Sedation, pain management and resuscitation
Summary
Advances in minimally invasive percutaneous cardiovascular procedures have resulted in an increasing need for patients to be managed with sedative and analgesic medication outside the traditional operating room.
Sedation techniques, together with good pain relief, make it possible to perform these interventions and make it more acceptable to patients. Therefore, sedation and analgesia have become common practice in interventional cardiology. Many patients undergoing percutaneous coronary intervention have severe cardiovascular disease, obesity or pulmonary comorbidity and are therefore at high risk for hemodynamic instability.
These realities have resulted in more interventional cardiology practitioners being regularly exposed to critical care scenarios. The use of anxiolytic and analgesic medication is not without risk and it is not always easy to achieve the intended level of sedation. All personnel managing such situations must therefore have the necessary knowledge and skills to both recognise and manage adverse reactions safely. The catheter laboratory environment must contain all the relevant critical care equipment, including supplemental oxygen, suction, and equipment for airway support and bag-mask ventilation. Emergency protocols and training for cardiopulmonary resuscitation in the event of cardiac arrest or anaphylaxis must also be integrated into the skillset of practitioners.
Introduction
Over the last decades a growing number of diagnostic and interventional procedures have been performed outside the traditional operating room . This is largely due to the increase in minimally invasive, nonsurgical diagnostic and therapeutic interventions. Common interventions in the cardiac catheterization laboratory include diagnostic coronary angiography and percutaneous coronary interventions, electrophysiology procedures, catheter based interventions of congenital heart disease and transcatheter valve interventions .
Especially, transcatheter aortic valve implantation (TAVI) has been developed as a minimally invasive and effective treatment to treat severe aortic valve stenosis. These advances in minimally invasive percutaneous cardiovascular procedures have resulted in an increasing need for patients to be managed with sedative and analgesic medication outside the traditional operating room. Sedation techniques, together with good pain relief, make it possible to perform these interventions and make it more acceptable to patients. Therefore, sedation and analgesia have become common practice in interventional cardiology.
During percutaneous coronary intervention (PCI), peri-procedural sedation is sometimes applied to achieve a minimally depressed state of consciousness as pain or anxiety management. Also complications during coronary angiography or percutaneous coronary interventions may require the need for sedation. Finally, patients with ST segment elevation myocardial infarction arriving in the cardiac catheterization laboratory for primary percutaneous intervention may present with respiratory or cardiorespiratory arrest or cardiogenic shock and therefore require anesthesia. Since patients should not be exposed to unnecessary risks and patient safety must be preserved, this chapter will provide a guideline on the use of analgesics and sedation and the risks involved in using them. Nonetheless, it should be emphasised how important it is that these techniques should be used only by trained and skilled personnel. Sedation and analgesia for procedures performed outside the operating room on children is beyond the scope of this chapter.
Planning and patient selection
There are certain difficulties for anaesthesiologists in performing care remote from the main operating room. These challenges include lack of standard anaesthesia machines and monitors. Additional time is needed for the set-up and positioning of all equipment in the catherization laboratory. More-over, lack of familiar operators, nurses, techniques or procedures could enhance difficulty for the anaesthesia personnel. Therefore, as soon as the interventionist is aware of possible needed anaesthetic care, the anaesthetic team is consulted early for pre-procedural planning.
The interventionist consults the anesthesia personnel to determine what type of anaesthetic care is recommended, particularly for concerns such as severe patient pain or anxiety, inability to lie supine, inability to cooperate, an anticipated difficult airway or hemodynamic instability. The anesthesiologist reviews the pathology for which the procedure is being performed and patient comorbidities. It is especially important to discuss the type of procedure, the anticipated duration and complexity of the procedure. Also, providing portable shields, lead aprons and thyroid collars for all aesthetic personnel to minimize radiation exposure is mandatory.
The type of anaesthetic care is influenced by the type and duration of procedure but also by comorbid conditions. Appropriate preprocedural evaluation of the patient increases the likelihood of satisfactory sedation and decreases the likelihood of adverse outcomes. A recommended preprocedural evaluation of the patient is outlined in Figure 1. Older patients and those with renal or hepatic insufficiency may require dosing adjustments of different anesthesic agents. Comorbid conditions such as pulmonary hypertension with right ventricular dysfunction, chronic obstructive pulmonary disease (COPD), obstructive sleep apnea and obesity may cause respiratory or hemodynamic instability during sedation or general anesthesia.
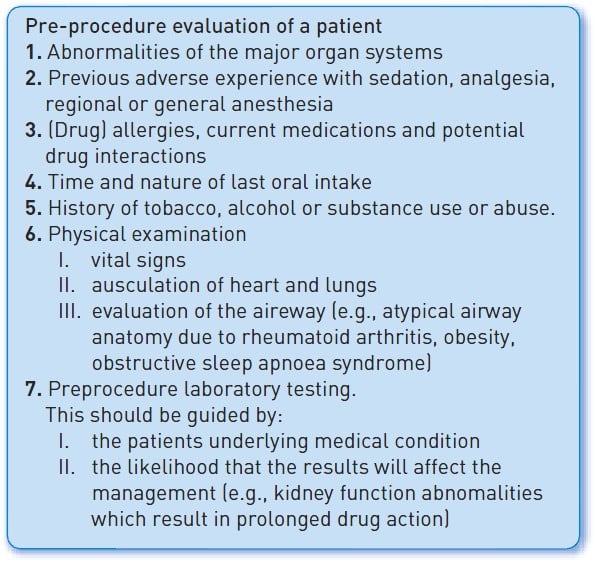
Figure 1
Patients should always be informed of, and agree to, the administration of sedation/analgesia and be made aware of the benefits, risks, limitations and alternatives. In accordance with general anaesthesia, patients undergoing sedation/analgesia should not drink fluids or eat solid meals as recommended by guidelines for preoperative fasting .
Goals and definitions of sedation and analgesia
Sedation is achieved using short-acting analgesic and sedative medication. Hence the operator can adequately perform its procedure, while together patients can be monitored safely for possible adverse events. Previously this type of sedation was called ‘conscious sedation’. However, currently the preferred term is “procedural sedation and analgesia” (PSA) because sedation frequently alters consciousness. The American Society of Anesthesiologists (ASA) state that sedation and analgesia are a continuum. This ranges from minimal sedation (anxiolysis) to general anesthesia. The level of sedation is independent of the administration route. Its depth can rapidly change when using aesthetics. Therefore it is highly important to continuously monitor the patient, even if he is responding conscious state .
The Joint Commission on Accreditation of Healthcare Organizations has attempted to define the levels of drug-induced sedation, which range from minimal sedation to general anesthesia .
- Minimal sedation (anxiolysis)– The patient responds normally to verbal commands. Cognitive function and coordination may be impaired, but airway reflexes, ventilatory and cardiovascular functions are unaffected.
- Moderate sedation and analgesia (previously conscious sedation)– The patient responds purposefully to verbal commands alone or when accompanied by light touch. Protective airway reflexes and adequate ventilation are maintained without intervention. Cardiovascular function remains stable. This means that the patient is more conscious than only reflexive withdraw after a painful stimulus.
- Deep sedation and analgesia – The patient cannot be easily aroused but responds purposefully to a painful stimulus. Ventilatory function can be impaired. Spontaneous ventilation may be inadequate but cardiovascular function is usually stable. Assistance may be needed to ensure the airway is protected and adequate ventilation maintained.
- General anesthesia – The patient cannot be aroused and often requires assistance to protect the airway and maintain ventilation. Cardiovascular function may be impaired. Patients do no respond to painful stimuli.
The intended level of sedation for minimally invasive procedures should be minimal to moderate sedation. Deep and general sedation should only be handled by a professional anaesthetic team. This is important as, for most PCI procedures, the operator must get feedback from the patient regarding chest pain, so high sedation levels are generally not recommended. Because of differences among patients, it is not possible to publish a list showing which procedures can be performed under a lower sedation level and which procedures should be performed under deeper sedation or even general anaesthesia. For example, many patients can undergo gastroscopy when minimally sedated to level, but there are also patients who only tolerate this procedure when under general anaesthesia. Some procedures, like percutaneous clipping of the mitral valve, closure of an ASD, in which TEE is used as well, usually require general anaesthesia. The dividing line between consciousness and unconsciousness can be subtle and the intended level of sedation may not be the one ultimately achieved, especially in older patients and/or patients in a poor general condition. Therefore, practitioners should always be able to rescue patients achieving a level of sedation deeper than originally intended. On the other hand, sedation which is too light for the intended procedure is not safer than oversedation. Undersedation can lead to tachypnoea, tachycardia, restlessness and fear which can increase the difficulty of the procedure and can be dangerous .
Monitoring
Every patient undergoing sedation and/or analgesia is given an intravenous access and is to be monitored by a trained person, whose primary and only task is monitoring of the patient. The physician carrying out the procedure cannot supervise the sedation and/or analgesia at the same time. Many complications associated with anesthesia can be avoided if trained persons are notified early. The allocated person should receive additional training in:
- Basic cardiopulmonary physiology and skills in airway management (head tilt, chin lift, jaw thrust manoeuvre, bag and mask ventilation).
- Pharmacology of sedatives, analgesics, the respective antagonists with their pharmacokinetics and interactions.
- The theory and practice of sedation procedures.
- Principles and practice of monitoring and their limitations.
- Complications of sedation and/or analgesia.
- Advanced life support skills.
- Recovery and discharge criteria.
Standard monitoring minimally consists of continuous pulse oximetry (SpO2 should be kept ≥95%), capnography, non-invasive (automated) blood pressure measurement, observation of breathing and its frequency. Especially in cardiac procedures which can give rise to dysrhythmias, an electrocardiogram should be made continuously , , . Alarm limits should be set appropriately. Additionally verbal responsed should be checked periodically, e.g. every five minutes. If verbal responses are not possible, some patients can give a ‘thumbs up’ or have other non-verbal ways of communication. Records must be made not only of the diagnostic or surgical procedure, but also of the sedation and/or analgesia. Vital signs and level of sedation should be noted at frequent intervals, after administration of drugs and in the immediate post-procedure period. Administration of drugs and type of drugs and dosage are recorded. Furthermore, a mask with a self-inflating bag, additional oxygen and resuscitation, including defibrillation equipment, are present and in working order. Also, a mechanical ventilator must be readily available. It is of the utmost importance that trained staff check this equipment daily, and after each resuscitation event (Figure 2). Later in this chapter more about resuscitation and required equipment.

Figure 2
The monitors display all the essential cardio-respiratory parameters during a procedure:
(A) ECG monitor. (B) Central venous pressure. (C) Arterial oxygen saturation. (D) Capnograph measuring end-tidal-CO2. (E) Arterial blood pressure. (F) Mean arterial blood pressure. (G)Ventilatory pressure. (H) Inspiratory Oxygen Fraction (FIO2). (I) Respiratory mode with ventilator settings (volume, frequency, PEEP).
VENTILATION
Drug-induced respiratory depression and airway obstruction are the most prominent adverse effects of sedation , . Therefore, pulse oximetry is widely used. However, pulse oximetry is not a valid tool to detect hypoventilation, airway obstruction or apnoea. Significant respiratory depression can occur despite normal oxygen saturation, especially when the patient receives supplemental oxygen . Pulse oximetry effectively detects hypoxemia and oxygen desaturation, being oxygenation. The adequacy of ventilation should be determined through continuous observation of patient respiration and/or monitoring for the presence of carbon dioxide exhaled by the patient (capnography). Capnography is the monitoring agent of choice for detecting hypoventilation (sensitivity 100%, specificity 64%), which potentially leads to hypoxia. However, obtaining a proper capnogram in a spontaneously ventilating patient is not always easy but should always be started once moderate sedation is achieved. .
HAEMODYNAMICS
Sedative and analgesic agents can blunt the autonomic compensation for hypovolaemia and procedure-related stress. On the other hand, inadequate sedation and/or analgesia can lead to hypertension, tachycardia and restlessness, and therefore inability to complete the procedure properly. Frequent communication with the patient, if possible, and recording of electrocardiogram and non-invasive blood pressure monitoring, at 5-minute intervals, enables the caregiver to detect problems and intervene.
Medication
If required, sedation and analgesia should be administered before starting the procedure. Preferably, sedation is given intravenously in small, incremental doses. Sufficient time must elapse between doses to allow the effect of each dose to be assessed before subsequent drug administration .
Preferably, effective pain relief is achieved by topical, infiltration or regional anaesthesia instead of intravenous sedation. Intravenous pain relief should come on top of other methods. If this is not possible, it is advisable to consult an anaesthesiologist. Also for reasons of safety, there is a preference to use monotherapy and to use fast-acting and short-acting drugs with which the medical team is familiar. The effect of intravenous use of long-acting medication is unpredictable and can lead to unwanted interactions, such as synergistic effects of drugs . Sedation should not be used as a replacement for analgesia. If both sedation and analgesia are necessary, the analgesic drugs should be given first because of synergistic effects . The effect of oral premedication should be taken into account.
Details for commonly used hypnotics and analgesics and their reversal agents are given in Table 1, Table 2, Table 3 and Table 4 respectively.
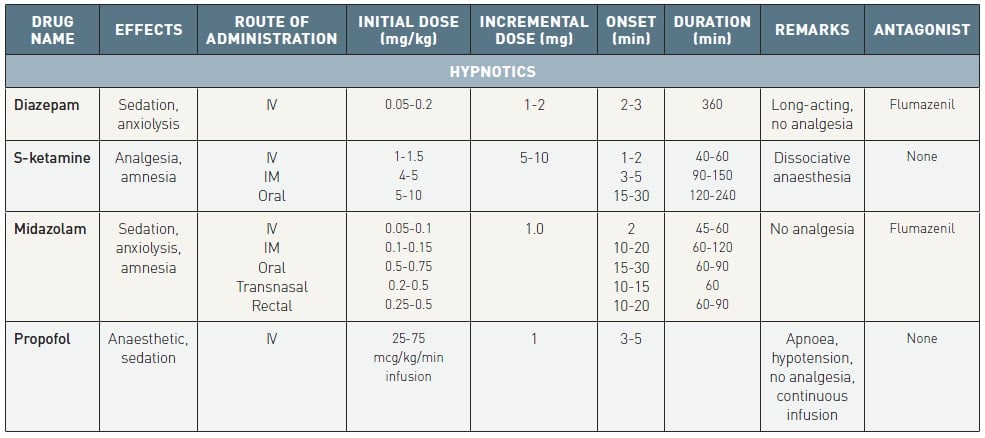
Table 1
Characteristics of commonly used hypnotics
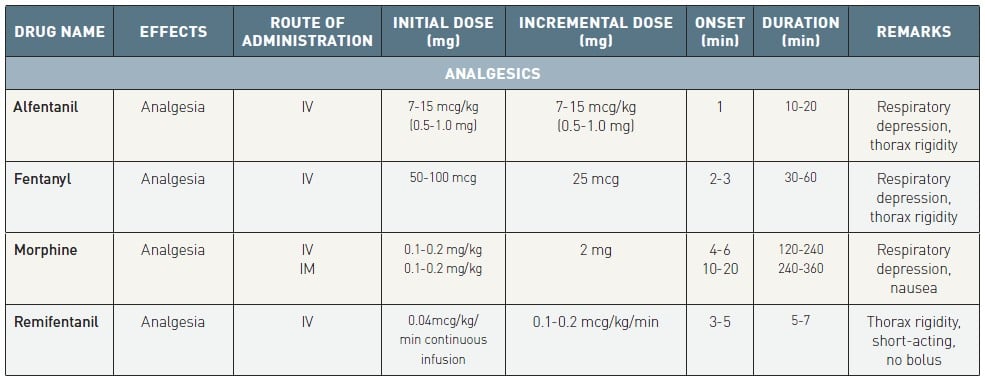
Table 2
Characteristics of commonly used analgesics
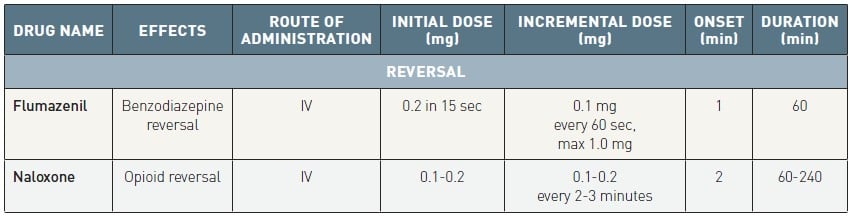
Table 3
Characteristics of reversal agents
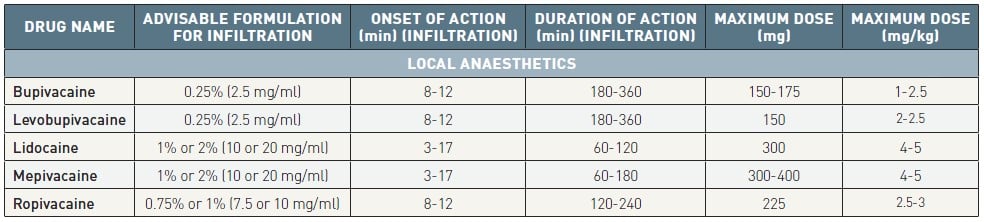
Table 4
Characteristics of commonly used local anaesthetic agents
HYPNOTICS
Propofol, ketamine and etomidate are intended by the ASA guidelines for general anesthesia. Sedatives, such as benzodiazepine, nitrous oxide, chloral hydrate and antihistamines are not primarily intended for general anesthesia. However, they may be given in combination. An intravenous line should be considered in every patient receiving sedation or anesthesia, also when this was achieved via a non-intravenous route .
Benzodiazepines
Diazepam
Diazepam is a benzodiazepine and is often used as premedication. Because it has a long duration of action (half-life 20-48 hours, 42-100 hours for desmethyldiazepam) , use of diazepam in sedation is not recommended.
Midazolam
Midazolam is a short-acting benzodiazepine. It results in anxiolysis, sedation and amnesia. Loss of consciousness occurs within 1-2.5 minutes after administration. Midazolam is metabolised in the liver into active metabolites. Half-life of midazolam is 1.5-2.5 hours and its main metabolite approximately 1 hour. It is excreted by the kidney. Side effects include paradoxical reactions such as dysphoria, agitation and restlessness.
Precautions/contraindications
In elderly patients, patients with heart failure or renal insufficiency, the half-life is prolonged with possible accumulation of metabolites. Midazolam should not be used in patients known to have myasthenia gravis.
S-Ketamine
S-Ketamine produces amnesia and analgesia. After intravenous administration, the effect sets in after 30-60 seconds and lasts 5-10 minutes in the case of a single shot. After intramuscular injection, the effect starts after 3-5 minutes and lasts 12-25 minutes. S-Ketamine is metabolised in the liver into active metabolites with analgesic effects (half-life 2 hours) and is excreted by the kidney. Side effects include hypertension, increase in intracranial and intraocular pressure, increased saliva production, tonic-clonic movements, unpleasant dreams, hallucinations and delirium.
Precautions/contraindications
S-Ketamine is associated with less cardiorespiratory depression, but airway obstruction, laryngospasm and aspiration of gastric contents can still occur. Also, S-ketamine produces dissociative anaesthesia, where some of the classic signs for measuring the depth of sedation can no longer be applied. Furthermore, there is no pharmacological antagonist for S-ketamine. We rarely use S-ketamine for the reasons mentioned above.
Propofol
Propofol is a short-acting sedative with a small therapeutic window. Loss of consciousness occurs within 1 minute after injection. In the liver, propofol is metabolised into inactive metabolites, which are 90% excreted by the kidney. Elimination is biphasic with half-life of 40 minutes and more than 3 hours. Preferably, propofol is administered through continuous infusion. This can be done using a target-controlled infusion technique in which a preset target plasma level of propofol is used. Side effects include pain at the site of injection. An attempt to diminish this side effect can be made by administering lidocaine 20 mg before injection of propofol.
Precautions/contraindications
Propofol can produce rapid, profound decreases in the levels of consciousness and cardiorespiratory function, especially when combined with other sedatives and/or analgesics. Because of the risk of bacterial contamination, propofol should be administered directly after preparation of the syringe. It should also be noted that there is no specific pharmacologic antagonist for propofol . At the moment, there is not enough experience with the new agent fospropofol to determine its place.
Etomidate
Etomidate is an anaesthetic without analgesic action. It increases the inhibitory action of the GABA receptor. The effect starts within one minute after administration and lasts for 3 to 5 minutes. Etomidate lowers the plasmalevels of cortisol and aldosterone for 6 to 8 hours. Therefore caution is needed in patients under high stresslevels, e.g. sepsis. Exogenous cortisol administration may be needed. Induction of anesthesia may give a transient drop in blood pressure. Hydrocortison can be given in case of overdosage .
Precautions/contraindications
Sedatives, antipsychotic, opioids and alcohol can enhance the sedative effect an may require a lower dosage. When combined with calcium antagonists, it can lower AV-conduction time. Fentanyl can lower its plasma clearance without lowering the half-life and in combination a dosage reduction of etomidate should be considered. MAO inhibitors should be withdrawn two weeks before the procedure.
ANALGESICS
Analgesics are given for pain but can give sedation as a side effect. Opioids are a well-known example of this.
Alfentanil
This is a synthetic opioid with strong analgesic properties. The analgesic effect starts almost immediately after administration and lasts about 10-20 minutes. Alfentanil is metabolised in the liver to inactive metabolites. Half-life is approximately 80 minutes. Side effects include respiratory depression (mainly with doses >1 mg), bradycardia, muscle rigidity (especially thorax), nausea and vomiting. Transitory hypotension can occur.
Precautions/contraindications
In case of hepatic and renal insufficiency, uncontrolled hypothyroidism, lung disease, alcoholism, obesity and in elderly patients, doses should be adjusted. Avoid administration of alfentanil during or within 2 weeks after withdrawing treatment with non-selective MAO inhibitors. Erythromycin and cimetidine can prolong the duration of effectiveness.
Fentanyl
This is a synthetic opioid with strong analgesic properties. The analgesic effect after intravenous administration is maximal after 2-3 minutes and lasts about 30-60 minutes. Fentanyl is metabolised in the liver and is mainly excreted by the kidney. Half-life is about 8 hours. Side effects include respiratory depression, muscle rigidity (especially thorax), bradycardia, nausea and vomiting.
Precautions/contraindications
In case of hepatic and renal insufficiency, uncontrolled hypothyroidism, lung disease, alcoholism, obesity and in elderly patients, doses should be adjusted. Avoid administration of alfentanil during or within 2 weeks after withdrawing treatment with non-selective MAO inhibitors.
Morphine
Morphine can be administered subcutaneously, intramuscularly or intravenously. Maximal analgesic effect is reached after 50-90 minutes, 30-60 minutes and 20 minutes respectively. The duration of effect can be as long as 7 hours. Half-life is 2-3 hours. 70% of morphine is metabolised in the liver to inactive metabolites, 3% is metabolised into morphine-6-glucuronide, which is more potent than morphine. 90% of morphine and its metabolites are excreted by the kidney. 7%-10% is excreted in faeces, mainly in bile. Side effects include respiratory depression, mood swings, miosis, hypothermia, nausea and vomiting, decreased gastric emptying, constipation, retention of urine, urticaria, pruritus, hypotension, bradycardia.
Precautions/contraindications
Prudence is in order in case of hypothyroidism, elderly patients, cardiovascular disease, liver and renal insufficiency, recent bowel surgery, epilepsy or treatment with MAO inhibitor.
Remifentanil
This is an opioid agonist with strong analgesic properties. Remifentanil is metabolised in blood and tissues by non-specific esterases. It is excreted by the kidney. Half-life is 3-10 minutes. It is very short-acting. When postprocedural pain is to be expected, other means of pain treatment should be started before remifentanil infusion is stopped. Remifentanil is administered by continuous infusion only. Because of risk of respiratory depression and thorax muscle rigidity, bolus injections are not recommended. In case of insufficient analgesia, the infusion rate must be increased.
COMPARISON OF MEDICATION
Midazolam alone versus midazolam combined with opioids showed similar pain, discomfort, hypoxemia and patient memories of the procedure. Moreover, midazolam alone compared to opioids alone showed comparable results for hyoxemia, patient memories, pain, hypercarbia and respiratory depression. Etomidate alone reported shorter sedation times than midazolam alone with similar recovery agitation, oxygen levels and apnoeas.
Patients treated with propofol for moderate sedation had a faster recovery and less hyoxemia than patients treated with midazolam. Similarly patients treated with propofol recovered faster and had a lower recall frequency than patients treated with diazepam. However, combining propofol with midazolam resulted in deeper sedation than propofol alone. Propofol and remifentanil also showed deeer sedation, less patient recall but more respiratory depression than remifentanil alone. When propofol was combined with ketamine, deeper sedation and more respiratory depression and hypoxia was found than with propofol alone. Propofol versus ketamine showed similar pain, recovery, sedation and oxygen levels.
Ketamine alone versus midazolam alone reported similar sedation scores, recovery time, recovery agitation and oxygen levels. Ketamine versus midazolam with fentanyl, showed lower sedation depth for ketamine but similar pain, hypoxemia and patient recall.
REVERSAL AGENTS
Specific reversal agents are available for opioids (naloxone) and benzodiazepines (flumazenil). Naloxone reverses opioid-induced sedation and respiratory depression. Acute reversal can, however, lead to pain, hypertension, tachycardia and pulmonary oedema. Flumazenil antagonises sedation and ventilatory depression induced by benzodiazepines. These reversal agents should be immediately available whenever opioid analgesics and/or benzodiazepines are administered for sedation/analgesia. Patients who become hypoxemic or apnoeic during sedation/analgesia should:
1) Be encouraged to take deep breaths;
2) Receive supplemental oxygen (face mask);
3) Receive positive pressure ventilation if spontaneous ventilation is inadequate.
These actions happen before or concomitantly with pharmacologic reversal. Reversal agents should be administered when airway control or spontaneous ventilation are inadequate. Since the effect of reversal agents can dissipate before the effect of opioids or benzodiazepines, sedation and cardiorespiratory depression can recur. Patients should therefore be observed long enough to ensure that this is not the case.
Flumazenil
This reversal agent antagonises central effects of benzodiazepines. Dose: 0.2 mg in 15 seconds. After one minute, if necessary, repeated boluses of 0.1 mg are titrated until the desired effect is achieved. The maximum dose is 1 mg. Flumazenil is metabolised in the liver into inactive metabolites. Half-life is 50-60 minutes. Side effects include nausea and vomiting and palpitations, shivering and convulsions after fast injection.
Naloxone
This is an opioid antagonist. After intravenous injection, the effect can be seen after 1-2 minutes and lasts 1-4 hours. It is recommended that the dose be titrated in 0.04-0.08 mg increments and that there should be a wait of 2-3 minutes between doses until the desired effect is achieved. By carefully titrating the dose, it can be possible to reverse respiratory depression without eliminating all the analgesic effect and without producing unwanted side effects, such as nausea and vomiting .
Naloxone is metabolised in the liver into inactive metabolites and excreted by the kidney. Half-life is 45-90 minutes. Side effects include nausea, vomiting, sweating, dizziness, hypertension, tachycardia, epileptic insults, cardiac arrest and recurrence of pain since the effects of opioids are counterbalanced.
ANTIEMETICS
Postoperative nausea and vomiting with sedation and analgesia are common with an incidence of 50% and 30%, respectively. The exact mechanism by which they develop is not known. There are several factors that play a role, including patient-related factors (female sex, non-smoking status, younger age and a history of postoperative nausea and vomiting or motion sickness), anaesthesia-related factors (general anesthesia, volatile anaesthetics, nitrous oxide, use of opioids) and surgery-related factors (duration and type of surgery) . Reducing baseline risk factors is a necessary step in prevention of vomiting and nausea. These measurements include: use of regional rather than general anesthesia; avoidance of nitric oxide and volatile anesthesia; preferable use of intravenous propofol; adequate hydration and minimalizing opioids.
Currently available antiemetics include 5-HT3-receptor antagonists which block serotonin receptors (e.g., dolasetron, granisetron, ondansetron), dopamine antagonists which act in the brain (e.g., domperidone, olanzapine, droperidol, haloperidol, metoclopramide), H1 receptor antagonists (e.g., cyclizine, meclozine, promethazine, hydroxyzine), NK-1 receptor antagonists (aprepitant, casopitant and rolapitant), antihistamine (meclizine) and dexamethasone. First generation 5HT3 antagonists have been associated with QTc prolongation. Therefore dolasetron is no longer used in the US because of its risk for QRc prolongation and torsade de points. However, combining an 5HT3 with droperidol did not increase QTc. Dexamethason may increase blood glucose levels and risk of infection up to 6 to 12 hours after administration.
Currently there is no evidence for routinely giving anti-emetics. When a patient has multiple risk factors for nausea, it is advised that a multimodal antiemetic prophylaxis is given (Figure 3) A combination of multiple different acting drugs has shown to be more effective than prophylaxis with a single agent. Prophylaxis should only be readminstered after more than 6 hours.Ondansetron 4 mg, droperidol 1.25 mg, and dexamethasone 4 mg were equally effective and each reduced risk of nausea and vomiting with 25%. Balanced antiemetic treatment is most effective, although the development of nausea and vomiting can never be prevented in 100% of cases. Type of medication should be individually chosen based upon risk profile of the patient .
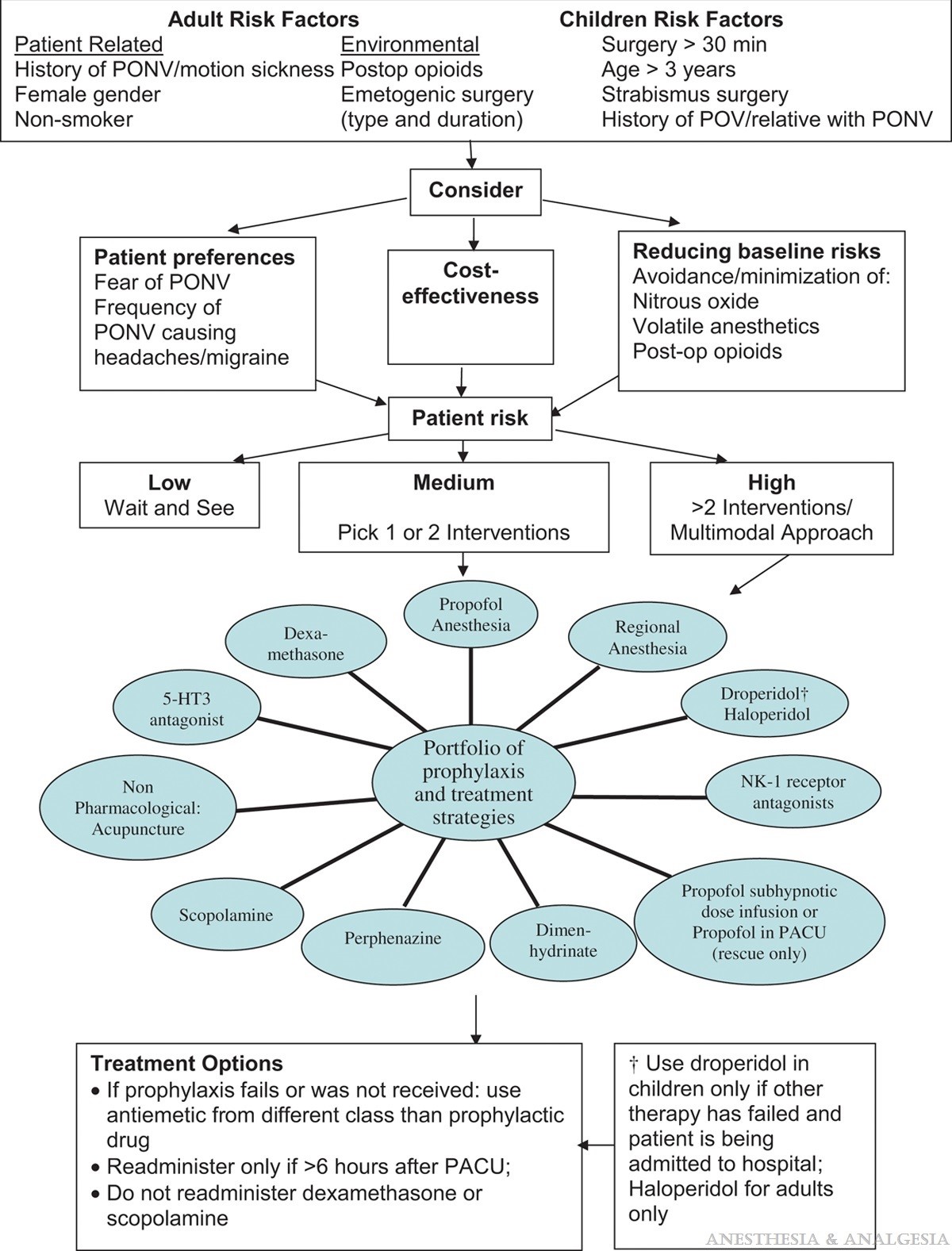
Figure 3
Proposed treatment regimen for local anaesthestic toxicity using IVLE
Recovery
After the procedure, patients must be observed carefully in a recovery area with the same monitoring possibilities. After moderate sedation, patient should be monitored until they meet discharge criteria. These criteria should be individually assessed and depend on the condition of the patient, the procedure and the level and type of anesthesia. Oxygenation is monitored until patients are no longer prone to respiratory depression . The recovery area should be adequately equipped with piped oxygen, suction possibilities, a crash trolley, masks with self-inflating bags and the same monitoring capabilities as during the procedure. Directly after the procedure, when the unpleasant or painful stimulus is removed, patients are at increased risk. Recovery area personnel is trained in early detection of complications. Vital signs and level of consciousness should be monitored frequently. Discharge can occur when the patient meets the following criteria:
- The patient is fully alert and orientated. When impaired at baseline, patients mental and physical status should be back at baseline level.
- Vital signs (cardiovascular function, airway patency and reflexes) have returned to normal values for this particular patient and are stable.
- Pain, discomfort, nausea and vomiting are under control within acceptable limits.
- Reversal agents should be given up to two hours before discharge. When its effects wears off, patients can become re-sedated.
- Patients discharged home should be accompanied by a responsible adult and information should be given about possible complications, diet, medication, lifestyle and contact details in case of an emergency.
If the patient is to go home, an accompanying person is responsible for the transport home and the care for the first 24 hours. Detailed and written instructions on how to deal with (severe) pain, bleeding, nausea and vomiting are given, including first-aid referral contact details.
Pain management
PAIN MEASUREMENT
There are several graphic pain scales that score the pain and help to assess the efficacy of the pain management. These include the Visual Analogue Scale (VAS), Numerical Rating Scale (NRS) or face scales, with VAS and NRS being most widely used. Typically these scales measure pain on a scale of 0 (no pain at all) to 10 (worst pain ever). Patients identify a number while viewing the scale, by placing an X or identify a matching face expression on a chart . Pain should be treated stepwise according to the analgesic ladder of the World Health Organization (Figure 4).
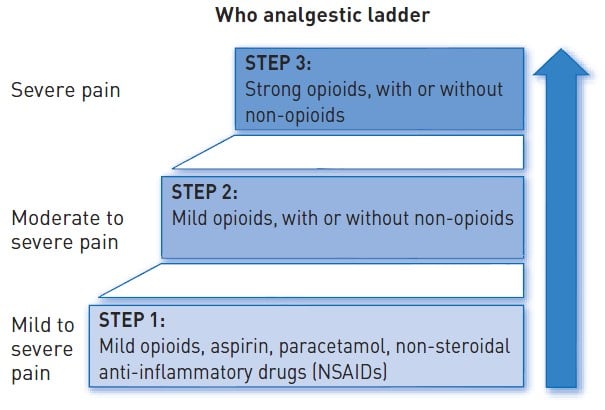
Figure 4
World Health Organisation Analgesic (Pain Relief) Ladder
LOCAL ANAESTHETICS
Local anaesthetics should be used for all percutaneous interventions at the puncture site, irrespective of the use of sedation and/or systemic analgesia. Lidocaine 1% or 2% is often used for this purpose; however, longer-acting local anaesthetic agents may also be used. To provide a marker for intravascular injection, epinephrine (5 mcg/ml or 1:200,000) could be added to local anaesthetic solutions. Vasoconstrictors also decrease the rate of vascular absorption, thereby improving the depth and the duration of anaesthesia. The extent to which epinephrine prolongs the duration of anaesthesia depends on the specific local anaesthetic used . Local (infiltration) anaesthesia is mainly used for effective pain relief during the procedure, but it can also be very effective for treatment of post procedural pain. Table 4 summarises the properties and maximal recommended doses for commonly used local anaesthetic agents.
Local anaesthetics block the generation and conduction of nerve impulses by blocking voltage-gated sodium channels. Small fibres are more sensitive than large nerve fibres and myelinated fibres are blocked before non-myelinated fibres of the same diameter. The nerve becomes inexcitable, it cannot transport impulses. Clinically, the loss of nerve function is manifested as loss of pain, temperature, touch, proprioception and then skeletal muscle tone .
High plasma concentrations of local anaesthetics can lead to toxicity. Sodium channels in other tissues become blocked. In the central nervous system this may cause loss of consciousness and seizures. In the heart it may cause heart block and malignant re-entry rhythms with ventricular fibrillation that may be resistant to electrical defibrillation. In vitro cardiovascular toxicity does not develop before the blood concentration is three times the concentration needed for convulsions. Patients with cardiac toxicity may therefore require prolonged cardiopulmonary resuscitation until local anaesthetic levels fall sufficiently for a normal rhythm to be restored . Moreover, local anaesthetics can cause conduction disturbances in the heart with the same mechanism as it does for the nerve block.
Because of this, maximal doses have been formulated for local anaesthetics. However, these maximal doses do not apply when local anaesthetic is being injected directly into a vessel. In most cases, systemic reactions from local anaesthetics are due to inadvertent intravascular administration, as opposed to a gross excess of local anaesthetic use . Allergic reactions to local aesthetics is rare, but some patients can react to its preservatives . It is preferable to use ropivacaine and levobupivacaine for infiltration anaesthesia because of their long duration of action and their more favourable profiles in view of the chance of toxicity. Signs and symptoms of toxicity are given in Figure 5.
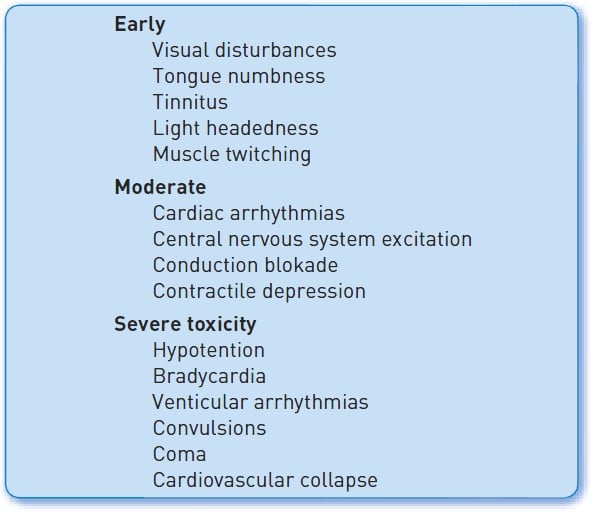
Figure 5
Possible signs and symptoms of local anaesthetic toxicity
Systemic analgesia
Studies have shown that postprocedure comfort largely depends on the perprocedural experience of the patient. During interventional procedures under standard care conditions, pain increases with the length of the procedure, regardless of the amount of drugs given . Sometimes, patients receive premedication in adjunct to preprocedure sedation and analgesia. Premedications and interprocedural drugs can carry over their therapeutic and adverse effects into the recovery period.
In acute coronary syndrome patients, it is important to realize that morphine delays oral P2Y 12 platelet inhibitor absorption and may be associated with adverse outcomes after myocardial infarction . The PACIFY single-centre trial included patients undergoing coronary angiography and randomized to intravenous fentanyl or not. All participants received local anaesthetic and intravenous midazolam. Those requiring PCI with stenting received 180 mg oral ticagrelor intra-procedurally. They found that fentanyl administration can impair ticagrelor absorption and delay platelet inhibition . The question remains whether differences in platelet reactivity limited to the first 2 hours after percutaneous coronary intervention translate into an increased risk of thrombotic events. In daily practice, patients will have been treated with a bolus unfractionated heparin during percutaneous coronary intervention. Unfractionated heparin has a plasma half-life of ≈60 to 90 minutes, ensuring adequate antithrombotic protection during that period . A systematic review of 11 studies did not show evidence of increased risk of poor clinical outcomes with intravenous morphine analgesia in patients undergoing primary PCI for STEMI .
In PACIFY there was a marginally lower numerical pain level in those who received fentanyl in the full PACIFY sample (2.3 vs. 1.5 on a 10-point scale, p = 0.14); although the absolute difference was small, statistically non-significant and of uncertain clinical significance. It should be noted that all patients received midazolam, which can cause post-procedural amnesia and could affect patient-reported intra-procedural pain and anxiety.
Anxiety
During CAG or PCI, many patients experience procedural anxiety. Prevalence rates are as high as 24% to 72% , , , . Benzodiazepines are traditionally administered pre-procedurally. Vlastra et al. studied 1682 patients undergoing CAG or PCI. These patients were randomized according to monthly rotational periods into: lorazepam 1 mg sl, oxazepam 10 mg/po, diazepam 5 mg/po, midazolam 7.5mg/po or no premedication. They showed that pre-procedural lorazepam or diazepam had a modestly positive effect on anxiety levels during the interventional procedure. However, oral oxazepam and midazolam did not reduce procedural anxiety.
Non-pharmacological interventions can also reduce periprocedural anxiety. Massage or guided imagination prior to the procedure led to lower self-reported peri-procedural anxiety in three randomized controlled trials , , . Relaxing music provided by an audiopillow was also associated with lower anxiety levels around the procedure . Aromatherapy and mindfulness-based interventions may also have a beneficial effect on anxiety , . However, it is difficult to compare the effects of these interventions to medication. Nevertheless, their possible adverse effects are negligible as compared to medication.
Procedural sedation and analgesia is increasingly used among PCI patients. A recent survey among interventional cardiologists reported that 67% of catheterization patients were sedated. In the United States 92% of cardiologists used sedation during CAG and PCI, while mostly using benzodiazepines and fentanyl. On the contrary, European interventional cardiologists used sedation in only half of the cases and solely 38% of patients from European cardiologists received any form of sedation .
The reason for this difference in sedation practice is probably multifactorial. First, the perception and also treatment of pain is different. In the US, pain is treated more aggressively and opioids are more often used for acute and chronic pain. Therefore opioids are also increasingly used as premedication. Second, both patients and physicians fear perprocedural pain which increases the use of routine fentanyl application. North American cardiologists more frequently believe that most patients would like to receive sedation than their colleagues from other countries (85% vs 30%) , .
Nonetheless routine opioid use is not without risk . Antiplatet inhibition is highly important for the short- and long-term success of PCI. Morphine interacts with oral P2Y12 inhibitors which result in delayed effects and lower blood concentrations of these P2Y12 inhibitors , , . Fentanyl is the most commonly used opioid for procedural sedation and analgesia during CAG and PCI , . Some countries widely use fentanyl together with benzodiazepines (e.g. diazepam or midazolam), however international guidelines on PCI do not specifically recommend this approach. Randomized studies on potential side effects of fentanyl during CAG or PCI are scarce. However, available evidence reports lower patient discomfort and pain after the administration of intravenous fentanyl, irrespective of co-administration of benzodiazepines. Hemodynamic responses did not vary significantly . Hemodynamic stability was better in patients treated with midazolam with or without fentanyl, as compared to placebo only. Here sedation scores, anxiety and patient/cardiologist satisfaction did not differ . Furthermore, fentanyl use was associated with a greater reduction in mean pain scores as compared to local anesthesia with lidocaine; to the combination of sedation and local anesthesia and to patients without premedication. Also, patients treated with sedation less frequently needed an additional analgesic during the procedure as compared to patients treated with only local lidocaine and to patients treated with both local anesthesia and sedation . On the contrary, pain perception when analgesics were administered before removing the femoral arterial sheath after PCI was not altered .
Resuscitation
Patients who undergo an intervention in the cardiac catheterisation laboratory run the risk of developing complications. Depending on the type of intervention performed, the nature of the complication and patient characteristics, these complications vary from minor to situations that can rapidly be life-threatening, e.g., ventricular arrhythmias, AV heart block, coronary artery complications such as perforation, air emboli, and allergic reactions. It is also possible that patients already need resuscitation on arrival in the cardiac catheterisation laboratory due to cardiogenic shock, pulmonary oedema or cardiac arrest. In addition, the advance of 24/7 direct access to the cardiac catheterisation laboratory by patients following acute myocardial infarction and out-of-hospital cardiac arrest means that the resuscitation protocol and skills must be integrated into the standard practice.
The American Heart Association (AHA), the European Resuscitation Council (ERC) and the International Liaison Committee on Resuscitation (ILCOR) have developed resuscitation guidelines that have been revised in 2015 . It is advisable for all personnel in the cardiac catheterisation laboratory to be familiar with the principles of basic and advanced life support. However, it is out of the scope of this chapter to discuss these guidelines fully here. They can be found in recommended references , , listed at the end of this chapter (Figure 6A and Figure 6B).
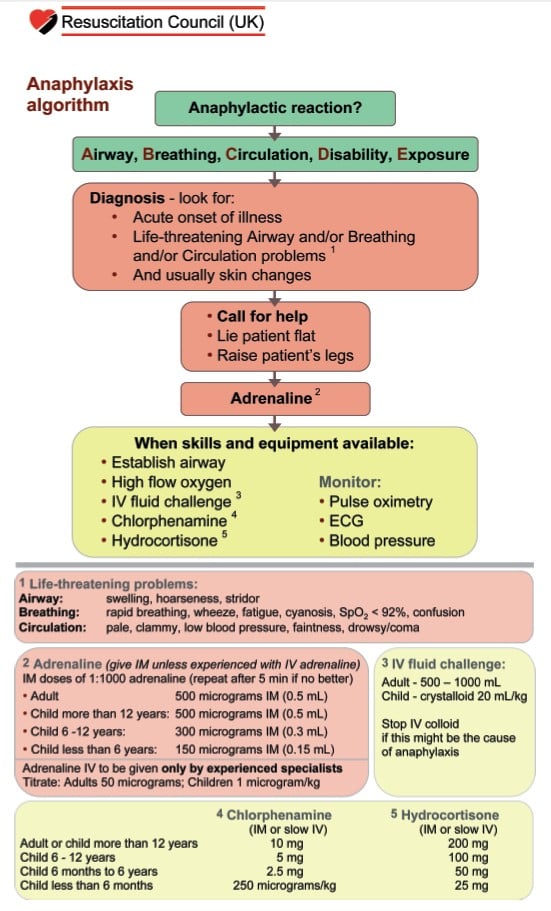
Figure 6A
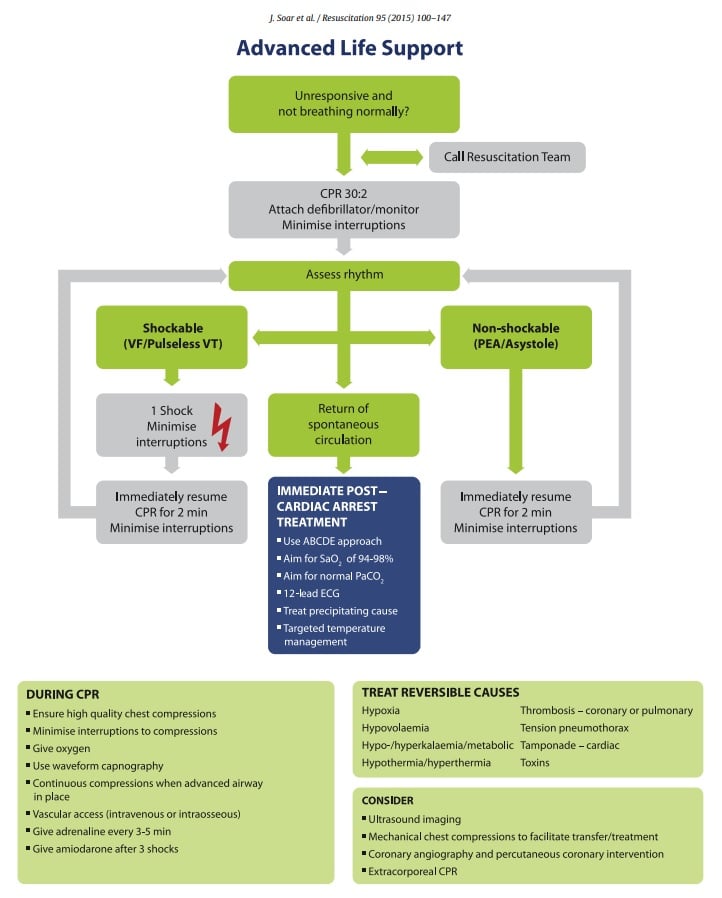
Figure 6B
Latest resuscitation guideline algorithm
REQUIRED EQUIPMENT IN THE CARDIAC CATHETERISATION LABORATORY
The American Society of Anesthesiologists (ASA) has developed guidelines for anaesthetic care delivered outside the operating suite , . These guidelines state that these are minimal guidelines which may be exceeded at any time as deemed necessary. The guidelines recommend that:
- Antagonists for benzodiazepines and opioids are immediately available. A team member in the catheterization laboratory should fully understands the pharmacology of anaesthetics, sedatives and its interactions.
- One person should be trained in early recognition and treatment of airway complications and ventilation problems.
- A defibrillator is present in the room.
- There is a reliable source of oxygen with backup supply. Oxygen piped from a central source is strongly encouraged. Oxygen supply should be enough for the length of the procedure.
- There is a suction source.
- In case inhalation anaesthetics are administered, there should be an adequate and reliable system for scavenging waste anaesthetic gases.
- There is a self-inflating hand resuscitator bag capable of administering 90% oxygen.
- There are anaesthesia drugs, supplies and equipment for the intended anaesthesia care.
- There is adequate monitoring equipment equivalent in function to that when used in operating rooms.
- There should be sufficient electrical outlets including outlets connected to emergency power supply.
- There should be adequate illumination of the patient, anaesthesia machine (when present) and monitoring equipment.
- There should be sufficient space to accommodate necessary equipment and personnel and allow access to the patient, anaesthesia machine (when present) and monitoring equipment.
- There should be an emergency cart with defibrillator, emergency drugs and other equipment to provide CPR.
- There should be trained personnel to support the anaesthesiologist with a means of two-way communication to request assistance.
- Appropriate post-anaesthesia management can be provided. Adequate personnel and equipment should be available for safe transport of the patient.
- Catheterization laboratory personnel knows how to alert the emergency advanced life support team, e.g. dedicated telephone number or button.
Although sedation, as intended in this chapter, is not equal to anaesthesia, we strongly recommend that these guidelines are followed in all settings when patients receive medication which alters pulmonary, cardiac and neurological function. Because of patient positioning and the movement of the table as well as the x-ray gantry, access to the patient can be a challenge (Figure 7). Furthermore, we would like to mention the need for radiation protection and we would advise new anaesthetic staff to familiarize themselves with the environment of the catheterisation laboratory beforehand, because of differences with other working areas. We would also like to emphasise that cardiopulmonary resuscitation should be considered any time an individual cannot adequately oxygenate or perfuse vital organs, not only following cardiac or respiratory arrest , .

Figure 7
MECHANICAL CHEST COMPRESSION
Over the last 10 years, several types of mechanical chest compression devices have been developed which can be used to deliver cardiopulmonary resuscitation (CPR). These devices rhythmically apply a force to the thorax of the patient through different mechanisms such as load-distributing bands, pistons and pneumatic vests. A load-distributing band is a wide band attached to a short backboard and is placed around the thorax of the patient. The band is then mechanically and rhythmically shortened and lengthened. Piston devices use compressed gas to drive a piston placed over the lower sternum of the patient. Some of these devices provide active compression/decompression CPR by using a suction cup. It is thought that in this way blood is pushed out of the heart and then respiratory gases and blood are sucked back into the thorax during the active decompression phase. Pneumatic vests are worn by the patient like a life vest. Rapid introduction of air into the vest causes chest compression , . The use of these mechanical devices has been proposed to improve CPR outcome since these devices deliver the right depth and rate of compressions without interruptions or fatigue. A Cochrane Review comparing mechanical and manual chest compressions concluded that evidence does not suggest that mechanical compression machines are superior to conventional manual chest compressions. One randomized controlled trial even showed worse neurological outcomes in mechanical chest compressions . The other six included studies did not find different neurological outcome or survival . However, a meta-analysis was not possible because of heterogeneity. They also point out that, in using these mechanical devices, one must pay attention to avoiding sternal or rib fractures. Effectiveness of compressions should be monitored as body posture can interact with the treatment effect due to the design of the device.
Cardiac arrest in the catheterisation laboratory during interventions is a circumstance in which the use of a mechanical compression device may offer special benefits. Often, continuing the intervention is the best option for attaining return of spontaneous circulation. Continued manual compressions with simultaneous intervention are exceedingly difficult to perform effectively. The use of a, mostly radiotranslucent, mechanical device enables continued intervention while maintaining chest compressions. Although there is no evidence for a better outcome in general, the use of a mechanical device may be considered for the following reasons: CPR may be maintained for a longer time, the personnel is protected from x-rays and there is no need for extra personnel to guarantee proper chest compressions for a longer time (Figure 8) .

Figure 8
Mechanical chest compression devices
RESUSCITATION IN COVID-19 PATIENTS
Resuscitation can generate COVID-19 aerosols by chest compressions, airway and ventilation interventions. COVID-19 is highly contagious and the main transmission route is by these respiratory secretions. These secretions can fall onto surfaces within two meters as droplets from the patient, but smaller airborne particles can remain in the air for a longer period . Every patient undergoing a procedure in the catheterization laboratory should be assessed for COVID-19 symptoms in advance. The European Resuscitation council recommends an adjusted resuscitation protocol for COVID-19 patients. (see algorhythm in Figure 9). Team size should be restricted and optimized. Everyone should wear appropriate personal protective equipment (PPE) with minimally an FFP3 mask, eye and face protection, long-sleeved gown and gloves. In case of shockable rhythm, up to 3 consecutive shocks can be given while putting on PPE. Also, a viral filter on the airway management should filter exhaled breaths. Manual ventilation with an ill-fitting mask will generate aerosols, therefore manual ventilation with a bag-mask should be limited and only performed by experienced staff. Rapid intubation prevents aerosols leaking from manual ventilation with the bag-mask. Also consider early stopping of CPR when reversible causes of arrest have been ruled out.
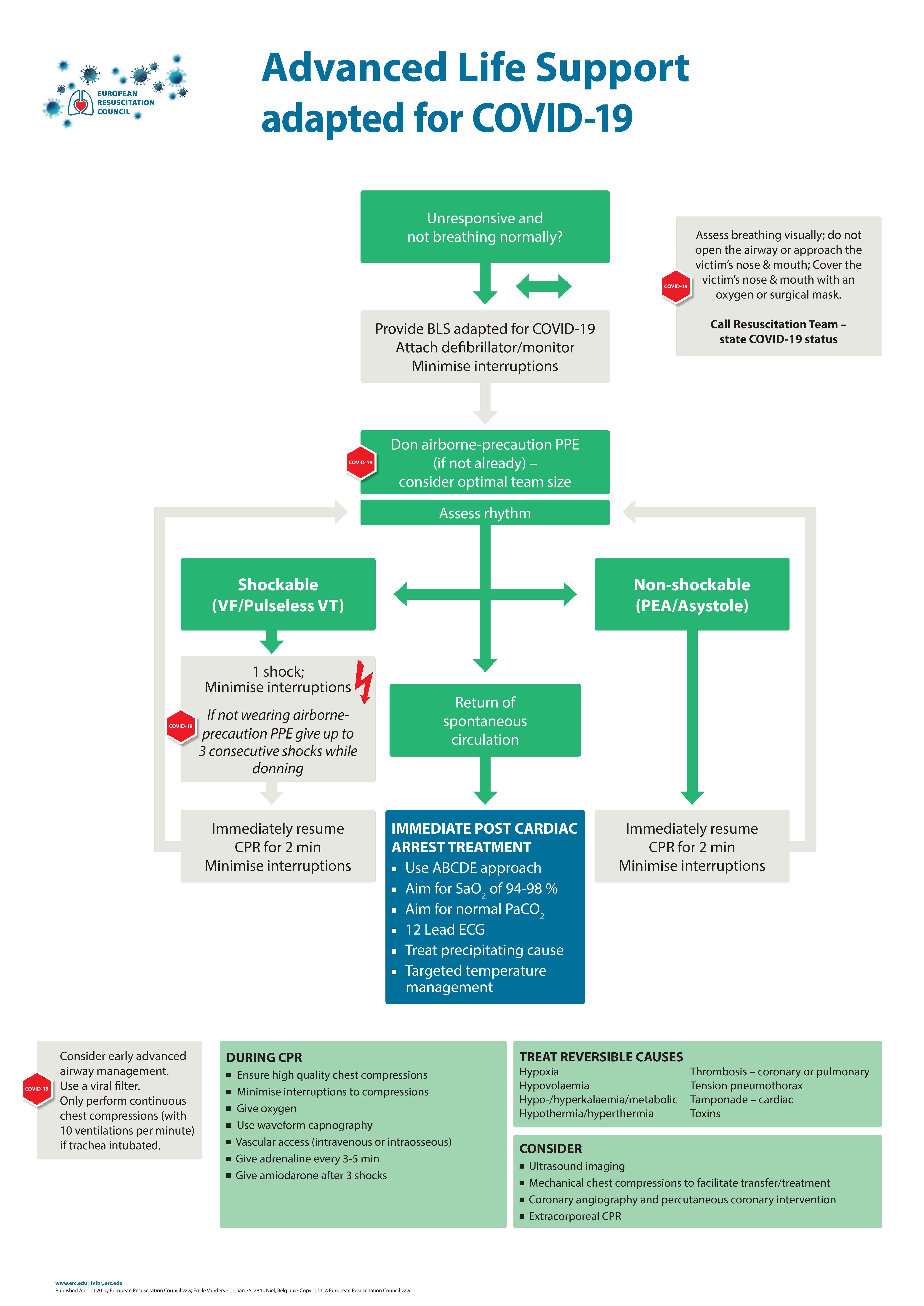
Figure 9
In a cohort of 136 in hospital cardiac arrests from Wuhan, return of spontaneous circulation was achieved in 18 patients (13%) of whom 3% survived 30 days and only one (<1%) had a favourable neurological outcome.
Personal perspective – Ronak Delewi
Pain and anxiety in the catheterization laboratory is frequently undertreated. This can have a massive impact on patients’ experience. Severe pain or anxiety may lead to patient delay in next episodes of cardiac symptoms. Moreover, untreated pain is associated with poorer hemodynamic stability during the procedure. Patient’s discomfort could lead to operator’s distraction from the job that needs to be done. Hence adequate training of catheterization laboratory staff on identifying and treating pain and/or anxiety should be done routinely. They need to be trained properly regarding the medication used, the risks involved and the steps to be taken in case of an emergency. Therefore, I would always recommend monitoring the patient extensively, and using medication for which a reversal agent is available. Also, non-pharmacological interventions are essential to reduce anxiety and pain. In my opinion and based on empirical evidence, a chat and a genuine interest in the patient’s wellbeing at the start of the procedure makes all the difference.