Gregory Ducrocq, Thomas R.D. Shaw, Habib Gamra, Peter C. Block, Neil R. Grubb, Carlos E. Ruiz, Alec Vahanian
Mitral valve replacement and repair
Updated on November 22, 2022
In recent years, transcatheter mitral repair procedures have emerged as an alternative therapeutic option to treat inoperable and high-risk surgical patients. Currently, the device with the widest clinical use is the MitraClip System (Abbott Vascular, Santa Clara, CA, USA), which has been proved to be a safe and effective tool to treat high-risk patients with both degenerative (DMR) and functional (FMR) mitral regurgitation (MR) . Other technologies, including chordal repair and annuloplasty, are emerging which will enrich the toolbox to repair the mitral valve with a transcatheter approach, and will make percutaneous approaches competitive with surgical repair .
However, although transcatheter repair has been associated with clinical improvement in different clinical settings, it is technically demanding and is associated with a 10-20% rate of persistent or recurrent MR >2+ after one year in different series, especially in the early experiences, largely depending on patient selection . Indeed, patient eligibility represents a limitation of transcatheter mitral repair, suggesting the need for a complementary and more reproducible percutaneous therapy.
Transcatheter mitral valve implantation (TMVI) with a transcatheter aortic prosthesis is already an option available for those patients with previous open-heart surgery and a degenerated bioprosthesis or with recurrent MR following annuloplasty (valve-in-valve and valve-in-ring procedures). In selected cases, an aortic valve transcatheter device can be implanted in patients with a severely calcified annulus, while implantation in non-calcific valves requires ad hoc devices.
Although transcatheter mitral implant in a native anatomy introduces a number of challenges, the feasibility of TMVI in human has recently been reported in high-risk patients with FMR and DMR.
TMVI has, overall, the potential to be more reproducible than repair, being applicable to many patients (one valve for all), and is also associated with predictable results regardless of anatomy.
The mitral valve apparatus is a very complex dynamic system involving several structures, interacting with the left ventricle, the left atrium and the aortic valve. There is a functional and anatomical continuity between the mitro-aortic annulus and the lateral wall, where the papillary muscles are attached. Such continuity has been recognised as important to maintain the structural and functional integrity of the left ventricle. The mitral valve is composed of a septal (anterior) leaflet, single, large and of triangular shape, which separates the inflow from the outflow of the left ventricle. Mobilisation of the anterior leaflet towards the interventricular septum may induce left ventricular outflow obstruction. This has been observed following transcatheter valve implantation, while it is seldom the case after surgical replacement since the anterior mitral leaflet is generally removed. The posterior leaflet is divided into multiple scallops, usually three: a lateral, a middle, and a medial scallop. There is wide variability in the shape and size of the leaflets, as well as in the distribution of chordae and papillary muscles. However, in most cases, the two papillary muscles (anterolateral and posteromedial) are connected symmetrically to both leaflets: each papillary muscle serves its half of the valve, with variable morphology of its head. In most cases, however, there are multiple heads serving one valve segment functionally and anatomically (typically three heads, serving the anterior leaflet, the commissure and the posterior leaflet). It is not rare to identify additional papillary muscles between the two main ones, and serving the middle scallop of the posterior leaflet individually.
From a purely technical standpoint, TMVI has several challenges. The first and most intuitive is related to the size of the anatomy. In patients with chronic MR the annulus is usually dilated, and large devices are required to obtain adequate fixation and sealing. Therefore, large delivery systems (≥24 Fr), which are not suitable for transfemoral approaches, are required on most occasions. The first-generation TMVI devices are based essentially on the transapical approach, which also allows ideal coaxiality to the mitral valve apparatus. As an alternative, to allow access for large delivery systems, the direct transatrial approach was initially used for mitral valve-in-ring procedures, but has essentially been abandoned because of suboptimal coaxial alignment. Transfemoral transarterial retrograde and transseptal (transfemoral or transjugular) approaches are complementary options for percutaneous TMVI delivery. However, all of them are challenging, given the angulation involved and the dimensions and inflexibility of the large devices. The transfemoral transseptal approach has already been successfully achieved in man and has future potential. On the other hand, with the transapical approach, complications of left ventricle (LV) apical access may be considerable, since the LV wall in heart failure patients with FMR is thin, and the LV is dilated, dysfunctional and arrhythmogenic. In addition, the influence of a surgical approach in end-stage heart failure patients could be unfavourable for ensuring the safety of the implant. Dedicated transapical closure devices for minimally invasive delivery are under development and may facilitate TMVI, but the role of the transapical approach in the future is questionable, as the devices will develop smaller profiles, become more steerable and more conformable, facilitating the transseptal approach.
Sealing and reliable fixation represent the major concerns of TMVI. Stable anchorage of the prosthesis to prevent displacement or migration is of extreme importance. Given the lack of heavy annular calcification in most patients, fixation methods relying solely on radial force are unlikely to be successful in the mitral position. Moreover, excessive radial forces increase the risk of compression and damage to adjacent structures such as the LV outflow tract (LVOT), the conduction system, the coronary sinus, the left circumflex artery, and the aortic root. Additional fixation elements are required to ensure proper fixation to the LV or to other components of the subvalvular apparatus.
Perivalvular regurgitation may be less tolerable in the mitral position compared to the aortic position, due to the high-pressure gradient across the mitral valve. Therefore, TMVI should aim for complete sealing. Different sealing solutions have been developed to enable effective interaction between the valve anatomy and the valves.
From an anatomical standpoint, the anatomical variations underlying MR introduce further challenges for prosthesis fixation, sealing and delivery. The anatomy variability is large between DMR and FMR: as an example, patients with Barlow’s disease have extreme excess of tissue and multisegmental prolapses which may prevent optimal fixation. On the other hand, patients with fibroelastic deficiency with small flails have fragile tissue, in which lack of tissue may not assure an adequate landing zone. The angle between the aortic and the mitral annulus, as well as the size of the ventricle, are the main predictors of left ventricular outflow tract obstruction following TMVI. Solutions to this issue include special fixation methods and various degrees of supra-annular valve configuration. However, the supra-annular design may induce flow disturbances at risk of thromboembolism, and the need for long-term anticoagulation. The precision of implantation and the configuration of the devices are crucial to minimise the risk of LVOT obstruction and left atrial protrusion. In this regard, the specific subgroup of patients with increased risk have to be clearly defined by further investigations.
Despite the major progress achieved over the past few decades, a significant proportion of patients who undergo mitral valve surgery require reoperation during follow-up. During the 10 years following mitral valve replacement or repair, reoperation is needed in 20% to 35% of patients . While redo surgery is the treatment of choice after bioprosthesis or ring annuloplasty failure, it may be associated with significant early mortality (5-12%), especially in patients with concurrent comorbidities .
Following the first descriptions of transcatheter aortic valve implantation (TAVI), treatment of failed aortic bioprostheses with transcatheter heart valve (THV) implantation has emerged as a promising alternative to redo surgery in high-risk patients. During the last four years, THV implantation, mainly using the SAPIEN/XT prostheses (Edwards Lifesciences, Irvine, CA, USA), has also been reported for treatment of failed mitral bioprostheses or rings, mainly through the transapical approach . Recently, other THV have been used in isolated cases .
1. Transapical approach
The procedure obeys the general principles of transapical TAVI. The J pre-shaped stiff wire is placed in the left atrium or upper right pulmonary artery after retrograde crossing of the mitral valve. The SAPIEN/XT/3 prosthesis is mounted upside down (in comparison with a transfemoral position) on the catheter in the retrograde orientation.
2. Transvenous, transseptal approach (Figure 1)
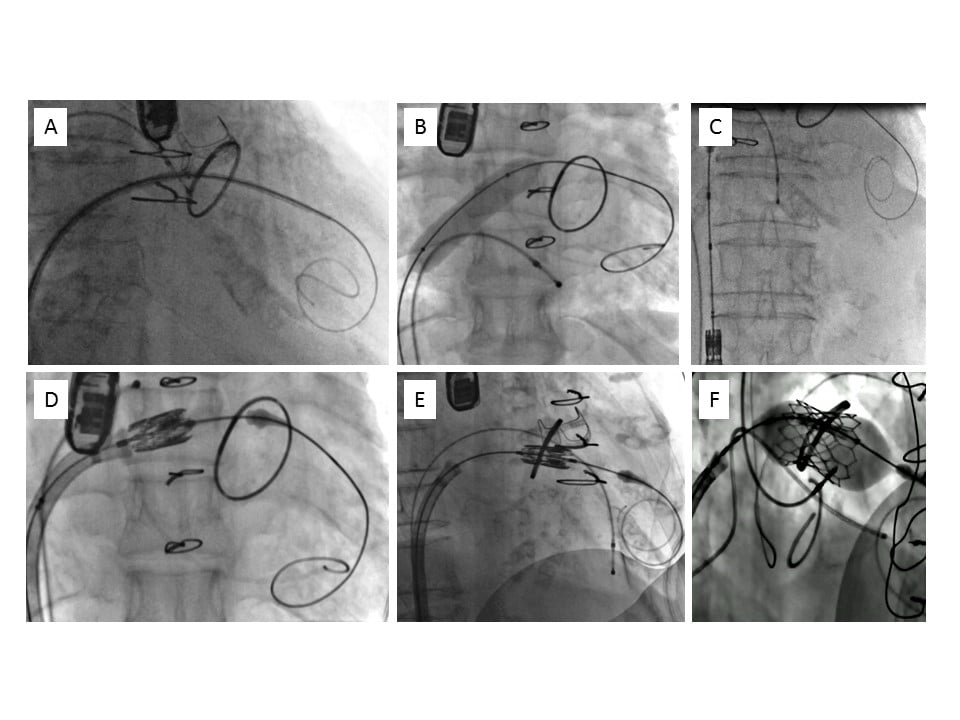
Transvenous, transseptal mitral valve-in-ring implantation.
A) After crossing the mitral ring, a J pre-shaped Super Stiff 0.035” guidewire is placed at the apex of the left ventricle.
B) The interatrial septum is dilated using 12-14 mm diameter peripheral balloons.
C) The SAPIEN/XT/3 valve is aligned in the inferior vena cava.
D) Using flexion of the catheter, the valve crosses the interatrial septum.
E) The valve is positioned within the mitral ring, in a perpendicular plane.
F) The valve is deployed using a slow and progressive inflation of the balloon.
The procedure is performed under general anaesthesia and transoesophageal echocardiographic (TOE) guidance. A bilateral femoral venous access is used. A temporary pacemaker lead is placed in the right ventricle as used during TAVI. Transseptal puncture is performed under TOE guidance in a “high “and “posterior” position in the fossa ovalis, similar to that used during MitraClip implantation. After placing a Mullins sheath in the left atrium, a bolus of heparin (70 IU/kg) is administered with the aim of achieving an activated clotting time of between 250 and 300 seconds. Then the mitral valve is crossed. The easiest technique consists in using a steerable Agilis™ catheter (St. Jude Medical, St. Paul, MN, USA), directed just in front of the mitral valve. Then, a 5 Fr Multipurpose catheter (Cook Medical, Bloomington, IN, USA) is advanced on a standard 0.035” guidewire. When the catheter has entered the left ventricle, a 0.035” Amplatz Super Stiff™ guidewire (Boston Scientific, Marlborough, MA, USA) with a “J” curve at the end is placed in the apex of the left ventricle (Figure 1A). The atrial septum is dilated using 12-14 mm peripheral balloons (Figure 1B). Regarding predilatation, the consensus is that it should be avoided for bioprostheses, because of the risk of fracture and embolisation of calcified degenerated leaflets, potentially leading to stroke or massive regurgitation. If it is mandatory because the valve cannot be crossed, it must be done with the utmost caution, using a very short inflation with an undersized balloon. Then the SAPIEN/XT/3 valve, mounted for antegrade implantation (similar to the position in transapical aortic valve procedures) on the catheter, is aligned and adjusted in the inferior vena cava and advanced through the atrial septum (Figure 1C, Figure 1D). The question of the orientation of the valve on the balloon catheter may seem obvious, but any lack of attention may lead to catastrophic consequences if the valve is crimped upside down. The THV is orientated towards the mitral valve and positioned using maximal flexion of the catheter in a projection perpendicular to the plane of the bioprosthesis/ring (Figure 1E). Implantation is performed by slow balloon inflation under rapid ventricular pacing (160-200 bpm) (Figure 1F). The final result of implantation is assessed by fluoroscopy (Figure 2) and TOE (Figure 3) in the catheterisation lab and CT before discharge. Contrast medium is not used during TMVI.
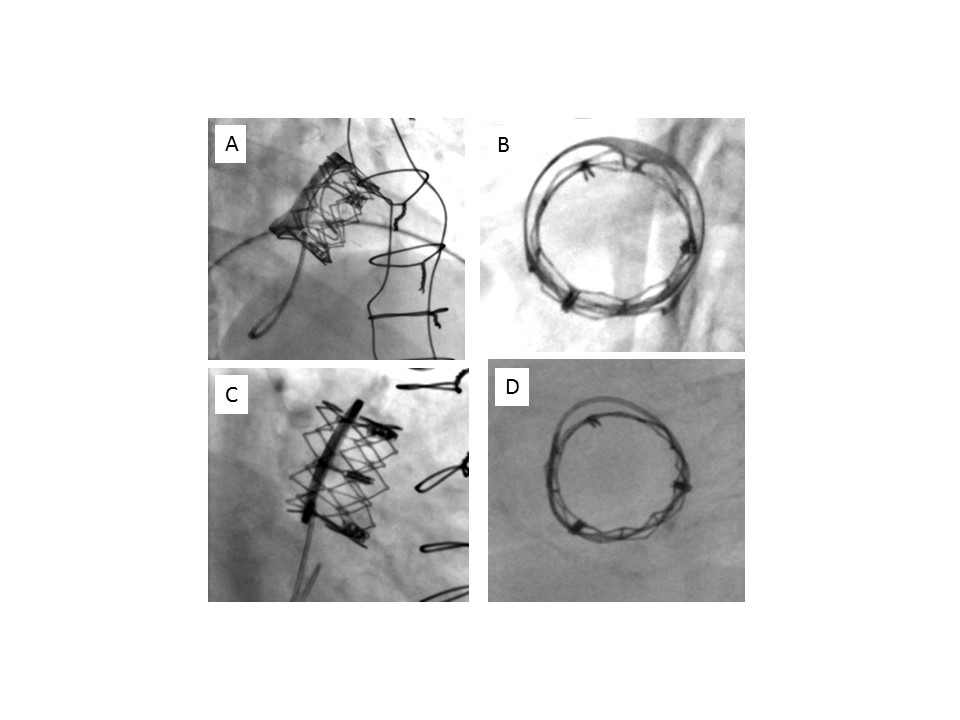
Immediate post-implantation fluoroscopic evaluation.
A) Valve-in-valve, profile.
B) Valve-in-valve, en face view.
C) Valve-in-ring, profile.
D) Valve-in-ring, en face view.
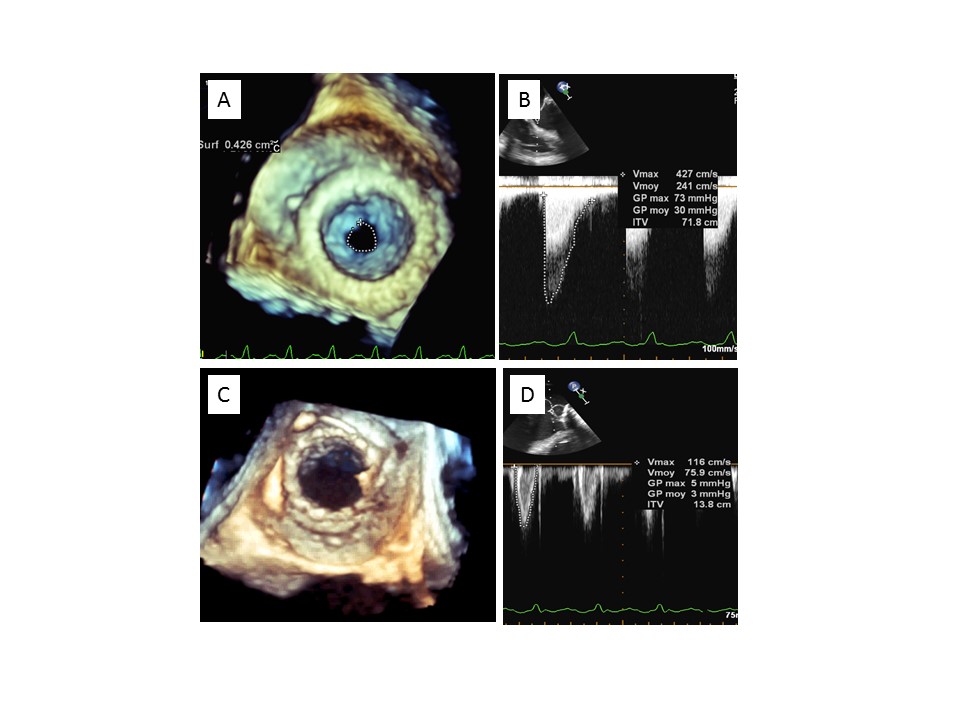
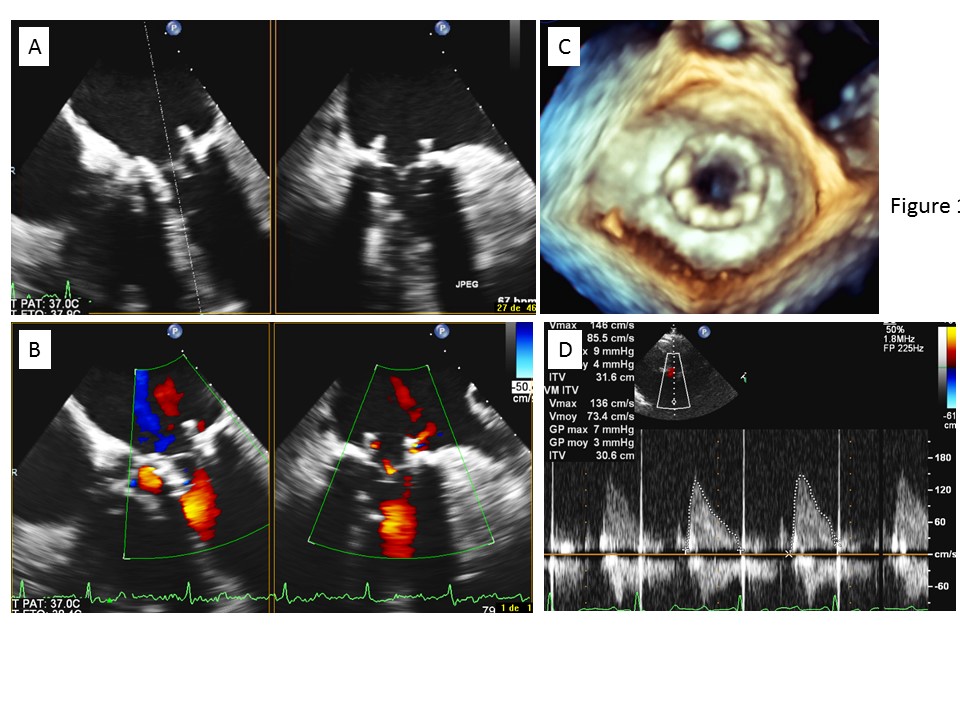
Immediate transoesophageal echocardiographic evaluation after transcatheter mitral valve-in-valve implantation.
A) Before implantation: 3D planimetry.
B) Before implantation: transprosthetic mitral gradient.
C) After implantation: 3D evaluation.
D) After implantation: transprosthetic mitral gradient.
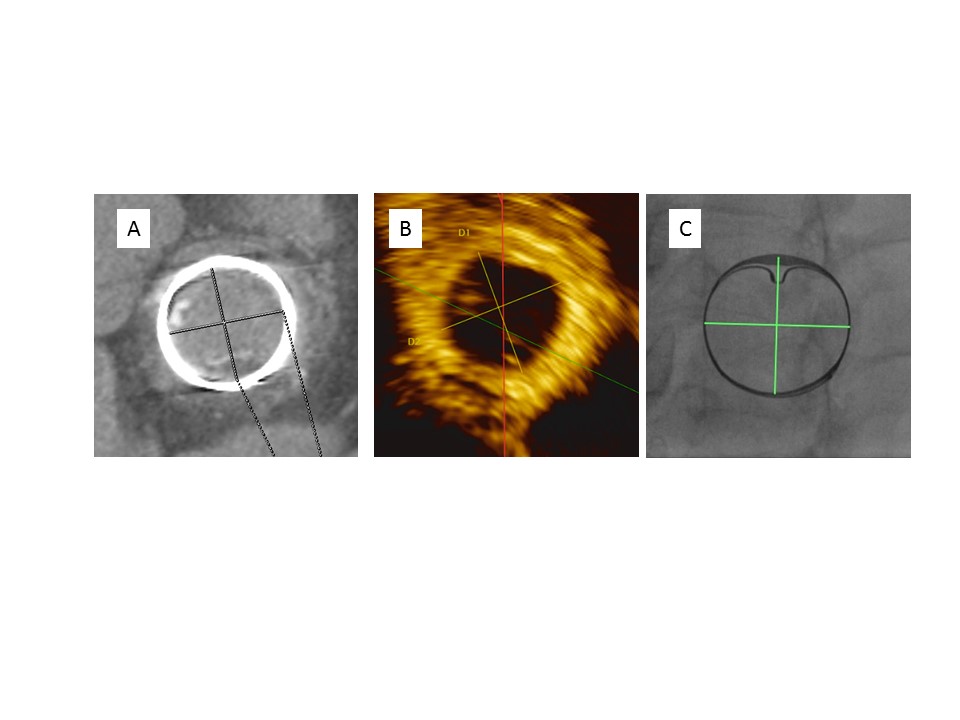
Figure 4. Multimodality imaging to measure valve inner diameters before transcatheter mitral valve implantation.
A) Computed tomography.
B) Transoesophageal echocardiography.
C) Fluoroscopy.
Multimodality imaging to measure valve inner diameters before transcatheter mitral valve implantation.
A) Computed tomography.
B) Transoesophageal echocardiography.
C) Fluoroscopy.
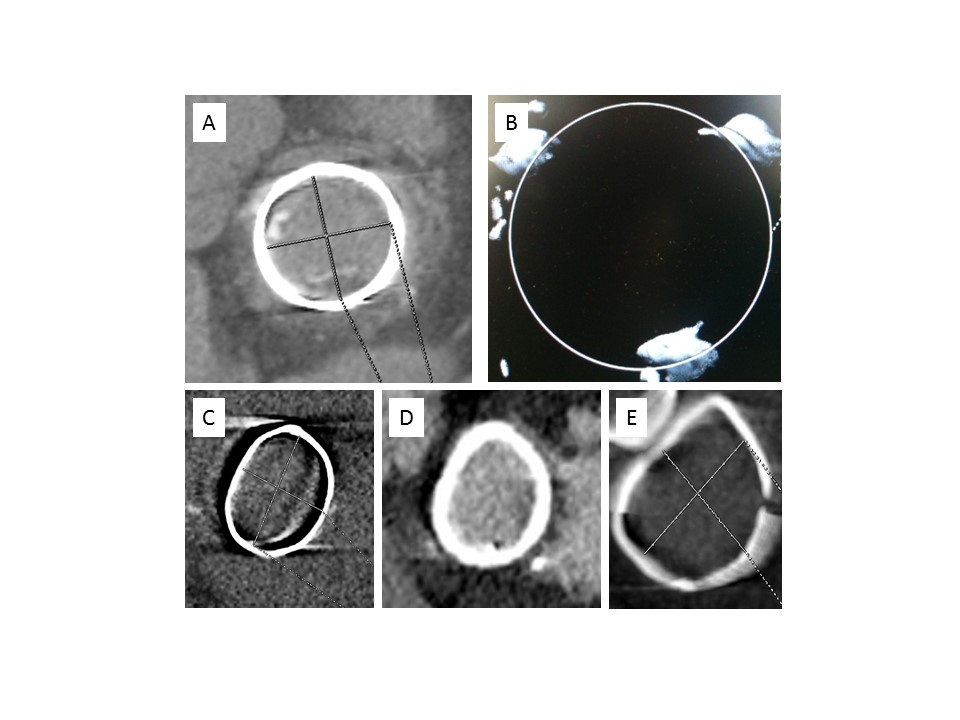
Computed tomography, various brands of surgical valves and rings commonly used.
A) PERIMOUNT valve: radiopaque ring, easy measurement of the inner diameter.
B) Mosaic valve: radiolucent ring, only three dots visible on the top of the frame.
C) Physio: semi-flexible ring.
D) Séguin: rigid ring.
E) Duran: flexible ring.
1. Bioprostheses
Several types of THV have been implanted as a result of degenerated mitral bioprostheses, mainly Carpentier-Edwards PERIMOUNT and porcine (Baxter/Edwards Lifesciences), Mosaic®, Hancock and Intact (Medtronic, Minneapolis, MN, USA), Biocor™ and Epic™ (St. Jude Medical). Their diameters, as announced by the manufacturers, ranged from 23 to 33 mm. In most cases, the THV used were the Edwards SAPIEN/XT/3 prostheses. As there is a discrepancy between the inner stent diameters of the prostheses announced by the manufacturers and those measured by TOE and computed tomography, careful evaluation and measurement using multimodality imaging should be systematically carried out in order to choose the appropriate size of THV to be implanted.
2. Rings
Implanted rings were mainly Physio I/II and Classic (Edwards Lifesciences), Duran (Medtronic), Séguin (St. Jude Medical), Carbomedics (Sorin [now LivaNova], Milan, Italy), with manufacturers’ diameters ranging from 26 to 36 mm. The sizing issue is particularly difficult here because these different ring brands are not circular and usually have an oval shape. In the absence of definite recommendations, the choice relies on an integrative approach, taking into account the three available measurement methods (TOE, computed tomography [CT], and fluoroscopy). In addition, for stenosed rings, THV sizing should take into account not only the inner ring diameter, but also the adjacent valvular tissue, which is not detected by CT or fluoroscopy (Figure 6). The measurement of an inflated balloon during predilatation may help to assess the amount of valvular tissue and avoid implanting too large a valve. The last issues are related to the various degrees of rigidity and the possible presence of open segments, which may preclude satisfactory results after valve-in-ring implantation. The Carpentier Classic rings are the most rigid and usually preclude complete deployment of the transcatheter valve. An underdeployment of the valve may lead to leaflet distortion, central regurgitation, high residual gradients and premature degeneration. The presence of gaps in the large diameter of the ring, as well as the presence of an open segment, may also lead to paravalvular leaks, with their haemodynamic consequences and the possibility of haemolysis (Figure 7). The semi-flexible Carpentier Physio rings and the flexible complete Duran rings are probably the most suitable for valve-in-ring implantation. This underlines the crucial importance of a careful medico-surgical evaluation before considering any valve-in-ring implantation.
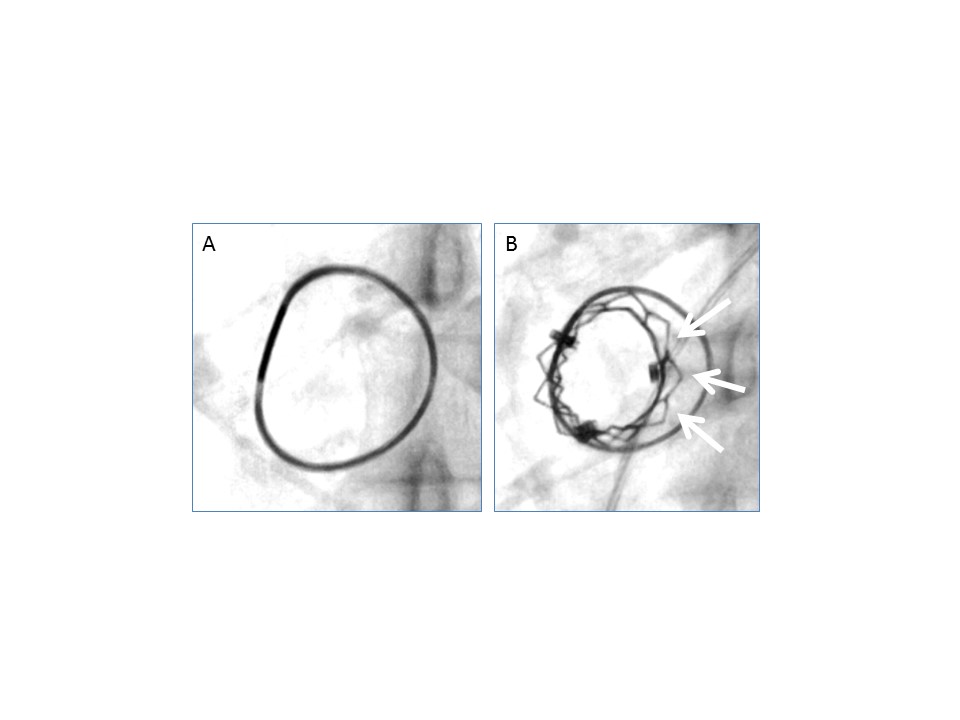
Fluoroscopy, severely stenotic mitral Physio ring.
A) Pre implantation.
B) Post implantation. The arrows show a large gap between the ring and the transcatheter valve, due to the presence of a large amount of valvular tissue in the context of severe mitral stenosis.
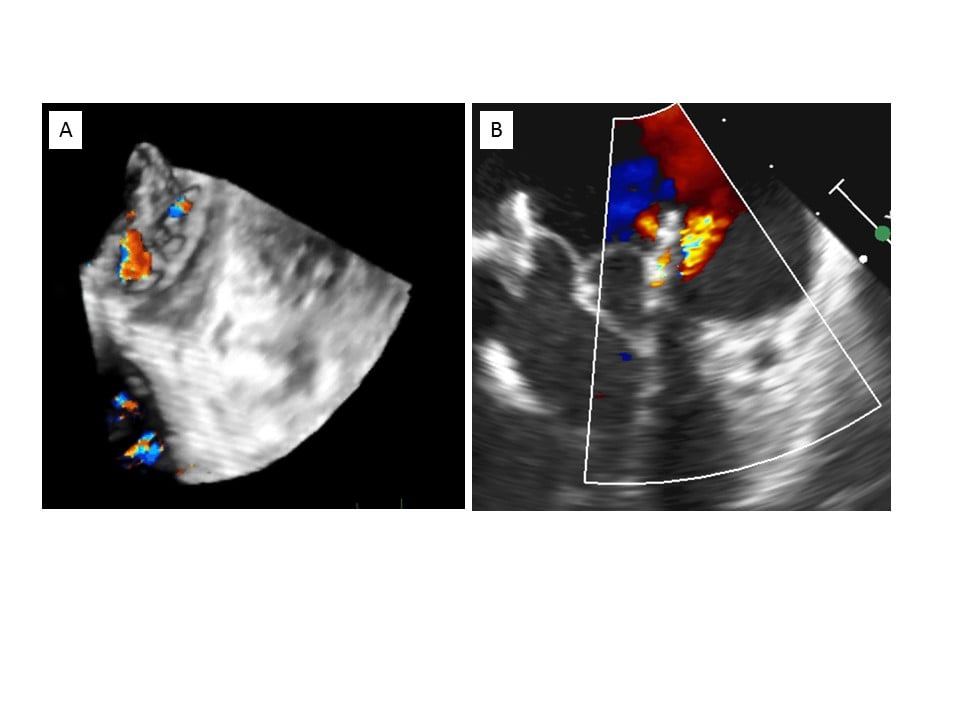
Transoesophageal echocardiography, paravalvular leak after valve-in-ring implantation.
A) 3D imaging showing mitral regurgitation with two jets localised within a gap between the surgical ring and the transcatheter valve.
B) 2D imaging.
The Valve in Valve Mitral app, developed by V. Bapat, is useful to guide the choice of the optimal THV size for the most frequently used mitral bioprostheses/rings.
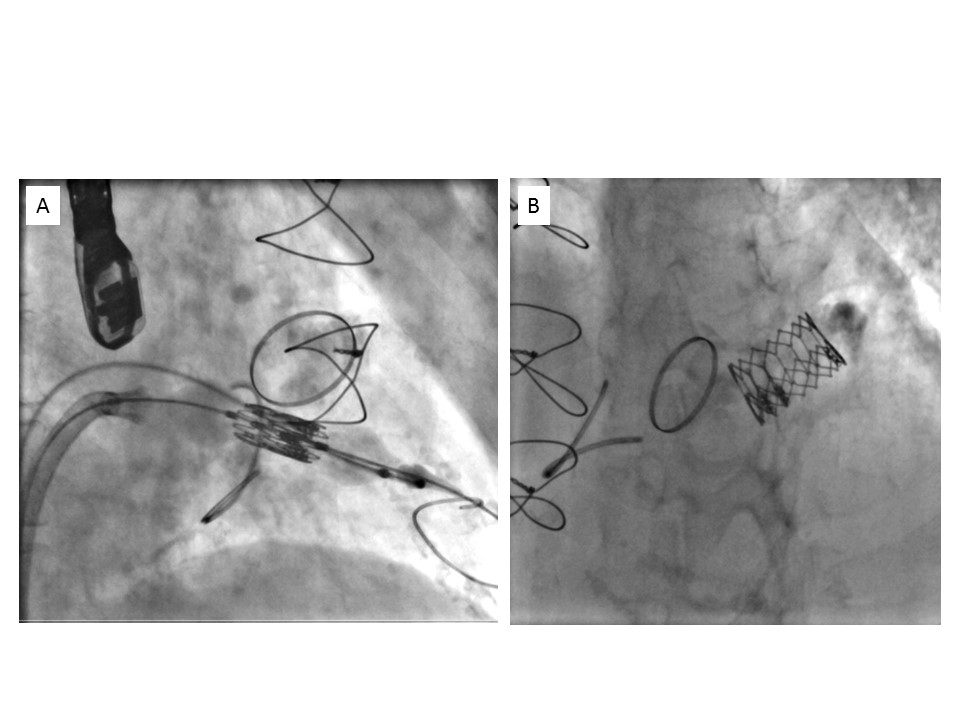
In most stented bioprostheses, positioning is easy, as the radiopaque ring and frame constitute ideal landmarks. It is essential to obtain a perfectly coaxial alignment with the bioprosthesis, which is facilitated by the transapical route, with an overlap below its basal ring towards the left atrium, to ensure a secure anchorage (Figure 8). The landmarks may differ in other bioprostheses, such as the Medtronic Mosaic, which includes only three radiopaque dots at the upper part of the frame. Here, the positioning should aim at placing the ventricular end of the THV just below these dots (Figure 9A). Finally, other stented bioprostheses are totally radiolucent, and the positioning is more difficult and exclusively echo-guided (Figure 9B).
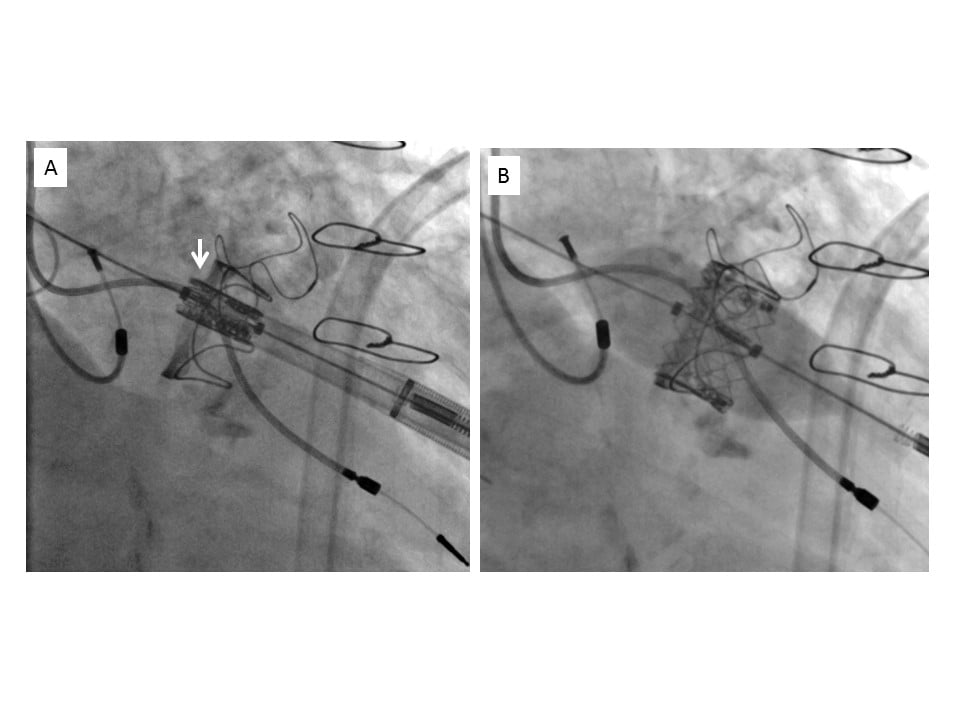
Transapical implantation of a SAPIEN XT valve in a PERIMOUNT mitral valve.
A) Positioning of the valve, with an overlap of 2 mm towards the left atrium (arrow).
B) Deployment of the valve in the appropriate position.
In annuloplasty rings, positioning is usually easy and aims at placing the THV 1/4 to 1/3 in the left atrium and 3/4 to 2/3 in the left ventricle. In addition, a final flared appearance of the THV should be achieved, if necessary by adding 1 to 3 additional cc in the inflation syringe, to secure its anchorage and avoid secondary atrial migration.
With both bioprostheses and rings, balloon inflation for delivery of the THV should be performed in a slow, two-step manner, to allow correction and perfect adjustment of its position.
Empirically, the antithrombotic regimen includes a combination of aspirin and anticoagulant therapy in all the patients for at least three months. This strategy is reinforced by reports of early or delayed valve thromboses after TAVI or TMVI (personal data). Thereafter, anticoagulant therapy may be stopped in the absence of other indications for long-term anticoagulation, such as atrial fibrillation.
1. Short-term
Since 2011, several short case series have shown the feasibility of valve-in-valve or valve-in-ring TMVI, mainly using the transapical approach, and reported favourable short-term outcomes.
Over the last years, data about TMVI in the setting of VIV and VIR have been published. The largest experience is reported by the Valve-In-Valve International Data (VIVID) registry, including a total of 857 VIV and 222 VIR cases with a median follow-up of 492 days . All patients enrolled belonged to the high or prohibitive risk category for redo surgery (median STS score= 8.6%). Most patients showed a mixed mechanism of failure (regurgitation and stenosis), followed by isolated stenosis (28%) and isolated regurgitation (15%). The most used prostheses for replacement were the SAPIEN 3 (42%). Overall technical success was 91%. However, residual mean gradient > 5 mmHg occurred in 61% of patients. Mispositioning occurred in 3.3% of the cases and in some of them a second valve implantation was required. Left ventricular outflow tract (LVOT) obstruction was reported in 2.6% of cases, being more common in the ViR group (5.9%) vs 1.8% in ViV. The 30-day mortality was 6.5% and 8.6 for the VIV and VIR groups, respectively.
Recently, two other registries confirmed the results observed in the VIVID registry , .
Recent data regarding transapical and transseptal approaches comparison were published by Nazir et al showing no significant differences with regards to 30-day mortality although device success rate was higher in the transapical group (89% vs. 68%, p=0.001).
2. Midterm/long-term
The aforementioned registries , provided also long-term data. The mortality differences between the two groups were even more evident at 1-year follow-up: 13.8 vs 23.2 for the VIV and VIR groups in the VIVID registry, respectively and 14.0% vs 30.6% according to data by Yoon et al. Of note, at multivariable analysis mitral VIR was independently associated with mortality with a 4-year adjusted survival of 53%.
Cheung et al reported the follow-up in 23 patients who underwent transapical valve-in-valve TMVI. At a median follow-up of 25 months, survival was 90%. One patient underwent successful mitral transapical reintervention at two months due to atrial migration of the THV. All patients alive were in NYHA Class I/II with good prosthetic valve performance.
More recently, Eleid et al examined 1-year outcome in 87 high-risk patients undergoing percutaneous transseptal implantation of balloon-expandable THV due to degenerated mitral bioprostheses (valve in valve, VIV, n= 60), previous ring annuloplasty (valve in ring, n=15), and severe mitral annular calcification, MAC, (valve in MAC, n= 12) . Procedural success was achieved in 97% of patients with VIV and 73% with valve in ring. Survival free of death or cardiovascular surgery was significantly better with mitral VIV compared with valve in ring or valve in mitral annular calcification (86% vs. 68%, p=0.008). Alongside this, THV implantation for failed annuloplasty rings and severe MAC associated with significant rates of obstruction, need for a second THV, and/or subsequent cardiovascular surgery. As regards thrombosis, it occurred in 2% of patients in spite of optimal anticoagulation suggesting the importance for systemic anticoagulation therapy in all patients undergoing percutaneous mitral valve implantation. Among the survivors symptoms relief was durable as most of them were in NYHA functional class I or II and echocardiographic results were excellent as far as the regurgitation and the mean transvalvular gradient are concerned. Sample size was not so big and some patients were lost at follow-up but data, especially for those undergoing VIV, were encouraging.
More data coming from the ongoing MITRAL (Mitral Implantation of Transcatheter Valves) trial (NCT02370511) were presented in the last EuroPCR by Guerrero M (Paris, 2019). The implanted THV were the Edwards Sapient XT/3 and the trial included 91 extremely high risk patients (STS PROM >15%): 30 undergoing VIV, 30 undergoing valve in ring and 31 undergoing valve in MAC. All VIV and valve in ring were performed through transseptal route, while valve in MAC followed also transatrial (48%) and transapical (3%) approach. After 1 year follow-up only one all-cause death occurred in the VIV group, whereas eight and ten occurred in the valve in ring and valve in MAC groups, respectively, confirming that mortality in those two groups is higher than in the mitral VIV group.
Good echocardiographic results and valve performances were maintained after one year follow up (all patients showed MR <2+ and mean gradient was <7 mmHg). Moreover, survivors experienced symptoms improvement after valve replacement and more than 80% of them were NYHA class I or II at 1 year follow up, independently from the group. Similarly to the Eleid data, thrombosis was a rare complication as it occurred in only one patient in the valve in MAC group: the patient was not receiving anticoagulation and was successfully treated with Warfarin without any consequences.
Interestingly, the only three cases of LVOT obstruction with hemodynamic compromise were in the valve in MAC group and in ten patients deemed at high risk for LVOT obstruction, alcohol septal ablation was performed prior to valve replacement. The strategy was successful suggesting a possible way to manage this risk.
Current results suggest that mitral VIV and VIR TMVI may represent attractive options in patients who are not deemed adequate candidates for redo surgery by a Heart Team but who warrant further intervention. They demonstrate a substantial improvement in early haemodynamic and functional status in these selected high-risk patients. In particular, VIV might represent the first-line therapy for failing bioprosthesis. On the contrary, the oval shape and the rigidity of most annuloplasty rings, combined with the higher risk of LVOT obstruction, explain why outcomes are less favourable after VIR , . Larger series with longer follow-up are needed to assess the potential role of this technique in the future. Although THV thrombosis is not frequent, future data should focus onto thrombosis risk and proper anticoagulation regiment as well as onto structural deterioration, as those represent the main determinants of durability.
Mitral annular calcification (MAC) is a chronic, degenerative process in the fibrous base of the mitral valve (Figure 10). Its development is related to several mechanisms, including mechanical factors such as excessive annular tension, atherosclerosis, abnormal calcium-phosphorus metabolism. The increase in life expectancy observed in developed countries explains why MAC has become more prevalent. Despite its frequency, its clinical relevance is underappreciated. MAC has been identified as an independent predictor of cardiovascular events, mitral valve disease, arrhythmias and mortality . Generally, it has little or no effect on valve function because it is not associated with leaflet commissural fusion. However, severe MAC may cause mitral regurgitation (MR) or mitral stenosis (MS) (Figure 11, Figure 12). The mechanisms leading to MR may combine failure of the calcified annulus to contract at the end of diastole, calcium infiltration of the base of the leaflets reducing their mobility, increasing traction on the chordae and elevating the leaflets. MS may be related to reduced annular dilatation during diastole and restriction of the anterior mitral leaflet motion.
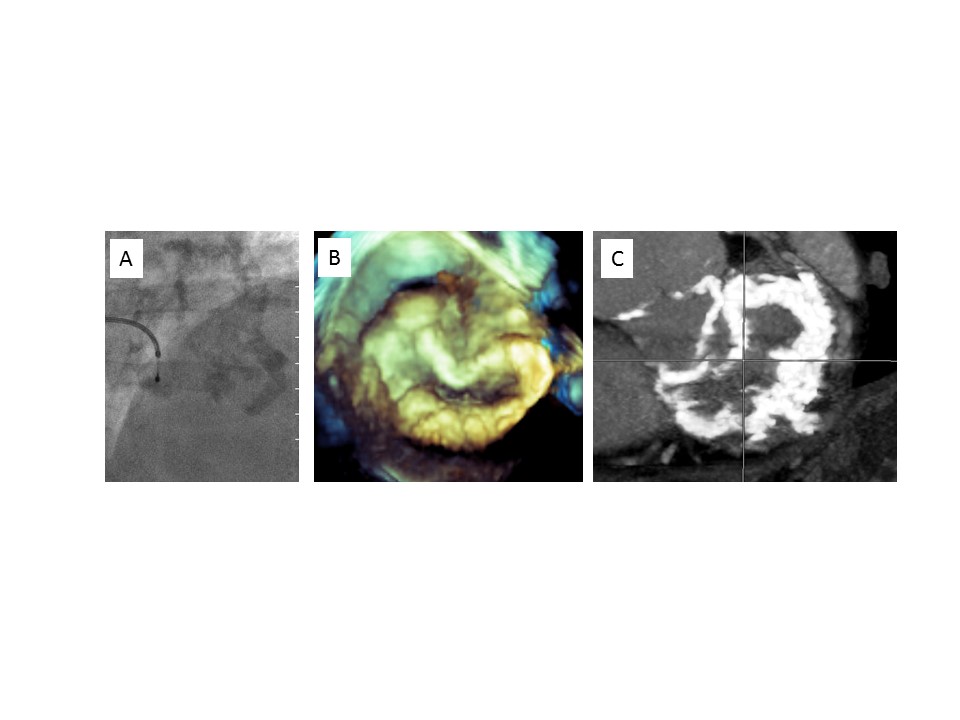
Mitral annulus calcification.
A) Fluoroscopy.
B) 3D echocardiography.
C) CT scan.
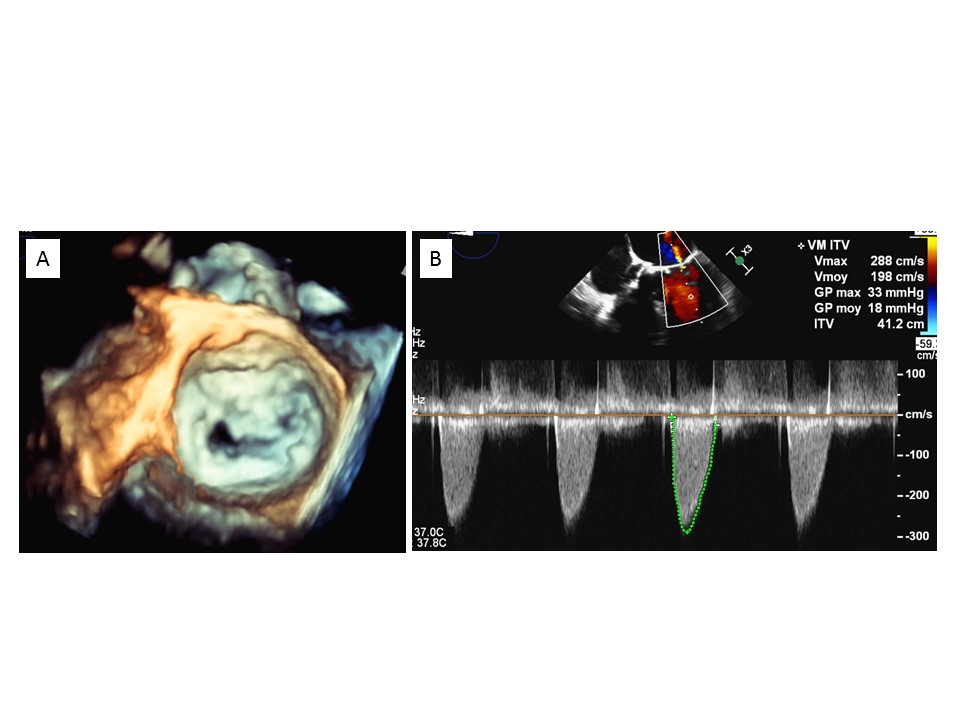
Mitral stenosis related to severe annulus calcification.
A) 3D echocardiography.
B) Transmitral gradient.
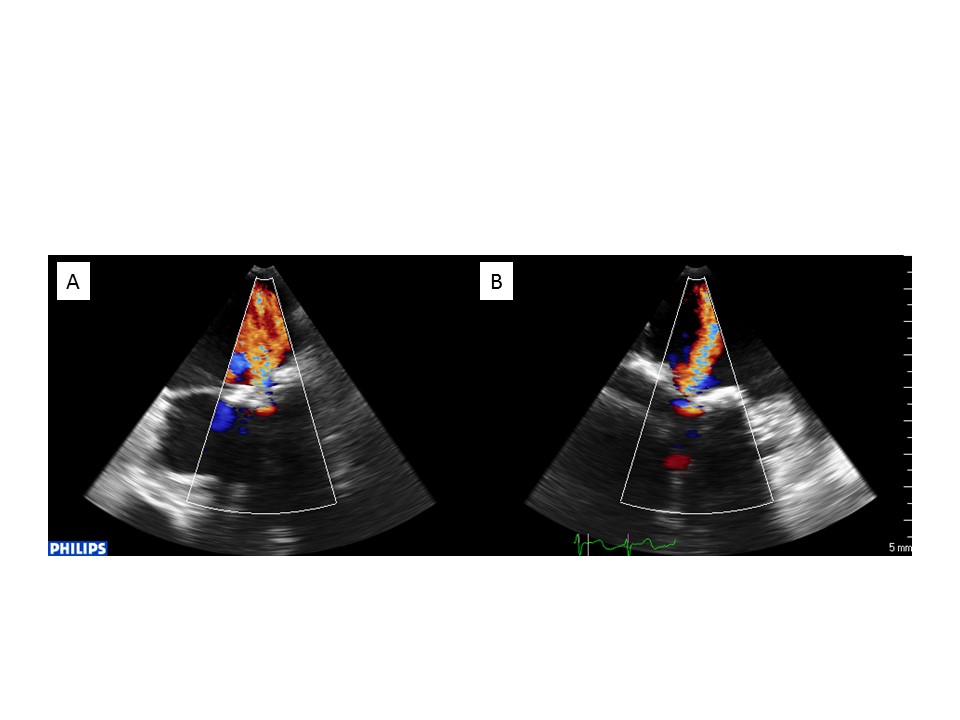
Mitral regurgitation related to severe annulus calcification.
Biplane 2D transoesophageal echocardiography showing severe mitral regurgitation related to severe annulus calcification; intercommissural (A) and LVOT (B) views.
Patients with extensive MAC may have an inoperable condition because of their intrinsic risk and insurmountable technical issues. The calcium burden poses technical challenges precluding successful surgery in many patients and increases the risk of rupture of the posterior wall of the left ventricle.
Recently, an early experience of TMVI for severe mitral valve disease due to MAC using TAVI prostheses has emerged, but available data are still very limited. They are based on several case reports and case series and on one international multicentre registry .
1. Surgical transatrial approach
The valve is delivered under direct visualisation in a non-beating heart. This approach allows operators to control the valve position in addition to placing two to three sutures between the valve stent frame and the mitral annulus to secure the valve in place to prevent embolisation. Also, the anterior mitral leaflet can be resected to decrease the risk of LVOT obstruction.2. Transapical approach
This technique provides an easy and direct access to the mitral valve and allows an optimal stabilisation of the prosthesis during its deployment. However, retrograde crossing of the mitral valve may be difficult, and this approach is exposed to the risk of access-site bleeding and pleural effusion.3. Transvenous, transseptal approach (Figure 13)
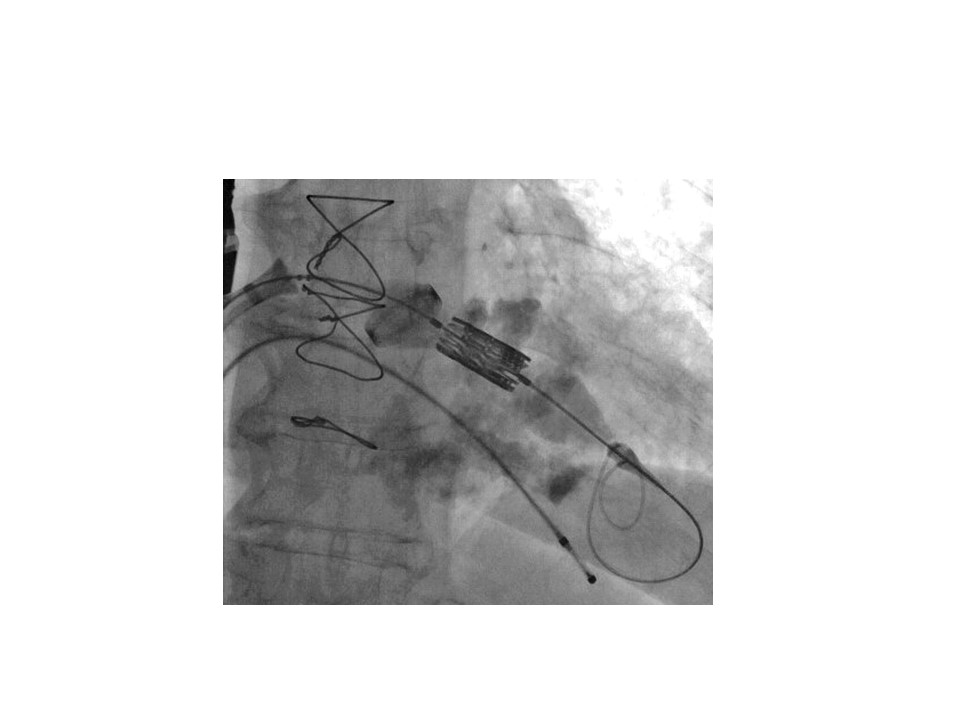
Pure transvenous, transseptal approach for transcatheter mitral valve implantation of a SAPIEN XT valve in mitral annular calcification.
A) Beginning of deployment.
B) After deployment.
4. Modified transseptal approach
This technique uses a transseptal access combined with an externalisation of the guidewire through a sheath percutaneously placed into the left ventricular apex. This may provide improved coaxiality and support during prosthesis deployment.
1. Type
Other transcatheter valves have been used in isolated cases: the Inovare valve (Braile Biomedica), the Melody valve (Medtronic), the Lotus valve (Boston Scientific), and the Direct Flow valve (Direct Flow Medical). The last two valves have the advantage of being repositionable and retrievable, which may decrease the risk of malposition, migration, paravalvular leak and LVOT obstruction. However, they are only available using the transapical access.
2. Sizing
In the absence of a validated reference method, the sizing of the calcified mitral annulus remains difficult and empirical. As extrapolated from TAVI, the most important information is provided by CT, although 3D TOE may also be useful to search for an integrative evaluation (Figure 14). The saddle shape of the mitral annulus and the irregularities of annular calcification increase the difficulty of a precise measurement. However, from experience, circularisation of the calcification may be expected after valve implantation. Thus, an acceptable approximation of the annulus size may be obtained by calculating its mean diameter or its perimeter. From a practical point of view, the 23 mm SAPIEN valve should not be used due to unacceptably high post-implantation gradients; the choice should be made between the 26 and 29 mm valves. In the presence of borderline diameters, the larger valve size should be preferred to limit the risk of post-implantation atrial migration. Balloon sizing may also be used to guide the decision.
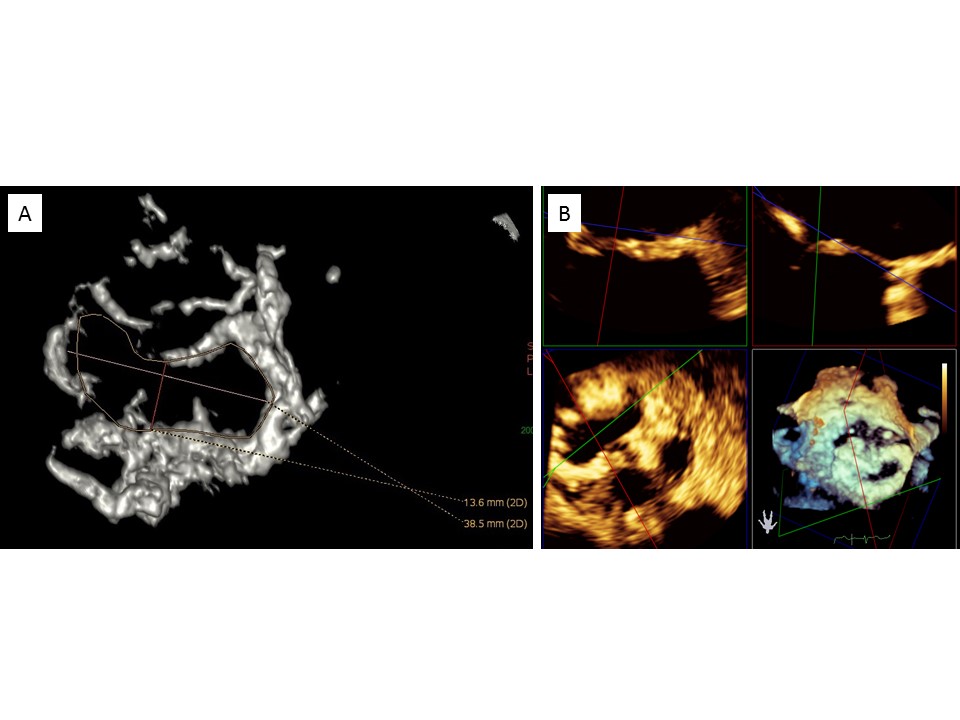
Sizing of mitral annulus calcification.
A) CT scan.
B) 3D transoesophageal echocardiography.
3. Positioning and deployment
The deployment of TAVI valves in MAC obeys the same general principles as in surgical mitral prostheses or rings. Whatever the approach chosen, it should be slow, thanks to very progressive and controlled balloon inflation, in order to be able to refine the position until at least two thirds of deployment. However, the landing zone is more difficult to define than for valve-in-valve or valve-in-ring implantation, because the edges of the mitral annulus are less clearly delineated. Annular calcification may reach the leaflets and the subvalvular apparatus or dive into the left ventricle, or extend towards the left atrium (Figure 15). In such cases, despite an adequate perpendicular projection, fluoroscopy may be misleading and echo guidance is mandatory (Figure 16). Usually, the 3D transoesophageal atrial view is the most informative, clearly showing the position of the atrial aspect of the prosthesis within the mitral annulus. Most importantly, the landmarks should take into account the type of SAPIEN prosthesis implanted. When using SAPIEN 3 prostheses, shortening of the atrial part should be anticipated, and the initial placement should be more atrial than when using a SAPIEN or SAPIEN XT prosthesis. Finally, it is recommended to overexpand the prosthesis by adding 1 to 3 cc to the nominal volume in the inflation syringe in order to flare the prosthesis and minimise the risk of displacement or migration (Figure 17).
Protrusive mitral annulus calcification extending towards the left atrium and ventricle, with no reliable fluoroscopic landmark of the landing zone.
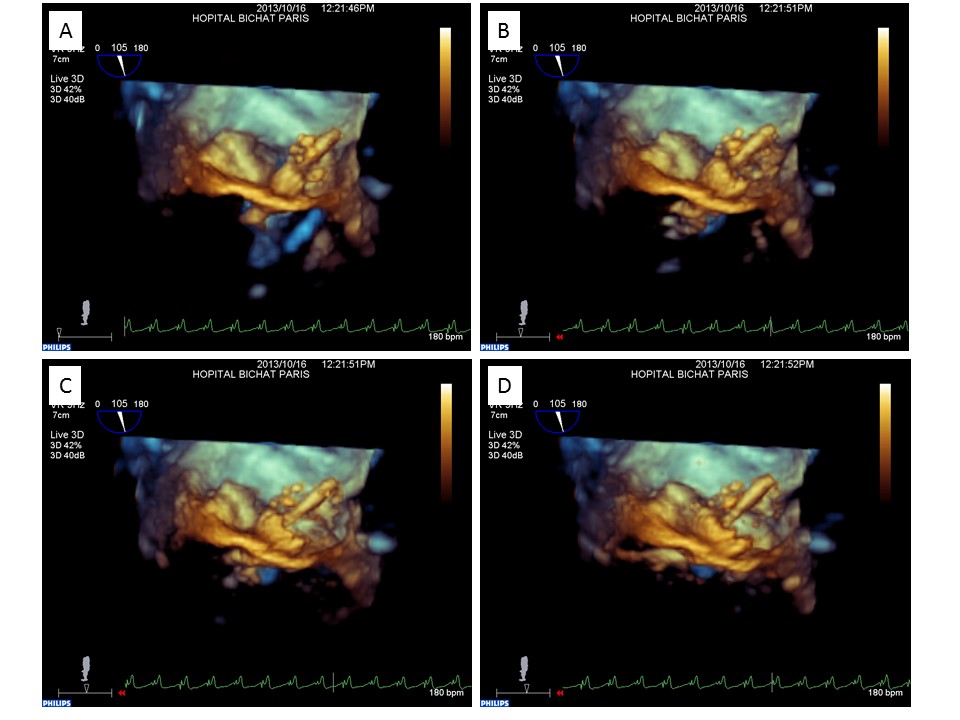
3D transoesophageal echocardiographic guidance of a SAPIEN XT valve implantation in a mitral annulus calcification.
A) – D) Different steps of deployment.
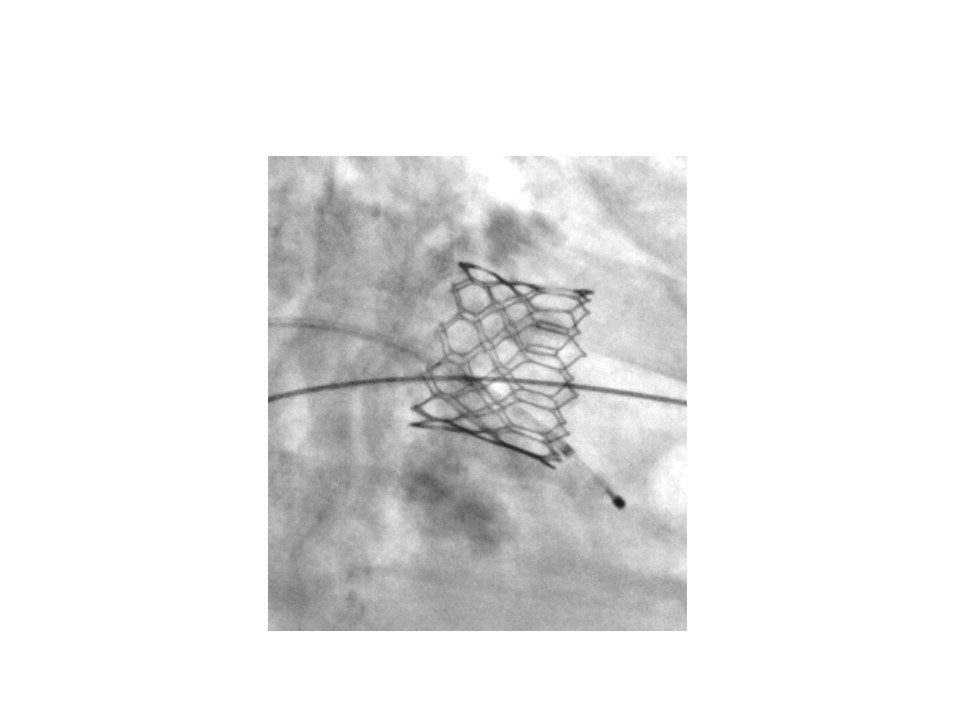
Fluoroscopy after implantation of a SAPIEN XT prosthesis in mitral annular calcification.
Flared appearance of the prosthesis to decrease the risk of secondary migration.
4. Post-procedural care
This pre-discharge evaluation should include a transthoracic and transoesophageal examination and a CT scan, which will be mandatory as initial reference for future evaluation at follow-up (Figure 18, Figure 19).
Post-implantation echocardiographic evaluation.
A) Biplane 2D transoesophageal echocardiography.
B) Colour biplane 2D transoesophageal echocardiography, with no visible mitral regurgitation.
C) 3D transoesophageal echocardiography, atrial view.
D) Transprosthetic mitral gradient.
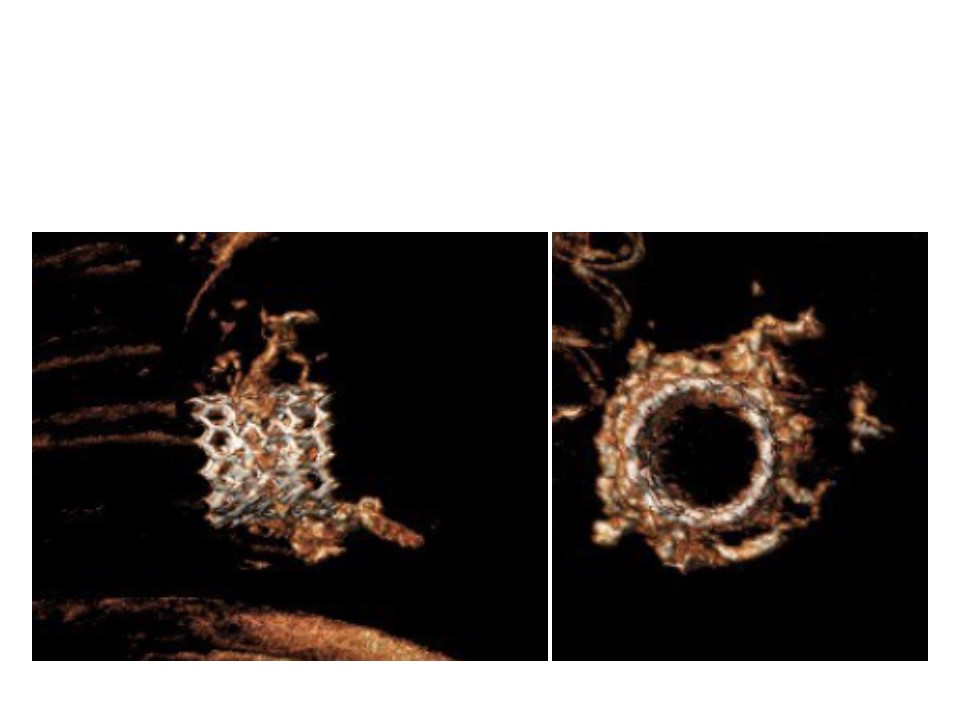
Post-implantation CT scan evaluation.
A) Profile.
B) En face view.
Empirically, the antithrombotic regimen includes a combination of aspirin and anticoagulant therapy in all the patients for at least three months. Thereafter, the latter may be stopped in the absence of other indications for long-term anticoagulation, such as atrial fibrillation.
Since 2013, several case reports of TMVI in MAC using TAVI valves have been described . They are presented in Table 1.
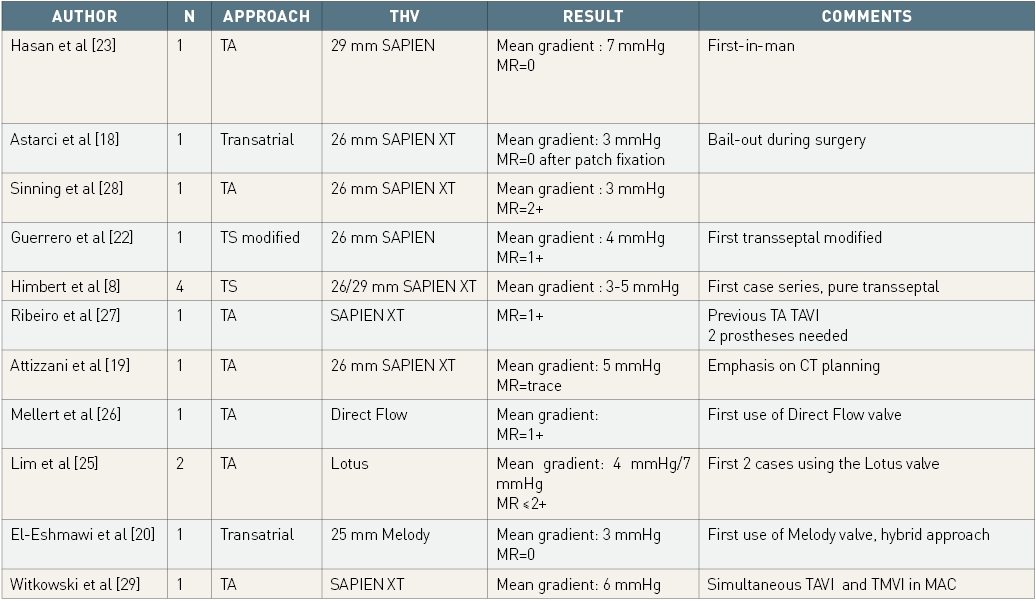
Published case reports of TAVI valve implantation in MAC.
MAC: mitral annulus calcification; TA: transapical; TAVI: transcatheter aortic valve implantation; THV: transcatheter heart valve; TMVI: transcatheter mitral valve implantation; TS: transseptal
Currently, the largest evidence assessing 30-day outcomes comes from the STS/TVT registry . Valve-in-MAC is the group with the lowest device success (59%) and the highest in-hospital (18%) and 30-day mortality (21.8%) as compared to VIV and VIR. Such negative results are due to multiple reasons. The most relevant is the higher incidence risk of LVOT obstruction. In addition, the complexity of the mitral anatomy, the difficulties in quantifying large annular area due to heavy calcifications and the lack of dedicated anchoring mechanisms for aortic THV increasing the risk for embolization might explain the worse outcomes. Of interest, the reported incidence of LVOT obstruction (10%) was significantly different from that observed by Yoon et al. (40%): this might be due the different definitions used in the two studies and also by a more careful CT scan characterization.
The above mentioned MITRAL (Mitral Implantation of Transcatheter Valves) trial (NCT02370511) presented in the last EuroPCR by Guerrero M (Paris, 2019) compared 91 extremely high risk patients undergoing VIV, valve in ring and valve in MAC with Edwards Sapient XT/3. Almost three fourth of valve in MAC group had severe mitral stenosis and 15% of them showed both mitral stenosis and regurgitation. The procedure was performed through transseptal (48%), transatrial (48%) and transapical (3%) approaches. The only three cases of LVOT obstruction with hemodynamic compromise occurred in this group suggesting the importance of a careful LVOT obstruction risk assessment in the baseline echocardiographic examination. Ten patients underwent prior alcohol septal ablation three-four weeks prior to the valve implantation. Valve in MAC group showed the higher mortality rate both at 30-day and at 1 year follow up (17% and 33%, respectively) as compared to VIV and valve in ring group, with a survival probability at 1 year of 67%. No significant differences were reported between the different approaches with regards to 1-year mortality. Only 1 case of valve thrombosis was reported but the patient was not assuming any anticoagulant and Warfarin administration was successful to solve the problem.
In the study by Eleid patients undergoing valve in MAC were 12 and again Edwards Sapien XT/3 were implanted. Procedural success was achieved in 75% of them with a total 30-day survival of 83%. Those data confirmed that valve in MAC has higher operative mortality and morbidity, but 1-year outcome after successfully procedures are favourable.
Recently, Sorajja et al tested the feasibility and outcome (median 12 months) for anatomically designed mitral prosthesis Tendyne . The multicenter study included nine patients undergoing transapical mitral replacement demonstrating acute procedural success in all patients with only one death occurring 41 days after the procedure. All patients experienced symptoms improvement and mitral prostheses performance were optimal also after a median 12 months follow up.
The mixed results observed during this initial experience emphasise the importance of the challenges still to be overcome before considering further expansion of the technique. Efforts should be made to improve both patient selection and procedural technique.
Little is known regarding criteria defining the best candidates for TMVI in this very high-risk population. Besides evaluation of the utility/futility of any intervention, the screening process to assess its technical feasibility and prevent potential complications largely remains to be established. The first decisive step is echocardiography, including 2D and 3D transoesophageal examination, which gives precious information on the anatomy of the mitral annulus. As for TAVI, a cardiac CT scan plays a major role. It is irreplaceable for defining the optimal route (transseptal vs. transapical), guiding the transseptal puncture site, measuring the annulus diameter and determining the adequate valve size, evaluating the amount and distribution of calcification to assess the safety of anchorage and avoiding prosthesis migration as well as paravalvular leaks. Most importantly, it provides crucial information regarding the risk of LVOT obstruction, which is probably the main complication to be feared and the most frequent technical cause of patient exclusion (Figure 20). Several anatomical predictors of LVOT obstruction have been identified: acute aorto-mitral annular angle (Figure 21), small left ventricular cavity and septal hypertrophy (Figure 22), short distance between the anterior mitral leaflet and the septum, long/calcified anterior leaflet, thickened and rigid subvalvular apparatus (Figure 23). 3D reconstructions including simulations of valves deployed in situ are useful and help to make the final decision, which is often difficult. In the future, 3D printing of the left ventricle and mitral valve apparatus should represent a major contribution to facilitate the anatomical screening and provide accurate simulations of the planned procedures.
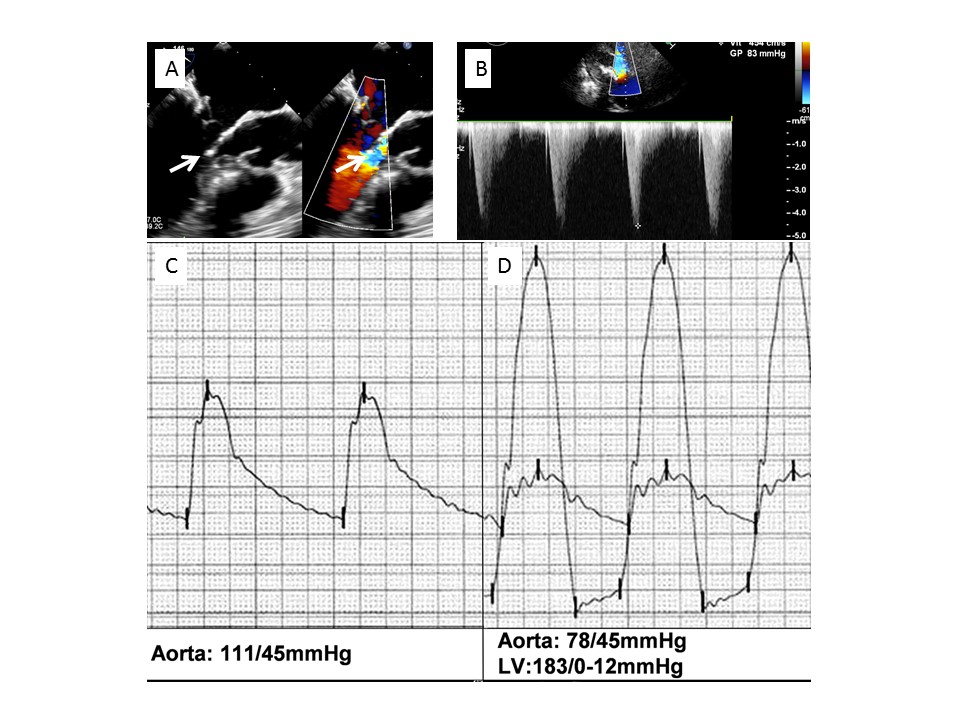
Left ventricular outflow tract obstruction after transcatheter implantation of a SAPIEN XT valve in a mitral annulus calcification.
A) 2D transoesophageal echocardiography, long-axis view; note the contact between the subvalvular mitral apparatus and the septal bulge (left arrow) and the aliasing in the left ventricular outflow tract (right arrow).
B) Gradient in the left ventricular outflow tract.
C) Aortic pressure before implantation.
D) Severe hypotension with 105 mmHg ventriculo-aortic peak to peak gradient post implantation.
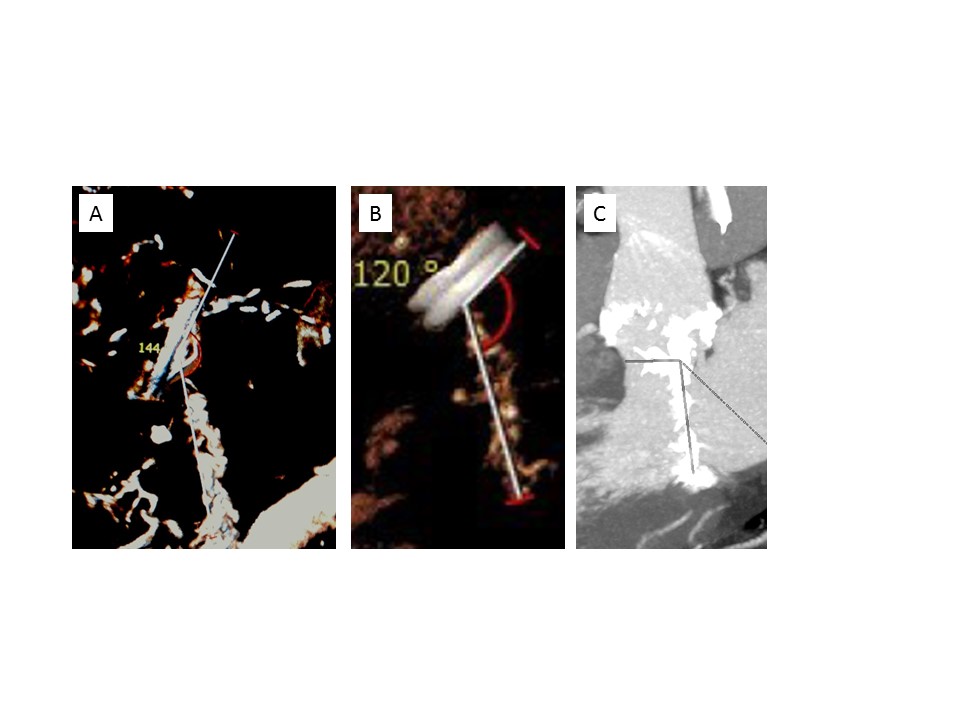
CT scan, determination of the aorto-mitral annular angle before transcatheter valve implantation in mitral annulus calcification.
A) Obtuse angle (>140°), minimal risk of left ventricular outflow tract obstruction.
B) Acceptable angle (120°).
C) Angle close to 90°, high risk of left ventricular outflow tract obstruction.
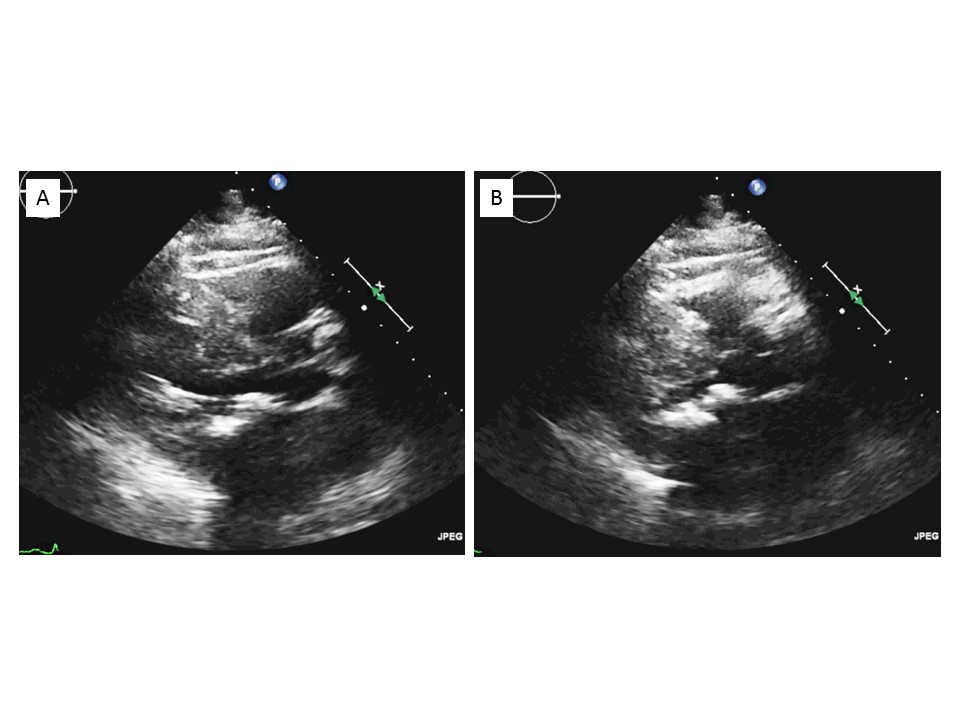
Transthoracic echocardiography, small left ventricular cavity and septal bulge contraindicating transcatheter valve implantation in mitral annulus calcification.
A) Diastole.
B) Systole.
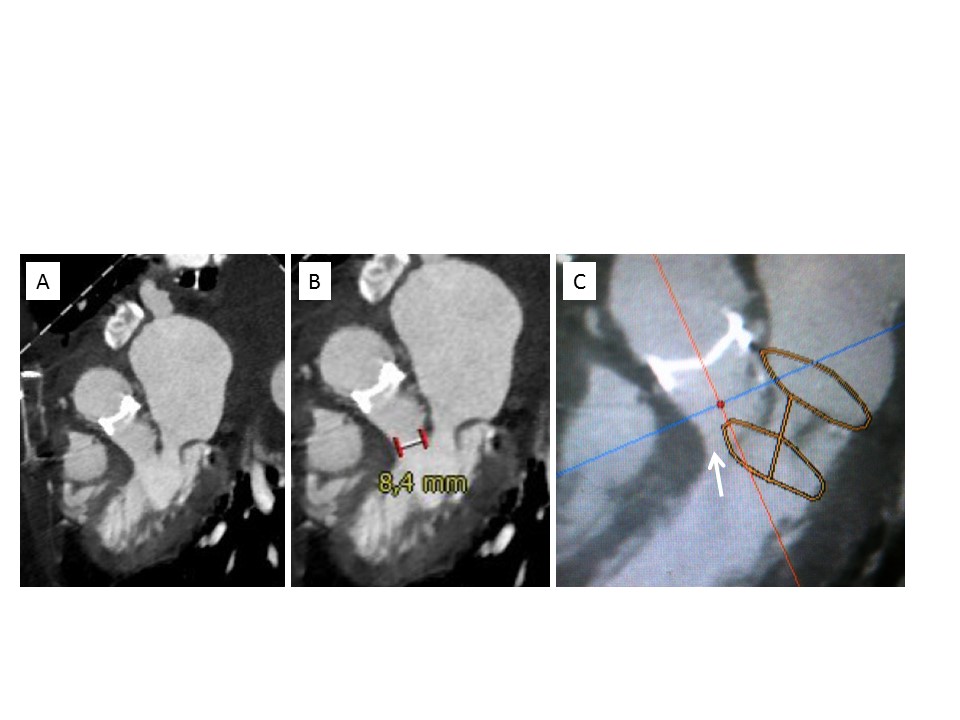
CT scan, screening before transcatheter valve implantation in mitral annulus calcification: prohibitive risk of left ventricular outflow tract obstruction.
A) Narrow outflow tract in diastole.
B) Measurement of the outflow tract, small distance between the anterior mitral leaflet and the septum (8.4 mm).
C) Simulation with a valve in place showing a severe obstruction of the outflow tract (arrow).
Recently, the intentional laceration of the anterior mitral leaflet (AML) has been proposed as a valid strategy to prevent the risk of LVOT obstruction. It has been first tested surgically in 8 patients undergoing transatrial TMVI together with AML resection . Despite the small sample size, no patients had LVOT obstruction and no in-hospital nor 30-day deaths were observed.
A fully percutaneous technique to achieve an intentional AML laceration has been described and recent data from a prospective, single-arm, multicenter study have been published (LAMPOON IDE, NCT03015194) , . It included 30 high/prohibitive surgical risk patients with high risk for LVOT obstruction (neo LVOT<200mm2, or long redundant AML). LAMPOON was successful in 100% of patients and 97% of them showed mean LVOT gradient <30 mmHg. Procedure success was achieved in almost three fourth of cases (73%), and in-hospital and 30-days survival was 93% (100% for ViR, 87% for ViM). Therefore, LAMPOON might represent an effective technique to overcome LVOT obstruction although ViMAC still remains a very high-risk category and larger data with longer follow-up are needed.
Another strategy might be the preventive alcohol ablation which has been investigated in the MITRAL trial , .
.jpg)
A: Tiara (Neovasc Inc., Richmond, BC, Canada). B: Tendyne (Abbott). C: Evoque (Edwards Lifesciences). D: Intrepid (Medtronic). E: Cardiovalve (Valtech Cardio Ltd, Or Yehuda, Israel). F: HighLife (HighLife SAS, Paris, France)
Updated data from the TIARA I and TIARA II studies have been presented at EuroPCR 2020 E-Course by Conradi L. Currently a total of 79 patients have been enrolled: 25 for the TIARA I, 32 for the TIARA II and 22 for compassionate use. Most of the patients showed a secondary functional MR with a mean LVEF of 37±9%. No procedural deaths have been reported, while 7 deaths occurred after 30 day follow-up, six of them being cardiovascular. No LVOT obstruction was observed although three cases of device malposition and 2 cases of device migration were reported. Prostheses performances were excellent after 1-year follow-up with all patients showing mild or less residual MR . Finally, significant symptoms improvement was also reported with more than 90% of patients being in NYHA I or II functional class. Although initial data seem to be encouraging, longer follow-up time and larger numbers are needed.
1. Transapical
2. Transfemoral
The transfemoral delivery system measures 33 Fr at its distal tip. It is passed over a customised PTFE-covered nitinol wire passed through the femoral vein into the right atrium, then via a transseptal puncture into the left atrium, through the left ventricle and aorta where it is captured and externalised with a snare passed up from the femoral artery, thus creating an arteriovenous wire path. Release of the valve and capture of the native leaflets follow a similar pattern to that using the transapical route .
Four implantations of the second generation of the device have subsequently been reported, three via the transapical route and one via the transfemoral route . In all cases the valve was successfully deployed. One of the transapical patients died of pneumonia on postoperative day nine. The remaining patients were discharged home with resolution of their MR and no paravalvular leaks, with follow-up ranging from 30 to 90 days.
Updated results were presented by Webb J at EuroPCR 2020 E-Course. A total of 15 patients undergoing transfemoral/transseptal approach have been enrolled so far, including compassionate use (n=8) and early feasibility study (n=7) cases. The most common etiology was mixed MR followed by functional and degenerative (27%). Technical success was achieved in all cases but one where conversion to surgery was needed. At 30-day follow-up one death occurred (7%) while PVL closure and LVOT obstruction requiring intervention were required in two and one patient, respectively. Early feasibility trials are currently underway (ClinicalTrials.gov Identifiers: NCT02718001, 2013-05C).
Together, the valve inner and outer form a self-expanding prosthesis which is connected to a braided fibre tether made of ultra-high molecular weight polyethylene. The tether is designed to stabilise the valve by passing through the left ventricular apex where it is secured to an external pad. This pad is a polyether ether ketone button covered in PET fabric, designed to promote ingrowth. During implantation, the tether is used to adjust tension and optimise the position of the valve within the mitral annulus. There is an “apical pad tool” that is designed to fasten the apical pad to the braided tether. It has an articulating head to facilitate proper angulation, and a cam rotator that drives a pin through the braided tether. The cam rotator allows unlocking and relocking of the pin in case the tension on the tether needs to be adjusted.
Thus, the Tendyne valve is designed to rest on the floor of the left atrium, providing countertraction to the tether force produced by the tether to resist migration of the valve into the left ventricle and prevent paravalvular leak.
The Tendyne valve size is chosen based on MDCT imaging of the patient’s mitral annular dimensions confirmed by intraoperative 3D TOE. The device is implanted under general anaesthesia via a transapical approach through a small left minithoracotomy. All the manoeuvres are performed (almost exclusively) using 2D and 3D TOE imaging guidance. The optimal apical puncture site is determined. A soft 0.035” wire is inserted into the left atrium and a balloon-tipped catheter advanced to ensure that the wire is not entrapped in the mitral subvalvar apparatus. A 34 Fr sheath is advanced over the soft wire into the left atrium. The implant device is advanced into the sheath and then extruded until the outer nitinol frame expands to about 85% of its final deployed size. The correct anatomical position of the D-shaped outer stent and the raised section of the atrial cuff are then determined by rotating the device. The device is then withdrawn towards the ventricle, into an intra-annular position, and then fully deployed. The apical pad is inserted into position over the tether. The tension on the tether is then adjusted to optimise the position of the device. Finally, the pin is driven through the braided tether to fix it in position.
Data including patients from the Global Feasibility Study and from CE mark approval study have recently been published . It included a total of 100 patients (mean STS score 7.8±5.7), mostly affected by secondary MR (89%). Implant success was achieved in 97% of cases while 3 implants were abandoned or retrieved. One-year all-cause mortality was 26% with survival rate of 72%. A total of nine device-related adverse events were reported (three haemolysis and six thrombosis). A clinical improvement was also observed as measured by NYHA functional class and Kansas questionnaire. Durable echocardiographic results were reported after Tendyne implantation: more than 90% of patients showed grade I/none residual MR without any significant transvalvular gradient confirming an acceptable safety profile and with effective clinical ad technical results.
Through a transapical approach, the system is advanced across the mitral valve. A flexible brim (which aids imaging during delivery) is deployed in the left atrium and the device is then withdrawn into the desired position within the annulus. The fixation ring is then expanded and finally the device is released.
A hydraulic mechanism provides controlled, precise deployment. There is no need for rotational alignment or to search for leaflet attachment. This system accommodates tilt and lateral misalignment.
Early experience data have been published by Bapat et al for the Intrepid Global Pilot Study. A total of fifty patients were enrolled, 72% of them affected by secondary MR, mean STS score of 6.4±5.5.Device success rate was 98% with no device malfunction/thrombosis reported. After 30-day follow-up mortality rate was 14% and rehospitalization for heart failure of 8%. MR after 173 day median follow-up was no more than mild and symptoms and quality of life as measured by NYHA functional class and Kansas questionnaire were both improved.
The Cardiovalve system (Valtech Cardio Ltd, Or Yehuda, Israel) features a self-expanding pericardial bovine valve mounted on a nitinol frame, specifically designed to be delivered through a transfemoral transseptal approach (28 Fr). It has multi-steerable catheter for coaxial implantation and implantation is mainly performed under echo and fluoro guidance. Currently, three sizes are available to cover all the mitral anatomies. The low device profile limits the risk of LVOT obstruction while allowing tridimensional manoeuvring within the left atrial and ventricular chamber, to achieve optimal alignment to leaflet grasping.
Currently, a prospective, multicenter and single arm pilot study is underway (AHEAD Trial). Data about the first five patients were presented by Maisano at EuroPCR 2019, Paris. All patients enrolled had functional MR with LVEF ≤40% and with a mean STS PROM of 6±7. All 5 patients showed none/mild post-procedural residual MR. However, more data are needed and the study plans to enroll a total of 30 patients. Alongside this the early feasibility study (AHEAD US) has also started to enroll patients in the US.
The HighLife transcatheter mitral valve replacement device (HighLife SAS, Paris, France) is a two-component system. A subannular implant (SAI) creates a closed loop with a fixed perimeter around the patient’s native valve leaflets and chordae. The valve prosthesis is then implanted over a delivery system and is anchored by interacting with the SAI. The valve prosthesis shape has a preformed groove in the annular region so as to create an interference with the SAI which blocks it from slipping into the atrium. The combination of these two opposite interactions results in a stable position. The HighLife valve itself is made from glutaraldehyde cross-linked bovine pericardium. The first human implants took place early in 2016.
The MValve (Boston Scientific) is a docking system that is implanted into the mitral valve/annulus which facilitates subsequent implantation of another transcatheter device. There has been some first-in-human experience with this device with subsequent implantation of the Lotus (TAVI) device (Boston Scientific), but substantial clinical data are still not available.
The Cephea system (Cephea Valve Technologies, Inc., San Jose, CA, USA) is based on a knitted nitinol mesh design, and is designed to afford multi-level conformability, retention and sealing. It is a low-profile device which is fully repositionable and recapturable. An interesting feature of this device is that it is specifically designed for transatrial and transseptal delivery. First in human experience has been recently described . It was implanted under general anaesthesia and TEE guidance. The valve was implanted through transseptal approach and echocardiographic assessment after valve implantation showed 2 mmHg transvalvular gradient and no intraprosthetic regurgitation. After 28 weeks follow-up echocardiographic parameters were unchanged and patient was in NYHA functional class I.
Altavalve (4C Medical Technologies) is a self-expanding, spherical shaped, nitinol and three bovine leaflets device. Currently, only first-in-human case has been described . It was implanted through the transapical approach although transseptal approach is going to be available soon. Procedure was technically successful and after 30 days follow-up no adverse events were reported.
Sapien M3 (Edwards Lifesciences) is a balloon-expandable valve with a cobalt-chromium frame and 3 bovine leaflets. It is implanted through the transfemoral route (20 Fr). Currently, first-in-human experience about ten patients with mixed aetiologies has been published by Webb et al. . Technical success was achieved in 90% of cases, residual MR was less than trivial in all patients with mean transvalvular gradient of 2 mmHg. No patients died and, at 30 days, there was no stroke, myocardial infarction, rehospitalization, LVOT obstruction, device migration, embolization, or conversion to mitral surgery.
Transcatheter mitral valve repair and replacement have specific advantages and disadvantages.
Arguably, in general, a repair approach is more respectful of the physiology of the mitral valve complex, which is composed of multiple anatomical components, including the leaflets, the annulus, the chordae, and the papillary muscles, and it is in continuity with the atrial wall and the aortic valve.
Mitral replacement is associated with a non-physiological inflow pattern, which results in increased LV stress and less efficient work, while the physiological vortex-like circulation is preserved after mitral repair. Other disadvantages of replacement over repair are the loss of mitro-aortic contiguity after replacement and the reduction of basal LV contraction due to the fixation of the prosthesis to the mitral annulus. In particular, the contribution of basal contraction to the cardiac output plays a major role in heart failure patients with severely depressed EF, suggesting that valve replacement may be detrimental in such patients. It should also be borne in mind that the life expectancy of a patient implanted with a prosthetic valve is reduced, mainly due to thromboembolic and haemorrhagic events and to the risk of prosthesis-related endocarditis.
The reduced impact of repair compared to replacement in terms of physiology and anatomical alterations confers a higher safety profile on repair, which in the future will probably be the basis for expanding transcatheter mitral repair indication towards an earlier indication.
On the other hand, the specific advantages of replacement are versatility and more predictable results in terms of MR reduction. Moreover, whilst in order to address the different anatomies with repair techniques a single operator should be confident with multiple devices and advanced imaging guidance modalities, and technologies according to the anatomy and to the specific lesions, TMVI will normally be technically less demanding, and potentially be applicable to many patients (one valve for all) regardless of anatomy. However, the anatomical eligibility of patients at the moment represents a major issue of TMVI, and a pre-procedural CT scan is mandatory in order to assess feasibility.
Given the specific advantages and disadvantages of repair and replacement, it is likely that these two approaches will, in the future, have a complementary rather than a competitive role, similar to surgery.
In general, it can be stated that, in patients with DMR, TMVI will probably have a limited role only in high-risk, elderly and inoperable patients, who are not amenable for minimally invasive surgical mitral valve repair or who have an anatomical contraindication for transcatheter mitral repair.
In patients with severe FMR, since the role of surgery is less well established, and most of the patients are treated medically, TMVI may potentially be a therapeutic option for a large number of patients, especially those with more advanced disease and severe anatomical and functional abnormalities, who are not eligible for valve repair.
In the future, careful patient selection will play a fundamental role in identifying specific patients most likely to benefit from TMVI vs. repair vs. mitral valve surgery. Large randomised trials will be needed in order to define the specific role of each therapeutic option.
The field of TMVI has grown slowly over the last years. However, TMVI is going to enrich the toolbox of percutaneous MV interventions thanks to the recent approval of the first dedicated TMVI prostheses (Tendyne) alongside with some technical improvements such as LAMPOON to prevent one of the most common and feared complications (LVOT obstruction), the ELASTA-Clip for MitraClip detachment prior to TMVI, the growing evidence supporting TMVI especially in the context of valve-in-valve. Currently, percutaneous repair has gained wider experience and is going to be preferred over TMVI due to durability, safety and pathophysiological reasons. In this perspective, TMVI is going to have a complementary role and considered for high-risk patients with unsuitable characteristics for repair, whereas ViV might become the treatment of choice, especially for those cases at higher surgical risk. Further data are needed in the setting of valve-in-ring and valve-in-MAC to establish the real benefit of replacement in such high-risk categories.
Most of the available data confirmed low procedural mortality and high technical success rate for most of the devices suggesting safety and feasibility of TMVI. Specifically, valve-in-valve showed very promising results and should be considered as a first-line therapy. On the contrary, TMVI for valve-in-ring and valve-in-MAC should be carefully evaluated as the long-term outcomes are poor.
Moreover, edge-to-edge therapies set the bar very high. The challenge for TMVI will be to demonstrate to be as safe and as effective as the MitraClip. For this reason, some studies (e.g. APOLLO trial) included also the edge-to-edge arm. Results from these studies will help to better understand potentialities and limitations of TMVI.
In addition, TMVI needs several technical and engineering improvements especially as regards the delivery. Currently most devices have a transapical approach whereas transseptal implantation might increase TMVI use and might improve also long-term outcomes.
Alongside this, in the future careful patient selection will play a fundamental role in identifying specific patients most likely to benefit from TMVI vs. repair vs. mitral valve surgery. For this reason, at the moment the role of heart team is crucial to detect best candidate for each procedure. In the future, Heart Valve Clinics will play an important role in order to offer the best available treatment option for the patients.
Large randomised trials will be needed in order to define the specific role of each therapeutic option and the best candidate.
Gregory Ducrocq, Thomas R.D. Shaw, Habib Gamra, Peter C. Block, Neil R. Grubb, Carlos E. Ruiz, Alec Vahanian
Updated on November 22, 2022
Horacio Medina de Chazal, Ali Zgheib, Angelo Quagliana, Michael Chetrit, Jean Buithieu, Giuseppe Martucci, Marco Spaziano, Ali Abualsaud, Ole de Baker, Laurence Campens, Pascal Theriault-Lauzier, Jere...
Updated on November 23, 2022
Olaf W. Franzen, Ole De Backer, Mirjam Wild, Lars Sondergaard
Updated on May 13, 2021
Mirjam Wild, Maurizio Taramasso, Alison Duncan, Giulio Russo, Dominique Himbert, Francesco Maisano, Nicolo Piazza, Fabien Praz
Updated on May 11, 2023