization 48. Lawton JS, Tamis-Holland JE, Bangalore S, Bates ER, Beckie TM, Bischoff JM, Bittl JA, Cohen MG, DiMaio JM, Don CW, Fremes SE, Gaudino MF, Goldberger ZD, Grant MC, Jaswal JB, Kurlansky PA, Mehran R, Metkus TS Jr, Nnacheta LC, Rao SV, Sellke FW, Sharma G, Yong CM, Zwischenberger BA. 2021 ACC/AHA/SCAI Guideline for Coronary Artery Revascularization: Executive Summary: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022 Jan 18;145(3):e4-e17. Link provide any guidance on biomarker testing in patients undergoing revascularization procedures. However, specific recommendations have been proposed by the 4th version of UDMI 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link and by 2020 ESC Guidelines on NSTE-ACS 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link.
DEFINITION OF TYPE IV POSTPROCEDURAL MI (PMI)
The universal definition of MI has introduced another specific category, namely type 4a, type 4b and type 4c for peri-procedural MI to distinguish it from spontaneous MI, type 1 and type 2 (Table 4).
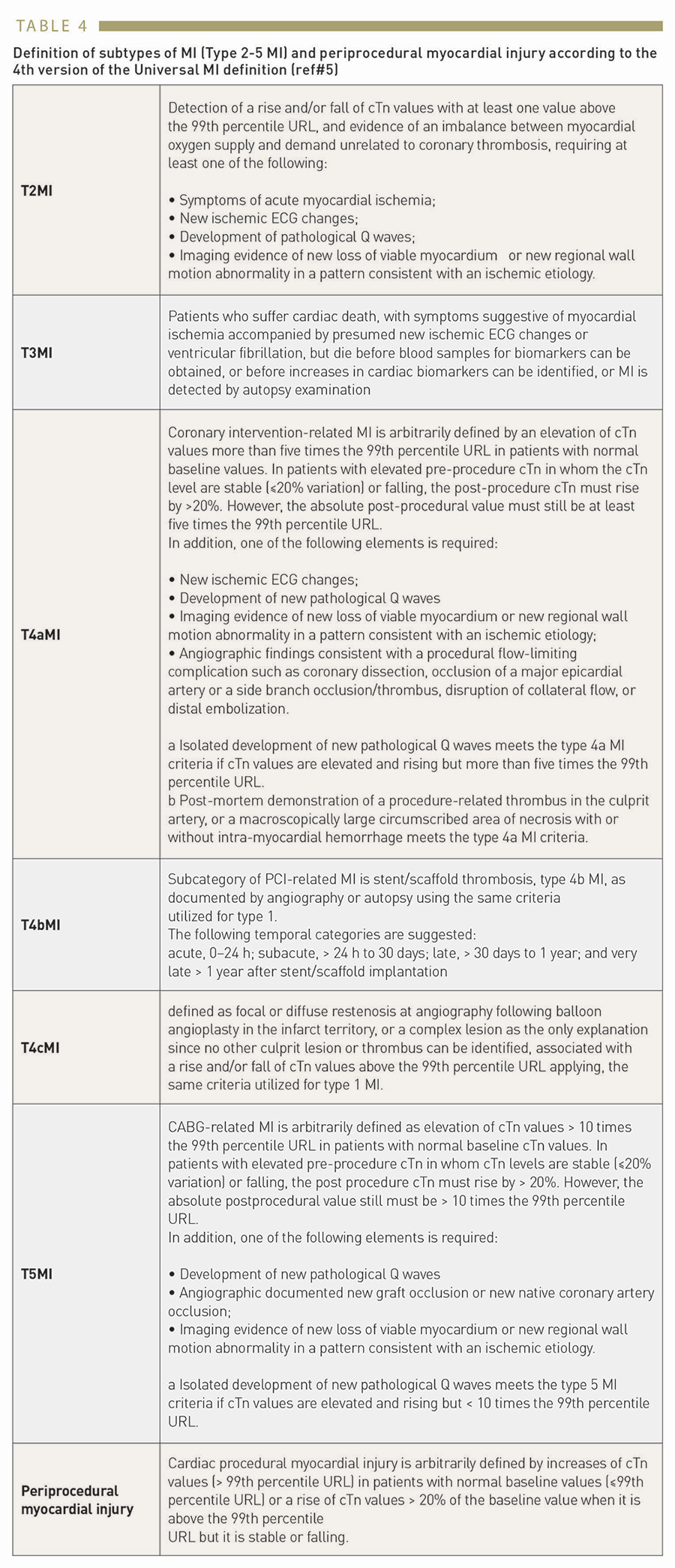
Table 4
Definition of subtypes of MI (Type 2-5 MI) and periprocedural myocardial injury according to the 4th version of the Universal MI definition (ref#5)
This discrimination appears increasingly important as recent ACS trials found that PMI occurred more often (>2 times) but was less prognostically important than spontaneously occurring MI after adjustment for baseline and procedural characteristics 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link.
Assuming a normal troponin at baseline, a PCI-related increase of troponin > 5-times the upper reference limit (99th percentile) is by convention defined as peri-procedural MI according to the 4th version of the Universal MI definition 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link. The update of the Universal MI definition requires the presence of an additional clinical feature suggesting myocardial ischemia other than the PCI procedure itself. Thus, the diagnosis of type 4 MI can now only be made if the patient experienced chest pain, or developed ECG changes, new wall motion abnormalities or in the presence of new nonviable myocardium. Otherwise, even a post-procedural increase above 5-times ULN should not be labelled as a type 4 MI but as peri-procedural myocardial injury. There is no established consensus on the definition of peri-procedural myocardial infarction or injury and other societies and working groups promote distinct definitions , , 10. Thielmann M, Sharma V, Al-Attar N, Bulluck H, Bisleri G, Bunge JJH, Czerny M, Ferdinandy P, Frey UH, Heusch G, Holfeld J, Kleinbongard P, Kunst G, Lang I, Lentini S, Madonna R, Meybohm P, Muneretto C, Obadia JF, Perrino C, Prunier F, Sluijter JPG, Van Laake LW, Sousa-Uva M, Hausenloy DJ. ESC Joint Working Groups on Cardiovascular Surgery and the Cellular Biology of the Heart Position Paper: perioperative myocardial injury and infarction in patients undergoing coronary artery bypass graft surgery. Eur Heart J 2017;38:2392–2407. Link11. Moussa ID, Klein LW, Shah B, Mehran R, Mack MJ, Brilakis ES, Reilly JP, Zoghbi G, Holper E, Stone GW. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol. 2013;62:1563–1570. Link12. Garcia-Garcia HM, McFadden EP, Farb A, Mehran R, Stone GW, Spertus J, Onuma Y, Morel MA, van Es GA, Zuckerman B, Fearon WF, Taggart D, Kappetein AP, Krucoff MW, Vranckx P, Windecker S, Cutlip D, Serruys PW; Academic Research Consortium. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 Consensus Document. Circulation 2018;137:2635–2650. Link.
Regardless the exact thresholds defining post-procedural MI, elevations of cardiac troponin and cardiac enzymes following PCI were related to ischemic myocardial injury. Consistently, Johansen et al were able to demonstrate that the majority of cTnT elevations after PCI persisted for at least 96 hours indicating ongoing release of cTnT from the contractile apparatus reflecting irreversible myocardial injury 49. Johansen O, Brekke M, Stromme JH, Valen V, Seljeflot I, Skjaeggestad O, Arnesen H. Myocardial damage during percutaneous transluminal coronary angioplasty as evidenced by troponin T measurements. Eur Heart J. 1998; 19:112–117. Link. In contrast-enhanced cardiac MRI areas of myocardial infarction were identified as the substrate of minor serum marker elevations , 50. Ricciardi MJ, Wu E, Davidson CJ, Choi KM, Klocke FJ, Bonow RO, Judd RM, Kim RJ. Visualization of discrete microinfarction after percutaneous coronary intervention associated with mild creatine kinase-MB elevation. Circulation. 2001; 103: 2780-3. Link51. Selvanayagam JB, Porto I, Channon K, Petersen SE, Francis JM, Neubauer S, Banning AP. Troponin elevation after percutaneous coronary intervention directly represents the extent of irreversible myocardial injury: insights from cardiovascular magnetic resonance imaging. Circulation. 2005; 111: 1027-32. Link.
Suggested cutoffs for cardiac troponins and cardiac enzymes vary considerably, and the use of hs-cTn assays to diagnose type 4a MI (and type 5 MI) is an area of active research. Recently, the optimal hs-cTnT thresholds to predict cardiovascular events at 30 days and 1 year were reported , 52. Zeitouni M, Silvain J, Guedeney P, Kerneis M, Yan Y, Overtchouk P, Barthelemy O, Hauguel-Moreau M, Choussat R, Helft G, Le Feuvre C, Collet JP, Montalescot G; ACTION Study Group. Periprocedural myocardial infarction and injury in elective coronary stenting. Eur Heart J. 2018;39:1100–1109. Link53. Ndrepepa G, Colleran R, Braun S, Cassese S, Hieber J, Fusaro M, Kufner S, Ott I, Byrne RA, Husser O, Hengstenberg C, Laugwitz KL, Schunkert H, Kastrati A. High-sensitivity troponin T and mortality after elective percutaneous coronary intervention. J Am Coll Cardiol. 2016;68: 2259–2268. Link to be very close to the 5-fold increase supporting the decision of the 4th version of UDMI to maintain these threshold 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link.
If the values are stable or falling, criteria for re-infarction by further measurement of biomarkers together with ECG criteria can be applied. A diagnostic dilemma arises if cardiac troponin is elevated before the procedure and not stable for at least two samples 6 hours apart. In this situation, there are insufficient data to recommend biomarker criteria for the diagnosis of post-procedural myocardial infarction.
Myocardial Infarction or injury following CABG (Type 5 MI)
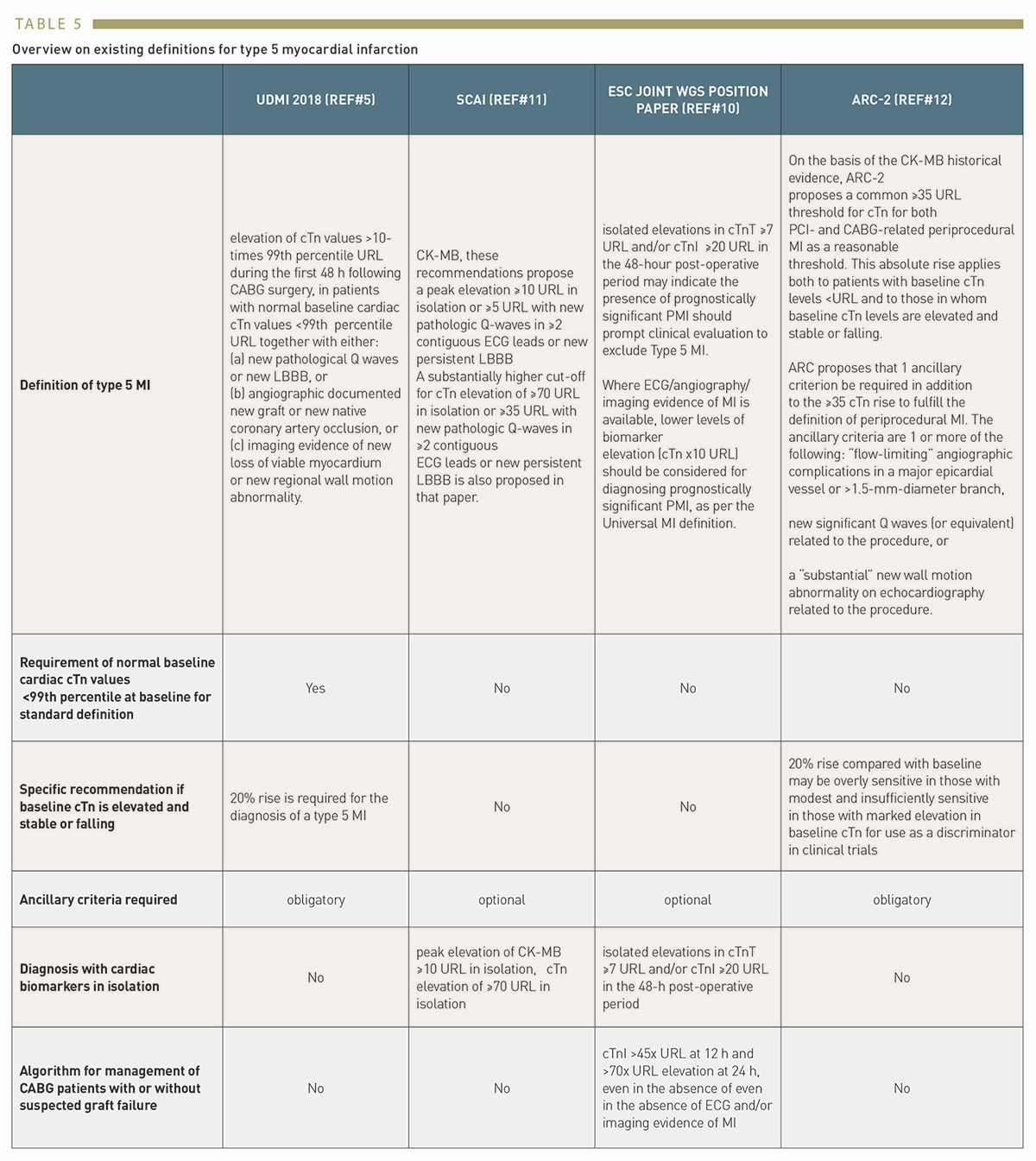
Diagnosis of myocardial injury or myocardial infarction post cardiac surgery, particularly an ongoing ischemia due to graft failure requiring immediate action, is even more challenging because virtually every patient will develop a brisk increase in cardiac enzymes or troponin levels early after surgery, irrespective on-pump or off-pump surgery. In discordance with type 4 MI where its detection may benefit from the higher sensitivity of the hs-cTn assay, clinical specificity for acute myocardial infarction in general and ischemia requiring urgent action in particular are of greater importance. Studies utilizing cardiac magnetic resonance imaging have shown a moderate correlation between early post-CABG cardiac biomarker elevation and the extent of new myocardial necrosis subsequently observed by late gadolinium enhancement , 54. Pegg TJ, Maunsell Z, Karamitsos TD, Taylor RP, James T, Francis JM, Taggart DP, White H, Neubauer S, Selvanayagam JB. Utility of cardiac biomarkers for the diagnosis of type V myocardial infarction after coronary artery bypass grafting: insights from serial cardiac MRI. Heart. 2011;97:810–816. Link55. van Gaal WJ, Arnold JR, Testa L, Karamitsos T, Lim CC, Ponnuthurai FA, Petersen S, Francis JM, Selvanayagam J, Sayeed R, West N, Westaby S, Neubauer S, Banning AP. Myocardial injury following coronary artery surgery versus angioplasty (MICASA): a randomised trial using biochemical markers and cardiac magnetic resonance imaging. Eurointervention. 2011;6:703–710. Link. This discrepancy has been mainly attributed to a wash-out phenomenon that reflects complete reperfusion which, however, may mask MI due to native or graft vessel occlusion 56. Sandoval Y, Jaffe AS. Letter by Sandoval and Jaffe Regarding Article, Temporal Release of High-Sensitivity Cardiac Troponin T and I and Copeptin After Brief Induced Coronary Artery Balloon Occlusion in Humans. Circulation. 2021 Aug 31;144(9):e168. Link. However, existing definitions launched by SCAI, 11. Moussa ID, Klein LW, Shah B, Mehran R, Mack MJ, Brilakis ES, Reilly JP, Zoghbi G, Holper E, Stone GW. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol. 2013;62:1563–1570. Link, ESC Joint Working Groups on Cardiovascular Surgery and the Cellular Biology 10. Thielmann M, Sharma V, Al-Attar N, Bulluck H, Bisleri G, Bunge JJH, Czerny M, Ferdinandy P, Frey UH, Heusch G, Holfeld J, Kleinbongard P, Kunst G, Lang I, Lentini S, Madonna R, Meybohm P, Muneretto C, Obadia JF, Perrino C, Prunier F, Sluijter JPG, Van Laake LW, Sousa-Uva M, Hausenloy DJ. ESC Joint Working Groups on Cardiovascular Surgery and the Cellular Biology of the Heart Position Paper: perioperative myocardial injury and infarction in patients undergoing coronary artery bypass graft surgery. Eur Heart J 2017;38:2392–2407. Link, ESC Working group and Academic Research Consortium 12. Garcia-Garcia HM, McFadden EP, Farb A, Mehran R, Stone GW, Spertus J, Onuma Y, Morel MA, van Es GA, Zuckerman B, Fearon WF, Taggart D, Kappetein AP, Krucoff MW, Vranckx P, Windecker S, Cutlip D, Serruys PW; Academic Research Consortium. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 Consensus Document. Circulation 2018;137:2635–2650. Link regarding type 5 MI (Table 5) differ regarding their emphasis on specificity , , , 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link10. Thielmann M, Sharma V, Al-Attar N, Bulluck H, Bisleri G, Bunge JJH, Czerny M, Ferdinandy P, Frey UH, Heusch G, Holfeld J, Kleinbongard P, Kunst G, Lang I, Lentini S, Madonna R, Meybohm P, Muneretto C, Obadia JF, Perrino C, Prunier F, Sluijter JPG, Van Laake LW, Sousa-Uva M, Hausenloy DJ. ESC Joint Working Groups on Cardiovascular Surgery and the Cellular Biology of the Heart Position Paper: perioperative myocardial injury and infarction in patients undergoing coronary artery bypass graft surgery. Eur Heart J 2017;38:2392–2407. Link11. Moussa ID, Klein LW, Shah B, Mehran R, Mack MJ, Brilakis ES, Reilly JP, Zoghbi G, Holper E, Stone GW. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol. 2013;62:1563–1570. Link12. Garcia-Garcia HM, McFadden EP, Farb A, Mehran R, Stone GW, Spertus J, Onuma Y, Morel MA, van Es GA, Zuckerman B, Fearon WF, Taggart D, Kappetein AP, Krucoff MW, Vranckx P, Windecker S, Cutlip D, Serruys PW; Academic Research Consortium. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 Consensus Document. Circulation 2018;137:2635–2650. Link. SCAI 11. Moussa ID, Klein LW, Shah B, Mehran R, Mack MJ, Brilakis ES, Reilly JP, Zoghbi G, Holper E, Stone GW. Consideration of a new definition of clinically relevant myocardial infarction after coronary revascularization: an expert consensus document from the Society for Cardiovascular Angiography and Interventions (SCAI). J Am Coll Cardiol. 2013;62:1563–1570. Link favors the use of CKMB over cardiac troponin, and recommends higher thresholds for diagnosis, and but also encourages interpretation of biomarker elevations in isolation without clinical criteria clinical criteria.
Table 5
Overview on existing definitions for type 5 myocardial infarction
Consistently, the ESC WG proposes an algorithm for managing CABG patients with or without suspected graft failure based on isolated elevations of biomarkers, even in the absence of ECG and/or imaging evidence of MI. In contrast, the ARC-2 consortium 12. Garcia-Garcia HM, McFadden EP, Farb A, Mehran R, Stone GW, Spertus J, Onuma Y, Morel MA, van Es GA, Zuckerman B, Fearon WF, Taggart D, Kappetein AP, Krucoff MW, Vranckx P, Windecker S, Cutlip D, Serruys PW; Academic Research Consortium. Standardized end point definitions for coronary intervention trials: the Academic Research Consortium-2 Consensus Document. Circulation 2018;137:2635–2650. Link mandates the presence of one or more ancillary criteria that are slightly different from the UDMI criteria (Table 5),
Overall, as outlined in a recent editorial 57. Giannitsis E, Frey N. Isolated early peak cardiac troponin for clinical decision-making after elective cardiac surgery: useless at best. Eur Heart J. 2022 Feb 17:ehab786. Link, early cardiac biomarker elevations after cardiac surgery seem to perform weak when used in isolation without additional clinical criteria.
Subtypes of peri-procedural MI post PCI
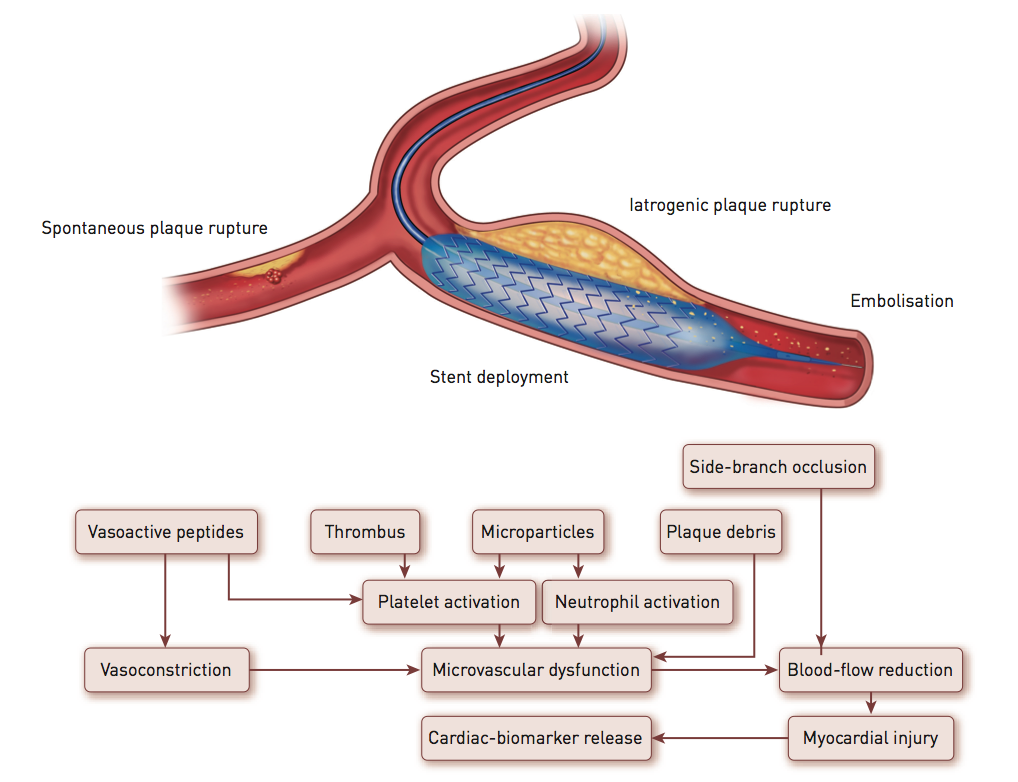
In general, two major pathological mechanisms have been proposed after PCI(Figure 4 , adapted from Prasad A 58. Prasad A, Herrmann J. Myocardial infarction due to percutaneous coronary intervention. N Engl J Med. 2011; 364:453-64. Link):
Figure 4
Pathological mechanisms leading to MI, i.e., spontaneous plaque rupture (type 1 MI), downstream embolisation of plaque material or activated platelets after mechanical disruption of the plaque from balloon inflation or coronary stenting, and mechanical complications such as side branch occlusion or coronary artery dissection
Type 1 or proximal type of periprocedural myocardial injury (25-50% of PMI). The major reason for myocardial injury arises from occlusion of a side branch during angioplasty. The risk increases when the side branch arises from within the target lesion of the native coronary artery or in the presence of ostial stenosis of the side branch. Responsible mechanisms of side branch occlusion include plaque shift, dissection of the dilated coronary artery extending to the side branch, thrombus formation, or plaque embolisation, and side branch spasm.
Type 2 or distal type of periprocedural myocardial injury (50% to 75% of PMI). Atherosclerotic plaque rupture and local vessel trauma lead to distal perfusion deficits in the distal perfusion territory. The mechanisms involved include distal embolisation of atheromatous debris and thrombotic material, leucocyte and platelet activation leading to microvascular plugging of platelets and neutrophils, neurohumoral activation and modulation of vascular and myocardial function, and oxidative stress and inflammation.
PROGNOSTIC RELEVANCE OF other BIOMARKER ELEVATIONs BEFORE AND AFTER ELECTIVE PCI
While increasing cTn concentrations reflect the complexity and mirror peri-procedural myocardial necrosis and short-term outcomes, pre-procedural cTn elevations indicate structural heart disease and pre-existing atherothrombotic burden and seemingly predict better long-term outcomes , 59. Jeremias A, Kleiman NS, Nassif D, Hsieh WH, Pencina M, Maresh K, Parikh M, Cutlip DE, Waksman R, Goldberg S, Berger PB, Cohen DJ, for the EVENT Registry Investigators. Prevalence and prognostic significance of preprocedural cardiac troponin elevation among patients with stable coronary artery disease undergoing percutaneous coronary intervention: results from the Evaluation of Drug Eluting Stents and Ischaemic Events registry. Circulation. 2008; 118:632– 637. Link60. Miller WL, Garratt KN, Burritt MF, Lennon RJ, Reeder GS, Jaffe AS. Baseline troponin level: key to understanding the importance of post-PCI troponin elevations. Eur Heart J. 2006; 27: 1061–1069. Link.
OTHER BIOMARKERS
Several biomarkers mirror complex co-existing and interrelated pathomechanisms beyond myocardial necrosis , 31. Armstrong EJ, Morrow DA, Sabatine MS. Inflammatory biomarkers in acute coronary syndromes: part I: introduction and cytokines. Circulation. 2006;113: e72-5. Link61. Giannitsis E, Katus HA. Biomarkers in acute coronary syndrome. In: The ESC textbook of intensive and acute cardiacv care, edTubaro M. Oxford University press. First edition, pp327-334. Link
Given the complex inter-related pathomechanisms, biomarkers can be used to identify and monitor components of pathophysiological processes and may be useful in the future to develop cardio-protective drugs that prevent microvascular obstruction, improve distal territory perfusion, limit inflammation and thereby reduce PMI and later native coronary artery or stent stenosis or thrombosis. Representative biomarkers of platelet activation and activated thrombosis in blood include measurement of soluble CD40 ligand (sCD40L) and other granule secretion products including platelet factor 4 (PF4). Measurement of high residual platelet reactivity or degree of platelet inhibition by several aggregometry based methods has emerged as an interesting technique to monitor the efficacy of dual antiplatelet therapy, with most interest on clopidogrel therapy due to higher prevalence of low or no-response, potential interaction with proton pump inhibitors and propensity to CYP2C19 loss of function. The measurement of haemostatic proteins may include tissue factor, thrombin-antithrombin-complex (TAT), prothrombin F1+2, and von Willebrand factor (vWF). The great obstacle of measuring haemostatic proteins are, however, mostly pre-analytical issues 62. Krychtiuk KA, Speidl WS, Giannitsis E, Gigante B, Gorog DA, Jaffe AS, Mair J, Möckel M, Mueller C, Storey RF, Vilahur G, Wojta J, Huber K, Halvorsen S, Geisler T, Morais J, Lindahl B, Thygesen K. Biomarkers of coagulation and fibrinolysis in acute myocardial infarction: a joint position paper of the Association for Acute CardioVascular Care and the European Society of Cardiology Working Group on Thrombosis. Eur Heart J Acute Cardiovasc Care. 2021 May 11;10(3):343-355. Link.
Biomarkers that indicate neurohumoral activation include serotonin and endothelin while natriuretic peptides including BNP and NT-proBNP may increase after severe myocardial ischaemia or haemodynamic stress during PCI , 32. James SK, Lindbäck J, Tilly J, Siegbahn A, Venge P, Armstrong P, Califf R, Simoons ML, Wallentin L, Lindahl B. Troponin-T and N-terminal pro-B-type natriuretic peptide predict mortality benefit from coronary revascularization in acute coronary syndromes: a GUSTO-IV substudy. J Am Coll Cardiol. 2006; 48: 1146-54. Link33. Goetze JP, Gore A, Moller CH, Steinbruchel DA, Rehfeld JF, Nielsen LB. Acute myocardial hypoxia increases BNP gene expression. FASEB J. 2004; 18: 1928-30. Link. Increased plasma BNP levels at baseline are associated with more complex lesions, which may play a role for chronic or repetitive ischaemia. Several investigators found that tissue hypoxia alone can trigger release of BNP, even in the absence of left ventricular dysfunction 33. Goetze JP, Gore A, Moller CH, Steinbruchel DA, Rehfeld JF, Nielsen LB. Acute myocardial hypoxia increases BNP gene expression. FASEB J. 2004; 18: 1928-30. Link. Whether elective PCI may cause significant alterations in natriuretic peptide level is unknown and findings are conflicting. In the JUMBO-TIMI 26 trial NT-pro BNP level were measured in 747 patients before and after elective or urgent PCI 63. Bonaca MP, Wiviott SD, Sabatine MS, Buros J, Murphy SA, Scirica BM, Rifai N, Antman EM, Morrow DA. Hemodynamic significance of periprocedural myocardial injury assessed with N-terminal pro-B-type natriuretic peptide after percutaneous coronary intervention in patients with stable and unstable coronary artery disease (from the JUMBO-TIMI 26 trial). Am J Cardiol. 2007; 99:344-8. Link. Patients with procedural MI had significantly higher levels of NT-pro-BNP at 12 to 24 hours (405 vs. 146 pg/ml, p <0.001). The magnitude of increase in NT-pro-BNP correlated strongly with the extent of myocardial injury, even in those with very low-level troponin increases. Thus, these findings suggest that peri-procedural myocardial injury, even at low levels, during PCI is associated with increased haemodynamic stress as measured by increasing NT-pro-BNP. In two small studies, circulating BNP levels increased after PCI of stable CAD patients. In another study on 103 patients, balloon inflations during elective PCI did not cause significant alterations in plasma BNP levels 64. Yildirir A, Acikel S, Ertan C, Aydinalp A, Ozin B, Muderrisoglu H. Effects of lesion complexity on baseline and postprocedural B-type natriuretic peptide levels in patients undergoing percutaneous coronary interventions. Tex Heart Inst J. 2007; 34:282-9. Link. It was speculated that short balloon inflations did not cause ischaemia severe enough to elevate BNP levels. In summary, baseline elevations of natriuretic peptides indicate adverse long-term prognosis independent of left ventricular dysfunction. However, the relevance of increases of BNP following elective PCI remains unsettled.
A number of studies suggest an association between baseline level of inflammatory markers including pro-inflammatory cytokines, metalloproteinases, selectins and adhesion molecules , 31. Armstrong EJ, Morrow DA, Sabatine MS. Inflammatory biomarkers in acute coronary syndromes: part I: introduction and cytokines. Circulation. 2006;113: e72-5. Link65. Toutouzas K, Colombo A, Stefanadis C. Inflammation and restenosis after percutaneous coronary interventions. Eur Heart J. 2004; 25:1679-87. Link. Among these inflammatory markers, CRP has been investigated extensively and an association between CRP levels and adverse outcome has been reported after elective and emergent PCI. However, study results focusing on the association between CRP level and events occurring after PCI is still controversial. Possible mechanisms for the association with post-procedural troponin increase and for the adverse outcomes include a relation between CRP and diffuse atherosclerotic disease, vulnerability of the atheromatous lesion that predispose to micro-embolisation or to a pro-thrombotic milieu at the site of angioplasty-induced vessel wall injury. Effective clopidogrel administration before PCI has been associated with less inflammation in response to vascular injury, as indicated by an attenuated increase in post-procedural CRP. Systemic inflammation also provides a link between PCI-associated infarctions and long-term events as previous studies have shown that elevated CRP predicts future events in patients with stable angina , 31. Armstrong EJ, Morrow DA, Sabatine MS. Inflammatory biomarkers in acute coronary syndromes: part I: introduction and cytokines. Circulation. 2006;113: e72-5. Link61. Giannitsis E, Katus HA. Biomarkers in acute coronary syndrome. In: The ESC textbook of intensive and acute cardiacv care, edTubaro M. Oxford University press. First edition, pp327-334. Link. In addition, there is some evidence that statin therapy may reduce cardiac event rates following PCI 66. Kereiakes DJ. Adjunctive pharmacotherapy before percutaneous coronary intervention in non-ST-elevation acute coronary syndromes: the role of modulating inflammation. Circulation. 2003; 108:III22-7. Link. It has been speculated that adjunctive pharmaceutical interventions such as statin therapy before intervention may positively modulate the inflammatory response, and thus may improve long-term outcomes after PCI and prevent restenosis, particularly among stable patients with persistently elevated CRP who are not under statin therapy.
Although several additional biomarkers have conferred prognostic information that is additive to and independent of cardiac troponins, 2020 ESC guidelines on NSTE-ACS 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link discourage the routine use of additional biomarkers for prognostication.
Conclusions
Biomarkers may help to identify pathophysiological processes of stable disease and potentially the transition from stable plaque to vulnerable plaque and plaque rupture. Representative biomarkers include markers of inflammation, activation of coagulation, oxidative stress, myocardial ischaemia and myocardial necrosis.
In clinical practice, cardiac troponins have been recommended as the preferred biomarkers for detection of myocardial necrosis due to high diagnostic sensitivity and their absolute cardiospecificity. Therefore, cardiac troponins represent the reference standard for diagnosis of myocardial infarction.
According to the Universal MI definition, spontaneous MI is diagnosed if troponin is elevated above the 99th percentile value of a reference population and shows a distinct rise and/or fall, together with signs or symptoms of myocardial ischaemia.
In order to distinguish spontaneous MI from more prevalent, but less prognostically relevant post-interventional MI, the universal definition of myocardial infarction introduced a specific category. Type 4 postprocedural MI following PCI is defined as a rise of cardiac troponin three times above the 99th percentile value. The clinical context of myocardial ischaemia is given by the nature of the intervention.
Regarding the prognostic relevance of post-procedural elevation of CKMB or cardiac troponin there are several issues and inconsistencies.
Accumulating evidence suggests that the measurement of a baseline cardiac troponin level with the use of a high-sensitivity assay, together with clinical and angiographic characteristics represents a powerful surrogate for the preprocedural risk of a patient.
Post-procedural elevations of cardiac troponin or CK-MB are less frequently observed in patients without pre-procedural elevations. However, relevant elevations above 5 times ULN may indicate short-term and long-term mortality. It appears that pre-procedural rather than post-procedural biomarker level predict short-term and long-term outcomes.
New algorithms for the management of patients undergoing elective PCI taking into account pre- and post-procedural biomarker level may help to identify patients at risk who might require prolonged observation, more intense secondary prevention, and repeat angiography, if clinically indicated, to improve short-term and long-term survival.
Personal perspective
Hugo A. Katus
Measurement of high sensitivity cardiac troponins has started to replace the use of conventional sensitive or contemporary sensitive cardiac troponin assays. These hs-cTn assays were consistently shown to improve earlier and more accurate diagnosis of MI and to facilitate earlier disposition of patients using fast diagnostic algorithms. In parallel, hs-cTn confer strong prognostic information that allows to discharge the majority of patients with suspected ACS after rule-out without an excess risk of death or recurrent MACE. Recently, hs-cTn testing is possible on POC instruments 9. Collet JP, Thiele H, Barbato E, Barthélémy O, Bauersachs J, Bhatt DL, Dendale P, Dorobantu M, Edvardsen T, Folliguet T, Gale CP, Gilard M, Jobs A, Jüni P, Lambrinou E, Lewis BS, Mehilli J, Meliga E, Merkely B, Mueller C, Roffi M, Rutten FH, Sibbing D, Siontis GCM; ESC Scientific Document Group. 2020 ESC Guidelines for the management of acute coronary syndromes in patients presenting without persistent ST-segment elevation. Eur Heart J. 2021 Apr 7;42(14):1289-1367. Link. While hospitals without or only temporal access to hs-cTn measurements are likely to benefit, the incremental value of POCT as a substitute to biochemistry from central lab is challenging since treatment and management decision do not only depend on the result of selected biomarkers.
Another challenge is the management of patients with myocardial injury, a highly prevalent phenomenon within the observation zone requiring additional cardiac imaging, and hs-cTn testing after 3 hours. It is attractive to speculate that additional biomarkers may play an important role for differential diagnosis and refinement of risk.
Finally, the UDMI definition 5. Thygesen K, Alpert JS, Jaffe AS, Chaitman BR, Bax JJ, Morrow DA, White HD; ESC Scientific Document Group. Fourth universal definition of myocardial infarction (2018). Eur Heart J. 2019;40(3):237-269. Link of type 2 MI and other infarct subtypes is not universally accepted and requires attention.