Department of Cardiology Bern University, Hospital Inselspital, Bern, Switzerland, Department of Cardiology Bern University, Hospital Inselspital, Bern, Switzerland, Department of Cardiology Bern University, Hospital Inselspital, Bern, Switzerland, Department of Cardiology Bern University, Hospital Inselspital, Bern, Switzerland
Addendum on mode of interventions for aortic stenosis: 2021 ESC/EACTS guidelines indications
Published on November 19, 2021
Introduction
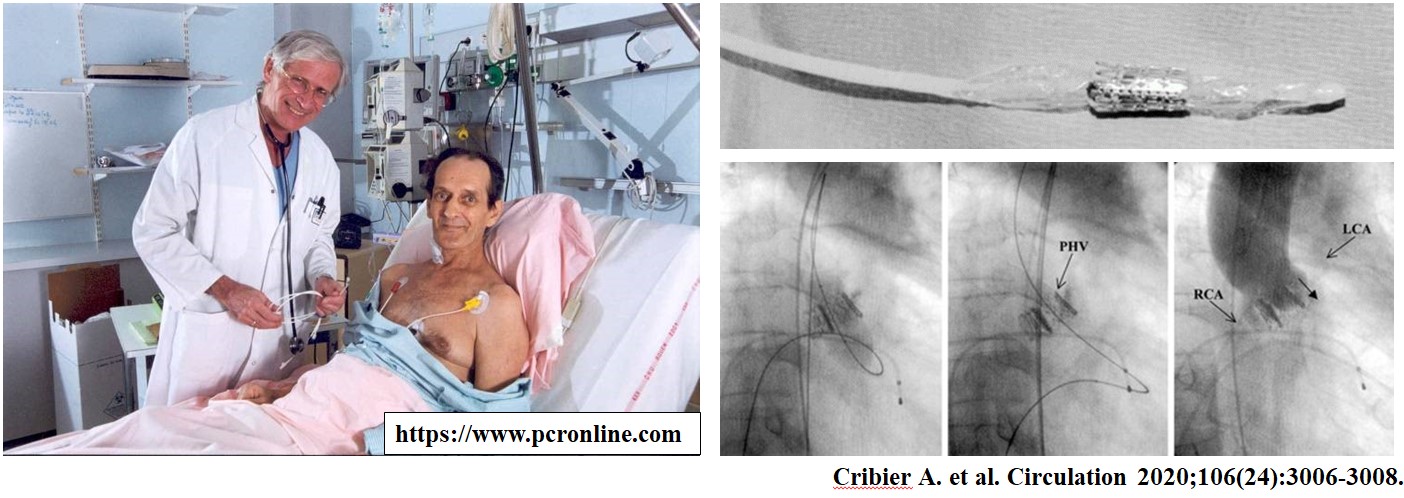
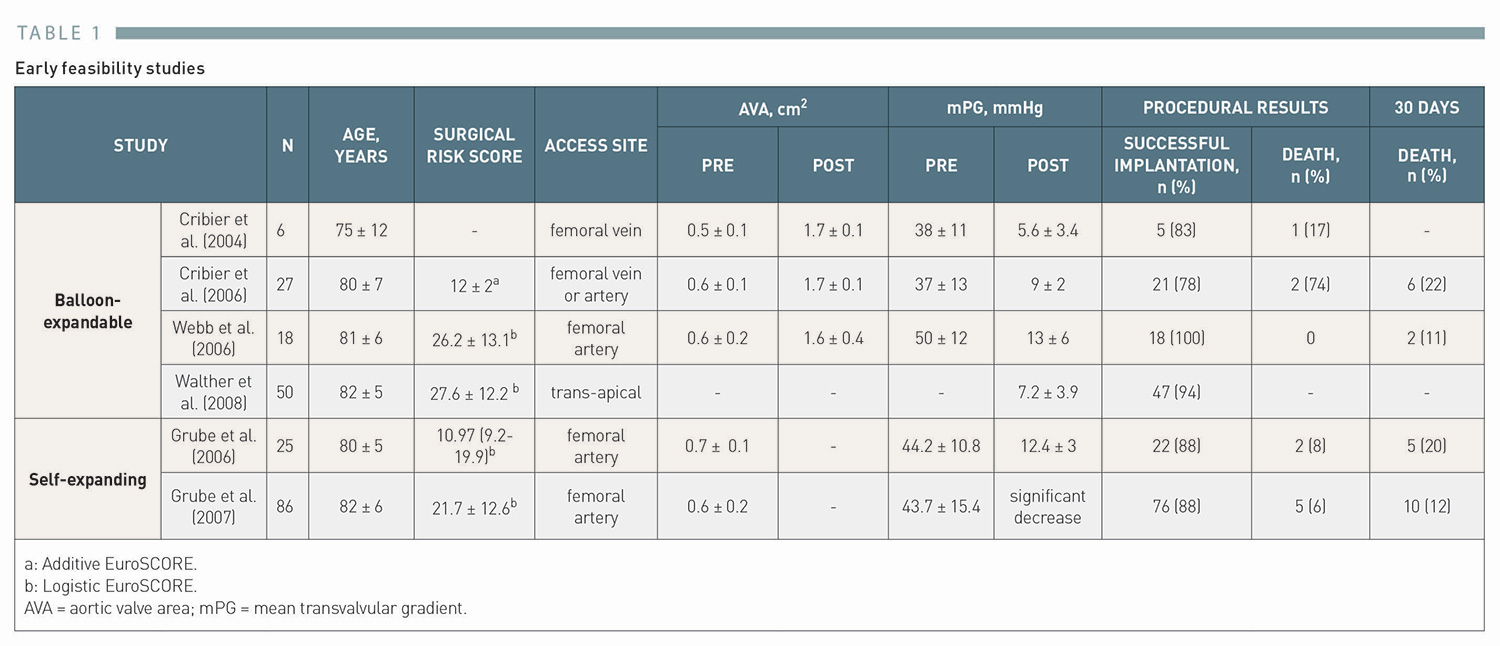
Surgical aortic valve replacement (SAVR) established in the 1960s has been the only definitive treatment for patients with aortic stenosis (AS) for more than four decades1. Effler DB, Favaloro R, Groves LK. Heart Valve Replacement. Clinical Experience. Ann Thorac Surg. 1965;1:4-24. Link. In 1986, Cribier and colleagues introduced balloon aortic valvuloplasty (BAV) as an alternative treatment for inoperable patients with severe AS2. Cribier A, Savin T, Saoudi N, Rocha P, Berland J, Letac B. Percutaneous transluminal valvuloplasty of acquired aortic stenosis in elderly patients: an alternative to valve replacement. Lancet. 1986;1(8472):63-7. Link. Although BAV achieved favourable acute hemodynamic outcomes, restenosis and clinical deterioration occur in most cases within 6-12 months and repeat procedures are frequently needed, 3. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62(4):270-5. Link4. Lieberman EB, Bashore TM, Hermiller JB, Wilson JS, Pieper KS, Keeler GP, Pierce CH, Kisslo KB, Harrison JK, Davidson CJ. Balloon aortic valvuloplasty in adults: failure of procedure to improve long-term survival. J Am Coll Cardiol. 1995;26(6):1522-8. Link. To address the limitation, the concept of transcatheter heart valve (THV) where a bioprosthetic valve was sewn into a stenting scaffold has been developed and repeatedly tested in animal models, 5. Andersen HR, Knudsen LL, Hasenkam JM. Transluminal implantation of artificial heart valves. Description of a new expandable aortic valve and initial results with implantation by catheter technique in closed chest pigs. Eur Heart J. 1992;13(5):704-8. Link6. Cribier AG. The Odyssey of TAVR from concept to clinical reality. Tex Heart Inst J. 2014;41(2):125-30. Link. In 2002, Cribier and colleagues performed the first-in-human antegrade transcatheter aortic valve implantation (TAVI), using a 24 Fr catheter delivery system that housed a 23 mm bovine pericardial balloon-expandable stent-valve (Figure 1) in a 57-year old inoperable patient with cardiogenic shock due to severe AS7. Cribier A, Eltchaninoff H, Bash A, Borenstein N, Tron C, Bauer F, Derumeaux G, Anselme F, Laborde F, Leon MB. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation. 2002;106(24):3006-8. Link. This patient had remarkable hemodynamic improvement after the procedure leading to subsequent feasibility studies (Table 1).
In the first study, the balloon-expandable THV composed of a stainless steel stent and bovine pericardial leaflets was successfully implanted in five out of six patients using a trans-septal antegrade approach via the femoral vein (24 Fr delivery system)8. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Sebagh L, Bash A, Nusimovici D, Litzler PY, Bessou JP, Leon MB. Early experience with percutaneous transcatheter implantation of heart valve prosthesis for the treatment of end-stage inoperable patients with calcific aortic stenosis. J Am Coll Cardiol. 2004;43(4):698-703. Link. In subsequent studies, successful implantation of the THV using a retrograde approach via the femoral artery (22-24 Fr delivery system) was reported9. Cribier A, Eltchaninoff H, Tron C, Bauer F, Agatiello C, Nercolini D, Tapiero S, Litzler PY, Bessou JP, Babaliaros V. Treatment of calcific aortic stenosis with the percutaneous heart valve: mid-term follow-up from the initial feasibility studies: the French experience. J Am Coll Cardiol. 2006;47(6):1214-23. Link. In 2007, trans-apical access (33 Fr delivery system) was introduced, and 47 out of 50 surgical high-risk patients had successful implantation of the balloon-expandable THV (Edwards SAPIEN THV, Edwards Lifesciences, Irvine, California)10. Walther T, Falk V, Kempfert J, Borger MA, Fassl J, Chu MW, Schuler G, Mohr FW. Transapical minimally invasive aortic valve implantation; the initial 50 patients. Eur J Cardiothorac Surg. 2008;33(6):983-8. Link. In parallel, a self-expanding THV consisting of a nitinol frame and porcine pericardial leaflets has been developed (CoreValve, Medtronic, Minneapolis, Minnesota) (Figure 2)11. Grube E, Laborde JC, Gerckens U, Felderhoff T, Sauren B, Buellesfeld L, Mueller R, Menichelli M, Schmidt T, Zickmann B, Iversen S, Stone GW. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-risk patients with aortic valve disease: the Siegburg first-in-man study. Circulation. 2006;114(15):1616-24. Link. In 2006, Grube and colleagues reported the first-in-human results of the CoreValve experience. Successful implantation was achieved via the retrograde approach (21-24 Fr delivery system) in 22 out of 25 patients11. Grube E, Laborde JC, Gerckens U, Felderhoff T, Sauren B, Buellesfeld L, Mueller R, Menichelli M, Schmidt T, Zickmann B, Iversen S, Stone GW. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-risk patients with aortic valve disease: the Siegburg first-in-man study. Circulation. 2006;114(15):1616-24. Link. In a subsequent study using the second and third iteration CoreValve system (18-21 Fr delivery system), a total of 86 high-risk or inoperable patients were enrolled, and the implantation was successful in 76 patients (88%)12. Grube E, Schuler G, Buellesfeld L, Gerckens U, Linke A, Wenaweser P, Sauren B, Mohr FW, Walther T, Zickmann B, Iversen S, Felderhoff T, Cartier R, Bonan R. Percutaneous aortic valve replacement for severe aortic stenosis in high-risk patients using the second- and current third-generation self-expanding CoreValve prosthesis: device success and 30-day clinical outcome. J Am Coll Cardiol. 2007;50(1):69-76. Link. Throughout these studies, successful implantation of the THV resulted in significant hemodynamic improvement with favourable short-term clinical outcomes (Table 1).
Figure 2
First implantation of the CoreValve ReValving System
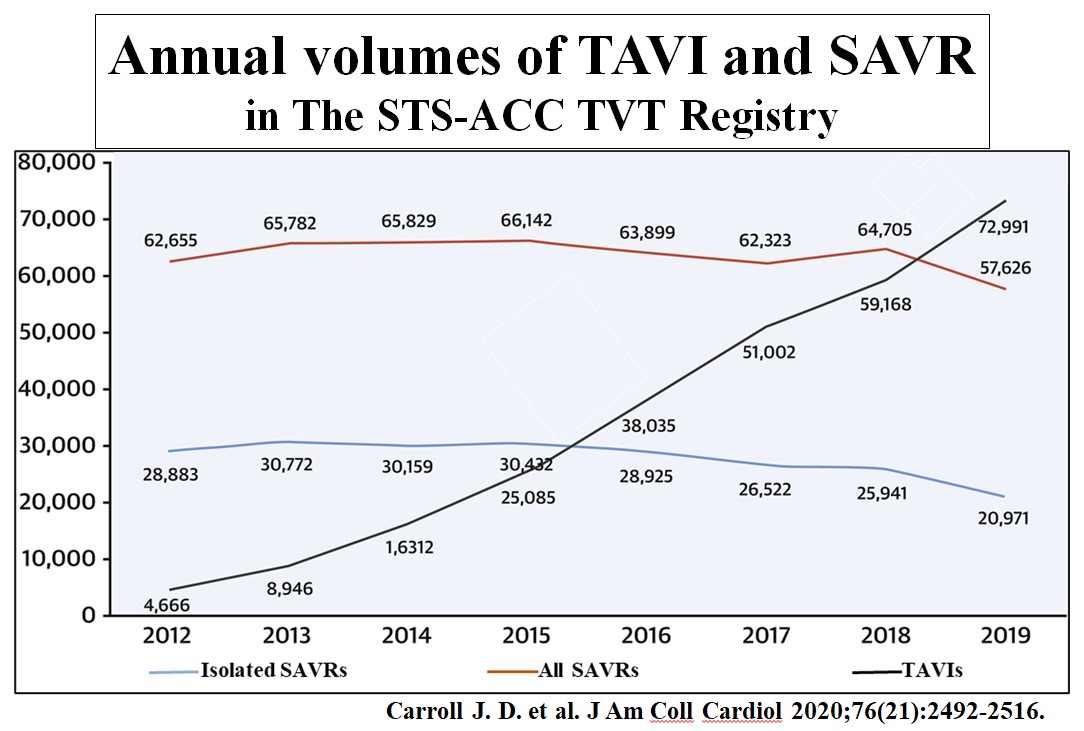
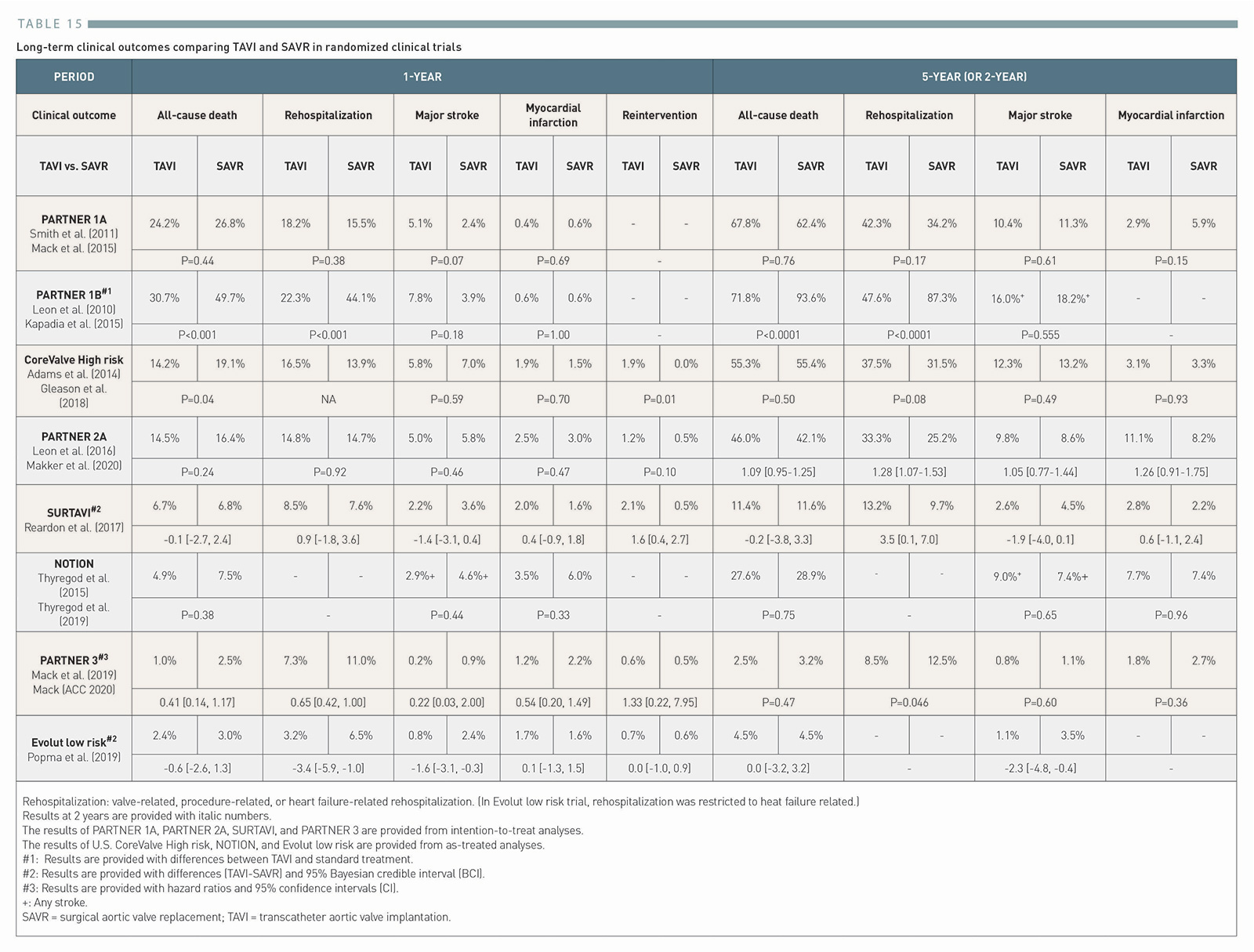
TAVI has rapidly evolved with iterative improvements both in devices and implantation technique as well as generation of robust clinical evidence derived from several randomized clinical trials , , , , , , , 13. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S, Investigators PT. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-607. Link14. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ, Investigators PT. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98. Link15. Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, Gleason TG, Buchbinder M, Hermiller J, Jr., Kleiman NS, Chetcuti S, Heiser J, Merhi W, Zorn G, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte J, Maini B, Mumtaz M, Chenoweth S, Oh JK, Investigators USCC. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370(19):1790-8. Link16. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, Doshi D, Cohen DJ, Pichard AD, Kapadia S, Dewey T, Babaliaros V, Szeto WY, Williams MR, Kereiakes D, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Moses JW, Trento A, Brown DL, Fearon WF, Pibarot P, Hahn RT, Jaber WA, Anderson WN, Alu MC, Webb JG, Investigators P. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374(17):1609-20. Link17. Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Sondergaard L, Mumtaz M, Adams DH, Deeb GM, Maini B, Gada H, Chetcuti S, Gleason T, Heiser J, Lange R, Merhi W, Oh JK, Olsen PS, Piazza N, Williams M, Windecker S, Yakubov SJ, Grube E, Makkar R, Lee JS, Conte J, Vang E, Nguyen H, Chang Y, Mugglin AS, Serruys PW, Kappetein AP, Investigators S. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376(14):1321-1331. Link18. Thyregod HG, Steinbruchel DA, Ihlemann N, Nissen H, Kjeldsen BJ, Petursson P, Chang Y, Franzen OW, Engstrom T, Clemmensen P, Hansen PB, Andersen LW, Olsen PS, Sondergaard L. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65(20):2184-94. Link19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. After the regulatory approval of TAVI in Europe in 2007 and the United States (US) in 2011, TAVI has been widely adopted across Europe, Asia and North America, , 21. Eggebrecht H, Mehta RH. Transcatheter aortic valve implantation (TAVI) in Germany 2008-2014: on its way to standard therapy for aortic valve stenosis in the elderly. EuroIntervention. 2016;11(9):1029-33. Link22. Carroll JD, Mack MJ, Vemulapalli S, Herrmann HC, Gleason TG, Hanzel G, Deeb GM, Thourani VH, Cohen DJ, Desai N, Kirtane AJ, Fitzgerald S, Michaels J, Krohn C, Masoudi FA, Brindis RG, Bavaria JE. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76(21):2492-2516. Link23. Durko AP, Osnabrugge RL, Van Mieghem NM, Milojevic M, Mylotte D, Nkomo VT, Pieter Kappetein A. Annual number of candidates for transcatheter aortic valve implantation per country: current estimates and future projections. Eur Heart J. 2018;39(28):2635-2642. Link, and is now the “standard of care” for the treatment of severe AS alongside SAVR (Figure 3), 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link. In this chapter, we will provide a detailed description of current indications, patient selection for TAVI, and the procedural considerations. Furthermore, we will summarize the available evidence and emerging indications in the field of TAVI.
The primary aetiology of AS includes degenerative changes, congenital abnormalities, and rheumatic valve disease. Degenerative calcific stenosis is the most prevalent form of AS26. Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM, Pibarot P. Calcific aortic stenosis. Nat Rev Dis Primers. 2016;2:16006. Link. It is characterized by progressive fibro-calcific remodelling and thickening of the aortic valve leaflets caused by genetic factors, lipoprotein deposition and oxidation, chronic inflammation, and osteoblastic transformation of cardiac valve interstitial cells26. Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM, Pibarot P. Calcific aortic stenosis. Nat Rev Dis Primers. 2016;2:16006. Link. Clinical risk factors mediating the degenerative change of the aortic valve include advanced age, male gender, hypertension, diabetes, hypercholesterolemia, and smoking, similar to risk factors for atherosclerosis, 27. Stewart BF, Siscovick D, Lind BK, Gardin JM, Gottdiener JS, Smith VE, Kitzman DW, Otto CM. Clinical factors associated with calcific aortic valve disease. Cardiovascular Health Study. J Am Coll Cardiol. 1997;29(3):630-4. Link28. Sverdlov AL, Ngo DT, Chapman MJ, Ali OA, Chirkov YY, Horowitz JD. Pathogenesis of aortic stenosis: not just a matter of wear and tear. Am J Cardiovasc Dis. 2011;1(2):185-99. Link. Indeed, both clinical entities frequently co-exist29. Goel SS, Ige M, Tuzcu EM, Ellis SG, Stewart WJ, Svensson LG, Lytle BW, Kapadia SR. Severe aortic stenosis and coronary artery disease--implications for management in the transcatheter aortic valve replacement era: a comprehensive review. J Am Coll Cardiol. 2013;62(1):1-10. Link. Bicuspid aortic valve is the most common congenital heart disease related to AS occurring in 1-2% of the general population30. Fedak PW, Verma S, David TE, Leask RL, Weisel RD, Butany J. Clinical and pathophysiological implications of a bicuspid aortic valve. Circulation. 2002;106(8):900-4. Link. Patients with bicuspid anatomy are more often exposed to degenerative changes and develop AS one or two decades earlier than those with a tricuspid valve26. Lindman BR, Clavel MA, Mathieu P, Iung B, Lancellotti P, Otto CM, Pibarot P. Calcific aortic stenosis. Nat Rev Dis Primers. 2016;2:16006. Link, and the majority of aortic valve replacements in patients ≤70 years of age are related to bicuspid anatomy, 31. Roberts WC, Ko JM. Frequency by decades of unicuspid, bicuspid, and tricuspid aortic valves in adults having isolated aortic valve replacement for aortic stenosis, with or without associated aortic regurgitation. Circulation. 2005;111(7):920-5. Link32. Siu SC, Silversides CK. Bicuspid aortic valve disease. J Am Coll Cardiol. 2010;55(25):2789-800. Link. Rheumatic valve disease is another important cause of aortic stenosis. It is characterized by non-calcific thickening of the leaflets and fusion of the commissures33. Roberts K, Colquhoun S, Steer A, Remenyi B, Carapetis J. Screening for rheumatic heart disease: current approaches and controversies. Nat Rev Cardiol. 2013;10(1):49-58. Link. While it is less common in industrialized nations due to appropriate preventive measures, it remains a common health problem in developing countries, and the diagnosis should be considered specifically in recently immigrated patients from these countries34. Otto CM, Prendergast B. Aortic-valve stenosis--from patients at risk to severe valve obstruction. N Engl J Med. 2014;371(8):744-56. Link.
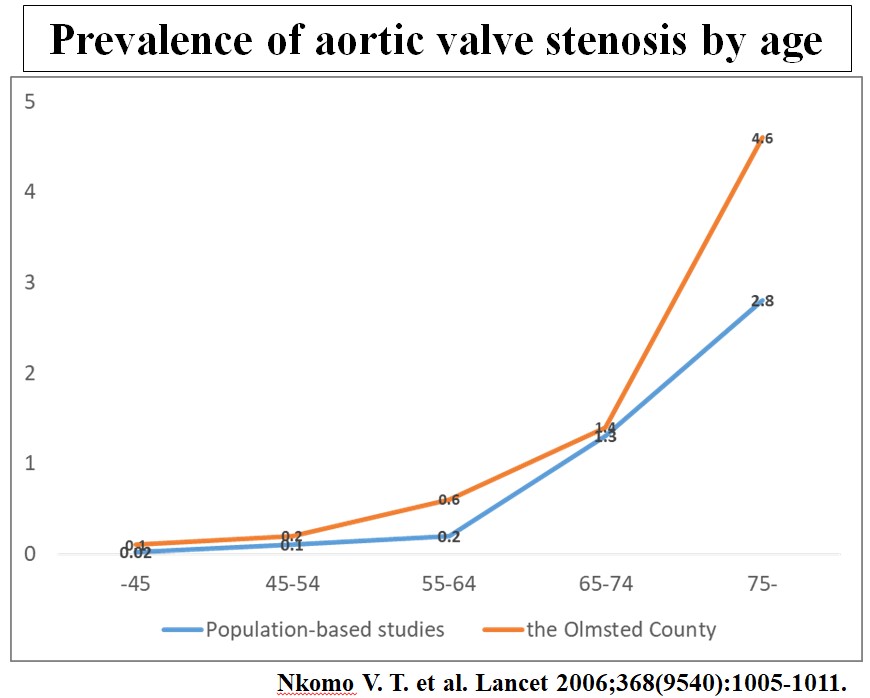
The prevalence of aortic stenosis
The global burden of degenerative AS is increasing due to aging of the population and population growth. In the general US population in areas with systematic echocardiography, the prevalence of moderate or severe AS ranges from 0.02% to 0.1% in subjects aged <45 years to as high as 2.8% to 4.6% in those aged ≥75 years (Figure 4)35. Nkomo VT, Gardin JM, Skelton TN, Gottdiener JS, Scott CG, Enriquez-Sarano M. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368(9540):1005-11. Link. In 2017, there were an estimated 12.6 million (95% uncertainty interval [UI] 11.4 million-13.8 million) cases of calcific aortic valve disease and an estimated 102,700 (95% UI 82,700-107,900) calcific aortic valve disease deaths globally36. Yadgir S, Johnson CO, Aboyans V, Adebayo OM, Adedoyin RA, Afarideh M, Alahdab F, Alashi A, Alipour V, Arabloo J, Azari S, Barthelemy CM, Benziger CP, Berman AE, Bijani A, Carrero JJ, Carvalho F, Daryani A, Duraes AR, Esteghamati A, Farid TA, Farzadfar F, Fernandes E, Filip I, Gad MM, Hamidi S, Hay SI, Ilesanmi OS, Naghibi Irvani SS, Jurisson M, Kasaeian A, Kengne AP, Khan AR, Kisa A, Kisa S, Kolte D, Manafi N, Manafi A, Mensah GA, Mirrakhimov EM, Mohammad Y, Mokdad AH, Negoi RI, Thi Nguyen HL, Nguyen TH, Nixon MR, Otto CM, Patel S, Pilgrim T, Radfar A, Rawaf DL, Rawaf S, Rawasia WF, Rezapour A, Roever L, Saad AM, Saadatagah S, Senthilkumaran S, Sliwa K, Tesfay BE, Tran BX, Ullah I, Vaduganathan M, Vasankari TJ, Wolfe CDA, Yonemoto N, Roth GA, Global Burden of Disease Study Nonrheumatic Valve Disease C. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990-2017. Circulation. 2020;141(21):1670-1680. Link. A recent study estimated that nearly 270,000 patients per year could be potential TAVI candidates in European countries and North America following the expansion of TAVI to low-risk patients23. Durko AP, Osnabrugge RL, Van Mieghem NM, Milojevic M, Mylotte D, Nkomo VT, Pieter Kappetein A. Annual number of candidates for transcatheter aortic valve implantation per country: current estimates and future projections. Eur Heart J. 2018;39(28):2635-2642. Link. Furthermore, a shift towards the elderly in developing countries, where rheumatic fever remains the primary cause of AS, will lead to a transition from rheumatic to degenerative AS as a leading cause of aortic valve replacement in these countries and will further increase the global burden of AS requiring intervention36. Yadgir S, Johnson CO, Aboyans V, Adebayo OM, Adedoyin RA, Afarideh M, Alahdab F, Alashi A, Alipour V, Arabloo J, Azari S, Barthelemy CM, Benziger CP, Berman AE, Bijani A, Carrero JJ, Carvalho F, Daryani A, Duraes AR, Esteghamati A, Farid TA, Farzadfar F, Fernandes E, Filip I, Gad MM, Hamidi S, Hay SI, Ilesanmi OS, Naghibi Irvani SS, Jurisson M, Kasaeian A, Kengne AP, Khan AR, Kisa A, Kisa S, Kolte D, Manafi N, Manafi A, Mensah GA, Mirrakhimov EM, Mohammad Y, Mokdad AH, Negoi RI, Thi Nguyen HL, Nguyen TH, Nixon MR, Otto CM, Patel S, Pilgrim T, Radfar A, Rawaf DL, Rawaf S, Rawasia WF, Rezapour A, Roever L, Saad AM, Saadatagah S, Senthilkumaran S, Sliwa K, Tesfay BE, Tran BX, Ullah I, Vaduganathan M, Vasankari TJ, Wolfe CDA, Yonemoto N, Roth GA, Global Burden of Disease Study Nonrheumatic Valve Disease C. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990-2017. Circulation. 2020;141(21):1670-1680. Link.
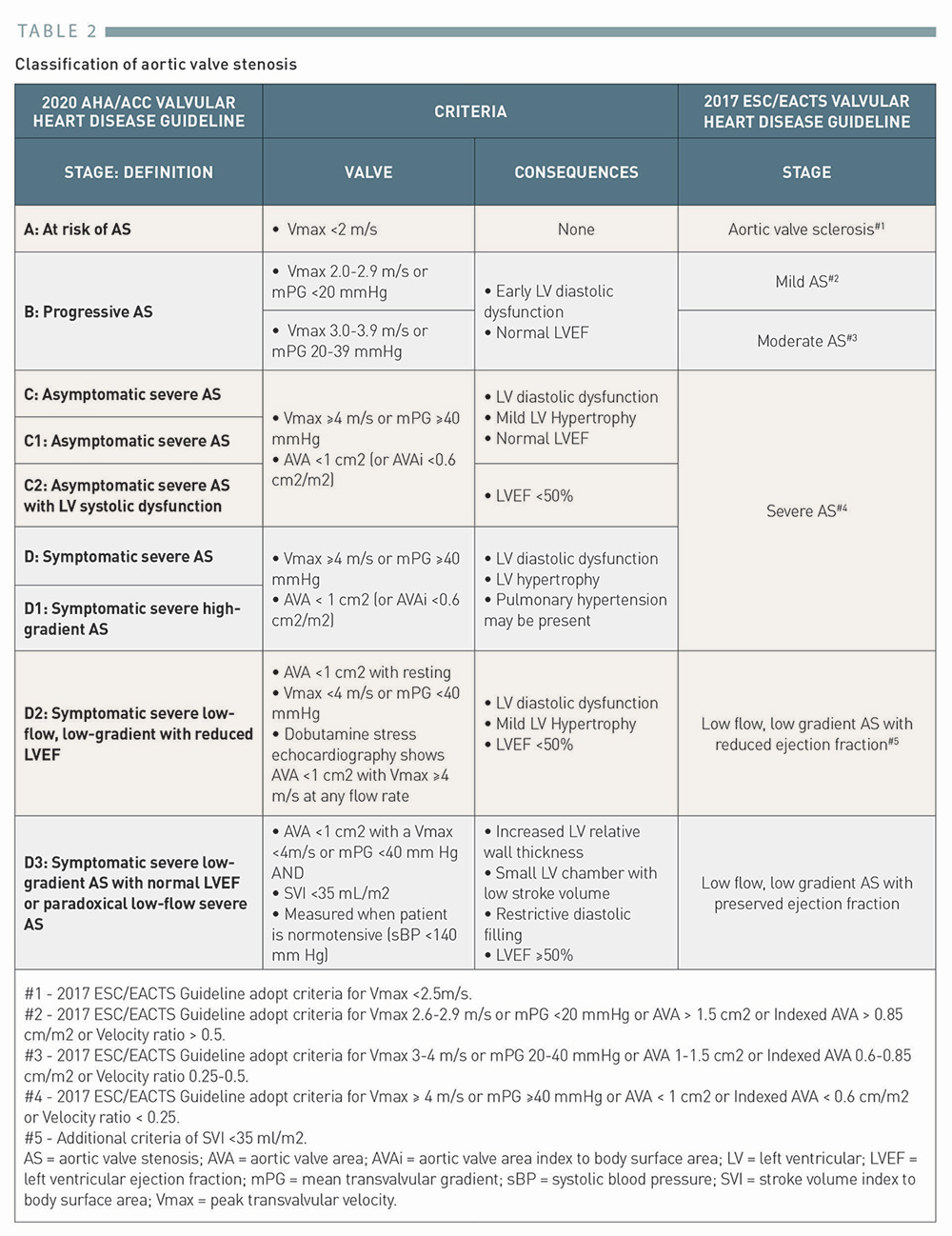
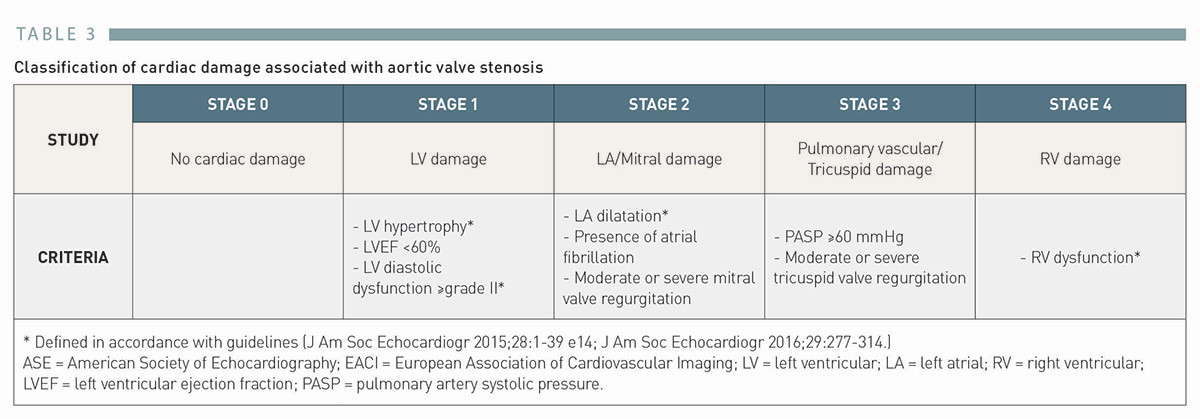
AS is a progressive disease defined by the presence of aortic valve thickening and/or calcification resulting in significant hemodynamic burden and afterload increase. The diagnosis and classification of AS should be based on the integration of clinical symptoms (dyspnoea, angina, and syncope) and echocardiographic assessment (transaortic velocity, pressure gradient, and aortic valve area) (Table 2). While US and European guidelines propose different classification schemes of AS, the definition of severe AS, the target of replacement therapy, is consistent and comprises transaortic velocity ≥4 m/sec, mean transvalvular pressure gradient ≥40 mmHg, and aortic valve area ≤1 cm, 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link (Table 2). As downstream cardiac damage caused by long-standing increased ventricular wall stress frequently coexists and affects prognosis in patients with AS, a new staging classification characterizing the extent of cardiac damage, instead of the valve-related factors, was recently proposed and validated in several independent cohorts, 37. Genereux P, Pibarot P, Redfors B, Mack MJ, Makkar RR, Jaber WA, Svensson LG, Kapadia S, Tuzcu EM, Thourani VH, Babaliaros V, Herrmann HC, Szeto WY, Cohen DJ, Lindman BR, McAndrew T, Alu MC, Douglas PS, Hahn RT, Kodali SK, Smith CR, Miller DC, Webb JG, Leon MB. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J. 2017;38(45):3351-3358. Link38. Fukui M, Gupta A, Abdelkarim I, Sharbaugh MS, Althouse AD, Elzomor H, Mulukutla S, Lee JS, Schindler JT, Gleason TG, Cavalcante JL. Association of Structural and Functional Cardiac Changes With Transcatheter Aortic Valve Replacement Outcomes in Patients With Aortic Stenosis. JAMA Cardiol. 2019;4(3):215-222. Link(Table 3).
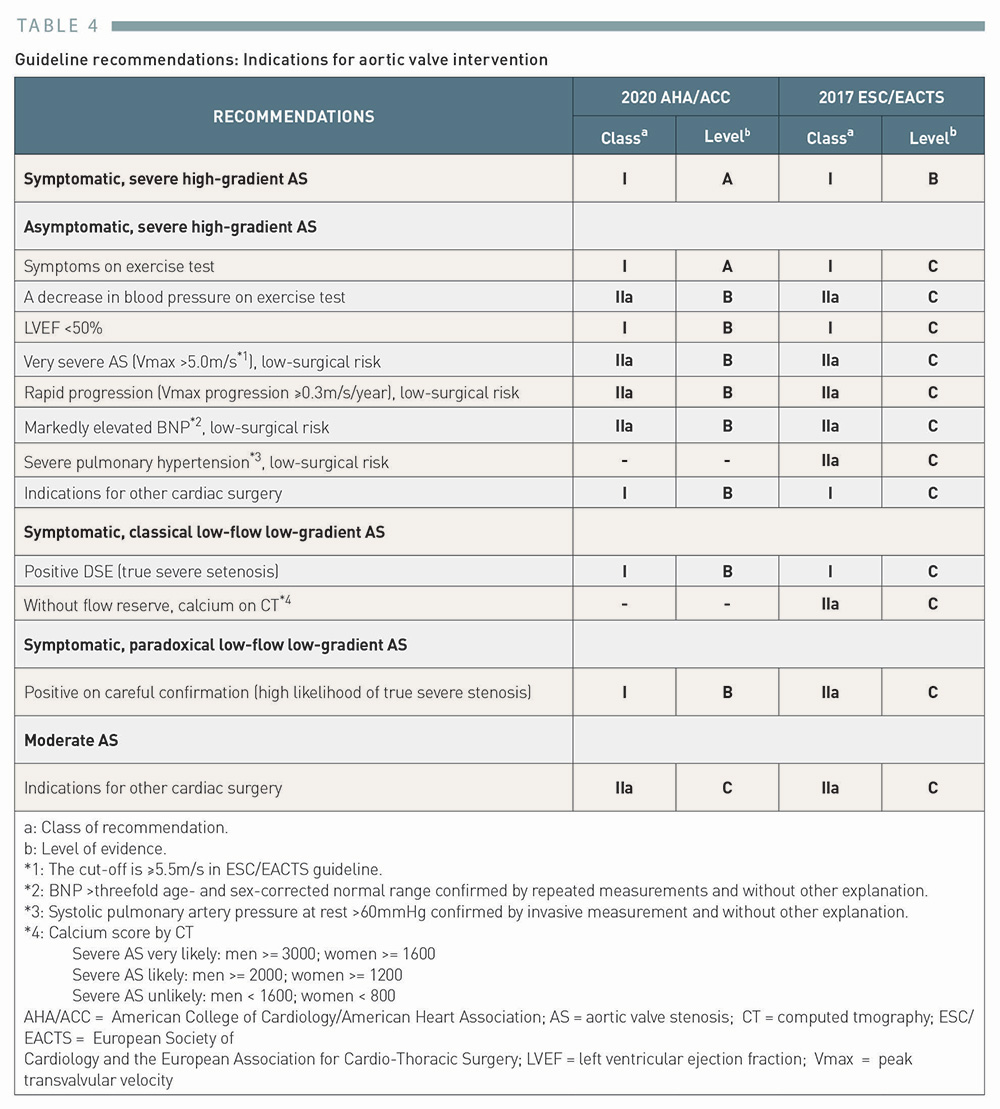
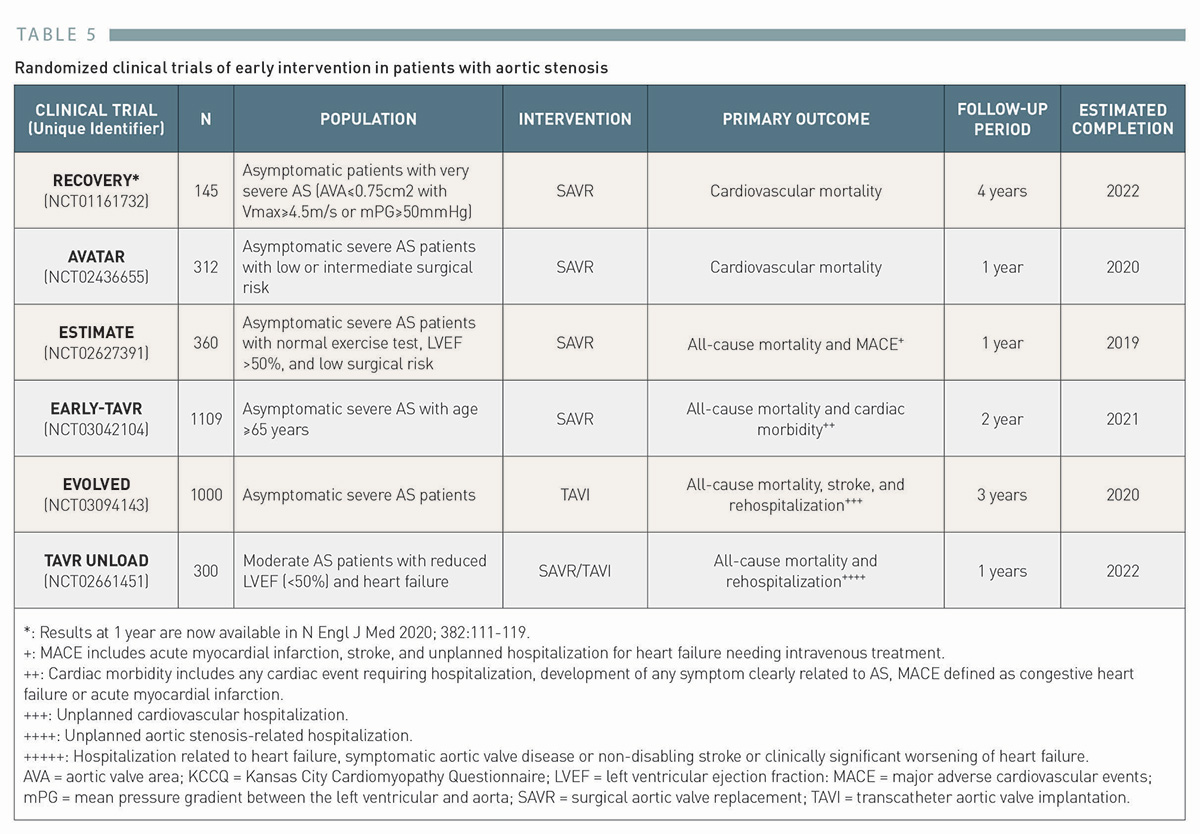
Aortic valve replacement therapy (TAVI or SAVR) should be considered in case of severe AS with/without relevant symptoms (Table 4). Currently, guidelines do not provide clear guidance for patients in grey zone entities such as moderate AS or asymptomatic severe AS without signs of reduced left ventricular (LV) ejection fraction, very severe stenosis, elevated biomarkers, pulmonary hypertension, or rapid progression, 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link. However, recent observational studies suggest poorer prognosis than previously expected in these patients, raising interest in earlier intervention. In a multicentre registry including 1,808 asymptomatic patients with severe AS, the long-term outcome was poor when managed conservatively, and was significantly better when treated with early SAVR in a propensity-score matched analysis (5-year mortality: 26.4% vs. 15.4%, P=0.009)40. Taniguchi T, Morimoto T, Shiomi H, Ando K, Kanamori N, Murata K, Kitai T, Kawase Y, Izumi C, Miyake M, Mitsuoka H, Kato M, Hirano Y, Matsuda S, Nagao K, Inada T, Murakami T, Takeuchi Y, Yamane K, Toyofuku M, Ishii M, Minamino-Muta E, Kato T, Inoko M, Ikeda T, Komasa A, Ishii K, Hotta K, Higashitani N, Kato Y, Inuzuka Y, Maeda C, Jinnai T, Morikami Y, Sakata R, Kimura T, Investigators CAR. Initial Surgical Versus Conservative Strategies in Patients With Asymptomatic Severe Aortic Stenosis. J Am Coll Cardiol. 2015;66(25):2827-2838. Link. Furthermore, in a large observational study including more than 200,000 participants with systematic assessment of AS severity, even moderate AS was associated with poor long-term survival that was similar to those with severe AS (5-year mortality: 56% and 67%, respectively)41. Strange G, Stewart S, Celermajer D, Prior D, Scalia GM, Marwick T, Ilton M, Joseph M, Codde J, Playford D, National Echocardiography Database of Australia contributing s. Poor Long-Term Survival in Patients With Moderate Aortic Stenosis. J Am Coll Cardiol. 2019;74(15):1851-1863. Link. With advances in techniques and technology of aortic valve replacement therapies, the procedural risk has been continuously reduced, and therefore, these patients may also potentially benefit from aortic valve intervention. Currently, multiple randomized controlled trials are ongoing to evaluate the safety and efficacy of early intervention in patients with asymptomatic severe AS or moderate AS, 43. Bing R, Everett RJ, Tuck C, Semple S, Lewis S, Harkess R, Mills NL, Treibel TA, Prasad S, Greenwood JP, McCann GP, Newby DE, Dweck MR. Rationale and design of the randomized, controlled Early Valve Replacement Guided by Biomarkers of Left Ventricular Decompensation in Asymptomatic Patients with Severe Aortic Stenosis (EVOLVED) trial. Am Heart J. 2019;212:91-100. Link44. Spitzer E, Van Mieghem NM, Pibarot P, Hahn RT, Kodali S, Maurer MS, Nazif TM, Rodes-Cabau J, Paradis JM, Kappetein AP, Ben-Yehuda O, van Es GA, Kallel F, Anderson WN, Tijssen J, Leon MB. Rationale and design of the Transcatheter Aortic Valve Replacement to UNload the Left ventricle in patients with ADvanced heart failure (TAVR UNLOAD) trial. Am Heart J. 2016;182:80-88. Link (Table 5).
Table 4
Guideline recommendations: Indications for aortic valve intervention
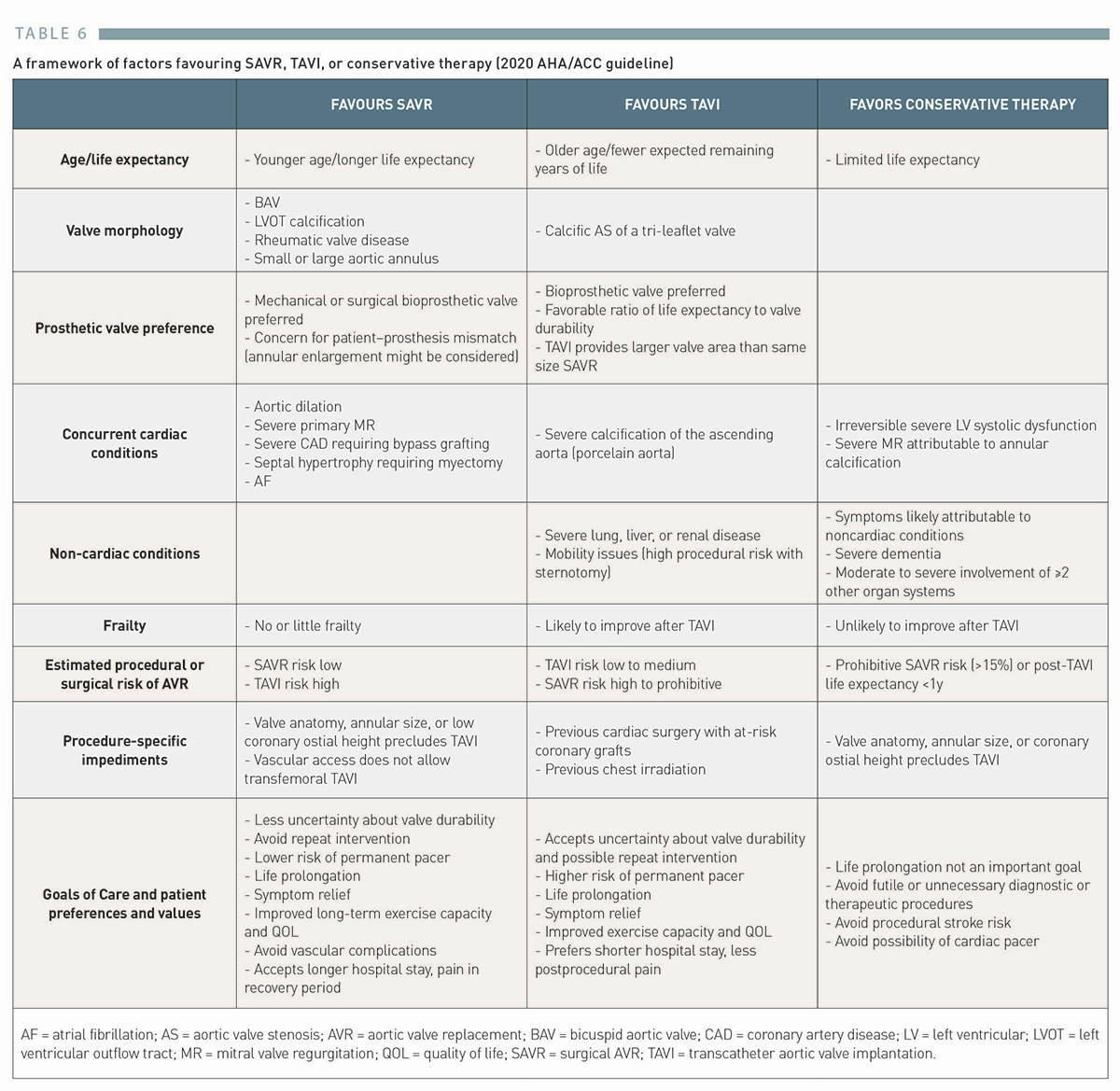
Indications for TAVI were first limited to high or prohibitive surgical risk patients with symptomatic severe AS45. Nishimura RA, Otto CM, Bonow RO, Carabello BA, Erwin JP, 3rd, Guyton RA, O’Gara PT, Ruiz CE, Skubas NJ, Sorajja P, Sundt TM, 3rd, Thomas JD, American College of Cardiology/American Heart Association Task Force on Practice G. 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2014;63(22):e57-185. Link. Following several iterative randomized clinical trials demonstrating superiority or non-inferiority of TAVI compared to SAVR, the most recent 2020 ACC/AHA Valvular Heart Disease guidelines recommend TAVI as alternative to SAVR in patients >65 years of age who are candidates for bioprostheses across the entire spectrum of surgical risk as assessed by the Heart team24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. As both replacement therapies have their own strengths and limitations, the decision making for TAVI versus SAVR should be made individually, considering age, clinical and anatomical factors, and patient preferences (Table 6). The multidisciplinary Heart team involved in the decision-making process should always be updated with backgrounds and available evidence on the pertinent factors. The subsequent sections highlight the most important factors that should be considered to form the basis of the individual decision-making.
Table 6
A framework of factors favouring SAVR, TAVI, or conservative therapy (2020 AHA/ACC guideline)
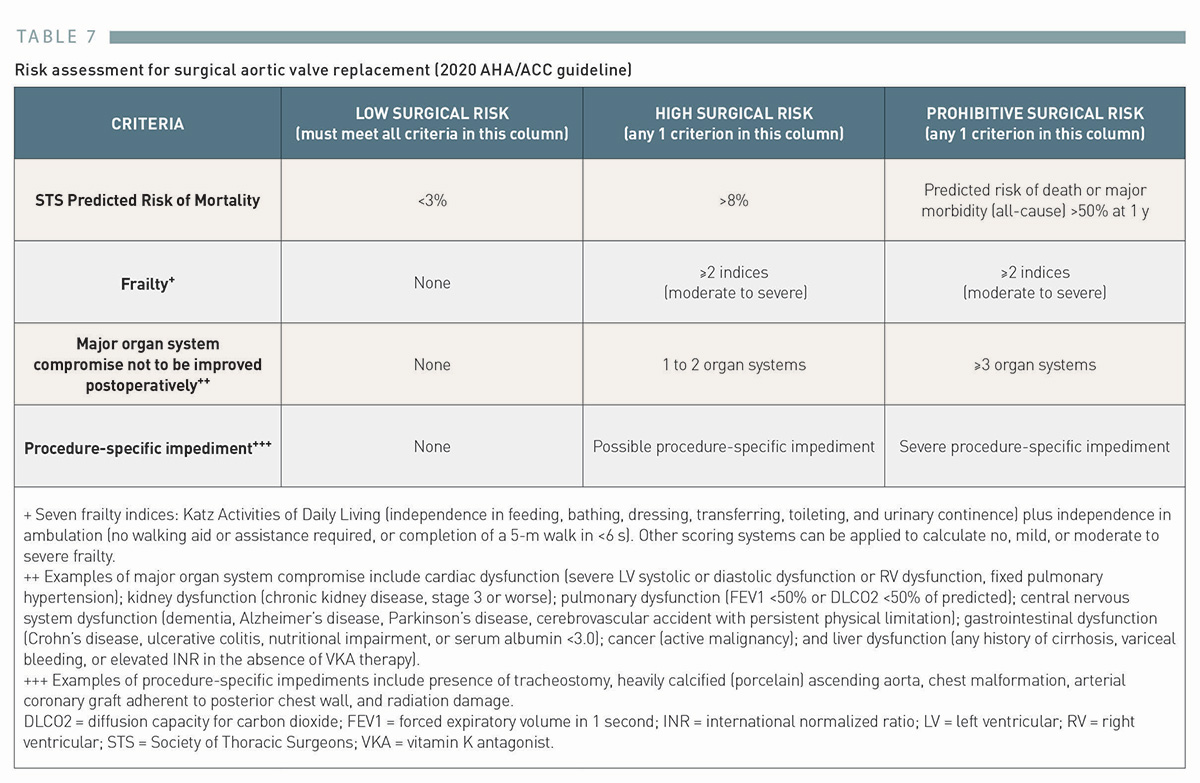
Surgical risk is usually assessed by risk scores such as STS-PROM (Society of Thoracic Surgeons Predicted Risk of Mortality) and EuroSCORE II, 46. O’Brien SM, Shahian DM, Filardo G, Ferraris VA, Haan CK, Rich JB, Normand SL, DeLong ER, Shewan CM, Dokholyan RS, Peterson ED, Edwards FH, Anderson RP, Society of Thoracic Surgeons Quality Measurement Task F. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2--isolated valve surgery. Ann Thorac Surg. 2009;88(1 Suppl):S23-42. Link47. Nashef SA, Roques F, Sharples LD, Nilsson J, Smith C, Goldstone AR, Lockowandt U. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41(4):734-44; discussion 744-5. Link. According to these scores, patients have been stratified into three risk categories: high (>8%), intermediate (4%-8%), and low (<3-4%) surgical risk. If patients have a predicted risk of death or major morbidity (all-cause) >50% at 1 year, disease affecting >3 major organ systems, moderate or severe frailty, or severe procedure-specific impediment (porcelain aorta, prior chest radiation, or arterial bypass graft adherent to the chest wall), they are considered to have a prohibitive surgical risk24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link (Table 7). While surgical risk classification based on the STS score was commonly used to establish evidence across the different risk categories and identify patients suitable for TAVI to date, it is only of limited utility today in the allocation of TAVI versus SAVR.
Table 7
Risk assessment for surgical aortic valve replacement (2020 AHA/ACC guideline)
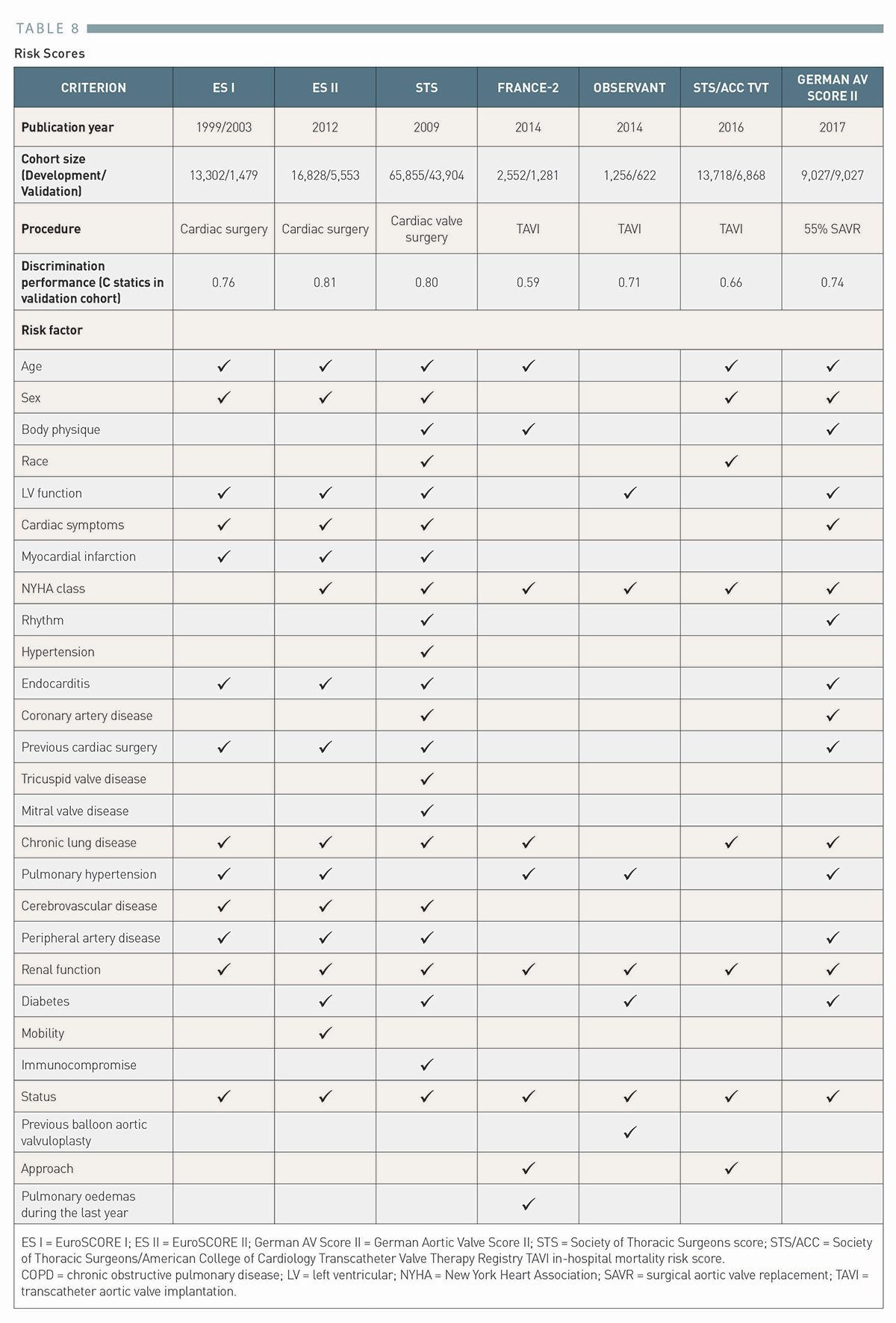
Of note, the risk scores (STS-PROM and EuroSCORE) have been derived from cohorts of patients undergoing cardiac surgery, and their predictive performances in TAVI patients have been limited48. Wang TKM, Wang MTM, Gamble GD, Webster M, Ruygrok PN. Performance of contemporary surgical risk scores for transcatheter aortic valve implantation: A meta-analysis. Int J Cardiol. 2017;236:350-355. Link. Although TAVI specific risk prediction models such as FRANCE-249. Iung B, Laouenan C, Himbert D, Eltchaninoff H, Chevreul K, Donzeau-Gouge P, Fajadet J, Leprince P, Leguerrier A, Lievre M, Prat A, Teiger E, Laskar M, Vahanian A, Gilard M, Investigators F. Predictive factors of early mortality after transcatheter aortic valve implantation: individual risk assessment using a simple score. Heart. 2014;100(13):1016-23. Link, OBSERVANT50. Capodanno D, Barbanti M, Tamburino C, D’Errigo P, Ranucci M, Santoro G, Santini F, Onorati F, Grossi C, Covello RD, Capranzano P, Rosato S, Seccareccia F, Group OR. A simple risk tool (the OBSERVANT score) for prediction of 30-day mortality after transcatheter aortic valve replacement. Am J Cardiol. 2014;113(11):1851-8. Link, GAVS-II51. Schiller W, Barnewold L, Kazmaier T, Beckmann A, Masseli F, Welz A, Szecsenyi J, Heller G. The German Aortic Valve Score II. Eur J Cardiothorac Surg. 2017;52(5):881-887. Link, and the TVT registry model52. Edwards FH, Cohen DJ, O’Brien SM, Peterson ED, Mack MJ, Shahian DM, Grover FL, Tuzcu EM, Thourani VH, Carroll J, Brennan JM, Brindis RG, Rumsfeld J, Holmes DR, Jr., Steering Committee of the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy R. Development and Validation of a Risk Prediction Model for In-Hospital Mortality After Transcatheter Aortic Valve Replacement. JAMA Cardiol. 2016;1(1):46-52. Link have been developed and validated, 53. Pilgrim T, Franzone A, Stortecky S, Nietlispach F, Haynes AG, Tueller D, Toggweiler S, Muller O, Ferrari E, Noble S, Maisano F, Jeger R, Roffi M, Grunenfelder J, Huber C, Wenaweser P, Windecker S. Predicting Mortality After Transcatheter Aortic Valve Replacement: External Validation of the Transcatheter Valve Therapy Registry Model. Circ Cardiovasc Interv. 2017;10(11). Link54. Wolff G, Shamekhi J, Al-Kassou B, Tabata N, Parco C, Klein K, Maier O, Sedaghat A, Polzin A, Sugiura A, Jung C, Grube E, Westenfeld R, Icks A, Zeus T, Sinning JM, Baldus S, Nickenig G, Kelm M, Veulemans V. Risk modeling in transcatheter aortic valve replacement remains unsolved: an external validation study in 2946 German patients. Clin Res Cardiol. 2020. Link, they did not outperform the conventional surgical risk scores (Table 8), and STS-PROM and EuroSCORE II remain the dominant risk prediction models in the current guidelines, 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link.
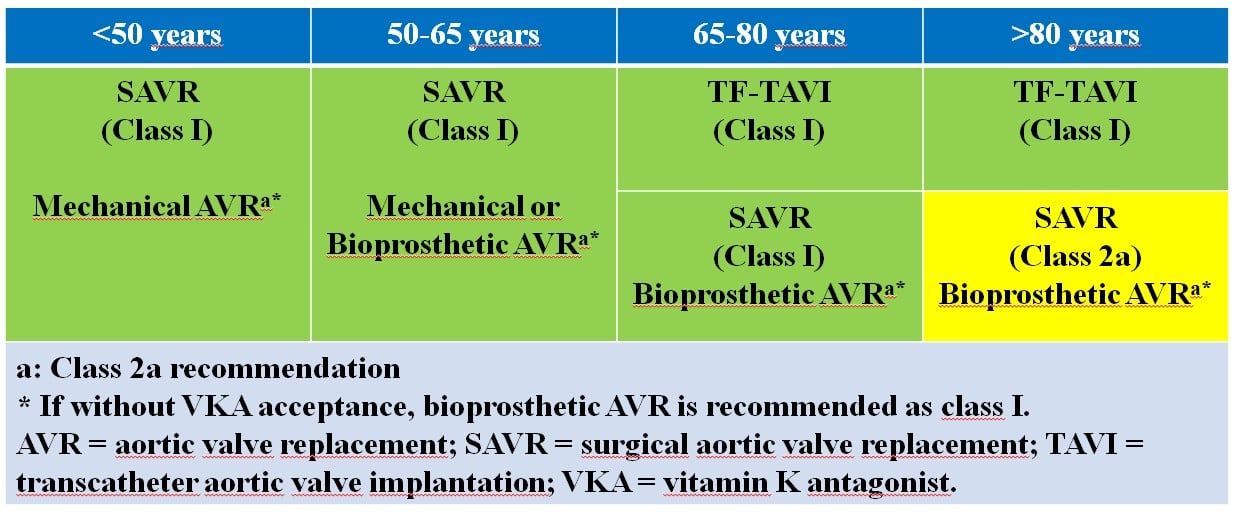
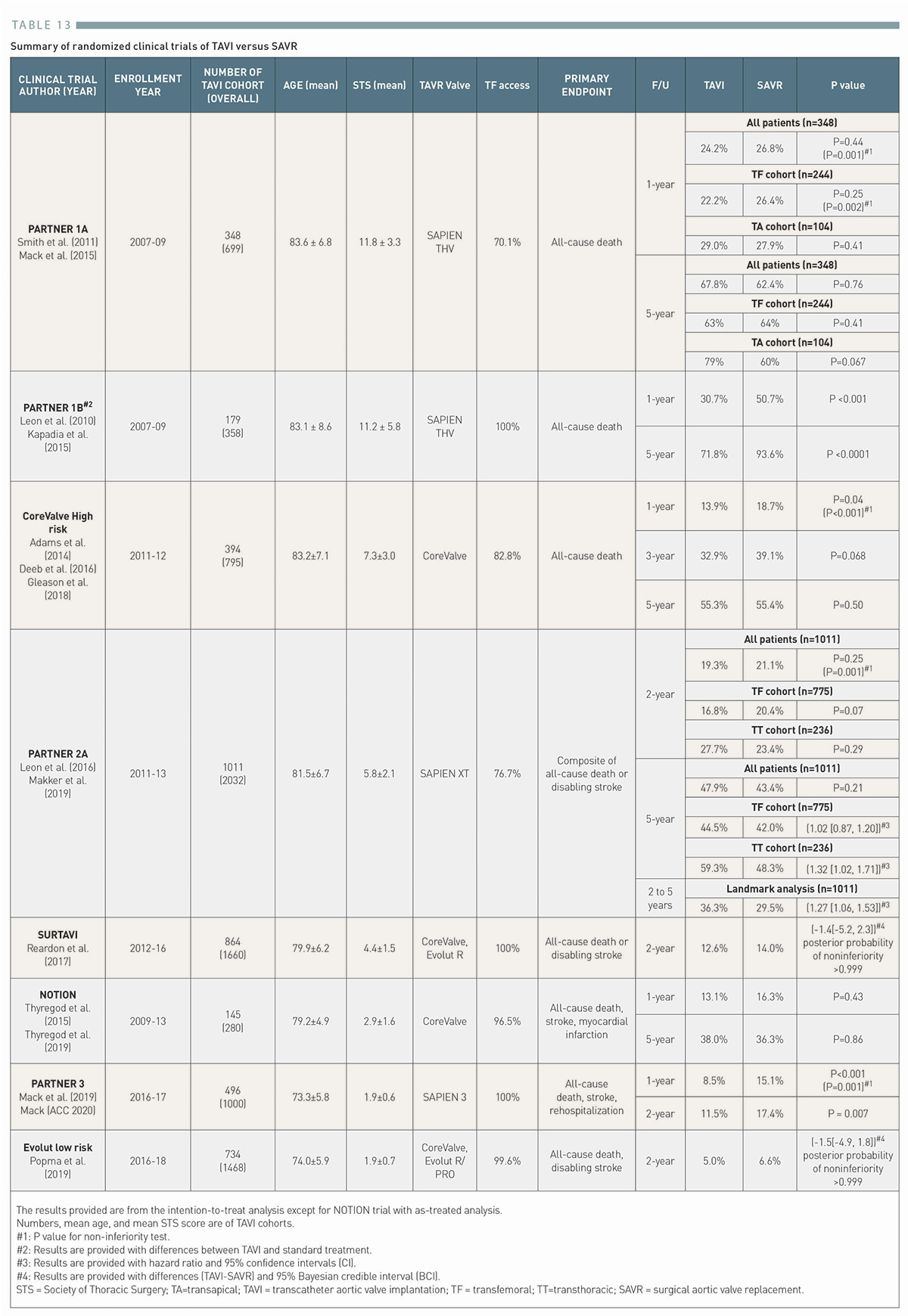
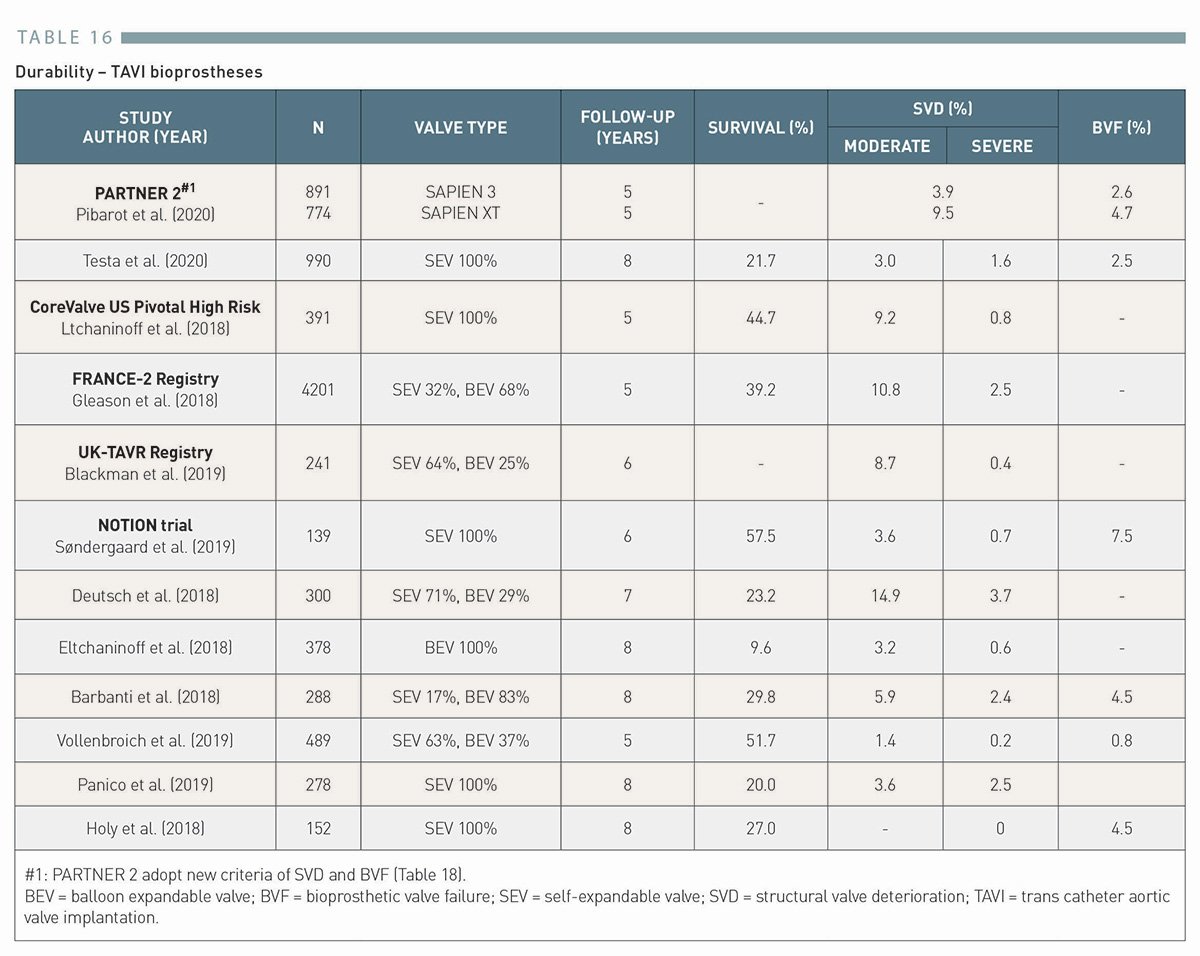
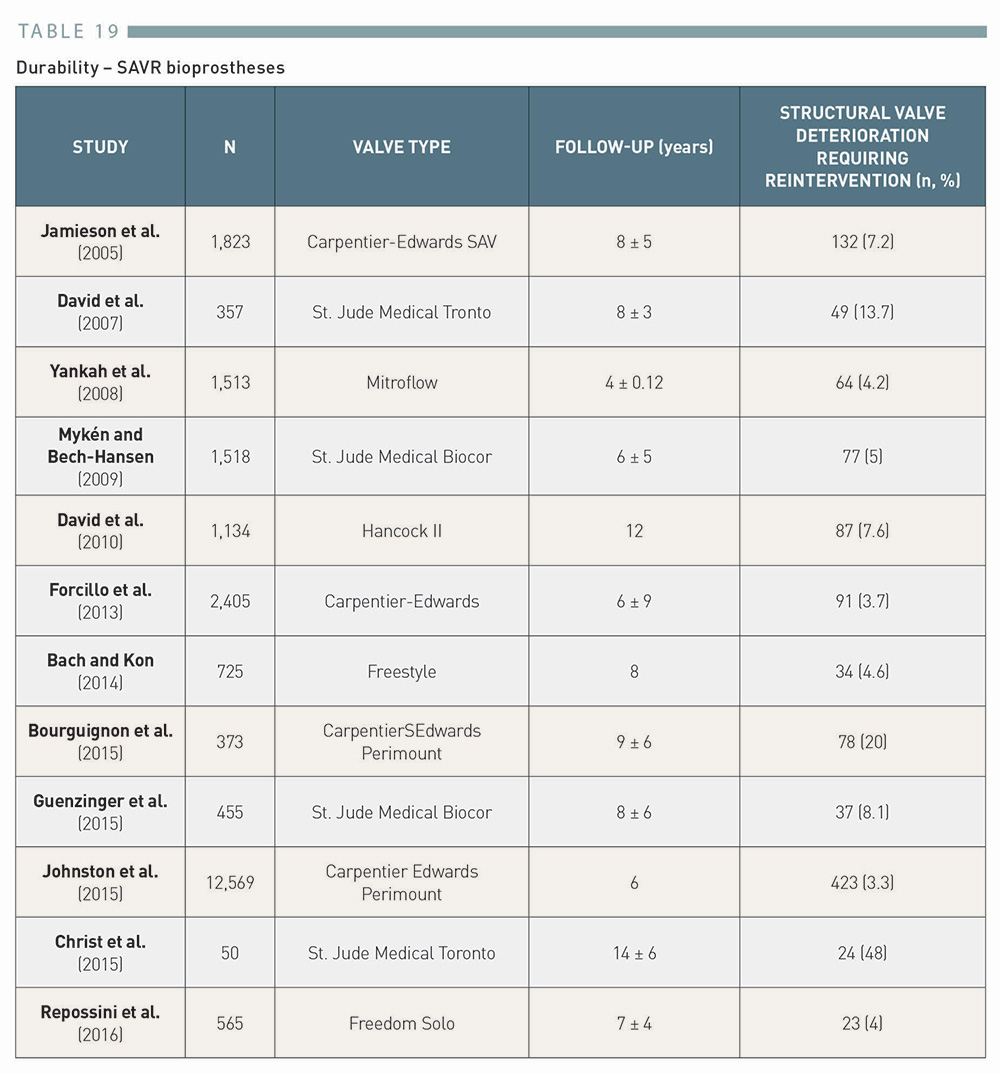
While surgical risk is no longer a dominant factor in decision-making, age remains one of the most important variables24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link (Figure 5). Although the peak age of patients undergoing TAVI or SAVR is >75 years of age, a non-negligible proportion of patients require intervention before 70 years of age55. Hamm CW, Mollmann H, Holzhey D, Beckmann A, Veit C, Figulla HR, Cremer J, Kuck KH, Lange R, Zahn R, Sack S, Schuler G, Walther T, Beyersdorf F, Bohm M, Heusch G, Funkat AK, Meinertz T, Neumann T, Papoutsis K, Schneider S, Welz A, Mohr FW, Board GA-E. The German Aortic Valve Registry (GARY): in-hospital outcome. Eur Heart J. 2014;35(24):1588-98. Link. Of note, even in the most recent low risk trials comparing TAVI and SAVR, the mean age of patients enrolled was >70 years, and only 7% in the PARTNER 3 trial19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link and 1.3% in the EVOLUT low-risk trial20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link were aged ≤60 years. Due to lack of evidence in younger populations, the most recent 2020 ACC/AHA Valvular Heart Disease guidelines provide recommendations for TAVI in patients aged ≥65 years, whereas SAVR with either mechanical or bioprosthetic valves is recommended for patients <65 years of age24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. For patients aged <50 years, the use of mechanical valves is particularly highlighted given a higher and earlier risk of bioprosthetic valve deterioration. In contrast, for patients who are >80 years of age or for younger patients with a life-expectancy <10 years without anatomic contraindication, transfemoral TAVI is recommended in preference to SAVR. In patients who are aged 65 to 80 years, both TAVI and SAVR should be considered according to these guidelines taking into account other clinical and anatomical factors as well as patient preferences24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. It should also be noted that data on durability of THVs is currently limited up to 8 years, as will be discussed in a later section. Clinically relevant deterioration of surgical bioprostheses typically occurs after >10 years. A balance between patient life-expectancy and known valve durability should always be carefully weighed in the decision-making of the Heart Team.
Figure 5
Simplified flowchart: choice of SAVR versus TAVI according to age based on 2020 ACC/AHA Valvular Heart Disease Guidelines
Observational studies have suggested that TAVI may be of particular benefit in women, 56. Saad M, Nairooz R, Pothineni NVK, Almomani A, Kovelamudi S, Sardar P, Katz M, Abdel-Wahab M, Bangalore S, Kleiman NS, Block PC, Abbott JD. Long-Term Outcomes With Transcatheter Aortic Valve Replacement in Women Compared With Men: Evidence From a Meta-Analysis. JACC Cardiovasc Interv. 2018;11(1):24-35. Link57. Chieffo A, Petronio AS, Mehilli J, Chandrasekhar J, Sartori S, Lefevre T, Presbitero P, Capranzano P, Tchetche D, Iadanza A, Sardella G, Van Mieghem NM, Meliga E, Dumonteil N, Fraccaro C, Trabattoni D, Mikhail G, Sharma S, Ferrer MC, Naber C, Kievit P, Baber U, Snyder C, Sharma M, Morice MC, Mehran R, Investigators W-T. 1-Year Clinical Outcomes in Women After Transcatheter Aortic Valve Replacement: Results From the First WIN-TAVI Registry. JACC Cardiovasc Interv. 2018;11(1):1-12. Link, while SAVR has been associated with a greater risk of in-hospital adverse outcomes than in men, 58. Chaker Z, Badhwar V, Alqahtani F, Aljohani S, Zack CJ, Holmes DR, Rihal CS, Alkhouli M. Sex Differences in the Utilization and Outcomes of Surgical Aortic Valve Replacement for Severe Aortic Stenosis. J Am Heart Assoc. 2017;6(9). Link59. Wong SC, Yeo I, Bergman G, Feldman DN, Singh H, Minutello R, Kim LK. The Influence of Gender on In-Hospital Clinical Outcome Following Isolated Mitral or Aortic Heart Valve Surgery. Cardiovasc Revasc Med. 2019;20(6):468-474. Link. In a meta-analysis of four pivotal randomized clinical trials (PARTNER IA, US CoreValve High Risk, PARTNER II, and NOTION)60. Siontis GC, Praz F, Pilgrim T, Mavridis D, Verma S, Salanti G, Sondergaard L, Juni P, Windecker S. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of severe aortic stenosis: a meta-analysis of randomized trials. Eur Heart J. 2016;37(47):3503-3512. Link, there was a borderline significant interaction for sex (P=0.05), suggesting a mortality reduction in favour of TAVI compared to SAVR among women (hazard ratio [HR] 0.68, 95% confidence interval [CI] 0.50 to 0.91) but not men (HR 0.99, 95% CI 0.77 to 1.28). In contrast, a sub-study of the SURTAVI trial demonstrated that all-cause mortality or disabling stroke at 2 years was similar between TAVI and SAVR for both female (10.2% vs. 10.5%, P=0.90) and male patients (14.5% vs. 14.4%, P=0.99)61. Van Mieghem NM, Reardon MJ, Yakubov SJ, Heiser J, Merhi W, Windecker S, Makkar RR, Cheng W, Robbins M, Fail P, Feinberg E, 2nd, Stoler RC, Hebeler R, Serruys PW, Popma JJ. Clinical outcomes of TAVI or SAVR in men and women with aortic stenosis at intermediate operative risk: a post hoc analysis of the randomised SURTAVI trial. EuroIntervention. 2020;16(10):833-841. Link. Although there is conflicting evidence on sex differences on outcomes after TAVI and SAVR, female sex may be considered a factor favouring TAVI over SAVR particularly in surgical high-risk patients or those with expected prosthesis-patient mismatch.
Frailty
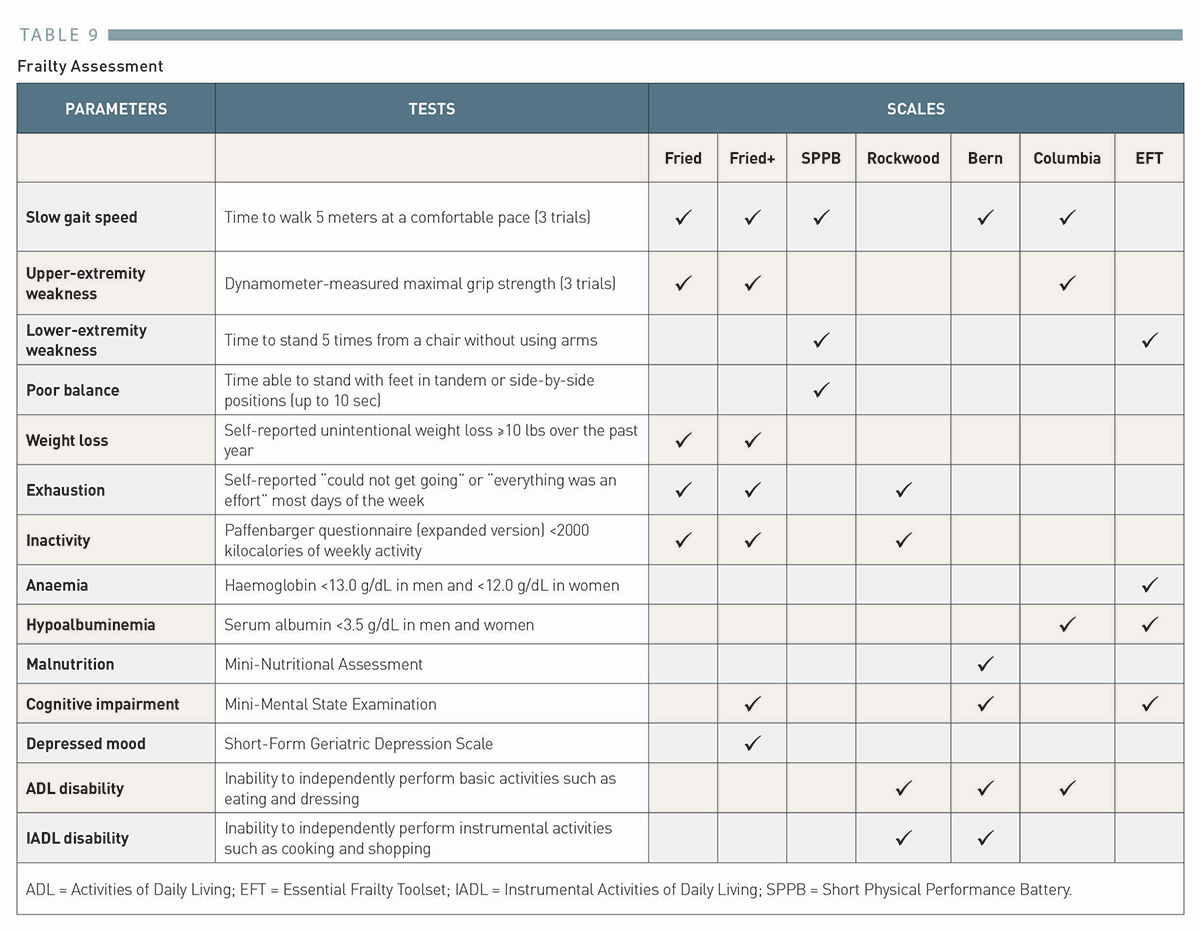
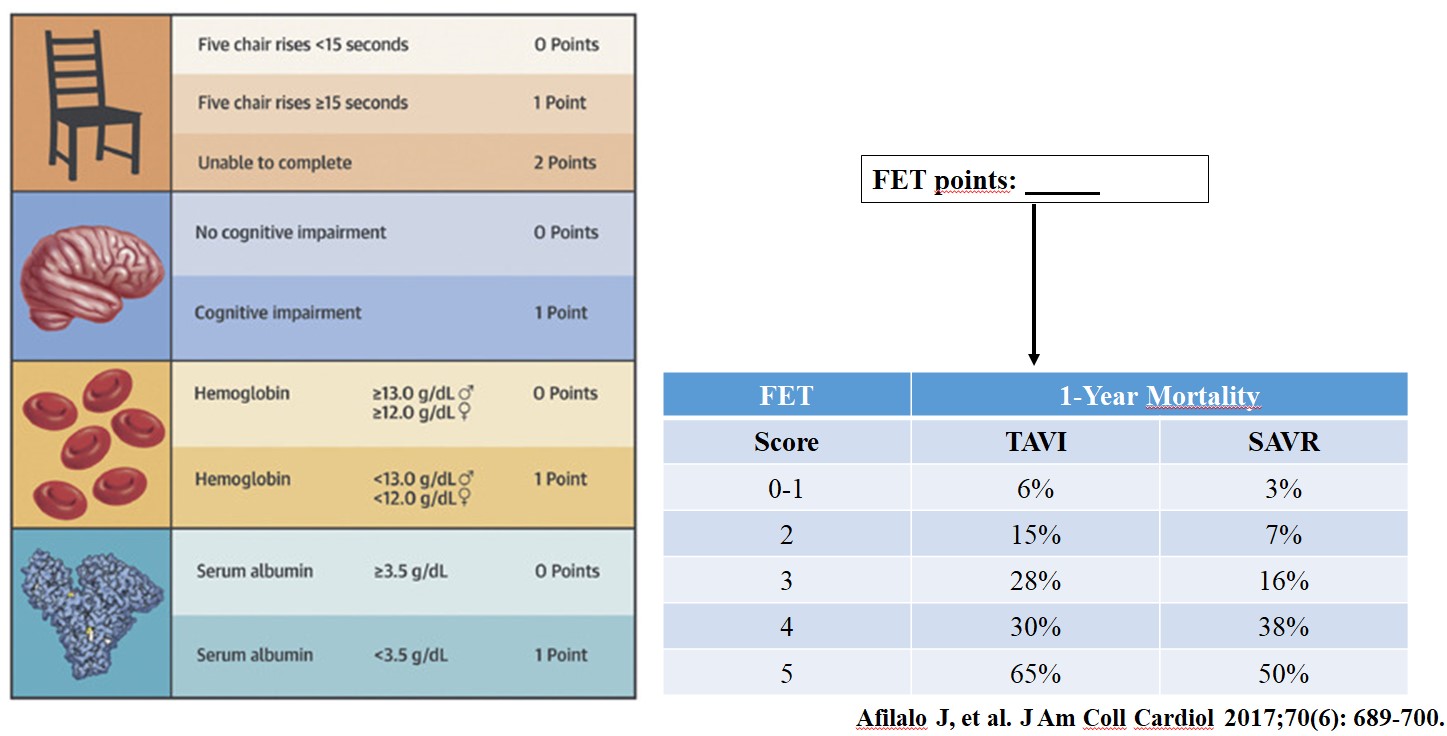
Frailty, a state of increased vulnerability resulting from aging-associated decline in reserve and function across multiple physiologic systems, is another important clinical factor that must be considered in the patient selection process24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. Despite variations in the assessment (Table 9), frailty has been consistently associated with an increased risk of morbidity, mortality, and functional decline after both TAVI and SAVR, , , , , 62. Sepehri A, Beggs T, Hassan A, Rigatto C, Shaw-Daigle C, Tangri N, Arora RC. The impact of frailty on outcomes after cardiac surgery: a systematic review. J Thorac Cardiovasc Surg. 2014;148(6):3110-7. Link63. Stortecky S, Schoenenberger AW, Moser A, Kalesan B, Juni P, Carrel T, Bischoff S, Schoenenberger CM, Stuck AE, Windecker S, Wenaweser P. Evaluation of multidimensional geriatric assessment as a predictor of mortality and cardiovascular events after transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2012;5(5):489-496. Link64. Green P, Arnold SV, Cohen DJ, Kirtane AJ, Kodali SK, Brown DL, Rihal CS, Xu K, Lei Y, Hawkey MC, Kim RJ, Alu MC, Leon MB, Mack MJ. Relation of frailty to outcomes after transcatheter aortic valve replacement (from the PARTNER trial). Am J Cardiol. 2015;116(2):264-9. Link65. Afilalo J, Lauck S, Kim DH, Lefevre T, Piazza N, Lachapelle K, Martucci G, Lamy A, Labinaz M, Peterson MD, Arora RC, Noiseux N, Rassi A, Palacios IF, Genereux P, Lindman BR, Asgar AW, Kim CA, Trnkus A, Morais JA, Langlois Y, Rudski LG, Morin JF, Popma JJ, Webb JG, Perrault LP. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol. 2017;70(6):689-700. Link66. Okuno T, Koseki K, Nakanishi T, Ninomiya K, Tomii D, Tanaka T, Sato Y, Osanai A, Sato K, Koike H, Yahagi K, Kishi S, Komiyama K, Aoki J, Yokozuka M, Miura S, Tanabe K. Prognostic Impact of Computed Tomography-Derived Abdominal Fat Area on Transcatheter Aortic Valve Implantation. Circ J. 2018;82(12):3082-3089. Link67. Okuno T, Koseki K, Nakanishi T, Sato K, Ninomiya K, Tomii D, Tanaka T, Sato Y, Horiuchi Y, Koike H, Yahagi K, Komiyama K, Tanaka J, Aoki J, Yokozuka M, Miura S, Tanabe K. Evaluation of objective nutritional indexes as predictors of one-year outcomes after transcatheter aortic valve implantation. J Cardiol. 2019;74(1):34-39. Link. In a prospective multinational cohort of elderly patients undergoing TAVI or SAVR (FRAILTY-AVR), multiple frailty scales (Fried68. Fried LP, Tangen CM, Walston J, Newman AB, Hirsch C, Gottdiener J, Seeman T, Tracy R, Kop WJ, Burke G, McBurnie MA, Cardiovascular Health Study Collaborative Research G. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56(3):M146-56. Link, Fried+69. Theou O, Cann L, Blodgett J, Wallace LM, Brothers TD, Rockwood K. Modifications to the frailty phenotype criteria: Systematic review of the current literature and investigation of 262 frailty phenotypes in the Survey of Health, Ageing, and Retirement in Europe. Ageing Res Rev. 2015;21:78-94. Link, Rockwood70. Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, Mitnitski A. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489-95. Link, Short Physical Performance Battery71. Guralnik JM, Simonsick EM, Ferrucci L, Glynn RJ, Berkman LF, Blazer DG, Scherr PA, Wallace RB. A short physical performance battery assessing lower extremity function: association with self-reported disability and prediction of mortality and nursing home admission. J Gerontol. 1994;49(2):M85-94. Link, Bern63. Stortecky S, Schoenenberger AW, Moser A, Kalesan B, Juni P, Carrel T, Bischoff S, Schoenenberger CM, Stuck AE, Windecker S, Wenaweser P. Evaluation of multidimensional geriatric assessment as a predictor of mortality and cardiovascular events after transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2012;5(5):489-496. Link, Columbia64. Green P, Arnold SV, Cohen DJ, Kirtane AJ, Kodali SK, Brown DL, Rihal CS, Xu K, Lei Y, Hawkey MC, Kim RJ, Alu MC, Leon MB, Mack MJ. Relation of frailty to outcomes after transcatheter aortic valve replacement (from the PARTNER trial). Am J Cardiol. 2015;116(2):264-9. Link, and the Essential Frailty Toolset65. Afilalo J, Lauck S, Kim DH, Lefevre T, Piazza N, Lachapelle K, Martucci G, Lamy A, Labinaz M, Peterson MD, Arora RC, Noiseux N, Rassi A, Palacios IF, Genereux P, Lindman BR, Asgar AW, Kim CA, Trnkus A, Morais JA, Langlois Y, Rudski LG, Morin JF, Popma JJ, Webb JG, Perrault LP. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol. 2017;70(6):689-700. Link) have been evaluated. In a cohort including 1,020 patients with a median age of 82 years, the prevalence of frailty ranged from 26% to 68% depending on the scale used, and frailty was associated with mortality and disability at 1 year. Furthermore, the Essential Frailty Toolset, integrating lower-extremity weakness, cognitive impairment, anaemia, and hypoalbuminemia, outperformed the other scales and was recommended for use in this setting65. Afilalo J, Lauck S, Kim DH, Lefevre T, Piazza N, Lachapelle K, Martucci G, Lamy A, Labinaz M, Peterson MD, Arora RC, Noiseux N, Rassi A, Palacios IF, Genereux P, Lindman BR, Asgar AW, Kim CA, Trnkus A, Morais JA, Langlois Y, Rudski LG, Morin JF, Popma JJ, Webb JG, Perrault LP. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol. 2017;70(6):689-700. Link (Figure 6). While the presence of frailty supports selection of TAVI in preference to SAVR, severely advanced frailty may suggest the futility of the intervention and favour conservative management rather than TAVI24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link.
The prevalence of coronary artery disease (CAD) in patients with severe AS ranges between 15% to 80%, depending on the definition of CAD used and the populations studied72. Faroux L, Guimaraes L, Wintzer-Wehekind J, Junquera L, Ferreira-Neto AN, Del Val D, Muntane-Carol G, Mohammadi S, Paradis JM, Rodes-Cabau J. Coronary Artery Disease and Transcatheter Aortic Valve Replacement: JACC State-of-the-Art Review. J Am Coll Cardiol. 2019;74(3):362-372. Link. Severe CAD has been associated with impaired mid- and long-term outcomes after TAVI73. Witberg G, Regev E, Chen S, Assali A, Barbash IM, Planer D, Vaknin-Assa H, Guetta V, Vukasinovic V, Orvin K, Danenberg HD, Segev A, Kornowski R. The Prognostic Effects of Coronary Disease Severity and Completeness of Revascularization on Mortality in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2017;10(14):1428-1435. Link. Thus, screening for CAD using contrast-enhanced coronary computed tomography (CT) or invasive coronary angiography74. Chieffo A, Giustino G, Spagnolo P, Panoulas VF, Montorfano M, Latib A, Figini F, Agricola E, Gerli C, Franco A, Giglio M, Cioni M, Alfieri O, Camici PG, Colombo A. Routine Screening of Coronary Artery Disease With Computed Tomographic Coronary Angiography in Place of Invasive Coronary Angiography in Patients Undergoing Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2015;8(7):e002025. Link, is mandatory before TAVI, 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link. In the presence of complex left main and/or multivessel disease with SYNTAX score >33, SAVR with concomitant coronary artery bypass grafting (CABG) should be favoured, 75. Mohr FW, Morice MC, Kappetein AP, Feldman TE, Stahle E, Colombo A, Mack MJ, Holmes DR, Jr., Morel MA, Van Dyck N, Houle VM, Dawkins KD, Serruys PW. Coronary artery bypass graft surgery versus percutaneous coronary intervention in patients with three-vessel disease and left main coronary disease: 5-year follow-up of the randomised, clinical SYNTAX trial. Lancet. 2013;381(9867):629-38. Link76. Thalji NM, Suri RM, Daly RC, Greason KL, Dearani JA, Stulak JM, Joyce LD, Burkhart HM, Pochettino A, Li Z, Frye RL, Schaff HV. The prognostic impact of concomitant coronary artery bypass grafting during aortic valve surgery: implications for revascularization in the transcatheter era. J Thorac Cardiovasc Surg. 2015;149(2):451-60. Link. Otherwise, percutaneous coronary intervention (PCI) before TAVI has been shown to be safe and feasible in observational studies, 77. Bajaj A, Pancholy S, Sethi A, Rathor P. Safety and feasibility of PCI in patients undergoing TAVR: A systematic review and meta-analysis. Heart Lung. 2017;46(2):92-99. Link78. Chakravarty T, Sharma R, Abramowitz Y, Kapadia S, Latib A, Jilaihawi H, Poddar KL, Giustino G, Ribeiro HB, Tchetche D, Monteil B, Testa L, Tarantini G, Facchin M, Lefevre T, Lindman BR, Hariri B, Patel J, Takahashi N, Matar G, Mirocha J, Cheng W, Tuzcu ME, Sievert H, Rodes-Cabau J, Colombo A, Finkelstein A, Fajadet J, Makkar RR. Outcomes in Patients With Transcatheter Aortic Valve Replacement and Left Main Stenting: The TAVR-LM Registry. J Am Coll Cardiol. 2016;67(8):951-960. Link, and is a reasonable strategy,24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link although the timing of PCI relative to TAVI remains controversial. Although it is generally believed that PCI should be performed prior to TAVI owing to the potential difficulties in coronary access especially in cases of self-expanding devices79. Ochiai T, Chakravarty T, Yoon SH, Kaewkes D, Flint N, Patel V, Mahani S, Tiwana R, Sekhon N, Nakamura M, Cheng W, Makkar R. Coronary Access After TAVR. JACC Cardiovasc Interv. 2020;13(6):693-705. Link, a strategy of PCI after TAVI may be preferred in case of complex coronary interventions (Figure 7).
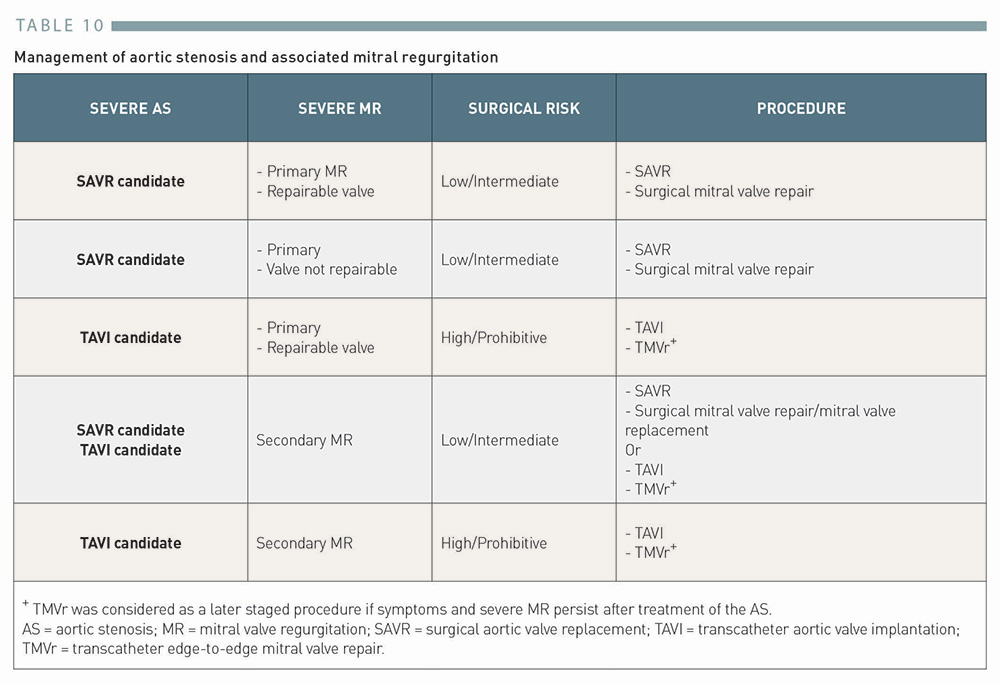
The presence of other associated valve lesions is an important consideration in the treatment decision, and should be carefully evaluated before the intervention80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link. Mitral regurgitation (MR) is the most common valve disease in patients undergoing TAVI, with a prevalence ranging between 10% to 40%80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link. In patients with combined AS and MR, increased LV pressure may exacerbate the mitral regurgitant volume, while decreased forward flow across the aortic valve may underestimate the severity of AS, 80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link81. Unger P, Pibarot P, Tribouilloy C, Lancellotti P, Maisano F, Iung B, Pierard L, European Society of Cardiology Council on Valvular Heart D. Multiple and Mixed Valvular Heart Diseases. Circ Cardiovasc Imaging. 2018;11(8):e007862. Link. Thus, the severity assessment of both lesions presents a particular diagnostic challenge and should be carefully made by echocardiography using a multiparametric approach. The optimal treatment strategy is challenging in this setting as there are many potential scenarios and nuances that may lead to different treatment options, , 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link (Table 10). In patients with severe AS and severe primary MR, SAVR and combined mitral valve surgery is reasonable unless the surgical risk is high or prohibitive24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. Secondary MR may improve after TAVI82. Vollenbroich R, Stortecky S, Praz F, Lanz J, Franzone A, Zuk K, Heg D, Valgimigli M, O’Sullivan CJ, Heinisch C, Roost E, Wenaweser P, Windecker S, Pilgrim T. The impact of functional vs degenerative mitral regurgitation on clinical outcomes among patients undergoing transcatheter aortic valve implantation. Am Heart J. 2017;184:71-80. Link. Otherwise, TAVI followed by transcatheter mitral valve edge-to-edge repair may be an option that should be discussed by the Heart team taking into account multiple factors24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link.
Table 10
Management of aortic stenosis and associated mitral regurgitation
Mixed AS and mitral stenosis (MS) is another challenging entity of diagnosis as the combination results in a greater reduction in cardiac output, leading to underestimation in the severity of both lesions80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link. Echocardiography and invasive haemodynamic measurements are usually necessary to assess the severity of each lesion adequately. In patients with severe AS and severe MS (mitral valve area ≤1.5 cm2), SAVR and combined mitral valve surgery should be considered unless the surgical risk is high or prohibitive24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. If the valve morphology is suitable for percutaneous mitral balloon commissurotomy (PMBC), TAVI combined with PMBC may also be a reasonable option. In case of a high or prohibitive surgical risk and unfavourable valve morphology for PMBC, decision-making is more challenging. Although transcatheter mitral valve replacement has recently evolved and may be an option, the data are limited at this moment and may require transapical access, 83. Sinning JM, Mellert F, Schiller W, Welz A, Nickenig G, Hammerstingl C. Transcatheter mitral valve replacement using a balloon-expandable prosthesis in a patient with calcified native mitral valve stenosis. Eur Heart J. 2013;34(33):2609. Link84. Ribeiro HB, Doyle D, Urena M, Allende R, Amat-Santos I, Pasian S, Bilodeau S, Mohammadi S, Paradis JM, DeLarochelliere R, Rodes-Cabau J, Dumont E. Transapical mitral implantation of a balloon-expandable valve in native mitral valve stenosis in a patient with previous transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2014;7(10):e137-9. Link.
Tricuspid regurgitation
Clinically relevant tricuspid regurgitation (TR) has been documented in 11% to 27% of patients undergoing TAVI80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link. While concomitant tricuspid valve surgery is indicated for progressive or severe TR when performing SAVR, there is currently no data or recommendation in the management of TR for TAVI patients24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. As both prospective and retrospective studies provide promising results of transcatheter devices for the treatment of secondary TR, 85. Nickenig G, Weber M, Lurz P, von Bardeleben RS, Sitges M, Sorajja P, Hausleiter J, Denti P, Trochu JN, Nabauer M, Dahou A, Hahn RT. Transcatheter edge-to-edge repair for reduction of tricuspid regurgitation: 6-month outcomes of the TRILUMINATE single-arm study. Lancet. 2019;394(10213):2002-2011. Link86. Taramasso M, Benfari G, van der Bijl P, Alessandrini H, Attinger-Toller A, Biasco L, Lurz P, Braun D, Brochet E, Connelly KA, de Bruijn S, Denti P, Deuschl F, Estevez-Loureiro R, Fam N, Frerker C, Gavazzoni M, Hausleiter J, Ho E, Juliard JM, Kaple R, Besler C, Kodali S, Kreidel F, Kuck KH, Latib A, Lauten A, Monivas V, Mehr M, Muntane-Carol G, Nazif T, Nickening G, Pedrazzini G, Philippon F, Pozzoli A, Praz F, Puri R, Rodes-Cabau J, Schafer U, Schofer J, Sievert H, Tang GHL, Thiele H, Topilsky Y, Rommel KP, Delgado V, Vahanian A, Von Bardeleben RS, Webb JG, Weber M, Windecker S, Winkel M, Zuber M, Leon MB, Hahn RT, Bax JJ, Enriquez-Sarano M, Maisano F. Transcatheter Versus Medical Treatment of Patients With Symptomatic Severe Tricuspid Regurgitation. J Am Coll Cardiol. 2019;74(24):2998-3008. Link, transcatheter tricuspid valve intervention after TAVI may be a reasonable option if the surgical risk is high or prohibitive. Of note, clinically relevant TR has been shown to improve in 15% to 60% after TAVI80. Khan F, Okuno T, Malebranche D, Lanz J, Praz F, Stortecky S, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13(13):1503-1514. Link.
Non-cardiac conditions
Non-cardiac conditions such as severe lung, liver, and renal disease, are important considerations in decision-making. In a systematic review and meta-analysis including 51,530 patients undergoing TAVI, chronic obstructive pulmonary disease (COPD) was present in 12% to 43% of patients, and was associated with an increased risk of mortality and treatment futility after TAVI87. Liao YB, He ZX, Zhao ZG, Wei X, Zuo ZL, Li YJ, Xiong TY, Xu YN, Feng Y, Chen M. The relationship between chronic obstructive pulmonary disease and transcatheter aortic valve implantation--A systematic review and meta-analysis. Catheter Cardiovasc Interv. 2016;87 Suppl 1:570-8. Link. When compared to SAVR, TAVI was associated with better in-hospital outcomes (mortality: 3.3% vs. 4.2%, P=0.035), lower health care cost ($56,099 vs. $63,146, P<0.001), and shorter hospital stay (mean, 7.7 vs. 13.0 days, P<0.001), in a propensity-matched cohort including >1,200 pairs from the Nationwide Inpatient Sample (NIH) database in the US88. Ando T, Adegbala O, Akintoye E, Ashraf S, Pahuja M, Briasoulis A, Takagi H, Grines CL, Afonso L, Schreiber T. Is Transcatheter Aortic Valve Replacement Better Than Surgical Aortic Valve Replacement in Patients With Chronic Obstructive Pulmonary Disease A Nationwide Inpatient Sample Analysis. J Am Heart Assoc. 2018;7(7). Link. Similarly, in a propensity-matched cohort including 268 patients with liver cirrhosis from the NIH database, TAVI, compared to SAVR was associated with lower in-hospital mortality (8.2% vs. 18.7%, P=0.018), shorter hospital stay (mean, 12 vs. 16 days, P=0.005), and fewer use of health care resources89. Alqahtani F, Aljohani S, Ghabra A, Alahdab F, Kawsara A, Holmes DR, Alkhouli M. Outcomes of Transcatheter Versus Surgical Aortic Valve Implantation for Aortic Stenosis in Patients With Hepatic Cirrhosis. Am J Cardiol. 2017;120(7):1193-1197. Link. In the NIH database, chronic kidney disease (CKD) and end-stage renal disease (ESDR) were present in 33.5% and 4.1%, respectively. Compared with patients without CKD, both CKD and ESRD were associated with higher in-hospital mortality (3.8% vs. 4.5% vs. 8.3%, adjusted odds ratio [OR] 1.39, 95% CI 1.24 to 1.55 for CKD, and adjusted OR 2.58, 95% CI 2.09 to 3.13 for ESRD) and a higher rate of major cardiovascular events, 90. Gupta T, Goel K, Kolte D, Khera S, Villablanca PA, Aronow WS, Bortnick AE, Slovut DP, Taub CC, Kizer JR, Pyo RT, Abbott JD, Fonarow GC, Rihal CS, Garcia MJ, Bhatt DL. Association of Chronic Kidney Disease With In-Hospital Outcomes of Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2017;10(20):2050-2060. Link91. Kumar N, Khera R, Garg N, Echouffo-Tcheugui JB, Venkatraman A, Pandey A, Bhatt DL. Comparison of Outcomes of Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Chronic Kidney Disease. Am J Cardiol. 2018;121(3):343-348. Link. In a sub-study of the CoreValve US Pivotal High Risk Trial, TAVI results in a lower rate of 3-year major adverse cardiovascular and renal events (a composite of all-cause mortality, myocardial infarction, cerebrovascular events, and new requirement of dialysis) compared with SAVR in patients with CKD (42.1% vs. 51.0%, P=0.04)92. Pineda AM, Kevin Harrison J, Kleiman NS, Reardon MJ, Conte JV, O’Hair DP, Chetcuti SJ, Huang J, Yakubov SJ, Popma JJ, Beohar N. Clinical impact of baseline chronic kidney disease in patients undergoing transcatheter or surgical aortic valve replacement. Catheter Cardiovasc Interv. 2019;93(4):740-748. Link. Although there is no randomized comparison of TAVI versus SAVR in these settings, the less invasive nature of TAVI is particularly attractive given the higher risk of peri-procedural complications in these patients. While the presence of non-cardiac comorbidities favours TAVI over SAVR, advanced stages of comorbidities or involvement of more than two organ systems may predict treatment futility of TAVI, and conservative management may also be considered in selected cases24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link.
Valve anatomy
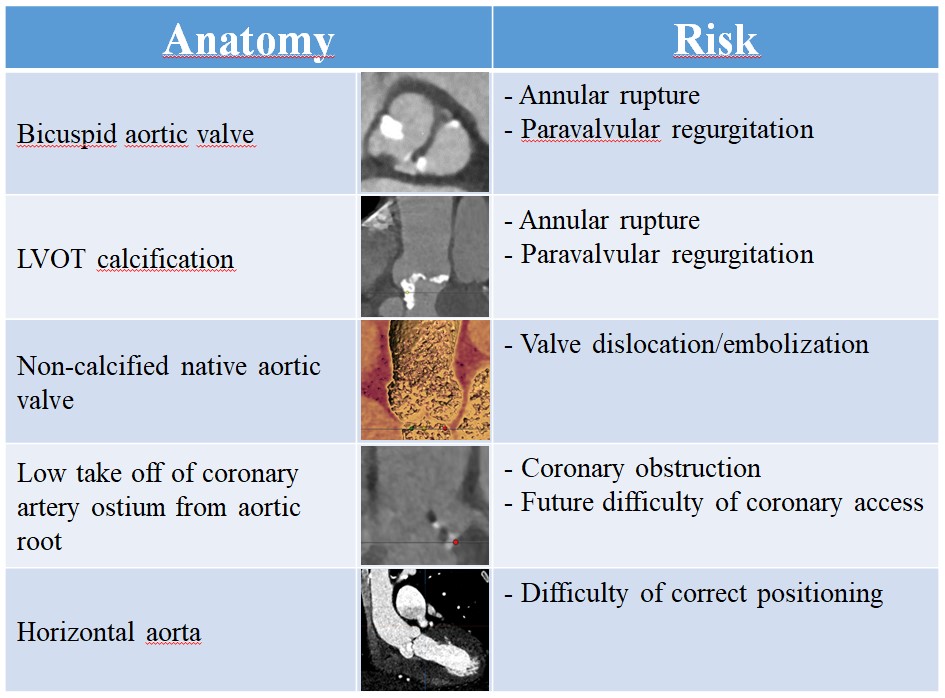
Valve anatomy as assessed on multi-detector computed tomography (MDCT), is of particular importance in patient selection for TAVI or SAVR. Typical anatomical risk factors for TAVI that must be meticulously evaluated before the procedure and their associated risks are listed in Figure 8. Bicuspid aortic valve (Figure 8) has important anatomical challenges such as presence of raphe, extent and location of calcification, and associated aortopathy. All pivotal RCTs excluded this patient population, and there is a paucity of data in terms of safety and efficacy of TAVI for bicuspid aortic valve. In an analysis of the STS/ACC TVT registry data including 2,691 propensity-matched pairs of bicuspid and tricuspid AS, patients with bicuspid aortic valve had a comparable mortality at 30 days (2.6% vs. 2.5%, P=0.82) and 1 year (10.5% vs. 12.0%, P=0.31) after TAVI using the SAPIEN 3 THV93. Makkar RR, Yoon SH, Leon MB, Chakravarty T, Rinaldi M, Shah PB, Skipper ER, Thourani VH, Babaliaros V, Cheng W, Trento A, Vemulapalli S, Kapadia SR, Kodali S, Mack MJ, Tang GHL, Kaneko T. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. JAMA. 2019;321(22):2193-2202. Link. The stroke rate was higher in patients with bicuspid AS at 30 days (2.5% vs. 1.6%, P=0.02), but the difference was not significant at 1 year (3.4% vs. 3.1%, P=0.16). There were no significant differences between groups in implant success (99.0% vs. 99.0%, P>0.99) or device success (96.5% vs. 96.6%, P=0.87); however, conversion to surgery (0.9% vs. 0.4%, P=0.03) and annular rupture (0.3% vs. 0%, P=0.02) occurred more frequently in patients with bicuspid AS. In a recent analysis based on a broader cohort (using any commercial devices) from the STS/ACC TVT registry including 5,412 bicuspid AS and 165,547 tricuspid AS94. Halim SA, Edwards FH, Dai D, Li Z, Mack MJ, Holmes DR, Tuzcu EM, Thourani VH, Harrison JK, Brennan JM. Outcomes of Transcatheter Aortic Valve Replacement in Patients With Bicuspid Aortic Valve Disease: A Report From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation. 2020;141(13):1071-1079. Link, a lower 1-year adjusted risk of mortality (HR 0.88, 95% CI 0.78 to 0.99) and comparable 1-year adjusted risk of stroke (HR 1.14, 95% CI 0.94 to 1.39) were observed for patients with bicuspid AS versus tricuspid AS. Device success was slightly lower in the bicuspid AS group (96.0% vs. 96.7%, P=0.004). Patients with bicuspid AS had higher incidences of moderate or greater paravalvular regurgitation (PVR) (4.7% vs. 3.5%, P<0.001) and second valve implantation (1.7% vs. 1.2%, P=0.002), and higher residual gradients (10 mmHg vs. 9 mmHg, P<0.001) than those with tricuspid AS. The use of current-generation devices for bicuspid AS was associated with a higher device success rate (96.3% vs. 93.5%, P=0.001) with a lower incidence of moderate or greater PVR (2.7% vs. 14.0%, P<0.001) in comparison with older-generation devices. A recent core laboratory CT analysis in a multinational registry (n=1,034) identified calcified raphe and excess leaflet calcification in bicuspid aortic valve as the risk factors for procedural complications and mid-term mortality after TAVI using current-generation devivecs95. Yoon SH, Kim WK, Dhoble A, Milhorini Pio S, Babaliaros V, Jilaihawi H, Pilgrim T, De Backer O, Bleiziffer S, Vincent F, Shmidt T, Butter C, Kamioka N, Eschenbach L, Renker M, Asami M, Lazkani M, Fujita B, Birs A, Barbanti M, Pershad A, Landes U, Oldemeyer B, Kitamura M, Oakley L, Ochiai T, Chakravarty T, Nakamura M, Ruile P, Deuschl F, Berman D, Modine T, Ensminger S, Kornowski R, Lange R, McCabe JM, Williams MR, Whisenant B, Delgado V, Windecker S, Van Belle E, Sondergaard L, Chevalier B, Mack M, Bax JJ, Leon MB, Makkar RR, Bicuspid Aortic Valve Stenosis Transcatheter Aortic Valve Replacement Registry I. Bicuspid Aortic Valve Morphology and Outcomes After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76(9):1018-1030. Link. The Evolut Low Risk Bicuspid Study (NCT03635424) is the first prospective study to examine the safety and efficacy of TAVI in patients with bicuspid AS. Early results recently reported were encouraging96. Waksman R, Craig PE, Torguson R, Asch FM, Weissman G, Ruiz D, Gordon P, Ehsan A, Parikh P, Bilfinger T, Levitt R, Hahn C, Roberts D, Ingram M, Hanna N, Comas G, Zhang C, Ben-Dor I, Satler LF, Garcia-Garcia HM, Shults C, Rogers T. Transcatheter Aortic Valve Replacement in Low-Risk Patients With Symptomatic Severe Bicuspid Aortic Valve Stenosis. JACC Cardiovasc Interv. 2020;13(9):1019-1027. Link.
Severely calcified aortic valve complex is another important anatomical feature that requires particular attention related to PVR and aortic root injury after TAVI97. Jilaihawi H, Makkar RR, Kashif M, Okuyama K, Chakravarty T, Shiota T, Friede G, Nakamura M, Doctor N, Rafique A, Shibayama K, Mihara H, Trento A, Cheng W, Friedman J, Berman D, Fontana GP. A revised methodology for aortic-valvar complex calcium quantification for transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2014;15(12):1324-32. Link. In particular, left ventricular outflow tract (LVOT) calcification has been singled out as the most important hostile anatomy for TAVI (Figure 8). In a retrospective analysis of a prospective TAVI registry including 1,635 patients, moderate or severe LVOT calcification conferred an increased risk of annular rupture when treated with balloon-expandable devices, and a higher incidence of PVR irrespective of valve type or generation98. Okuno T, Asami M, Heg D, Lanz J, Praz F, Hagemeyer D, Brugger N, Grani C, Huber A, Spirito A, Raber L, Stortecky S, Windecker S, Pilgrim T. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13(15):1789-1799. Link. When LVOT calcification is recognized on pre-procedural MDCT, its volume, extension and distribution, as well as shape should be evaluated. If the relevant risk for adverse events related to TAVI is deemed high, SAVR may be preferred if the surgical risk is acceptable.
Other important anatomic considerations include non-calcified aortic valve, low take off of coronary artery ostium from the aortic root, and extremely horizontal aorta (Figure 8). Non- calcified native aortic valves have been considered a risk factor for valve dislocation or embolization after TAVI due to the lack of calcification anchoring the prosthesis99. Van Mieghem NM, Schultz CJ, van der Boon RM, Nuis RJ, Tzikas A, Geleijnse ML, van Domburg RT, Serruys PW, de Jaegere PP. Incidence, timing, and predictors of valve dislodgment during TAVI with the Medtronic Corevalve System. Catheter Cardiovasc Interv. 2012;79(5):726-32. Link. Although recent observational studies suggest that both balloon-expandable and self-expanding devices can be safely implanted in patients with non-calcified aortic valves, 100. Xiong TY, Feng Y, Liao YB, Li YJ, Zhao ZG, Wei X, Xu YN, Wei JF, Peng Y, Piazza N, Mylotte D, Chen M. Transcatheter aortic valve replacement in patients with non-calcific aortic stenosis. EuroIntervention. 2018;13(15):e1756-e1763. Link101. Abramowitz Y, Jilaihawi H, Pibarot P, Chakravarty T, Kashif M, Kazuno Y, Maeno Y, Kawamori H, Mangat G, Friedman J, Cheng W, Makkar RR. Severe aortic stenosis with low aortic valve calcification: characteristics and outcome following transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2017;18(6):639-647. Link, attention should be paid especially when concomitant aortic regurgitation is present. Low take off of coronary artery ostium from the aortic root may predispose patients to the risk of coronary obstruction and future difficulty of coronary access, and should be carefully assessed in the decision between TAVI and SAVR, 79. Ochiai T, Chakravarty T, Yoon SH, Kaewkes D, Flint N, Patel V, Mahani S, Tiwana R, Sekhon N, Nakamura M, Cheng W, Makkar R. Coronary Access After TAVR. JACC Cardiovasc Interv. 2020;13(6):693-705. Link102. Ribeiro HB, Webb JG, Makkar RR, Cohen MG, Kapadia SR, Kodali S, Tamburino C, Barbanti M, Chakravarty T, Jilaihawi H, Paradis JM, de Brito FS, Jr, Canovas SJ, Cheema AN, de Jaegere PP, del Valle R, Chiam PT, Moreno R, Pradas G, Ruel M, Salgado-Fernandez J, Sarmento-Leite R, Toeg HD, Velianou JL, Zajarias A, Babaliaros V, Cura F, Dager AE, Manoharan G, Lerakis S, Pichard AD, Radhakrishnan S, Perin MA, Dumont E, Larose E, Pasian SG, Nombela-Franco L, Urena M, Tuzcu EM, Leon MB, Amat-Santos IJ, Leipsic J, Rodes-Cabau J. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. J Am Coll Cardiol. 2013;62(17):1552-62. Link. Preventative management of coronary obstruction when performing TAVI will be discussed in a later section. Extremely horizontal aorta poses a technical challenge to successful positioning and optimal deployment of a THV. Patients with aortic angulation >70° were excluded from clinical trials of self-expanding devices103. Abramowitz Y, Maeno Y, Chakravarty T, Kazuno Y, Takahashi N, Kawamori H, Mangat G, Cheng W, Jilaihawi H, Makkar RR. Aortic Angulation Attenuates Procedural Success Following Self-Expandable But Not Balloon-Expandable TAVR. JACC Cardiovasc Imaging. 2016;9(8):964-72. Link. In a retrospective analysis including 582 patients undergoing TAVI, increased aortic root angulation was associated with a lower device success rate in self-expanding devices (76.1% vs. 96.4%, P=0.002) but not in balloon-expandable devices (97.9% vs. 97.9%, P=0.97)103. Abramowitz Y, Maeno Y, Chakravarty T, Kazuno Y, Takahashi N, Kawamori H, Mangat G, Cheng W, Jilaihawi H, Makkar RR. Aortic Angulation Attenuates Procedural Success Following Self-Expandable But Not Balloon-Expandable TAVR. JACC Cardiovasc Imaging. 2016;9(8):964-72. Link.
In contrast, for patients at risk of prosthesis-patient mismatch, in whom the expected effective orifice area of the planned prosthesis is too small in relation to body size, TAVI may be favoured over SAVR. In a sub-analysis of PARTNER IA, the incidence of severe prosthesis-patient mismatch was 28.1% in the SAVR cohort versus 19.7% in the TAVI cohort (P<0.001)104. Pibarot P, Weissman NJ, Stewart WJ, Hahn RT, Lindman BR, McAndrew T, Kodali SK, Mack MJ, Thourani VH, Miller DC, Svensson LG, Herrmann HC, Smith CR, Rodes-Cabau J, Webb J, Lim S, Xu K, Hueter I, Douglas PS, Leon MB. Incidence and sequelae of prosthesis-patient mismatch in transcatheter versus surgical valve replacement in high-risk patients with severe aortic stenosis: a PARTNER trial cohort--a analysis. J Am Coll Cardiol. 2014;64(13):1323-34. Link. Similarly, in a sub-analysis of US CoreValve High Risk, severe prosthesis-patient mismatch occurred in 20.7% after SAVR and in 7.0% after TAVI (P<0.001)105. Zorn GL, 3rd, Little SH, Tadros P, Deeb GM, Gleason TG, Heiser J, Kleiman NS, Oh JK, Popma JJ, Adams D, Huang J, Reardon MJ. Prosthesis-patient mismatch in high-risk patients with severe aortic stenosis: A randomized trial of a self-expanding prosthesis. J Thorac Cardiovasc Surg. 2016;151(4):1014-22, 1023 e1-3. Link. The supra-annular design of some self-expanding THVs may be advantageous in terms of the risk of prosthesis-patient mismatch106. Okuno T, Khan F, Asami M, Praz F, Heg D, Winkel MG, Lanz J, Huber A, Grani C, Raber L, Stortecky S, Valgimigli M, Windecker S, Pilgrim T. Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement With Supra-Annular and Intra-Annular Prostheses. JACC Cardiovasc Interv. 2019. Link. The presence of porcelain aorta, coronary artery bypass grafts at risk of injury upon sternotomy, sequelae of chest radiation, and severe chest deformation or scoliosis are also suggested as anatomical factors favouring TAVI over SAVR.
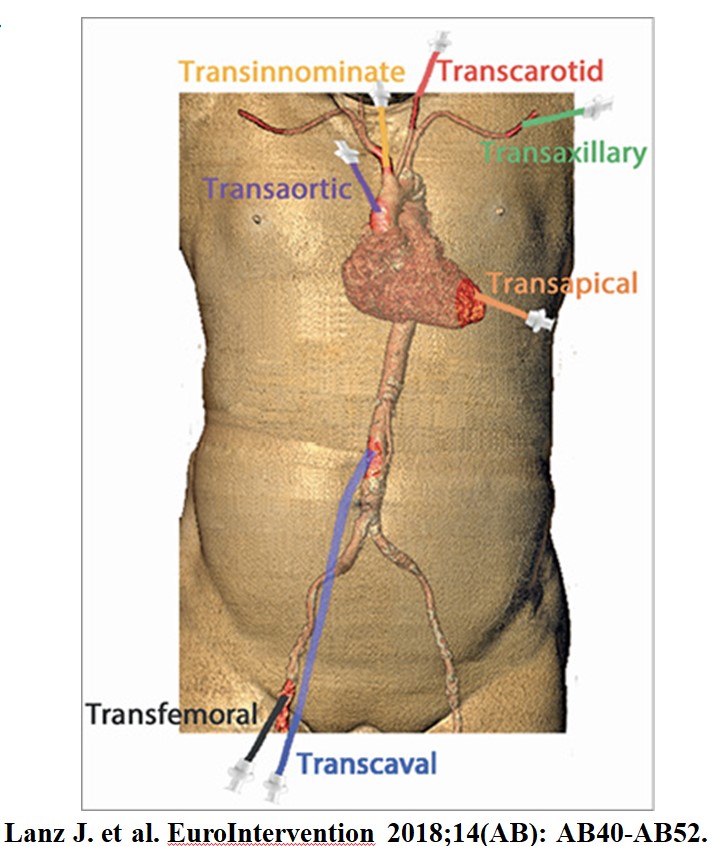
Vascular access
Vascular access must be carefully evaluated on pre-procedural MDCT in addition to the aforementioned valve anatomical considerations. Currently available THV sheaths and delivery systems have minimal luminal diameters depending on the platform ranging as low as 14 Fr requiring a minimal vessel diameter of 5.5 mm. Tortuosity and calcific burden of the artery may affect the suitability of the vascular access. In general, transfemoral access is considered the least invasive and the default strategy when performing TAVI. Although there are multiple alternative options such as transthoracic, transsubclavian/axillary, transcarotid, and transcaval access107. Lanz J, Greenbaum A, Pilgrim T, Tarantini G, Windecker S. Current state of alternative access for transcatheter aortic valve implantation. EuroIntervention. 2018;14(AB):AB40-AB52. Link(Figure 9), there are limited data from randomized trials comparing alternative access TAVI versus SAVR. Of note, the recent low risk trials predominantly enrolled patients who were eligible for transfemoral TAVI, 19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. Furthermore, in the transthoracic TAVI cohort of the PARTNER 2A trial, TAVI was inferior to SAVR in terms of death or disabling stroke at 5 years (59.3% vs. 48.3%, P=0.03)108. Makkar RR, Thourani VH, Mack MJ, Kodali SK, Kapadia S, Webb JG, Yoon SH, Trento A, Svensson LG, Herrmann HC, Szeto WY, Miller DC, Satler L, Cohen DJ, Dewey TM, Babaliaros V, Williams MR, Kereiakes DJ, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Brown DL, Fearon WF, Russo MJ, Pibarot P, Hahn RT, Jaber WA, Rogers E, Xu K, Wheeler J, Alu MC, Smith CR, Leon MB, Investigators P. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382(9):799-809. Link. Conversely, in a propensity-matched study of the national French TAVI registry (FRANCE TAVI), non-femoral peripheral TAVI, including transcarotid (n=914) and transsubclavian (n=702) access, was associated with similar outcomes compared with transfemoral TAVI (n=19,995), except for a 2-fold lower rate of major vascular complications (OR 0.45, 95% CI 0.21 to 0.93, P=0.032) and unplanned vascular repairs (OR 0.41, 95% CI 0.29 to 0.59, P<0.001). The authors concluded that non-femoral peripheral TAVI may be favoured over SAVR in patients who are deemed ineligible for transfemoral TAVI109. Beurtheret S, Karam N, Resseguier N, Houel R, Modine T, Folliguet T, Chamandi C, Com O, Gelisse R, Bille J, Joly P, Barra N, Tavildari A, Commeau P, Armero S, Pankert M, Pansieri M, Siame S, Koning R, Laskar M, Le Dolley Y, Maudiere A, Villette B, Khanoyan P, Seitz J, Blanchard D, Spaulding C, Lefevre T, Van Belle E, Gilard M, Eltchaninoff H, Iung B, Verhoye JP, Abi-Akar R, Achouh P, Cuisset T, Leprince P, Marijon E, Le Breton H, Lafont A. Femoral Versus Nonfemoral Peripheral Access for Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2019;74(22):2728-2739. Link.
In patients with aortic root dilation requiring surgical replacement or septal hypertrophy requiring myectomy, SAVR may be favoured over TAVI unless the surgical risk is high or prohibitive24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. In addition to the above mentioned considerations, patient preferences are of paramount importance and should be emphasized in the decision-making process.
The Heart Team
As discussed above, there are currently a wide variety of clinical scenarios and treatment strategies in patients with AS. Thus, the value of the multidisciplinary Heart team is increasingly important for the individual patient assessment and decision-making. The Heart team generally consists of cardiologists with expertise in the clinical evaluation of patients with valvular heart disease, multi-modality cardiac imaging specialists, interventional cardiologists with expertise in transcatheter valvular interventions, and surgeons experienced in valve surgery. Other team members may include cardiovascular nurses, cardiovascular anaesthesiologists, and intensivists involved in peri-procedural care. The involvement of the primary care clinician who is familiar with the wishes, values and expectations of the patient and patient him-/her-self are also of critical importance. Current guidelines allocate a class I recommendation for the evaluation by the multidisciplinary Heart team in patients with severe valvular heart disease, 24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link110. Baumgartner H, Hung J, Bermejo J, Chambers JB, Edvardsen T, Goldstein S, Lancellotti P, LeFevre M, Miller F, Jr., Otto CM. Recommendations on the Echocardiographic Assessment of Aortic Valve Stenosis: A Focused Update from the European Association of Cardiovascular Imaging and the American Society of Echocardiography. J Am Soc Echocardiogr. 2017;30(4):372-392. Link.
TAVI procedure
Pre-procedural planning
Pre-procedural planning is of critical importance when considering TAVI. The multidisciplinary Heart team plays a pivotal role in integrating the patient clinical factors and anatomical factors obtained by MDCT, echocardiography, and cardiac catheterization to determine the best procedural strategy. As there are multiple device options in this field (Figure 10 and Figure 11), the Heart team needs to be familiar with the strengths and limitations of each device111. Claessen BE, Tang GHL, Kini AS, Sharma SK. Considerations for Optimal Device Selection in Transcatheter Aortic Valve Replacement: A Review. JAMA Cardiol. 2021;6(1):102-112. Link. In brief, balloon-expandable devices are superior in terms of PVR and ease of implantation, supra-annular self-expanding devices are superior in terms of haemodynamic transvalvular gradients, prosthesis-patient mismatch and risk of annular rupture106. Okuno T, Khan F, Asami M, Praz F, Heg D, Winkel MG, Lanz J, Huber A, Grani C, Raber L, Stortecky S, Valgimigli M, Windecker S, Pilgrim T. Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement With Supra-Annular and Intra-Annular Prostheses. JACC Cardiovasc Interv. 2019. Link. A more detailed description of the available evidence for the device comparison will be provided in a later section. Device sizing should also be discussed based on the manufacturers’ sizing recommendations and MDCT-derived annulus size. In case of borderline annulus size, the sizing decision may result in oversizing or undersizing depending on the degree of calcification, and the size of the sinus of Valsalva, the ascending aorta, and the LVOT 112. Okuno T, Heg D, Lanz J, Praz F, Gräni C, Langhammer B, Reineke D, Räber L, Wenaweser P, Pilgrim T, Windecker S, Stortecky S. Heart valve sizing and clinical outcomes in patients undergoing transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2021[Online ahead of print.] Link. While transfemoral access is the default strategy, alternative access may be considered in patients with unfavourable femoral access. The selection of the alternative access is determined by patients’ anatomic features and comorbidities as well as local experience.
Preventative strategies and management of potential complications should also be discussed by the Heart team before the procedure. If patients are deemed at high risk of coronary obstruction, coronary protection with guidewires and an undeployed balloon or stent positioned in the coronary artery may be considered113. Abramowitz Y, Chakravarty T, Jilaihawi H, Kashif M, Kazuno Y, Takahashi N, Maeno Y, Nakamura M, Cheng W, Makkar RR. Clinical impact of coronary protection during transcatheter aortic valve implantation: first reported series of patients. EuroIntervention. 2015;11(5):572-81. Link. If coronary occlusion occurs, the stent can be pulled back and deployed in a “chimney” fashion to maintain coronary patency (Figure 12)114. Mercanti F, Rosseel L, Neylon A, Bagur R, Sinning JM, Nickenig G, Grube E, Hildick-Smith D, Tavano D, Wolf A, Colonna G, Latib A, Mitomo S, Petronio AS, Angelillis M, Tchetche D, De Biase C, Adamo M, Nejjari M, Digne F, Schafer U, Amabile N, Achkouty G, Makkar RR, Yoon SH, Finkelstein A, Dvir D, Jones T, Chevalier B, Lefevre T, Piazza N, Mylotte D. Chimney Stenting for Coronary Occlusion During TAVR: Insights From the Chimney Registry. JACC Cardiovasc Interv. 2020;13(6):751-761. Link. Recently, BASILICA (Bioprosthetic or native Aortic Scallop Intentional Laceration to Prevent Iatrogenic Coronary Artery Obstruction) has been proposed as an alternative strategy to prevent coronary obstruction115. Khan JM, Greenbaum AB, Babaliaros VC, Rogers T, Eng MH, Paone G, Leshnower BG, Reisman M, Satler L, Waksman R, Chen MY, Stine AM, Tian X, Dvir D, Lederman RJ. The BASILICA Trial: Prospective Multicenter Investigation of Intentional Leaflet Laceration to Prevent TAVR Coronary Obstruction. JACC Cardiovasc Interv. 2019;12(13):1240-1252. Link(Figure 12). In brief, an electrified guidewire is used to lacerate the aortic valve leaflet that would otherwise obstruct a coronary ostium to preserve coronary inflow. While this technique is usually employed for valve-in-valve procedures, it may also be considered for native valve anatomy. Of note, it does not resolve the risk of coronary obstruction in all cases, particularly when the valve frame of the THV obstructs the coronary artery ostia by sequestering the sinus of Valsalva. For the prevention of cerebrovascular events, cerebral embolic protection devices, filters designed to capture or deflect emboli to the brain may be considered (Figure 13). Although randomized clinical trials have not been powered to demonstrate efficacy116. Kapadia SR, Kodali S, Makkar R, Mehran R, Lazar RM, Zivadinov R, Dwyer MG, Jilaihawi H, Virmani R, Anwaruddin S, Thourani VH, Nazif T, Mangner N, Woitek F, Krishnaswamy A, Mick S, Chakravarty T, Nakamura M, McCabe JM, Satler L, Zajarias A, Szeto WY, Svensson L, Alu MC, White RM, Kraemer C, Parhizgar A, Leon MB, Linke A, Investigators ST. Protection Against Cerebral Embolism During Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2017;69(4):367-377. Link, a recent meta-analysis showed a reduced 30-day stroke rate (OR 0.55, 95% CI 0.31-0.98) in patients treated with these devices117. Testa L, Latib A, Casenghi M, Gorla R, Colombo A, Bedogni F. Cerebral Protection During Transcatheter Aortic Valve Implantation: An Updated Systematic Review and Meta-Analysis. J Am Heart Assoc. 2018;7(10). Link. More recently, a patient level pooled analysis showed a significantly lower incidence of procedural stroke (1.88% vs. 5.44%, P=0.003) in patients treated with the devices118. Seeger J, Kapadia SR, Kodali S, Linke A, Wohrle J, Haussig S, Makkar R, Mehran R, Rottbauer W, Leon M. Rate of peri-procedural stroke observed with cerebral embolic protection during transcatheter aortic valve replacement: a patient-level propensity-matched analysis. Eur Heart J. 2019;40(17):1334-1340. Link.
The TAVI procedure can be done in a hybrid operating room or cardiac catheterization laboratory under general anaesthesia or local anaesthesia with or without conscious sedation. As the learning curve of the TAVI procedure continues to improve in addition to the expansion to lower risk patient populations, an increased number of procedures are being performed under local anaesthesia with or without conscious sedation. General anaesthesia is typically reserved for non-femoral access TAVI or anticipated complex procedures. In a randomized clinical trial comparing local anaesthesia with conscious sedation versus general anaesthesia in patients undergoing TAVI (SOLVE-TAVI), local anaesthesia with conscious sedation resulted in lower rates of catecholamine utilization (62.8% vs. 97.3%, P<0.001) but the primary composite endpoint of all-cause death, stroke, myocardial infarction, infection requiring antibiotic treatment, and acute kidney injury at 30 days was similar between both groups (27.2% vs. 26.4%, P for equivalence = 0.015)119. Thiele H, Kurz T, Feistritzer HJ, Stachel G, Hartung P, Lurz P, Eitel I, Marquetand C, Nef H, Doerr O, Vigelius-Rauch U, Lauten A, Landmesser U, Treskatsch S, Abdel-Wahab M, Sandri M, Holzhey D, Borger M, Ender J, Ince H, Oner A, Meyer-Saraei R, Hambrecht R, Fach A, Augenstein T, Frey N, Konig IR, Vonthein R, Ruckert Y, Funkat AK, Desch S, Berggreen AE, Heringlake M, de Waha-Thiele S, Investigators S-T. General Versus Local Anesthesia With Conscious Sedation in Transcatheter Aortic Valve Implantation: The Randomized SOLVE-TAVI Trial. Circulation. 2020;142(15):1437-1447. Link.
Antithrombotic Therapy
There are limited data to guide the antithrombotic management before and during TAVI. Typically, pre-procedural loading with low-dose aspirin is used and procedural anticoagulation is achieved with administration of unfractionated heparin maintaining an activated clotting time (ACT) of 250-300 seconds. Bivalirudin may be used alternatively in patients with a history of heparin-induced thrombocytopenia. In a randomized trial comparing bivalirudin and heparin as the procedural anticoagulant agent in patients undergoing transfemoral TAVI120. Dangas GD, Lefevre T, Kupatt C, Tchetche D, Schafer U, Dumonteil N, Webb JG, Colombo A, Windecker S, Ten Berg JM, Hildick-Smith D, Mehran R, Boekstegers P, Linke A, Tron C, Van Belle E, Asgar AW, Fach A, Jeger R, Sardella G, Hink HU, Husser O, Grube E, Deliargyris EN, Lechthaler I, Bernstein D, Wijngaard P, Anthopoulos P, Hengstenberg C, Investigators B-. Bivalirudin Versus Heparin Anticoagulation in Transcatheter Aortic Valve Replacement: The Randomized BRAVO-3 Trial. J Am Coll Cardiol. 2015;66(25):2860-2868. Link, anticoagulation with bivalirudin did not meet superiority criteria for major bleeding at 48 hours (6.9% vs. 9.0%, P=0.27), but was found non-inferior in terms of net adverse cardiovascular events including all-cause death, myocardial infarction, or stroke at 30 days (14.4% vs. 16.1%, P for noninferiority <0.01). For patients on oral anticoagulation (OAC), the decision to continue OAC during the procedure should be made individually based on patients’ bleeding/thromboembolic risks. In a recent retrospective multicentre European study, continuation of OAC throughout the procedure did not increase bleeding (11.3% vs. 14.3%, P=0.39) or vascular complication rates (11.0% vs. 12.3%, P=0.52) compared with interruption of OAC. In this study, the international normalized ratio (INR) on the day of TAVI was targeted to be 2.0 to 2.5, except for patients with mechanical valves for whom a target INR of up to 3.5 was accepted, for patients with continuation of vitamin K antagonists (VKA). Direct oral anticoagulants (DOACs) were omitted the morning of the procedure. During the procedure, intravenous heparin was used targeting an ACT of 250-300 seconds121. Brinkert M, Mangner N, Moriyama N, Keller LS, Hagemeyer D, Crusius L, Lehnick D, Kobza R, Abdel-Wahab M, Laine M, Stortecky S, Pilgrim T, Nietlispach F, Ruschitzka F, Thiele H, Linke A, Toggweiler S. Safety and Efficacy of Transcatheter Aortic Valve Replacement With Continuation of Vitamin K Antagonists or Direct Oral Anticoagulants. JACC Cardiovasc Interv. 2021;14(2):135-144. Link.
Antibiotic prophylaxis
Current guidelines for the management of infective endocarditis recommend the administration of perioperative antibiotic prophylaxis covering the most frequent microorganisms underlying early prosthetic valve infections after surgery (coagulase-negative staphylococci and Staphylococcus aureus)122. Habib G, Lancellotti P, Antunes MJ, Bongiorni MG, Casalta JP, Del Zotti F, Dulgheru R, El Khoury G, Erba PA, Iung B, Miro JM, Mulder BJ, Plonska-Gosciniak E, Price S, Roos-Hesselink J, Snygg-Martin U, Thuny F, Tornos Mas P, Vilacosta I, Zamorano JL, Group ESCSD. 2015 ESC Guidelines for the management of infective endocarditis: The Task Force for the Management of Infective Endocarditis of the European Society of Cardiology (ESC). Endorsed by: European Association for Cardio-Thoracic Surgery (EACTS), the European Association of Nuclear Medicine (EANM). Eur Heart J. 2015;36(44):3075-3128. Link. However, in a recent dedicated analysis from the SWISS TAVI registry123. Stortecky S, Heg D, Tueller D, Pilgrim T, Muller O, Noble S, Jeger R, Toggweiler S, Ferrari E, Taramasso M, Maisano F, Hoeller R, Wenaweser P, Nietlispach F, Widmer A, Huber C, Roffi M, Carrel T, Windecker S, Conen A. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;75(24):3020-3030. Link, antimicrobial susceptibility testing showed that 47.9% of patients with early peri-procedural prosthetic valve endocarditis had a pathogen that was not susceptible to the default antibiotic prophylaxis. This was mainly due to an increased rate of enterococcal infections during the peri-procedural period, that are not typically covered by first- or second-generation cephalosporins. An intravenous dose of amoxicillin/clavulanic acid, ampicillin/sulbactam, or vancomycin (for patients allergic to penicillin) were suggested as reasonable options.
Procedural Steps (Transfemoral TAVI)
1. Femoral main access (for delivery of a THV) and contra-lateral access (for aortic root angiography to guide implantation of a THV) are first obtained. Ultrasound-guided needle puncture is recommended to ensure the puncture site is in the common femoral segment over the femoral head avoiding the femoral bifurcation and in a segment free of significant calcification124. Vincent F, Spillemaeker H, Kyheng M, Belin-Vincent C, Delhaye C, Pierache A, Denimal T, Verdier B, Debry N, Moussa M, Schurtz G, Porouchani S, Cosenza A, Juthier F, Pamart T, Richardson M, Coisne A, Hertault A, Sobocinski J, Modine T, Pontana F, Duhamel A, Labreuche J, Van Belle E. Ultrasound Guidance to Reduce Vascular and Bleeding Complications of Percutaneous Transfemoral Transcatheter Aortic Valve Replacement: A Propensity Score-Matched Comparison. J Am Heart Assoc. 2020;9(6):e014916. Link. Alternative secondary access from the radial artery is preferred by some practitioners although it may preclude cerebral protection with some devices125. Fernandez-Lopez L, Chevalier B, Lefevre T, Spaziano M, Unterseeh T, Champagne S, Benamer H, Sanguineti F, Garot P, Hovasse T. Implementation of the transradial approach as an alternative vascular access for transcatheter aortic valve replacement guidance: Experience from a high-volume center. Catheter Cardiovasc Interv. 2019;93(7):1367-1373. Link
2. The main access site is pre-closed typically by using one or two suture-based vascular closure devices (ProGlide, Abbott, Abbott Park, Illinois) (Figure 14). Alternative closure devices such as plug-based vascular closure device (MANTA, Teleflex, Wayne, Pennsylvania) may also be utilized (Figure 14). In a randomized clinical trial, there was no significant difference in the access site-related vascular complications between MANTA and ProGlide (10% vs. 4%, P=0.16). ProGlide required more often additional closure devices, whereas MANTA numerically required more covered stents and surgical bailouts126. van Wiechen MP, Tchetche D, Ooms JF, Hokken TW, Kroon H, Ziviello F, Ghattas A, Siddiqui S, Laperche C, Spitzer E, Daemen J, de Jaegere PP, Dumonteil N, Van Mieghem NM. Suture- or Plug-Based Large-Bore Arteriotomy Closure: A Pilot Randomized Controlled Trial. JACC Cardiovasc Interv. 2021;14(2):149-157. Link.
3. The TAVI delivery sheath (14-18 Fr) is inserted into the main access site using a stiff guidewire providing support and straightening iliofemoral tortuosity. Balloon angioplasty or intravascular lithotripsy may be used to facilitate sheath insertion in patients with extensive iliofemoral vascular disease with stenosis and/or calcification127. Di Mario C, Goodwin M, Ristalli F, Ravani M, Meucci F, Stolcova M, Sardella G, Salvi N, Bedogni F, Berti S, Babaliaros VC, Pop A, Caparrelli D, Stewart J, Devireddy C. A Prospective Registry of Intravascular Lithotripsy-Enabled Vascular Access for Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12(5):502-504. Link.
4. Ultrasound-guided venous access, which can either be at the internal jugular or femoral veins, is obtained for insertion of the temporary pacemaker and central venous access if needed. Conventionally, a temporary pacemaker is introduced via the jugular or femoral venous system although some centres are adopting the LV pacing approach where the LV wire is used for temporary pacing thus eliminating the need for a separate puncture and theoretically reducing the associated risk of pericardial effusion. In a randomized clinical trial128. Faurie B, Souteyrand G, Staat P, Godin M, Caussin C, Van Belle E, Mangin L, Meyer P, Dumonteil N, Abdellaoui M, Monsegu J, Durand-Zaleski I, Lefevre T, Investigators ET. Left Ventricular Rapid Pacing Via the Valve Delivery Guidewire in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12(24):2449-2459. Link, LV pacing was associated with significantly reduced procedure duration (48.4 ± 16.9 min vs. 55.6 ± 26.9 min, P=0.0013), while maintaining similar efficacy and safety compared with RV pacing. Effective stimulation, defined as achievement and maintenance of a systolic blood pressure ≤60 mmHg for more than 30 seconds without loss-of-capture was similar in both groups (84.9 vs. 87.1%, P=0.60). Procedural success was achieved at similar rates (100% vs. 99.3%, P=0.99), with comparable risks of major adverse cardiovascular events including all-cause death, major cerebrovascular events, myocardial infarction, cardiac tamponade, bleeding events, and vascular complications (13.9% vs. 17.1%, P=0.44).
5. The 3-cusp coplanar angle for valve implantation is derived from MDCT and confirmed using aortic root angiography. The nadirs of the three aortic cusps should lie along a single line in this implantation angle. For self-expanding THV implantation, the cusp-overlap view overlapping the right coronary cusp and left coronary cusp may be alternatively used129. Tang GHL, Zaid S, Michev I, Ahmad H, Kaple R, Undemir C, Cohen M, Lansman SL. Cusp-Overlap View Simplifies Fluoroscopy-Guided Implantation of Self-Expanding Valve in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2018;11(16):1663-1665. Link (Figure 15).
6. Using an Amplatz left (AL 1) catheter and a standard straight-tipped wire (hydrophilic or metallic), the aortic valve is crossed. Alternative catheters such as an internal mammary or Judkins right can be used depending on the horizontal orientation of the aortic root. Once the wire is across the valve, the catheter is carefully advanced into the LV and the straight-tipped wire is removed for an exchange length J-shaped wire.
7. A pigtail catheter is placed in exchange for the catheter in the LV and directed towards the LV apex. At this time, simultaneous pressure assessment in the LV and aorta allow for measurement and recording of the transvalvular gradient.
8. Subsequently, a pre-shaped stiff wire is inserted into the LV through the pigtail catheter. Careful attention should be paid to avoid entrapment of the pigtail catheter or wire in the sub-valvular mitral valve apparatus which is typically facilitated by using a RAO fluoroscopic projection.
9. THV is checked for appropriate crimping and loading onto the delivery catheter as well as correct orientation. Crimping, loading, and verification of orientation for each valve platform can be found in the appropriate instructions for use.
10. In cases of very severe and calcified stenosis, pre-dilation may be undertaken under rapid pacing (at rates 160 to 200 bpm for up to 20-30 seconds) to facilitate the THV delivery. The size of the balloon should not exceed the minimum aortic annulus diameter obtained from MDCT. Of note, the efficacy of pre-dilation has been unclear in a randomized comparison of the implantation of a self-expanding THV with or without pre-dilation (N=171). Although pre-dilation was associated with a lower post-dilation rate (15.1% vs. 29.4%, P=0.03), device success rate was similar between the groups (74.4% vs. 76.5%; mean difference 2.1%; 90% CI -8.9% to 13%)130. Toutouzas K, Benetos G, Voudris V, Drakopoulou M, Stathogiannis K, Latsios G, Synetos A, Antonopoulos A, Kosmas E, Iakovou I, Katsimagklis G, Mastrokostopoulos A, Moraitis S, Zeniou V, Danenberg H, Vavuranakis M, Tousoulis D. Pre-Dilatation Versus No Pre-Dilatation for Implantation of a Self-Expanding Valve in All Comers Undergoing TAVR: The DIRECT Trial. JACC Cardiovasc Interv. 2019;12(8):767-777. Link.
11. Under fluoroscopic guidance, the THV is delivered over the stiff pre-shaped wire with careful attention to the wire position in the LV apex. The system is carefully advanced across the aortic arch avoiding direct interaction with aortic wall by appropriate deflection and/or rotation of the assembly.
12. Once the TAVI system has passed the aortic arch, the fluoroscopic angle is changed to the 3-cusp coplanar view or the cusp-overlap view (typically for self-expanding devices). Subsequently, the THV is carefully advanced across the aortic valve using a pigtail catheter placed in the non-coronary (or right coronary) cusp for reference. Aortic root angiography is then performed to confirm appropriate position.
13. The THV deployment technique is device specific as follows:
Valve alignment needs to be performed in a straight section of the aorta. Once the THV has passed the aortic valve, disengage the balloon lock and retract the tip of the Flex Catheter to the centre of the triple marker, and engage the balloon lock again. Utilize the Flex wheel to adjust the co-axiality of the THV and the fine adjustment wheel to correct the position of the THV across the valve. Before deployment, ensure that the THV is accurately positioned between the alignment markers and the Flex Catheter tip is over the triple marker. Under rapid pacing (to decrease systolic pressure to 50 mmHg or below), deployment is performed with slow controlled inflation until the complete predetermined volume within the indeflator has been administered and maintained for 3 seconds. When the balloon catheter has been completely deflated, turn off the pacemaker and remove the delivery system. Conventionally, the implantation depth is aimed in a ratio of valve frame in the aorta to LVOT of 70:30 or 80:20. Recently, a high deployment technique (HDT) has been proposed to achieve even higher implantation of the THV. This technique has three unique features: (1) The THV is deployed in the right anterior oblique/caudal view, with exact angulation determined by removing the parallax after advancing the crimped valve across the aortic valve; (2) The THV is positioned by aligning the radiolucent line that is located at the superior aspect of the lowest set of stent struts of the crimped valve at the base of the non-coronary cusp; and (3) a straight flush catheter, instead of a pigtail catheter, is positioned at the base of the non-coronary cusp and left in place after the deployment aortogram to confirm valve stent coverage of the inferior-most point of the aortic sinus. In a single center observational study including 622 conventional deployments and 406 HDTs131. Sammour Y, Banerjee K, Kumar A, Lak H, Chawla S, Incognito C, Patel J, Kaur M, Abdelfattah O, Svensson LG, Tuzcu EM, Reed GW, Puri R, Yun J, Krishnaswamy A, Kapadia S. Systematic Approach to High Implantation of SAPIEN-3 Valve Achieves a Lower Rate of Conduction Abnormalities Including Pacemaker Implantation. Circ Cardiovasc Interv. 2021;14(1):e009407. Link, mean implantation depth was significantly smaller with HDT than the conventional technique (1.5 ± 1.6 mm vs. 3.2 ± 1.9mm, P<0.001), which translated into lower rates of new permanent pacemaker implantation (PPI: 5.5% vs. 13.1%, P<0.001) and new onset left bundle branch block (LBBB: 5.3% vs. 12.2%, P<0.001) at 30 days. Only one patient (0.2%) had valve embolization with HDT. There was no differences in mild (16.5% vs. 15.9%, P=0.804), or ≥moderate PVR (1% vs. 2.7%, P=0.081) between both groups at 1 year.
Once the THV is brought into appropriate implanting position (targeting an implant depth of 3-5 mm or higher), deployment (unsheathing) is performed by rotating the deployment knob in the direction of the arrows. Frequently, during the deployment, controlled pacing (90 to 120 bpm) is applied to increase the valve stability. Periodic aortic root injections guide adequate positioning during placement. Once blood pressure drops due to temporal occlusion of the aortic valve by the THV, the operator must continue to turn the deployment wheel until blood pressure recovers. There is a tactile indicator that provides feedback to indicate that the capsule is nearing the “point of no recapture” (at approximately 2/3 deployed). At this point, the imaging projection should be adjusted to remove the parallax in valve inflow to determine valve position using aortic root angiography. If the operators are satisfied with the valve position and performance (aiming at no more than 2-4 mm extension into LVOT), the THV is fully released. The detachment of frame paddles must be confirmed under fluoroscopy, and the nose cone centred before the delivery system is withdrawn.
Portico (Abbott, Abbott Park, Illinois) Figure 18:
Once the THV is advanced across the aortic valve, position the delivery system so that the inner shaft marker band is aligned with the annular plane. Deployment (unsheathing) is then initiated by turning the deployment wheel in the direction of the arrow on the handle, typically under controlled pacing (90 to 120 bpm). There is a clicking sound when the delivery system has reached the partial deployment lock. The deployment mechanism will not re-engage until the deployment lock button is depressed. At this point, the imaging projection should be adjusted to remove the parallax in valve inflow and then confirm the valve positioning using aortic root angiography. If the appropriate positioning is confirmed, complete valve deployment by pressing the deployment lock button, then turning the deployment wheel in the direction of the arrow on the handle until the valve capsule is fully retracted. The detachment of retainer tabs must be confirmed under fluoroscopy before the system is withdrawn.
In contrast to the above mentioned self-expanding devices, ACURATE neo has a unique deployment system132. Okuno T, Lanz J, Pilgrim T. ACURATE neo: How Is This TAVR Valve Doing to Fit into an Increasingly Crowded Field. Curr Cardiol Rep. 2020;22(10):107. Link. Due to the lower radial force of the stent frame, effective balloon pre-dilation is recommended to facilitate device expansion. Once the THV has passed the aortic valve, ensure that the THV is correctly positioned as indicated by the radiopaque intersection line (marker band) being in the annular plane. Deployment can be performed in a two-step manner. The first step can be initiated by turning the 1[st] rotating knob of the release handle counter-clockwise until full stop. This step should be done rather slowly in order to recognize any inappropriate movement of the device. After the first step, the stabilization arms are fully deployed and the upper crown is partly deployed as well. The positioning of the THV should be verified using aortic root angiography. At this stage, it is still possible to adjust the positioning. If the operator is satisfied with the position, the second step is initiated by removal of the safety knob. After retrieval of the pigtail catheter, turn the 2[nd] rotating knob of the release handle counter-clockwise until full stop to fully deploy the THV. While it is not mandatory, rapid ventricular pacing may facilitate stable valve positioning. The detachment of the frame paddles must be confirmed under fluoroscopy, and the nose cone centred before the delivery system is withdrawn.
14. After THV deployment, a pigtail catheter is reintroduced into the LV cavity, and simultaneous pressure measurements across the prosthetic valve are obtained. Measurements of the transvalvular gradient and diastolic pressure are important to determine the hemodynamic result. Subsequently, aortic root angiography is performed to assess the presence and severity of PVR as well as to make sure that the THV is implanted in an appropriate position, without aortic root rupture or acute coronary obstruction. Echocardiography may be utilized for the assessment of PVR additionally or alternatively. The assessment and the management of the complications will be discussed in a later section.
15. Post-dilation may be required in some cases to achieve optimal THV expansion and reduce PVR. The size of the balloon is typically the same as the perimeter/area derived annulus diameter obtained from MDCT.
16. After confirmation of the optimal result, the TAVI sheath is carefully withdrawn into the ipsilateral iliac artery. The contra-lateral femoral access site may be used to “cross-over” to the main access side. Cross-over may be performed by using an amputated pigtail catheter (distal tip cut using sterile scissors) or using a dedicated catheter. This catheter will allow for angiographic confirmation of the result upon removal of the TAVI sheath and may serve for bailout balloon angioplasty or covered stent implantation in case of the failure of vascular closure at the main access site. Subsequently the large bore TAVI sheath is removed and the pre-closure sutures tightened with a guidewire still in place. An additional closure device such as Angio-Seal (Terumo, Shibuya, Tokyo) or manual compression may be required if minor bleeding persists. If major bleeding exists despite application of the suture-based closure device (ProGlide), then a plug-based closure device (MANTA) can be considered as a bailout strategy. Deployment of a covered stent may be required if these attempts fail.
17. Bedside transthoracic echocardiography is performed at the end of the procedure and before the patient leaves the procedure room to assess the valve and LV function as well as to exclude a new pericardial effusion. The cardiac monitor should also be assessed for evidence of new conduction disturbances such as LBBB and intermittent or persistent complete heart block.
Alternative access TAVI
Transapical access
Transapical access is performed via a left anterolateral intercostal incision followed by needle puncture of the apex through a pledgeted purse-string suture. A dedicated sheath is placed and the THV deployed in a similar fashion to the transfemoral approach thereafter. This access is typically used for the Edwards SAPIEN platform. Of note, it is still a type of thoracotomy and associated with delayed recovery due to its invasiveness. In the PARTNER IA trial, the risk of all-cause mortality at 5 years was 79% in the transapical TAVI group versus 60% in the SAVR group (P=0.067)133. Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, Webb JG, Douglas PS, Anderson WN, Blackstone EH, Kodali SK, Makkar RR, Fontana GP, Kapadia S, Bavaria J, Hahn RT, Thourani VH, Babaliaros V, Pichard A, Herrmann HC, Brown DL, Williams M, Akin J, Davidson MJ, Svensson LG, investigators Pt. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385(9986):2477-84. Link. More recently, in the PARTNER II trial, transthoracic TAVI (including both transapical and transaortic) was associated with a higher rate of death or disabling stroke at 5 years compared with SAVR108. Makkar RR, Thourani VH, Mack MJ, Kodali SK, Kapadia S, Webb JG, Yoon SH, Trento A, Svensson LG, Herrmann HC, Szeto WY, Miller DC, Satler L, Cohen DJ, Dewey TM, Babaliaros V, Williams MR, Kereiakes DJ, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Brown DL, Fearon WF, Russo MJ, Pibarot P, Hahn RT, Jaber WA, Rogers E, Xu K, Wheeler J, Alu MC, Smith CR, Leon MB, Investigators P. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382(9):799-809. Link.
Transaortic access
Transaortic access is performed through the ascending aorta via a right anterior mini-thoracotomy in the second intercostal space. The aorta is inspected to avoid areas of calcification. Using a purse-string suture, needle puncture and access with a dedicated sheath is obtained. The puncture is made with a minimum of 6 cm above the aortic annulus for the CoreValve platform and 8 cm for the SAPIEN platform. The valve is then deployed in the same way as via the transfemoral approach134. Bapat V, Khawaja MZ, Attia R, Narayana A, Wilson K, Macgillivray K, Young C, Hancock J, Redwood S, Thomas M. Transaortic Transcatheter Aortic valve implantation using Edwards Sapien valve: a novel approach. Catheter Cardiovasc Interv. 2012;79(5):733-40. Link.
Transsubclavian/axillary access
Transsubclavian/axillary access is the most commonly used alternative access. Trans-subclavian access is typically performed via surgical cut-down, while trans-axillary may be performed percutaneously with pre-closure sutures most frequently into the proximal third of the axillary artery. There is no dedicated sheath available. A left-sided approach is selected in >95% of cases as a more favourable alignment of the THV with the native valve is achieved. The presence of the left internal mammary artery graft in patients with coronary artery bypass surgery is considered a relative contra-indication in the absence of native coronary artery flow to the left anterior descending artery or other territory that is supplied by the graft. In a recent retrospective analysis of the STS/ACC TVT registry, transsubclavian/axillary approach was used in 1,249 (34.4%) of 3,628 patients undergoing alternative access. After propensity-matching, trans-subclavian/axillary approach had lower 30-day mortality (5.3% vs. 8.4%, P<0.01), shorter lengths of intensive care unit and hospital stay, but a higher stroke rate (6.3% vs. 3.1%, P<0.05) compared with transthoracic approach135. Dahle TG, Kaneko T, McCabe JM. Outcomes Following Subclavian and Axillary Artery Access for Transcatheter Aortic Valve Replacement: Society of the Thoracic Surgeons/American College of Cardiology TVT Registry Report. JACC Cardiovasc Interv. 2019;12(7):662-669. Link.
Transcarotid access
Transcarotid access is performed percutaneously under local anaesthesia with cerebral oximetry monitoring. Satisfactory vessel size and vessel quality are critical determinants for efficacy and safety as is an anatomically complete Circle of Willis. In a retrospective analysis of a multicentre registry including 329 alternative access TAVI patients (2012-2017), transcarotid TAVI was associated with less new-onset atrial fibrillation (3.2% vs. 19.0%, P=0.002), acute kidney injury (0% vs. 12.1%, P=0.002), and shorter median length of hospital stay (6 days vs. 8 days, P<0.001) compared with transthoracic TAVI after propensity-matching136. Chamandi C, Abi-Akar R, Rodes-Cabau J, Blanchard D, Dumont E, Spaulding C, Doyle D, Pagny JY, DeLarochelliere R, Lafont A, Paradis JM, Puri R, Karam N, Maes F, Rodriguez-Gabella T, Chassaing S, Le Page O, Kalavrouziotis D, Mohammadi S. Transcarotid Compared With Other Alternative Access Routes for Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2018;11(11):e006388. Link.
Transcaval access
Transcaval access requires a dedicated pre-TAVI planning from the baseline MDCT. A calcium-free target on the right aortic wall that allows safe passage of the TAVI sheath from the inferior vena cava to the abdominal aorta needs to be identified. The trajectory of the sheath must be free of interposed obstacles (bowel), and the area of aortic entry should avoid important arterial branches, which allows for provisional covered stent bailout if needed. In brief, the femoral vein is accessed and a coronary guidewire (0.014 inch) connected to electrocautery is used to cross from the inferior vena cava into the abdominal aorta where it can be snared and advanced towards the aortic arch. The coronary guidewire is then exchanged for a stiff guidewire (0.035 inch). The TAVI sheath can be introduced via the stiff wire and the procedure can carry on as in the case of transfemoral TAVI. Once the THV has been deployed, a nitinol cardiac occluder (Amplatzer Duct Occluder or Amplatzer Ventricular Septal Defect Occluder, Abbott) is used to seal the arteriotomy in the abdominal aorta137. Greenbaum AB, Babaliaros VC, Chen MY, Stine AM, Rogers T, O’Neill WW, Paone G, Thourani VH, Muhammad KI, Leonardi RA, Ramee S, Troendle JF, Lederman RJ. Transcaval Access and Closure for Transcatheter Aortic Valve Replacement: A Prospective Investigation. J Am Coll Cardiol. 2017;69(5):511-521. Link. In a recent observational multicentre European study, transcaval TAVI was successful in 49 out of 50 patients suggesting it to be feasible and safe for high-risk AS patients who are not suitable for transfemoral or transsubclavian/axillary access138. Costa G, De Backer O, Pilgrim T, Kasel M, Redwood S, Aminian A, Lanz J, Michel J, Patterson T, Windecker S, Prendergast B, Greenbaum AB, Sondergaard L. Feasibility and safety of transcaval transcatheter aortic valve implantation: a multicentre European registry. EuroIntervention. 2020;15(15):e1319-e1324. Link.
Procedural Complications
In this section, we will provide key information of major procedural complications related to the TAVI procedure: PVR, annular rupture, coronary artery obstruction, valve dislocation/embolization, atrioventricular (AV) conduction disturbances, vascular complications, and stroke139. Scarsini R, De Maria GL, Joseph J, Fan L, Cahill TJ, Kotronias RA, Burzotta F, Newton JD, Kharbanda R, Prendergast B, Ribichini F, Banning AP. Impact of Complications During Transfemoral Transcatheter Aortic Valve Replacement: How Can They Be Avoided and Managed. J Am Heart Assoc. 2019;8(18):e013801. Link(Figure 20).
PVR is typically assessed by post-procedural aortic root angiography and/or transthoracic or transesophageal echocardiography (Figure 20). If significant PVR is observed, additional procedures need to be considered depending on the expected mechanism. If the leak is due to under-expansion of the THV, post-dilation should be performed to obtain optimal expansion. In case of THV malposition, a valve-in-valve procedure may be considered.
Advances in the TAVI transcatheter heart valve prostheses such as a circumferential outer sealing skirt and repositionable features (in some self-expanding devices) as well as improved THV sizing based on MDCT measurements have remarkably reduced the risk of PVR. Moderate or severe PVR occurred in 0.8% in the PARTNER 3 trial19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link and in 3.4% in the Evolut Low Risk trial20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. In a real world STS/ACC TVT registry22. Carroll JD, Mack MJ, Vemulapalli S, Herrmann HC, Gleason TG, Hanzel G, Deeb GM, Thourani VH, Cohen DJ, Desai N, Kirtane AJ, Fitzgerald S, Michaels J, Krohn C, Masoudi FA, Brindis RG, Bavaria JE. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76(21):2492-2516. Link, the rate was reported to be 1.5% in 2019. In contrast, even in the recent low risk trials, the rate of any PVR including mild PVR was reported as high as 40%, 19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. Although moderate or severe PVR has been consistently associated with increased mortality, there is conflicting data on the adverse effect of mild PVR, which may be of particular importance among younger patients with longer life-expectancy, , 140. Athappan G, Patvardhan E, Tuzcu EM, Svensson LG, Lemos PA, Fraccaro C, Tarantini G, Sinning JM, Nickenig G, Capodanno D, Tamburino C, Latib A, Colombo A, Kapadia SR. Incidence, predictors, and outcomes of aortic regurgitation after transcatheter aortic valve replacement: meta-analysis and systematic review of literature. J Am Coll Cardiol. 2013;61(15):1585-95. Link141. Van Belle E, Juthier F, Susen S, Vincentelli A, Iung B, Dallongeville J, Eltchaninoff H, Laskar M, Leprince P, Lievre M, Banfi C, Auffray JL, Delhaye C, Donzeau-Gouge P, Chevreul K, Fajadet J, Leguerrier A, Prat A, Gilard M, Teiger E. Postprocedural aortic regurgitation in balloon-expandable and self-expandable transcatheter aortic valve replacement procedures: analysis of predictors and impact on long-term mortality: insights from the FRANCE2 Registry. Circulation. 2014;129(13):1415-27. Link142. Pibarot P, Hahn RT, Weissman NJ, Arsenault M, Beaudoin J, Bernier M, Dahou A, Khalique OK, Asch FM, Toubal O, Leipsic J, Blanke P, Zhang F, Parvataneni R, Alu M, Herrmann H, Makkar R, Mack M, Smalling R, Leon M, Thourani VH, Kodali S. Association of Paravalvular Regurgitation With 1-Year Outcomes After Transcatheter Aortic Valve Replacement With the SAPIEN 3 Valve. JAMA Cardiol. 2017;2(11):1208-1216. Link.
Annular rupture
Annular rupture is a rare (<1%) but devastating complication that may occur after balloon-expandable THV implantation or aggressive pre/post-dilation of any valve type in the setting of a severely calcified valve with extension into the aortic root and LVOT98. Okuno T, Asami M, Heg D, Lanz J, Praz F, Hagemeyer D, Brugger N, Grani C, Huber A, Spirito A, Raber L, Stortecky S, Windecker S, Pilgrim T. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13(15):1789-1799. Link. If rapid hemodynamic collapse occurs and is unexplained, the presence of annular rupture should be meticulously assessed. Other possible causes of hemodynamic instability should also be considered, such as coronary artery obstruction, injury of the LV or right ventricle with pericardial effusions, aortic dissection, or retroperitoneal haemorrhage. Typically, annular rupture is identified by aortic root angiography and/or echocardiography with pericardial effusion (Figure 20). However, in some cases such as infra-annular injury, transesophageal echocardiography may be required for its detection. Furthermore, the clinical manifestations may vary depending on the location and extent of the injury. Rupture may only be apparent some hours after the procedure or later. Small injuries (contained rupture) may even be unrecognized. In cases of suspected rupture, serial imaging and/or MDCT may be required. The treatment approaches include surgical or interventional repair/reconstruction, isolated pericardial drainage, and a conservative strategy, depending on the type of rupture, its clinical manifestations, and the patient’s background although outcomes remain poor143. Pasic M, Unbehaun A, Buz S, Drews T, Hetzer R. Annular rupture during transcatheter aortic valve replacement: classification, pathophysiology, diagnostics, treatment approaches, and prevention. JACC Cardiovasc Interv. 2015;8(1 Pt A):1-9. Link.
Coronary artery obstruction
Coronary artery obstruction is a rare (<1%) but life-threatening complication caused by native leaflets or device material overlapping the coronary ostia144. Ribeiro HB, Nombela-Franco L, Urena M, Mok M, Pasian S, Doyle D, DeLarochelliere R, Cote M, Laflamme L, DeLarochelliere H, Allende R, Dumont E, Rodes-Cabau J. Coronary obstruction following transcatheter aortic valve implantation: a systematic review. JACC Cardiovasc Interv. 2013;6(5):452-61. Link(Figure 20). The left main coronary artery is more commonly involved, while right coronary artery occlusion rarely occurs. Low coronary height (<10mm), narrow sinus of Valsalva, and heavily calcified leaflets are considered high risk anatomic features. Pre-dilation with simultaneous aortic root angiography may help to identify the potential risk of coronary artery obstruction. As described previously, in patients who are deemed at high risk of coronary artery obstruction, preventative strategies such as coronary protection, 113. Abramowitz Y, Chakravarty T, Jilaihawi H, Kashif M, Kazuno Y, Takahashi N, Maeno Y, Nakamura M, Cheng W, Makkar RR. Clinical impact of coronary protection during transcatheter aortic valve implantation: first reported series of patients. EuroIntervention. 2015;11(5):572-81. Link114. Mercanti F, Rosseel L, Neylon A, Bagur R, Sinning JM, Nickenig G, Grube E, Hildick-Smith D, Tavano D, Wolf A, Colonna G, Latib A, Mitomo S, Petronio AS, Angelillis M, Tchetche D, De Biase C, Adamo M, Nejjari M, Digne F, Schafer U, Amabile N, Achkouty G, Makkar RR, Yoon SH, Finkelstein A, Dvir D, Jones T, Chevalier B, Lefevre T, Piazza N, Mylotte D. Chimney Stenting for Coronary Occlusion During TAVR: Insights From the Chimney Registry. JACC Cardiovasc Interv. 2020;13(6):751-761. Link or BASILICA145. Lederman RJ, Babaliaros VC, Rogers T, Khan JM, Kamioka N, Dvir D, Greenbaum AB. Preventing Coronary Obstruction During Transcatheter Aortic Valve Replacement: From Computed Tomography to BASILICA. JACC Cardiovasc Interv. 2019;12(13):1197-1216. Link may be considered (Figure 12). Acute coronary artery obstruction typically causes rapidly worsening hypotension with dynamic electrocardiographic changes. In such cases, immediate angiographic assessment should be performed to identify the affected lesion. Subsequently, the lesion should be treated typically with percutaneous coronary stenting.
Valve dislocation/embolization
Valve dislocation/embolization occurs in approximately 1%. The incidence has decreased over time attributable to increasing institutional and operator experience and the availability of repositionable devices and refined delivery catheters. Valve dislocations are either towards the aorta or into the LV cavity (Figure 20). Although it usually occurs immediately during or after THV implantation, late device migration (up to 1 year after TAVI) has been reported146. Nkomo VT, Suri RM, Pislaru SV, Greason KL, Sinak LJ, Holmes DR, Mathew V, Rihal CS. Delayed transcatheter heart valve migration and failure. JACC Cardiovasc Imaging. 2014;7(9):960-2. Link. Non-calcified native aortic valve leaflets, eccentric and asymmetric calcifications, pre-existing aortic regurgitation, and acute aortic angulation are considered high risk anatomic features related to valve dislocation/embolization. In an international retrospective registry147. Kim WK, Schafer U, Tchetche D, Nef H, Arnold M, Avanzas P, Rudolph T, Scholtz S, Barbanti M, Kempfert J, Mangieri A, Lauten A, Frerker C, Yoon SH, Holzamer A, Praz F, De Backer O, Toggweiler S, Blumenstein J, Purita P, Tarantini G, Thilo C, Wolf A, Husser O, Pellegrini C, Burgdorf C, Antolin RAH, Diaz VAJ, Liebetrau C, Schofer N, Mollmann H, Eggebrecht H, Sondergaard L, Walther T, Pilgrim T, Hilker M, Makkar R, Unbehaun A, Borgermann J, Moris C, Achenbach S, Dorr O, Brochado B, Conradi L, Hamm CW. Incidence and outcome of peri-procedural transcatheter heart valve embolization and migration: the TRAVEL registry (TranscatheteR HeArt Valve EmboLization and Migration). Eur Heart J. 2019;40(38):3156-3165. Link, valve dislocation/embolization occurred in 273 out of 29,636 patients (0.92%), of which 217 were into the aorta and 56 into the LV. Bailout measures included repositioning attempts using snares (Amplatz GooseNeck, Medtronic) or miscellaneous tools (41.0%), multiple valve implantation (83.2%), and conversion to surgery (19.0%). In a study with 1:4 propensity score matching, valve dislocation/embolization was associated with an increased risk of stroke at 30 days (10.6% vs. 2.8%, P<0.001) and mortality at 30 days (18.6% vs. 4.9%, P<0.001) and at 1 year (30.5% vs. 16.6%, P<0.001).
Atrioventricular (AV) conduction disturbance
AV conduction impairment, including advanced heart block and new LBBB, is a common adverse event and remains a limitation of TAVI. The incidence is higher with self-expanding devices compared with balloon-expandable devices. In recent low-risk trials, new PPI was required in 6.5% after balloon-expandable TAVI19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link (comparable to SAVR) and in 17.4% after self-expanding TAVI20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. The incidence of new LBBB has been reported as 12% to 24% for SAPIEN 3 and 34% for Evolut R139. Scarsini R, De Maria GL, Joseph J, Fan L, Cahill TJ, Kotronias RA, Burzotta F, Newton JD, Kharbanda R, Prendergast B, Ribichini F, Banning AP. Impact of Complications During Transfemoral Transcatheter Aortic Valve Replacement: How Can They Be Avoided and Managed. J Am Heart Assoc. 2019;8(18):e013801. Link. Pre-existing right bundle branch block, short membranous septum length, non-coronary cusp device landing zone calcification, and deep implantation of the THV have been identified as independent predictors of new conduction disturbances148. Maeno Y, Abramowitz Y, Kawamori H, Kazuno Y, Kubo S, Takahashi N, Mangat G, Okuyama K, Kashif M, Chakravarty T, Nakamura M, Cheng W, Friedman J, Berman D, Makkar RR, Jilaihawi H. A Highly Predictive Risk Model for Pacemaker Implantation After TAVR. JACC: Cardiovascular Imaging. 2017;10(10, Part A):1139-1147. Link.
Although the development of AV conduction impairment usually occurs within 24 hours, it sometimes occurs later than 48 hours after TAVI or even after discharge from the hospital. Therefore, monitoring by telemetry should be continued after the procedure and potential risk assessment of delayed conduction disturbances should be made before discharge, 149. Rodes-Cabau J, Ellenbogen KA, Krahn AD, Latib A, Mack M, Mittal S, Muntane-Carol G, Nazif TM, Sondergaard L, Urena M, Windecker S, Philippon F. Management of Conduction Disturbances Associated With Transcatheter Aortic Valve Replacement: JACC Scientific Expert Panel. J Am Coll Cardiol. 2019;74(8):1086-1106. Link150. Lilly SM, Deshmukh AJ, Epstein AE, Ricciardi MJ, Shreenivas S, Velagapudi P, Wyman JF. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76(20):2391-2411. Link. Although the impact of new PPI or LBBB on cardiovascular mortality remains a subject of debate151. Faroux L, Chen S, Muntane-Carol G, Regueiro A, Philippon F, Sondergaard L, Jorgensen TH, Lopez-Aguilera J, Kodali S, Leon M, Nazif T, Rodes-Cabau J. Clinical impact of conduction disturbances in transcatheter aortic valve replacement recipients: a systematic review and meta-analysis. Eur Heart J. 2020. Link, the conduction disturbances may lead to LV dyssynchrony/dysfunction, lead-induced tricuspid regurgitation, and other pacing lead adverse events (fracture and endocarditis) at later follow-up. Therefore, the risk should be particularly weighed when performing TAVI for younger patients with longer life-expectancy.
Vascular complications
Although the incidence has decreased over time (2% to 4% in the recent low-risk trials, 19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link) due to smaller and more flexible delivery systems and increasing operator experience, major vascular complications are still common and associated with increased mortality152. Généreux P, Webb JG, Svensson LG, Kodali SK, Satler LF, Fearon WF, Davidson CJ, Eisenhauer AC, Makkar RR, Bergman GW, Babaliaros V, Bavaria JE, Velazquez OC, Williams MR, Hueter I, Xu K, Leon MB. Vascular Complications After Transcatheter Aortic Valve Replacement: Insights From the PARTNER (Placement of AoRTic TraNscathetER Valve) Trial. Journal of the American College of Cardiology. 2012;60(12):1043-1052. Link. Vascular complications typically include dissection, stenosis, perforation, and pseudoaneurysm or aneurysm. The most frequent cause is a closure device failure leading to continued bleeding or stenosis (Figure 20). Routine angiography via a crossover catheter to assess for aortic/iliofemoral dissection, perforation, or stenosis after TAVI sheath removal is facilitates early recognition. In most cases, vascular complications can be treated percutaneously using bailout balloon angioplasty or covered stent implantation via the crossover catheter153. Stortecky S, Wenaweser P, Diehm N, Pilgrim T, Huber C, Rosskopf AB, Khattab AA, Buellesfeld L, Gloekler S, Eberle B, Schmidli J, Carrel T, Meier B, Windecker S. Percutaneous management of vascular complications in patients undergoing transcatheter aortic valve implantation. JACC Cardiovasc Interv. 2012;5(5):515-524. Link. Surgical repair is typically reserved for extensive dissection or bleeding or challenging anatomy in close proximity to the femoral bifurcation.
Stroke
A recent meta-analysis of randomized clinical trials has reported that TAVI is associated with a 19% lower risk of stroke throughout 2 years compared with SAVR154. Siontis GCM, Overtchouk P, Cahill TJ, Modine T, Prendergast B, Praz F, Pilgrim T, Petrinic T, Nikolakopoulou A, Salanti G, Sondergaard L, Verma S, Juni P, Windecker S. Transcatheter aortic valve implantation vs. surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. 2019;40(38):3143-3153. Link. However, stroke remains one of the most feared complications of TAVI associated with considerable morbidity and mortality155. Vlastra W, Jimenez-Quevedo P, Tchetche D, Chandrasekhar J, de Brito FS, Jr., Barbanti M, Kornowski R, Latib A, D’Onofrio A, Ribichini F, Baan J, Tijssen JGP, De la Torre Hernandez JM, Dumonteil N, Sarmento-Leite R, Sartori S, Rosato S, Tarantini G, Lunardi M, Orvin K, Pagnesi M, Hernandez-Antolin R, Modine T, Dangas G, Mehran R, Piek JJ, Delewi R. Predictors, Incidence, and Outcomes of Patients Undergoing Transfemoral Transcatheter Aortic Valve Implantation Complicated by Stroke. Circ Cardiovasc Interv. 2019;12(3):e007546. Link. Stroke related to TAVI most frequently occurs during or within 24-48 hours after the procedure. While acute stroke is more likely to be related to procedural factors such as embolization of debris/thrombus and sustained hypotension, subacute or late stroke may be the consequence of bioprosthetic valve thrombosis, new-onset atrial fibrillation, and atherothrombotic burden. Patient-related factors such as prior cerebrovascular events, atrial fibrillation, chronic kidney disease, and severely calcified aortic valve, concomitant mitral stenosis, as well as procedural-related factor such as post-dilation, device dislocation/embolization, and lower operator experience has been associated with an increased risk of stroke following TAVI, , 155. Vlastra W, Jimenez-Quevedo P, Tchetche D, Chandrasekhar J, de Brito FS, Jr., Barbanti M, Kornowski R, Latib A, D’Onofrio A, Ribichini F, Baan J, Tijssen JGP, De la Torre Hernandez JM, Dumonteil N, Sarmento-Leite R, Sartori S, Rosato S, Tarantini G, Lunardi M, Orvin K, Pagnesi M, Hernandez-Antolin R, Modine T, Dangas G, Mehran R, Piek JJ, Delewi R. Predictors, Incidence, and Outcomes of Patients Undergoing Transfemoral Transcatheter Aortic Valve Implantation Complicated by Stroke. Circ Cardiovasc Interv. 2019;12(3):e007546. Link156. Auffret V, Regueiro A, Del Trigo M, Abdul-Jawad Altisent O, Campelo-Parada F, Chiche O, Puri R, Rodes-Cabau J. Predictors of Early Cerebrovascular Events in Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2016;68(7):673-84. Link157. Okuno T, Hagemeyer D, Brugger N, Ryffel C, Heg D, Lanz J, Praz F, Stortecky S, Raber L, Roten L, Reichlin T, Windecker S, Pilgrim T. Valvular and Nonvalvular Atrial Fibrillation in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13(18):2124-2133. Link. Optimal anticoagulation during the procedure is essential for the prevention of stroke. As previously described, cerebral embolic protection devices may be used for the prevention of cerebrovascular events during the procedure (Figure 13). Once stroke or transient ischemic attack is suspected, patients should undergo prompt examination by a neurologist and diagnostic imaging whenever indicated. Interventional neuroradiology treatment may be performed in accordance with the neurology consultation.
Postprocedural Care
The immediate post procedure phase is important as early adverse events such as pericardial effusion, vascular related bleeding, stroke, and arrhythmias may occur during this time. Patients are monitored in a continuous care setting immediately following the procedure. Telemetry is typically continued to assess for new AV conduction disturbances or any other arrhythmia for at least 24 hours after the procedure or until discharge if the relevant risk is considered high. Echocardiography should routinely be performed before discharge to evaluate early post-procedural prosthetic valve function. After discharge, patients typically undergo routine clinical and echocardiographic follow-up at 1 month, 6, and 12 months, and then annually. Prophylaxis for bacterial endocarditis should be recommended if patients undergo any relevant procedures with risk for bacteraemia such as invasive dental procedures.
Antithrombotic management
In general, patients undergoing TAVI are treated with life-long single antiplatelet therapy (SAPT) with low-dose aspirin (75 to 100 mg daily) (Class IIaB)24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. If aspirin is contraindicated, clopidogrel or another P2Y12 inhibitor may serve as an alternative. While the routine use of dual-antiplatelet therapy (DAPT) for 3 to 6 months followed by life-long SAPT has been the default strategy until recently, 25. Baumgartner H, Falk V, Bax JJ, De Bonis M, Hamm C, Holm PJ, Iung B, Lancellotti P, Lansac E, Rodriguez Munoz D, Rosenhek R, Sjogren J, Tornos Mas P, Vahanian A, Walther T, Wendler O, Windecker S, Zamorano JL. 2017 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2017;38(36):2739-2791. Link158. Nishimura Rick A, Otto Catherine M, Bonow Robert O, Carabello Blase A, Erwin John P, Fleisher Lee A, Jneid H, Mack Michael J, McLeod Christopher J, O’Gara Patrick T, Rigolin Vera H, Sundt Thoralf M, Thompson A. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Circulation. 2017;135(25):e1159-e1195. Link, it is now only considered for patients who are at low risk of bleeding (Class IIbB)24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. The results of randomized clinical trials comparing SAPT versus DAPT in patients undergoing TAVI are summarized in Table 11, , 159. Ussia GP, Scarabelli M, Mule M, Barbanti M, Sarkar K, Cammalleri V, Imme S, Aruta P, Pistritto AM, Gulino S, Deste W, Capodanno D, Tamburino C. Dual antiplatelet therapy versus aspirin alone in patients undergoing transcatheter aortic valve implantation. Am J Cardiol. 2011;108(12):1772-6. Link160. Stabile E, Pucciarelli A, Cota L, Sorropago G, Tesorio T, Salemme L, Popusoi G, Ambrosini V, Cioppa A, Agrusta M, Catapano D, Moscariello C, Trimarco B, Esposito G, Rubino P. SAT-TAVI (single antiplatelet therapy for TAVI) study: a pilot randomized study comparing double to single antiplatelet therapy for transcatheter aortic valve implantation. Int J Cardiol. 2014;174(3):624-7. Link161. Rodes-Cabau J, Masson JB, Welsh RC, Garcia Del Blanco B, Pelletier M, Webb JG, Al-Qoofi F, Genereux P, Maluenda G, Thoenes M, Paradis JM, Chamandi C, Serra V, Dumont E, Cote M. Aspirin Versus Aspirin Plus Clopidogrel as Antithrombotic Treatment Following Transcatheter Aortic Valve Replacement With a Balloon-Expandable Valve: The ARTE (Aspirin Versus Aspirin + Clopidogrel Following Transcatheter Aortic Valve Implantation) Randomized Clinical Trial. JACC Cardiovasc Interv. 2017;10(13):1357-1365. Link. In the most recent and largest randomized clinical trial (POPular TAVI cohort A), SAPT was superior in terms of the composite of bleeding and thromboembolic events (23% vs. 31.1%, risk ratio 0.74, 95% CI for superiority 0.57 to 0.95, P for superiority =0.04), and noninferior in terms of thromboembolic events (9.7% vs. 9.9%, difference -0.2 percentage points, 95% CI for noninferiority -4.7 to 4.3, P for noninferiority = 0.004) at 1 year as compared with DAPT162. Brouwer J, Nijenhuis VJ, Delewi R, Hermanides RS, Holvoet W, Dubois CLF, Frambach P, De Bruyne B, van Houwelingen GK, Van Der Heyden JAS, Tousek P, van der Kley F, Buysschaert I, Schotborgh CE, Ferdinande B, van der Harst P, Roosen J, Peper J, Thielen FWF, Veenstra L, Chan Pin Yin D, Swaans MJ, Rensing B, van ’t Hof AWJ, Timmers L, Kelder JC, Stella PR, Baan J, Ten Berg JM. Aspirin with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;383(15):1447-1457. Link. OAC with VKA for at least 3 months after TAVI may also be considered in patients who are at low risk of bleeding (Class IIbB)24. Otto CM, Nishimura RA, Bonow RO, Carabello BA, Erwin JP, 3rd, Gentile F, Jneid H, Krieger EV, Mack M, McLeod C, O’Gara PT, Rigolin VH, Sundt TM, 3rd, Thompson A, Toly C. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2020:CIR0000000000000923. Link. This strategy may be beneficial for the prevention of bioprosthetic valve thrombosis163. De Backer O, Dangas GD, Jilaihawi H, Leipsic JA, Terkelsen CJ, Makkar R, Kini AS, Veien KT, Abdel-Wahab M, Kim WK, Balan P, Van Mieghem N, Mathiassen ON, Jeger RV, Arnold M, Mehran R, Guimaraes AHC, Norgaard BL, Kofoed KF, Blanke P, Windecker S, Sondergaard L, Investigators G-D. Reduced Leaflet Motion after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382(2):130-139. Link. However, the GALILEO trial showed a strategy of low-dose rivaroxaban (10 mg daily) plus low-dose aspirin was associated with a higher risk of death or thromboembolic events (HR 1.35, 95% CI 1.01 to 1.81, P=0.04) and a higher risk of bleeding (HR 1.50, 95% CI 0.95 to 2.37, P=0.08) than an antiplatelet-based strategy despite a lower risk of subclinical leaflet thrombosis (Table 11)164. Dangas GD, Tijssen JGP, Wohrle J, Sondergaard L, Gilard M, Mollmann H, Makkar RR, Herrmann HC, Giustino G, Baldus S, De Backer O, Guimaraes AHC, Gullestad L, Kini A, von Lewinski D, Mack M, Moreno R, Schafer U, Seeger J, Tchetche D, Thomitzek K, Valgimigli M, Vranckx P, Welsh RC, Wildgoose P, Volkl AA, Zazula A, van Amsterdam RGM, Mehran R, Windecker S, Investigators G. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382(2):120-129. Link. Current ongoing randomized clinical trials will add further insights to this field (Table 12)
Table 11
Randomized clinical trials on antithrombotic therapy after TAVI
If there is an established indication for DAPT, the antithrombotic management should follow the recommendations for the indication. Namely, patients should be treated with DAPT for 3-6 months after PCI in patients with chronic coronary syndromes and 6-12 months after PCI for acute coronary syndromes165. Valgimigli M, Bueno H, Byrne RA, Collet JP, Costa F, Jeppsson A, Juni P, Kastrati A, Kolh P, Mauri L, Montalescot G, Neumann FJ, Petricevic M, Roffi M, Steg PG, Windecker S, Zamorano JL, Levine GN, Group ESCSD, Guidelines ESCCfP, Societies ESCNC. 2017 ESC focused update on dual antiplatelet therapy in coronary artery disease developed in collaboration with EACTS: The Task Force for dual antiplatelet therapy in coronary artery disease of the European Society of Cardiology (ESC) and of the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2018;39(3):213-260. Link. For patients with an established indication for OAC, OAC should be continued after TAVI. In this setting, additional antiplatelet therapy is generally not recommended. In a recent randomized clinical trial (POPular TAVI cohort B), OAC alone was associated with a lower risk of bleeding (21.7% vs. 34.6%, risk ratio 0.63, 95% CI 0.43 to 0.90, P=0.01), and was noninferior in terms of the thromboembolic composite endpoint of cardiovascular death, ischemic stroke, or myocardial infarction (13.4% vs. 17.3%, difference -3.9 percentage points, 95% CI for noninferiority -11.9 to 4.0) at 1 year as compared with OAC with clopidogrel (Table 11)166. Nijenhuis VJ, Brouwer J, Delewi R, Hermanides RS, Holvoet W, Dubois CLF, Frambach P, De Bruyne B, van Houwelingen GK, Van Der Heyden JAS, Tousek P, van der Kley F, Buysschaert I, Schotborgh CE, Ferdinande B, van der Harst P, Roosen J, Peper J, Thielen FWF, Veenstra L, Chan Pin Yin D, Swaans MJ, Rensing B, van ’t Hof AWJ, Timmers L, Kelder JC, Stella PR, Baan J, Ten Berg JM. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;382(18):1696-1707. Link. Whether these patients should be treated with DOACs or VKA remains a subject of debate. In a retrospective study of the Japanese TAVI registry (OCEAN TAVI), DOACs were associated with a lower incidence of all-cause mortality compared with VKA (HR 0.53, 95%CI 0.25 to 0.96) after using inverse probability of treatment weighting based on the propensity score167. Kawashima H, Watanabe Y, Hioki H, Kozuma K, Kataoka A, Nakashima M, Nagura F, Nara Y, Yashima F, Tada N, Naganuma T, Yamawaki M, Yamanaka F, Shirai S, Mizutani K, Tabata M, Ueno H, Takagi K, Yamamoto M, Hayashida K, Investigator O-T. Direct Oral Anticoagulants Versus Vitamin K Antagonists in Patients With Atrial Fibrillation After TAVR. JACC Cardiovasc Interv. 2020;13(22):2587-2597. Link. The ENVISAGE-TAVI AF trial, comparing edoxaban versus VKA in this setting, will provide the clinical evidence on the safety and efficacy of these strategies (Table 12)168. Van Mieghem NM, Unverdorben M, Valgimigli M, Mehran R, Boersma E, Baber U, Hengstenberg C, Shi M, Chen C, Saito S, Veltkamp R, Vranckx P, Dangas GD. Edoxaban Versus standard of care and their effects on clinical outcomes in patients having undergone Transcatheter Aortic Valve Implantation in Atrial Fibrillation-Rationale and design of the ENVISAGE-TAVI AF trial. Am Heart J. 2018;205:63-69. Link.
Clinical Evidence
Randomized clinical trials: TAVI versus SAVR
TAVI has been thoroughly investigated in a number of randomized clinical trials using both balloon-expandable and self-expanding devices in elderly patients with symptomatic severe AS across the entire risk spectrum. Some of the trials have already reached 5-year follow-up and reported clinical and echocardiographic outcomes (PARTNER I and II, US CoreValve High Risk, and NOTION). The main results of the trials are summarized in Table 13, Table 14and Table 15.
Table 13
Summary of randomized clinical trials of TAVI versus SAVR.
The PARTNER I trial consisted of 2 randomized cohorts: cohort A14. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ, Investigators PT. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98. Link randomly assigned high-risk patients to either transfemoral/transapical TAVI (n=348) or SAVR (n=351); cohort B13. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S, Investigators PT. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-607. Link randomly assigned inoperable patients to either conservative treatment (n=179) or transfemoral TAVI (n=179). The Edwards SAPIEN balloon-expandable valve system was used for TAVI in this trial. The primary endpoint was all-cause death at 1 year.
In cohort B (mean age: 83 years), TAVI was associated with a 20% absolute risk reduction of all-cause death compared with conservative treatment at 1 year (30.7% vs. 50.7%, HR 0.55, 95% CI 0.40 to 0.74, P<0.001)13. Leon MB, Smith CR, Mack M, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Brown DL, Block PC, Guyton RA, Pichard AD, Bavaria JE, Herrmann HC, Douglas PS, Petersen JL, Akin JJ, Anderson WN, Wang D, Pocock S, Investigators PT. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363(17):1597-607. Link. The follow-up data reported up to 5 years showed TAVI to maintain superiority over medical treatment. At the end of 5-year follow-up, overall mortality was 71.8% in the TAVI group compared with 93.8% in the medical treatment group (HR 0.50, 95% CI 0.39 to 0.65, P<0.001).169. Kapadia SR, Leon MB, Makkar RR, Tuzcu EM, Svensson LG, Kodali S, Webb JG, Mack MJ, Douglas PS, Thourani VH, Babaliaros VC, Herrmann HC, Szeto WY, Pichard AD, Williams MR, Fontana GP, Miller DC, Anderson WN, Akin JJ, Davidson MJ, Smith CR, investigators Pt. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385(9986):2485-91. Link
In cohort A (mean age: 84 years), TAVI was non-inferior to SAVR in terms of all-cause death at 1 year (24.2 vs. 26.8%, P for noninferiority = 0.001)14. Smith CR, Leon MB, Mack MJ, Miller DC, Moses JW, Svensson LG, Tuzcu EM, Webb JG, Fontana GP, Makkar RR, Williams M, Dewey T, Kapadia S, Babaliaros V, Thourani VH, Corso P, Pichard AD, Bavaria JE, Herrmann HC, Akin JJ, Anderson WN, Wang D, Pocock SJ, Investigators PT. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364(23):2187-98. Link. At 5-year follow-up, the risk of all-cause death remained similar between TAVI and SAVR (67.8% vs. 62.4%, HR 1.04, 95% 0.86 to 1.24)133. Mack MJ, Leon MB, Smith CR, Miller DC, Moses JW, Tuzcu EM, Webb JG, Douglas PS, Anderson WN, Blackstone EH, Kodali SK, Makkar RR, Fontana GP, Kapadia S, Bavaria J, Hahn RT, Thourani VH, Babaliaros V, Pichard A, Herrmann HC, Brown DL, Williams M, Akin J, Davidson MJ, Svensson LG, investigators Pt. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385(9986):2477-84. Link. In a stratified analysis by access site, there was no difference in mortality between transfemoral TAVI and SAVR (63% vs. 64%, P=0.41), while transapical TAVI was associated with a numerically higher risk of mortality (79% vs. 60%, P=0.067) compared with SAVR at 5 years. The risk of repeat hospitalization (42.3% vs. 34.2%, P=0.17), stroke (10.4% vs. 11.3%, P=0.61), and myocardial infarction (2.9% vs. 5.9%, P-0.15), and functional status (NYHA class I or II: 85% vs. 81%, P=0.57) were comparable between the groups up to 5 years. In contrast, major vascular complications more frequently occurred after TAVI (11.9% vs. 4.7%, P=0.0002), while major bleeding more frequently occurred after SAVR (26.6% vs. 34.4%, P=0.003) (Table 13, Table 14and Table 15).
US CoreValve High Risk (CoreValve, High risk)
The US CoreValve High Risk trial compared TAVI by means of the CoreValve self-expanding valve system with SAVR in 795 high-risk patients (mean age: 83 years)15. Adams DH, Popma JJ, Reardon MJ, Yakubov SJ, Coselli JS, Deeb GM, Gleason TG, Buchbinder M, Hermiller J, Jr., Kleiman NS, Chetcuti S, Heiser J, Merhi W, Zorn G, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte J, Maini B, Mumtaz M, Chenoweth S, Oh JK, Investigators USCC. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370(19):1790-8. Link. TAVI was predominantly performed via transfemoral access. The primary endpoint was all-cause death at 1 year. TAVI was associated with a significantly lower risk of all-cause death at 1 year than SAVR (14.2% vs. 19.1%, P for noninferiority <0.001, P for superiority =0.04). At 5 years, both TAVI and SAVR resulted in similar survival outcomes (all-cause death: 55.3% vs. 55.4%, HR 0.93, 95% CI 0.77 to 1.14, P=0.5). Again, the risk of repeat hospitalization (37.5% vs. 31.5%, P=0.08), major stroke (12.3% vs. 13.2%, P=0.49), and myocardial infarction (3.1% vs. 3.3%, P=0.93), and functional status (NYHA class mean of 1.3 in both groups) were comparable between the groups up to 5 years, while major vascular complications occurred more frequently (7.1% vs. 2.0%, P=0.001) in the TAVI group and major bleedings more frequently (35.9% vs. 43.3%, P=0.05) in the SAVR group throughout the years (Table 13, Table 14and Table 15).
PARTNER II (SAPIEN XT, Intermediate risk)
In the PARTNER II trial, 2,032 intermediate-risk patients (mean age: 82 years) were randomized to TAVI using the SAPIEN XT balloon-expandable valve system or SAVR16. Leon MB, Smith CR, Mack MJ, Makkar RR, Svensson LG, Kodali SK, Thourani VH, Tuzcu EM, Miller DC, Herrmann HC, Doshi D, Cohen DJ, Pichard AD, Kapadia S, Dewey T, Babaliaros V, Szeto WY, Williams MR, Kereiakes D, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Moses JW, Trento A, Brown DL, Fearon WF, Pibarot P, Hahn RT, Jaber WA, Anderson WN, Alu MC, Webb JG, Investigators P. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374(17):1609-20. Link. Patients were stratified in cohorts according to access route (transfemoral = 76.3% or transthoracic = 23.7%) before the randomization. The primary endpoint was the composite of all-cause death or disabling stroke at 2 years. TAVI was noninferior to SAVR in terms of the primary endpoint at 2 years (19.3% vs. 21.1%, P for noninferiority =0.001). In the transfemoral access cohort, TAVI resulted in a lower rate of death or disabling stroke than SAVR (HR 0.79, 95% CI 0.62 to 1.00, P=0.05), while in the transthoracic access cohort, outcomes were similar between the two groups (HR 1.21, 95% CI 0.84 to 1.74, P=0.31). Five-year follow-up data from the trial has recently been reported108. Makkar RR, Thourani VH, Mack MJ, Kodali SK, Kapadia S, Webb JG, Yoon SH, Trento A, Svensson LG, Herrmann HC, Szeto WY, Miller DC, Satler L, Cohen DJ, Dewey TM, Babaliaros V, Williams MR, Kereiakes DJ, Zajarias A, Greason KL, Whisenant BK, Hodson RW, Brown DL, Fearon WF, Russo MJ, Pibarot P, Hahn RT, Jaber WA, Rogers E, Xu K, Wheeler J, Alu MC, Smith CR, Leon MB, Investigators P. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382(9):799-809. Link. There was no significant difference in the primary endpoint between the TAVI group and the SAVR group at 5 years (47.9% vs. 43.4%, HR 1.09. 95% CI 0.95 to 1.25, P=0.21). Results were similar for the transfemoral-access cohort (44.5% vs. 42.0%, HR 1.02, 95% CI 0.87 to 1.20), while the risk was higher after TAVI than after SAVR in the transthoracic-access cohort (59.3% vs. 48.3%, HR 1.32, 95% CI 1.02 to 1.71). Improvements in health status (NYHA class I or II: 89.0% vs. 92.7%; average increase in the KCCQ-OS score: 19.6 points and 20.5 points) were also similar at 5 years. However, more patients in the TAVI group than in the SAVR group had aortic-valve reintervention (3.2% vs. 0.8%, HR 3.28, 95% CI 1.32 to 8.13) and repeat hospitalization (33.3% vs. 25.2%, HR 1.28, 95% CI 1.07 to 1.53) at 5 years (Table 13, Table 14and Table 15).
SURTAVI (CoreValve/Evolut R, Intermediate risk)
The SURTAVI trial (n=1,746) was a randomized trial designed to compare the safety and efficacy of TAVI using the CoreValve (84%) or the Evolut R (16%) self-expanding valve system and SAVR in intermediate-risk patients (mean age: 80 years)17. Reardon MJ, Van Mieghem NM, Popma JJ, Kleiman NS, Sondergaard L, Mumtaz M, Adams DH, Deeb GM, Maini B, Gada H, Chetcuti S, Gleason T, Heiser J, Lange R, Merhi W, Oh JK, Olsen PS, Piazza N, Williams M, Windecker S, Yakubov SJ, Grube E, Makkar R, Lee JS, Conte J, Vang E, Nguyen H, Chang Y, Mugglin AS, Serruys PW, Kappetein AP, Investigators S. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376(14):1321-1331. Link. For the TAVI procedure, transfemoral access was preferred (94%); subclavian (2%) or direct aortic (4%) approaches were used in patients with unsuitable iliofemoral anatomy. The primary endpoint was the composite of all-cause death or disabling stroke at 2 years. A Bayesian interim analysis was prespecified when 1,400 patients had reached the 1 year follow-up. Consistent with the prior studies, TAVI was non-inferior to SAVR for the primary endpoint (12.6% vs. 14.0%, difference -1.4 percentage points, 95% Bayesian credible interval for difference (BCI) -5.2 to 2.3%, posterior probability of noninferiority >0.999). Each procedure was associated with different adverse events with higher moderate or severe PVR (5.3% vs. 0.6%, difference 4.7 percentage points, 95% BCI 2.8 to 6.8) and need for new PPI (25.9% vs. 6.6%, difference 18.9 percentage points, 95% BCI 15.9 to 22.7) in the TAVI group, and higher rates of acute kidney injury (1.7% vs. 4.4%, difference -2.7 percentage points, 95% BCI -4.4 to -1.0) and atrial fibrillation (12.9% vs. 43.4%. difference -30.5 percentage points, 95% BCI -34.7 to -26.4) in the SAVR group. At 2 years, there were no between-group differences in terms of all-cause death (11.4% vs. 11.6%), major stroke (2.6% vs. 4.5%), or myocardial infarction (2.8% vs. 2.2%) (Table 13, Table 14and Table 15).
NOTION (CoreValve, Intermediate/low risk)
The NOTION trial was a multicentre trial that randomized all comers with severe AS (age ≥70 years and no evidence of significant coronary artery disease) to TAVI with the CoreValve self-expanding valve system (Medtronic) or SAVR18. Thyregod HG, Steinbruchel DA, Ihlemann N, Nissen H, Kjeldsen BJ, Petursson P, Chang Y, Franzen OW, Engstrom T, Clemmensen P, Hansen PB, Andersen LW, Olsen PS, Sondergaard L. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65(20):2184-94. Link. The default access was femoral (96.5%), with left subclavian access as the second option (3.5%). A total of 280 patients (mean age 79 years) were included, and the majority of patients (81.8%) were considered low-risk patients. The primary endpoint was the composite of all-cause death, stroke, or myocardial infarction at 1 year. There were no differences between TAVI and SAVR for the primary endpoint (13.1% vs. 16.3%, P for superiority = 0.43) or any of its components at 1 year. At 30 days, there were more patients with life-threatening or major bleeding (11.3% vs. 20.9%, P=0.03), cardiogenic shock (4.2% vs. 10.4%, P=0.05), acute kidney injury (0.7% vs. 6.7%, P=0.01), and new-onset atrial fibrillation (16.9% vs. 57.8%, P<0.001) in the SAVR cohort, and more new PPI (34.1% vs. 1.6%, P<0.001) in the TAVI cohort. Moderate or severe PVR occurred more frequently after TAVI than SAVR at 3 months, and the difference remained stable during the first year (15.7% vs. 0.9%, P<0.001). The results were largely consistent at 5 years, with the incidence of the primary endpoint of 38.0% in the TAVI group and 36.3% in the SAVR group (P=0.86) (Table 13, Table 14and Table 15)170. Thyregod HGH, Ihlemann N, Jorgensen TH, Nissen H, Kjeldsen BJ, Petursson P, Chang Y, Franzen OW, Engstrom T, Clemmensen P, Hansen PB, Andersen LW, Steinbruchel DA, Olsen PS, Sondergaard L. Five-Year Clinical and Echocardiographic Outcomes from the Nordic Aortic Valve Intervention (NOTION) Randomized Clinical Trial in Lower Surgical Risk Patients. Circulation. 2019. Link.
PARTNER III (SAPIEN 3, Low risk)
The PARTNER 3 trial was a randomized trial (n=1,000) that compared transfemoral TAVI using the SAPIEN 3 balloon-expandable valve system with SAVR in low-risk patients (mean age 73 years)19. Mack MJ, Leon MB, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Pibarot P, Leipsic J, Hahn RT, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Pocock SJ, Alu MC, Webb JG, Smith CR. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019. Link. The primary endpoint was the composite of all-cause death, any stroke, or repeat hospitalization at 1 year. The Kaplan-Meier estimate of the rate of the primary endpoint was lower in the TAVI group than in the SAVR group (8.5% vs. 15.1%, absolute difference -6.6 percentage points, 95%CI -10.8 to -2.5, P for noninferiority <0.001, HR 0.54, 95% CI 0.37 to 0.79, P for superiority =0.001). At 30 days, TAVI resulted in lower rates of stroke (0.6% vs. 2.4%, P=0.02) and new-onset atrial fibrillation (5.0% vs. 39.5%, P<0.001) than SAVR. Of note, there were no significant between-group differences in major vascular complications (2.2% vs. 1.5%, HR 1.44, 95% CI 0.56 to 3.73) and new PPI (6.5% vs. 4.0%, HR 1.65, 95% CI 0.92 to 2.95). While the percentage of moderate or severe PVR was low and not statistically different between the groups (0.8% vs. 0.2%, P=0.38), mild PVR was more frequent after TAVI than SAVR (28.8% vs. 4.2%, P<0.001). The percentage of severe prosthesis-patient mismatch at 30 days was low and similar between the groups (4.6% vs. 6.3%, P=0.30)171. Pibarot P, Salaun E, Dahou A, Avenatti E, Guzzetti E, Annabi MS, Toubal O, Bernier M, Beaudoin J, Ong G, Ternacle J, Krapf L, Thourani VH, Makkar R, Kodali SK, Russo M, Kapadia SR, Malaisrie SC, Cohen DJ, Leipsic J, Blanke P, Williams MR, McCabe JM, Brown DL, Babaliaros V, Goldman S, Szeto WY, Genereux P, Pershad A, Alu MC, Xu K, Rogers E, Webb JG, Smith CR, Mack MJ, Leon MB, Hahn RT, Investigators P. Echocardiographic Results of Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients: The PARTNER 3 Trial. Circulation. 2020. Link (Table 13, Table 14and Table 15).
In the Evolut Low Risk trial, 1,468 low-risk patients (mean age 74 years) were randomized to TAVI or SAVR20. Popma JJ, Deeb GM, Yakubov SJ, Mumtaz M, Gada H, O’Hair D, Bajwa T, Heiser JC, Merhi W, Kleiman NS, Askew J, Sorajja P, Rovin J, Chetcuti SJ, Adams DH, Teirstein PS, Zorn GL, 3rd, Forrest JK, Tchetche D, Resar J, Walton A, Piazza N, Ramlawi B, Robinson N, Petrossian G, Gleason TG, Oh JK, Boulware MJ, Qiao H, Mugglin AS, Reardon MJ. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019. Link. TAVI was performed with the CoreValve (3.6%), Evolut R (74.1%), or Evolut PRO (22.3%) self-expanding valve systems (Medtronic). Transfemoral access was the default strategy (99.0%); alternative access included direct aortic (0.4%) and subclavian (0.6%) approaches. The primary endpoint was the composite of all-cause death or disabling stroke at 2 years. When 850 patients had reached 1-year follow-up, data were analysed using Bayesian methods. At 2 years, TAVI met non-inferiority compared to SAVR in terms of the primary endpoint (5.3% vs. 6.7%, difference -1.4 percentage points, 95% BCI -4.0 to 2.1, posterior probability of noninferiority >0.999). At 30 days, TAVI resulted in a lower incidence of disabling stroke (0.5% vs. 1.7%, difference -1.2, 95% BCI -2.4 to -0.2), bleeding complications (7.7% vs. 35.4%. difference -5.1, 95% BCI -7.5 to -2.9), acute kidney injury (0.9% vs. 2.8%, difference -1.8, 95% BCI -3.4 to -0.5), and new-onset atrial fibrillation (7.7% vs. 35.4%, difference -27.7, 95% BCI -31.8 to -23.6) as compared to SAVR. Conversely, the rates of new PPI (17.4% vs. 6.1%, difference 11.3, 95% BCI 8.0 to 14.7) were higher in the TAVI group than in the SAVR group. Moderate or severe PVR was present at 30 days in 3.5% of the TAVI group and in 0.5% in the SAVR group. Severe prosthesis-patient mismatch occurred at 1 year in 1.8% of the TAVI group and in 8.2% of the SAVR group (Table 13, Table 14and Table 15).
Durability Data
With accumulating evidence, TAVI is increasingly used among younger and lower-risk patients, who have longer life-expectancy. Favourable data on the durability of THVs have been reported from the randomized clinical trials and large scale real-world registries, but are limited up to 8 years (Table 16), , , , , 172. Didier R, Eltchaninoff H, Donzeau-Gouge P, Chevreul K, Fajadet J, Leprince P, Leguerrier A, Lievre M, Prat A, Teiger E, Lefevre T, Tchetche D, Carrie D, Himbert D, Albat B, Cribier A, Sudre A, Blanchard D, Rioufol G, Collet F, Houel R, Dos Santos P, Meneveau N, Ghostine S, Manigold T, Guyon P, Cuisset T, Le Breton H, Delepine S, Favereau X, Souteyrand G, Ohlmann P, Doisy V, Lognone T, Gommeaux A, Claudel JP, Bourlon F, Bertrand B, Iung B, Gilard M. Five-Year Clinical Outcome and Valve Durability After Transcatheter Aortic Valve Replacement in High-Risk Patients. Circulation. 2018;138(23):2597-2607. Link173. Blackman DJ, Saraf S, MacCarthy PA, Myat A, Anderson SG, Malkin CJ, Cunnington MS, Somers K, Brennan P, Manoharan G, Parker J, Aldalati O, Brecker SJ, Dowling C, Hoole SP, Dorman S, Mullen M, Kennon S, Jerrum M, Chandrala P, Roberts DH, Tay J, Doshi SN, Ludman PF, Fairbairn TA, Crowe J, Levy RD, Banning AP, Ruparelia N, Spence MS, Hildick-Smith D. Long-Term Durability of Transcatheter Aortic Valve Prostheses. J Am Coll Cardiol. 2019;73(5):537-545. Link174. Sondergaard L, Ihlemann N, Capodanno D, Jorgensen TH, Nissen H, Kjeldsen BJ, Chang Y, Steinbruchel DA, Olsen PS, Petronio AS, Thyregod HGH. Durability of Transcatheter and Surgical Bioprosthetic Aortic Valves in Patients at Lower Surgical Risk. J Am Coll Cardiol. 2019;73(5):546-553. Link175. Gleason TG, Reardon MJ, Popma JJ, Deeb GM, Yakubov SJ, Lee JS, Kleiman NS, Chetcuti S, Hermiller JB, Jr., Heiser J, Merhi W, Zorn GL, 3rd, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte JV, Mumtaz M, Oh JK, Huang J, Adams DH, CoreValve USPHRTCI. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J Am Coll Cardiol. 2018;72(22):2687-2696. Link176. Testa L, Latib A, Brambilla N, De Marco F, Fiorina C, Adamo M, Giannini C, Angelillis M, Barbanti M, Sgroi C, Poli A, Ferrara E, Bruschi G, Russo CF, Matteo M, De Felice F, Musto C, Curello S, Colombo A, Tamburino C, Petronio AS, Bedogni F. Long-term clinical outcome and performance of transcatheter aortic valve replacement with a self-expandable bioprosthesis. Eur Heart J. 2020;41(20):1876-1886. Link177. Pibarot P, Ternacle J, Jaber WA, Salaun E, Dahou A, Asch FM, Weissman NJ, Rodriguez L, Xu K, Annabi MS, Guzzetti E, Beaudoin J, Bernier M, Leipsic J, Blanke P, Clavel MA, Rogers E, Alu MC, Douglas PS, Makkar R, Miller DC, Kapadia SR, Mack MJ, Webb JG, Kodali SK, Smith CR, Herrmann HC, Thourani VH, Leon MB, Hahn RT, Investigators P. Structural Deterioration of Transcatheter Versus Surgical Aortic Valve Bioprostheses in the PARTNER-2 Trial. J Am Coll Cardiol. 2020;76(16):1830-1843. Link. The rates of structural valve deterioration (SVD) and bioprosthetic valve failure (BVF) between 5 and 8 years after TAVI ranged from 3.8% to 18.6% and 2.5% to 7.5%, depending on the definitions, the timing, and THV used.
When compared to SAVR valves, the durability of THVs were largely comparable up to 6 years. In the US CoreValve High Risk trial with use of the early-generation self-expanding device (CoreValve, Medtronic), the incidence of severe SVD was rare and similar between TAVI and SAVR at 5 years (0.8% vs. 1.7%, P=0.322). Although moderate SVD was more common after SAVR (9.2% vs. 26.6%, P<0.001), the difference was attributable to higher gradients in certain SAVR valves which may not be truly indicative of SVD but prosthesis-patient mismatch175. Gleason TG, Reardon MJ, Popma JJ, Deeb GM, Yakubov SJ, Lee JS, Kleiman NS, Chetcuti S, Hermiller JB, Jr., Heiser J, Merhi W, Zorn GL, 3rd, Tadros P, Robinson N, Petrossian G, Hughes GC, Harrison JK, Conte JV, Mumtaz M, Oh JK, Huang J, Adams DH, CoreValve USPHRTCI. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J Am Coll Cardiol. 2018;72(22):2687-2696. Link. This observation was largely consistent in the NOTION trial, where the same THV was implanted in intermediate- or low-risk patients. At 6 years, moderate or severe SVD occurred more frequently after SAVR than TAVI (4.8% vs. 24.0%, P<0.001), which was primarily related to higher gradients in the SAVR group. However, even if applying the modified definitions of SVD accounting for the number of patients with an increased gradient at the time of the implantation, SVD more frequently occurred after SAVR than TAVI (1.4% vs. 12.4%, P<0.001). In terms of BVF, the rate was low and similar for both groups through 6 years (7.5% vs. 6.7%, P=0.89)174. Sondergaard L, Ihlemann N, Capodanno D, Jorgensen TH, Nissen H, Kjeldsen BJ, Chang Y, Steinbruchel DA, Olsen PS, Petronio AS, Thyregod HGH. Durability of Transcatheter and Surgical Bioprosthetic Aortic Valves in Patients at Lower Surgical Risk. J Am Coll Cardiol. 2019;73(5):546-553. Link. In these two studies, SVD and BVF were defined according to a consensus statement from the European cardiovascular community (Table 17)178. Capodanno D, Petronio AS, Prendergast B, Eltchaninoff H, Vahanian A, Modine T, Lancellotti P, Sondergaard L, Ludman PF, Tamburino C, Piazza N, Hancock J, Mehilli J, Byrne RA, Baumbach A, Kappetein AP, Windecker S, Bax J, Haude M. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2017;38(45):3382-3390. Link. However, as shown above, the definitions had inherent limitations that SVD did not necessarily require a morphological/hemodynamical change over time, and higher gradients, which may not be attributable to SVD, largely contributed to the higher rates of SVD in the SAVR group. Thus, in a recent dedicated analysis of the populations from the PARTNER 2 trial and the PARTNER 2 SAPIEN 3 intermediate-risk observational study, new standardized definitions of SVD and BVF (Table 18) based on identification of structural and hemodynamic valve deterioration during echocardiographic follow-up were used177. Pibarot P, Ternacle J, Jaber WA, Salaun E, Dahou A, Asch FM, Weissman NJ, Rodriguez L, Xu K, Annabi MS, Guzzetti E, Beaudoin J, Bernier M, Leipsic J, Blanke P, Clavel MA, Rogers E, Alu MC, Douglas PS, Makkar R, Miller DC, Kapadia SR, Mack MJ, Webb JG, Kodali SK, Smith CR, Herrmann HC, Thourani VH, Leon MB, Hahn RT, Investigators P. Structural Deterioration of Transcatheter Versus Surgical Aortic Valve Bioprostheses in the PARTNER-2 Trial. J Am Coll Cardiol. 2020;76(16):1830-1843. Link. In the study, the second-generation SAPIEN XT THV had a higher rate of SVD (9.5% vs. 3.5%, P<0.001) than SAVR valves, whereas the third-generation SAPIEN 3 THV had a similar rate of SVD (3.9% vs. 3.5%, P=0.65) compared with a propensity-matched SAVR cohort throughout 5 years. Similarly, the 5-year cumulative incidence of all-cause BVF was higher in SAPIEN XT TAVI than SAVR (4.7% vs. 1.3%, P=0.004), while the rate was numerically but not statistically higher in SAPIEN 3 TAVI than SAVR (2.6% vs. 1.3%, P=0.083)177. Pibarot P, Ternacle J, Jaber WA, Salaun E, Dahou A, Asch FM, Weissman NJ, Rodriguez L, Xu K, Annabi MS, Guzzetti E, Beaudoin J, Bernier M, Leipsic J, Blanke P, Clavel MA, Rogers E, Alu MC, Douglas PS, Makkar R, Miller DC, Kapadia SR, Mack MJ, Webb JG, Kodali SK, Smith CR, Herrmann HC, Thourani VH, Leon MB, Hahn RT, Investigators P. Structural Deterioration of Transcatheter Versus Surgical Aortic Valve Bioprostheses in the PARTNER-2 Trial. J Am Coll Cardiol. 2020;76(16):1830-1843. Link.
Table 17
Definitions of structural valve deterioration and bioprosthetic valve failure according to a ESC/EACPI/EACTS consensus statement
Although the performance and durability of TAVI valves have been excellent and comparable to SAVR bioprostheses throughout 5-8 years, it should be noted that bioprosthetic valve deterioration mostly occurs >8-10 years after SAVR. Furthermore, although the reported durability of surgical bioprosthesis is >85% at 10 years, most studies have used reoperation instead of valve performance to define valve durability, which may have led to underestimation of the true incidence of SVD after SAVR (Table 19)179. Rodriguez-Gabella T, Voisine P, Puri R, Pibarot P, Rodes-Cabau J. Aortic Bioprosthetic Valve Durability: Incidence, Mechanisms, Predictors, and Management of Surgical and Transcatheter Valve Degeneration. J Am Coll Cardiol. 2017;70(8):1013-1028. Link. Thus, longer-term follow-up data (>8-10 years) using the uniform definitions of SVD and BVF are needed for both TAVI and SAVR valves.
Bioprosthetic valve thrombosis is relatively rare but considered one of the important causes of SVD. Conventionally, bioprostheses have been considered less thrombogenic than mechanical heart valves. However, recent ongoing evaluations of the performance and durability of bioprostheses and the advent of MDCT as a novel diagnostic modality pointed to the issue of bioprosthetic valve thrombosis in various types of THVs as well as SAVR valves, 180. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, Trento A, Guyton R, Babaliaros V, Williams M, Jilaihawi H, Kodali S, George I, Lu M, McCabe JM, Friedman J, Smalling R, Wong SC, Yazdani S, Bhatt DL, Bax J, Kapadia S, Herrmann HC, Mack M, Leon MB. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75(24):3003-3015. Link181. Blanke P, Leipsic JA, Popma JJ, Yakubov SJ, Deeb GM, Gada H, Mumtaz M, Ramlawi B, Kleiman NS, Sorajja P, Askew J, Meduri CU, Kauten J, Melnitchouk S, Inglessis I, Huang J, Boulware M, Reardon MJ, Evolut Low Risk LTISI. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75(19):2430-2442. Link. Bioprosthetic valve thrombosis typically includes two different entities - clinical valve thrombosis and subclinical leaflet thrombosis. Clinical valve thrombosis is defined by the detection of valve dysfunction secondary to thrombosis or a mobile mass suspicious of thrombus detected on the prosthesis much alike mechanical valve thrombosis on clinical grounds, 182. Latib A, Naganuma T, Abdel-Wahab M, Danenberg H, Cota L, Barbanti M, Baumgartner H, Finkelstein A, Legrand V, de Lezo JS, Kefer J, Messika-Zeitoun D, Richardt G, Stabile E, Kaleschke G, Vahanian A, Laborde JC, Leon MB, Webb JG, Panoulas VF, Maisano F, Alfieri O, Colombo A. Treatment and clinical outcomes of transcatheter heart valve thrombosis. Circ Cardiovasc Interv. 2015;8(4). Link183. Jose J, Sulimov DS, El-Mawardy M, Sato T, Allali A, Holy EW, Becker B, Landt M, Kebernik J, Schwarz B, Richardt G, Abdel-Wahab M. Clinical Bioprosthetic Heart Valve Thrombosis After Transcatheter Aortic Valve Replacement: Incidence, Characteristics, and Treatment Outcomes. JACC Cardiovasc Interv. 2017;10(7):686-697. Link. In contrast, subclinical leaflet thrombosis is most often an incidental finding, characterized by a thin layer of thrombus covering the aortic side of the leaflets as assessed by MDCT. This entity is further subcategorized into hypo-attenuated leaflet thickening (HALT) without leaflet motion abnormality and reduced leaflet motion (RLM), , , , , , , , , , 180. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, Trento A, Guyton R, Babaliaros V, Williams M, Jilaihawi H, Kodali S, George I, Lu M, McCabe JM, Friedman J, Smalling R, Wong SC, Yazdani S, Bhatt DL, Bax J, Kapadia S, Herrmann HC, Mack M, Leon MB. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75(24):3003-3015. Link181. Blanke P, Leipsic JA, Popma JJ, Yakubov SJ, Deeb GM, Gada H, Mumtaz M, Ramlawi B, Kleiman NS, Sorajja P, Askew J, Meduri CU, Kauten J, Melnitchouk S, Inglessis I, Huang J, Boulware M, Reardon MJ, Evolut Low Risk LTISI. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75(19):2430-2442. Link184. Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, De Backer O, Asch FM, Ruiz CE, Olsen NT, Trento A, Friedman J, Berman D, Cheng W, Kashif M, Jelnin V, Kliger CA, Guo H, Pichard AD, Weissman NJ, Kapadia S, Manasse E, Bhatt DL, Leon MB, Sondergaard L. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med. 2015;373(21):2015-24. Link185. Pache G, Schoechlin S, Blanke P, Dorfs S, Jander N, Arepalli CD, Gick M, Buettner HJ, Leipsic J, Langer M, Neumann FJ, Ruile P. Early hypo-attenuated leaflet thickening in balloon-expandable transcatheter aortic heart valves. Eur Heart J. 2016;37(28):2263-71. Link186. Hansson NC, Grove EL, Andersen HR, Leipsic J, Mathiassen ON, Jensen JM, Jensen KT, Blanke P, Leetmaa T, Tang M, Krusell LR, Klaaborg KE, Christiansen EH, Terp K, Terkelsen CJ, Poulsen SH, Webb J, Botker HE, Norgaard BL. Transcatheter Aortic Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications. J Am Coll Cardiol. 2016;68(19):2059-2069. Link187. Chakravarty T, Sondergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, Jilaihawi H, Shiota T, Abramowitz Y, Jorgensen TH, Rami T, Israr S, Fontana G, de Knegt M, Fuchs A, Lyden P, Trento A, Bhatt DL, Leon MB, Makkar RR. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. 2017;389(10087):2383-2392. Link188. Vollema EM, Kong WKF, Katsanos S, Kamperidis V, van Rosendael PJ, van der Kley F, de Weger A, Ajmone Marsan N, Delgado V, Bax JJ. Transcatheter aortic valve thrombosis: the relation between hypo-attenuated leaflet thickening, abnormal valve haemodynamics, and stroke. Eur Heart J. 2017;38(16):1207-1217. Link189. Marwan M, Mekkhala N, Goller M, Rother J, Bittner D, Schuhbaeck A, Hell M, Muschiol G, Kolwelter J, Feyrer R, Schlundt C, Achenbach S, Arnold M. Leaflet thrombosis following transcatheter aortic valve implantation. J Cardiovasc Comput Tomogr. 2018;12(1):8-13. Link190. Yanagisawa R, Hayashida K, Yamada Y, Tanaka M, Yashima F, Inohara T, Arai T, Kawakami T, Maekawa Y, Tsuruta H, Itabashi Y, Murata M, Sano M, Okamoto K, Yoshitake A, Shimizu H, Jinzaki M, Fukuda K. Incidence, Predictors, and Mid-Term Outcomes of Possible Leaflet Thrombosis After TAVR. JACC Cardiovasc Imaging. 2016. Link191. Dalen M, Sartipy U, Cederlund K, Franco-Cereceda A, Svensson A, Themudo R, Svenarud P, Bacsovics Brolin E. Hypo-Attenuated Leaflet Thickening and Reduced Leaflet Motion in Sutureless Bioprosthetic Aortic Valves. J Am Heart Assoc. 2017;6(8). Link192. Ruile P, Jander N, Blanke P, Schoechlin S, Reinohl J, Gick M, Rothe J, Langer M, Leipsic J, Buettner HJ, Neumann FJ, Pache G. Course of early subclinical leaflet thrombosis after transcatheter aortic valve implantation with or without oral anticoagulation. Clin Res Cardiol. 2017;106(2):85-95. Link.
Limited data are currently available on clinical valve thrombosis after TAVI (Table 20). In a retrospective multicentre study including 4,266 patients treated with the SAPIEN/SAPIEN XT THV or the CoreValve THV, 26 (0.61%) cases of clinical valve thrombosis at a median follow-up of 181 days were reported182. Latib A, Naganuma T, Abdel-Wahab M, Danenberg H, Cota L, Barbanti M, Baumgartner H, Finkelstein A, Legrand V, de Lezo JS, Kefer J, Messika-Zeitoun D, Richardt G, Stabile E, Kaleschke G, Vahanian A, Laborde JC, Leon MB, Webb JG, Panoulas VF, Maisano F, Alfieri O, Colombo A. Treatment and clinical outcomes of transcatheter heart valve thrombosis. Circ Cardiovasc Interv. 2015;8(4). Link. Another retrospective single-centre study reported an overall incidence of 2.8% (n=18) among 642 patients treated with various types of THVs at a median follow-up period of 181 days183. Jose J, Sulimov DS, El-Mawardy M, Sato T, Allali A, Holy EW, Becker B, Landt M, Kebernik J, Schwarz B, Richardt G, Abdel-Wahab M. Clinical Bioprosthetic Heart Valve Thrombosis After Transcatheter Aortic Valve Replacement: Incidence, Characteristics, and Treatment Outcomes. JACC Cardiovasc Interv. 2017;10(7):686-697. Link. In both studies, OAC was suggested to be effective for the treatment of valve thrombosis. In the latter study, the absence of OAC use, balloon-expandable valves, valve-in-valve procedures, and obesity appeared to be predictive for clinical valve thrombosis.
The prevalence of subclinical leaflet thrombosis was variably reported ranging from 7% to 40%, depending on the timing, THV type, and antithrombotic regimen (Table 20) , , , , , , , , , , 180. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, Trento A, Guyton R, Babaliaros V, Williams M, Jilaihawi H, Kodali S, George I, Lu M, McCabe JM, Friedman J, Smalling R, Wong SC, Yazdani S, Bhatt DL, Bax J, Kapadia S, Herrmann HC, Mack M, Leon MB. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75(24):3003-3015. Link181. Blanke P, Leipsic JA, Popma JJ, Yakubov SJ, Deeb GM, Gada H, Mumtaz M, Ramlawi B, Kleiman NS, Sorajja P, Askew J, Meduri CU, Kauten J, Melnitchouk S, Inglessis I, Huang J, Boulware M, Reardon MJ, Evolut Low Risk LTISI. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75(19):2430-2442. Link184. Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, De Backer O, Asch FM, Ruiz CE, Olsen NT, Trento A, Friedman J, Berman D, Cheng W, Kashif M, Jelnin V, Kliger CA, Guo H, Pichard AD, Weissman NJ, Kapadia S, Manasse E, Bhatt DL, Leon MB, Sondergaard L. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med. 2015;373(21):2015-24. Link185. Pache G, Schoechlin S, Blanke P, Dorfs S, Jander N, Arepalli CD, Gick M, Buettner HJ, Leipsic J, Langer M, Neumann FJ, Ruile P. Early hypo-attenuated leaflet thickening in balloon-expandable transcatheter aortic heart valves. Eur Heart J. 2016;37(28):2263-71. Link186. Hansson NC, Grove EL, Andersen HR, Leipsic J, Mathiassen ON, Jensen JM, Jensen KT, Blanke P, Leetmaa T, Tang M, Krusell LR, Klaaborg KE, Christiansen EH, Terp K, Terkelsen CJ, Poulsen SH, Webb J, Botker HE, Norgaard BL. Transcatheter Aortic Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications. J Am Coll Cardiol. 2016;68(19):2059-2069. Link187. Chakravarty T, Sondergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, Jilaihawi H, Shiota T, Abramowitz Y, Jorgensen TH, Rami T, Israr S, Fontana G, de Knegt M, Fuchs A, Lyden P, Trento A, Bhatt DL, Leon MB, Makkar RR. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. 2017;389(10087):2383-2392. Link188. Vollema EM, Kong WKF, Katsanos S, Kamperidis V, van Rosendael PJ, van der Kley F, de Weger A, Ajmone Marsan N, Delgado V, Bax JJ. Transcatheter aortic valve thrombosis: the relation between hypo-attenuated leaflet thickening, abnormal valve haemodynamics, and stroke. Eur Heart J. 2017;38(16):1207-1217. Link189. Marwan M, Mekkhala N, Goller M, Rother J, Bittner D, Schuhbaeck A, Hell M, Muschiol G, Kolwelter J, Feyrer R, Schlundt C, Achenbach S, Arnold M. Leaflet thrombosis following transcatheter aortic valve implantation. J Cardiovasc Comput Tomogr. 2018;12(1):8-13. Link190. Yanagisawa R, Hayashida K, Yamada Y, Tanaka M, Yashima F, Inohara T, Arai T, Kawakami T, Maekawa Y, Tsuruta H, Itabashi Y, Murata M, Sano M, Okamoto K, Yoshitake A, Shimizu H, Jinzaki M, Fukuda K. Incidence, Predictors, and Mid-Term Outcomes of Possible Leaflet Thrombosis After TAVR. JACC Cardiovasc Imaging. 2016. Link191. Dalen M, Sartipy U, Cederlund K, Franco-Cereceda A, Svensson A, Themudo R, Svenarud P, Bacsovics Brolin E. Hypo-Attenuated Leaflet Thickening and Reduced Leaflet Motion in Sutureless Bioprosthetic Aortic Valves. J Am Heart Assoc. 2017;6(8). Link192. Ruile P, Jander N, Blanke P, Schoechlin S, Reinohl J, Gick M, Rothe J, Langer M, Leipsic J, Buettner HJ, Neumann FJ, Pache G. Course of early subclinical leaflet thrombosis after transcatheter aortic valve implantation with or without oral anticoagulation. Clin Res Cardiol. 2017;106(2):85-95. Link. Importantly, the clinical relevance of this entity remains uncertain. Subclinical leaflet thrombosis has been associated with a significant but not clinically meaningful increase in mean aortic valve gradients in some studies, , , 180. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, Trento A, Guyton R, Babaliaros V, Williams M, Jilaihawi H, Kodali S, George I, Lu M, McCabe JM, Friedman J, Smalling R, Wong SC, Yazdani S, Bhatt DL, Bax J, Kapadia S, Herrmann HC, Mack M, Leon MB. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75(24):3003-3015. Link185. Pache G, Schoechlin S, Blanke P, Dorfs S, Jander N, Arepalli CD, Gick M, Buettner HJ, Leipsic J, Langer M, Neumann FJ, Ruile P. Early hypo-attenuated leaflet thickening in balloon-expandable transcatheter aortic heart valves. Eur Heart J. 2016;37(28):2263-71. Link186. Hansson NC, Grove EL, Andersen HR, Leipsic J, Mathiassen ON, Jensen JM, Jensen KT, Blanke P, Leetmaa T, Tang M, Krusell LR, Klaaborg KE, Christiansen EH, Terp K, Terkelsen CJ, Poulsen SH, Webb J, Botker HE, Norgaard BL. Transcatheter Aortic Valve Thrombosis: Incidence, Predisposing Factors, and Clinical Implications. J Am Coll Cardiol. 2016;68(19):2059-2069. Link187. Chakravarty T, Sondergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, Jilaihawi H, Shiota T, Abramowitz Y, Jorgensen TH, Rami T, Israr S, Fontana G, de Knegt M, Fuchs A, Lyden P, Trento A, Bhatt DL, Leon MB, Makkar RR. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. 2017;389(10087):2383-2392. Link, but not in the other studies, , 181. Blanke P, Leipsic JA, Popma JJ, Yakubov SJ, Deeb GM, Gada H, Mumtaz M, Ramlawi B, Kleiman NS, Sorajja P, Askew J, Meduri CU, Kauten J, Melnitchouk S, Inglessis I, Huang J, Boulware M, Reardon MJ, Evolut Low Risk LTISI. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75(19):2430-2442. Link184. Makkar RR, Fontana G, Jilaihawi H, Chakravarty T, Kofoed KF, De Backer O, Asch FM, Ruiz CE, Olsen NT, Trento A, Friedman J, Berman D, Cheng W, Kashif M, Jelnin V, Kliger CA, Guo H, Pichard AD, Weissman NJ, Kapadia S, Manasse E, Bhatt DL, Leon MB, Sondergaard L. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med. 2015;373(21):2015-24. Link190. Yanagisawa R, Hayashida K, Yamada Y, Tanaka M, Yashima F, Inohara T, Arai T, Kawakami T, Maekawa Y, Tsuruta H, Itabashi Y, Murata M, Sano M, Okamoto K, Yoshitake A, Shimizu H, Jinzaki M, Fukuda K. Incidence, Predictors, and Mid-Term Outcomes of Possible Leaflet Thrombosis After TAVR. JACC Cardiovasc Imaging. 2016. Link. Whether the presence of subclinical leaflet thrombosis leads to clinical valve thrombosis, bioprosthetic valve degeneration, or thromboembolic events remains to be investigated. Currently, only a single retrospective study, including 106 cases of RLM from the RESOLVE and SAVORY registries, has shown that RLM was significantly associated with an increased risk of cerebrovascular events187. Chakravarty T, Sondergaard L, Friedman J, De Backer O, Berman D, Kofoed KF, Jilaihawi H, Shiota T, Abramowitz Y, Jorgensen TH, Rami T, Israr S, Fontana G, de Knegt M, Fuchs A, Lyden P, Trento A, Bhatt DL, Leon MB, Makkar RR. Subclinical leaflet thrombosis in surgical and transcatheter bioprosthetic aortic valves: an observational study. Lancet. 2017;389(10087):2383-2392. Link. In a sub-study of the GALILEO randomized clinical trial, the rivaroxaban-based strategy was more effective than the antiplatelet-based strategy in reducing HALT (12.4% vs. 32.4%, difference -20.0 percentage points, 95% CI -30.9 to -8.5) and RLM (12.4% vs. 31.7%, difference -19.3, 95% CI -30.2 to -7.8); however, these effects did not translate into significant improvement in valve hemodynamic or in reductions of thromboembolic events, 163. De Backer O, Dangas GD, Jilaihawi H, Leipsic JA, Terkelsen CJ, Makkar R, Kini AS, Veien KT, Abdel-Wahab M, Kim WK, Balan P, Van Mieghem N, Mathiassen ON, Jeger RV, Arnold M, Mehran R, Guimaraes AHC, Norgaard BL, Kofoed KF, Blanke P, Windecker S, Sondergaard L, Investigators G-D. Reduced Leaflet Motion after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382(2):130-139. Link164. Dangas GD, Tijssen JGP, Wohrle J, Sondergaard L, Gilard M, Mollmann H, Makkar RR, Herrmann HC, Giustino G, Baldus S, De Backer O, Guimaraes AHC, Gullestad L, Kini A, von Lewinski D, Mack M, Moreno R, Schafer U, Seeger J, Tchetche D, Thomitzek K, Valgimigli M, Vranckx P, Welsh RC, Wildgoose P, Volkl AA, Zazula A, van Amsterdam RGM, Mehran R, Windecker S, Investigators G. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382(2):120-129. Link. Moreover, recent CT sub-studies of the randomized clinical trials suggested that subclinical leaflet thrombosis may also regress spontaneously without changing antithrombotic therapy, 180. Makkar RR, Blanke P, Leipsic J, Thourani V, Chakravarty T, Brown D, Trento A, Guyton R, Babaliaros V, Williams M, Jilaihawi H, Kodali S, George I, Lu M, McCabe JM, Friedman J, Smalling R, Wong SC, Yazdani S, Bhatt DL, Bax J, Kapadia S, Herrmann HC, Mack M, Leon MB. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75(24):3003-3015. Link181. Blanke P, Leipsic JA, Popma JJ, Yakubov SJ, Deeb GM, Gada H, Mumtaz M, Ramlawi B, Kleiman NS, Sorajja P, Askew J, Meduri CU, Kauten J, Melnitchouk S, Inglessis I, Huang J, Boulware M, Reardon MJ, Evolut Low Risk LTISI. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75(19):2430-2442. Link. As evidence is currently lacking on the incidence, clinical impact, and the optimal management, individually tailored strategies are required for patients diagnosed with bioprosthetic valve thrombosis after TAVI.
Prosthetic valve endocarditis
Prosthetic valve endocarditis (PVE) is a rare but serious complication associated with valve failure and mortality after TAVI. In a pooled cohort of all patients in the PARTNER I and II trials and continued registries193. Summers MR, Leon MB, Smith CR, Kodali SK, Thourani VH, Herrmann HC, Makkar RR, Pibarot P, Webb JG, Leipsic J, Alu MC, Crowley A, Hahn RT, Kapadia SR, Tuzcu EM, Svensson L, Cremer PC, Jaber WA. Prosthetic Valve Endocarditis After TAVR and SAVR: Insights From the PARTNER Trials. Circulation. 2019;140(24):1984-1994. Link, PVE occurred in 107 out of 8,530 patients during a mean follow-up of 2.7 years (5.06 events per 1000 person-year). The incidence was comparable between TAVI and SAVR (5.21 vs. 4.10 per 1000 person-years, P=0.44). In the national registry in Sweden194. Bjursten H, Rasmussen M, Nozohoor S, Gotberg M, Olaison L, Ruck A, Ragnarsson S. Infective endocarditis after transcatheter aortic valve implantation: a nationwide study. Eur Heart J. 2019;40(39):3263-3269. Link, 103 among 4,336 patients undergoing TAVI had definite diagnosis of endocarditis during a median follow-up of 25.1 months. The cumulative incidence was 1.4% (95% CI 1.0 to 1.8) during the first year and 0.8% (95% CI 0.6 to 1.1%) per year thereafter. Similarly, in the SWISS national TAVI registry123. Stortecky S, Heg D, Tueller D, Pilgrim T, Muller O, Noble S, Jeger R, Toggweiler S, Ferrari E, Taramasso M, Maisano F, Hoeller R, Wenaweser P, Nietlispach F, Widmer A, Huber C, Roffi M, Carrel T, Windecker S, Conen A. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;75(24):3020-3030. Link, PVE occurred in 149 patients among 7,203 patients with a median follow-up of 529 days. The incidence was 1.5% during the first year, and 0.4% per year thereafter. Across the studies, PVE was associated with poor prognosis. Future studies are needed to evaluate potential preventative measures to lower the risk of PVE after TAVI.
Randomized clinical trials: device comparison
Head-to-head comparisons of different TAVI devices are becoming increasingly important to guide device selection for individual patients. This section reviews the four recent randomized clinical trials comparing contemporary TAVI devices (Table 21), , , 195. Thiele H, Kurz T, Feistritzer HJ, Stachel G, Hartung P, Eitel I, Marquetand C, Nef H, Doerr O, Lauten A, Landmesser U, Abdel-Wahab M, Sandri M, Holzhey D, Borger M, Ince H, Oner A, Meyer-Saraei R, Wienbergen H, Fach A, Frey N, Konig IR, Vonthein R, Ruckert Y, Funkat AK, de Waha-Thiele S, Desch S. Comparison of newer generation self-expandable vs. balloon-expandable valves in transcatheter aortic valve implantation: the randomized SOLVE-TAVI trial. Eur Heart J. 2020;41(20):1890-1899. Link196. Makkar RR, Cheng W, Waksman R, Satler LF, Chakravarty T, Groh M, Abernethy W, Russo MJ, Heimansohn D, Hermiller J, Worthley S, Chehab B, Cunningham M, Matthews R, Ramana RK, Yong G, Ruiz CE, Chen C, Asch FM, Nakamura M, Jilaihawi H, Sharma R, Yoon SH, Pichard AD, Kapadia S, Reardon MJ, Bhatt DL, Fontana GP. Self-expanding intra-annular versus commercially available transcatheter heart valves in high and extreme risk patients with severe aortic stenosis (PORTICO IDE): a randomised, controlled, non-inferiority trial. Lancet. 2020;396(10252):669-683. Link197. Lanz J, Kim WK, Walther T, Burgdorf C, Mollmann H, Linke A, Redwood S, Thilo C, Hilker M, Joner M, Thiele H, Conzelmann L, Conradi L, Kerber S, Schymik G, Prendergast B, Husser O, Stortecky S, Heg D, Juni P, Windecker S, Pilgrim T, investigators SI. Safety and efficacy of a self-expanding versus a balloon-expandable bioprosthesis for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: a randomised non-inferiority trial. Lancet. 2019;394(10209):1619-1628. Link198. Tamburino C, Bleiziffer S, Thiele H, Scholtz S, Hildick-Smith D, Cunnington M, Wolf A, Barbanti M, Tchetche D, Garot P, Pagnotta P, Gilard M, Bedogni F, Van Belle E, Vasa-Nicotera M, Chieffo A, Deutsch O, Kempfert J, Sondergaard L, Butter C, Trillo-Nouche R, Lotfi S, Mollmann H, Joner M, Abdel-Wahab M, Bogaerts K, Hengstenberg C, Capodanno D. Comparison of Self-Expanding Bioprostheses for Transcatheter Aortic Valve Replacement in Patients With Symptomatic Severe Aortic Stenosis: SCOPE 2 Randomized Clinical Trial. Circulation. 2020;142(25):2431-2442. Link.
The SOLVE-TAVI trial is an investigator-initiated randomized clinical trial of 447 patients with symptomatic severe AS undergoing transfemoral TAVI comparing the Evolut R self-expanding with the SAPIEN 3 balloon-expandable transcatheter valve system195. Thiele H, Kurz T, Feistritzer HJ, Stachel G, Hartung P, Eitel I, Marquetand C, Nef H, Doerr O, Lauten A, Landmesser U, Abdel-Wahab M, Sandri M, Holzhey D, Borger M, Ince H, Oner A, Meyer-Saraei R, Wienbergen H, Fach A, Frey N, Konig IR, Vonthein R, Ruckert Y, Funkat AK, de Waha-Thiele S, Desch S. Comparison of newer generation self-expandable vs. balloon-expandable valves in transcatheter aortic valve implantation: the randomized SOLVE-TAVI trial. Eur Heart J. 2020;41(20):1890-1899. Link. The primary efficacy composite endpoint included all-cause death, stroke, moderate or severe PVR, and new PPI at 30 days. The study was powered for equivalence of the primary endpoint (equivalence margin 10% with significance level 0.05). At 30 days, the primary endpoint occurred in 28.4% of the Evolut R arm and 26.1% of the SAPIEN 3 arm, meeting the prespecified criteria of equivalence (P for equivalence = 0.04). Of note, there was a numerically higher stroke rate in the SAPIEN arm (4.7% vs. 0.5%), while the rate of moderate or severe PVR was numerically higher in the Evolut R arm (3.4% vs. 1.5%). The rate of new PPI was higher than expected by the researchers in both arms (23.0% vs. 19.2%) (Table 21).
PORTICO IDE
PORTICO IDE is a non-inferiority randomized clinical trial to evaluate the safety and efficacy of the Portico intra-annular self-expanding THV compared with any commercially available THVs (SAPIEN: 1.4%, SAPIEN XT: 7.2%, SAPIEN 3: 57.1%, CoreValve: 3.9%, Evolut R: 24.7%, and Evolut PRO: 5.8%)196. Makkar RR, Cheng W, Waksman R, Satler LF, Chakravarty T, Groh M, Abernethy W, Russo MJ, Heimansohn D, Hermiller J, Worthley S, Chehab B, Cunningham M, Matthews R, Ramana RK, Yong G, Ruiz CE, Chen C, Asch FM, Nakamura M, Jilaihawi H, Sharma R, Yoon SH, Pichard AD, Kapadia S, Reardon MJ, Bhatt DL, Fontana GP. Self-expanding intra-annular versus commercially available transcatheter heart valves in high and extreme risk patients with severe aortic stenosis (PORTICO IDE): a randomised, controlled, non-inferiority trial. Lancet. 2020;396(10252):669-683. Link. The primary safety endpoint was a composite of all-cause death, disabling stroke, life-threatening bleeding requiring transfusion, acute kidney injury requiring dialysis, or major vascular complication at 30 days. The primary efficacy endpoint was all-cause death or disabling stroke at 1 year. The non-inferiority margin was 8.5% for primary safety and 8.0% for primary efficacy endpoints. The Portico THV met non-inferiority criteria for the primary safety endpoint, which occurred in 13.8% of the Portico and in 9.6% of the commercial valve group (P for noninferiority = 0.034). At 1 year, the Portico THV also met noninferiority criteria for the primary efficacy endpoint (14.8% vs. 13.4%, P for non-inferiority = 0.006). At 2 years, rates of all-cause death (22.3% vs. 20.2%, P=0.40) or disabling stroke (3.1% vs. 5.0%, P=0.32) were similar between the groups. In terms of valve performance, the Portico THV was associated with similar mean transvalvular gradients (8.1 mmHg vs. 7.4 mmHg, P=0.18) and effective orifice area (1.86 cm2 vs. 1.76 cm2, P=0.16) as the Evolut R/PRO THV, and lower gradients and larger effective orifice area than the SAPIEN 3 THV (11.5 mmHg, P<0.001; and 1.62 cm2, P<0.001; respectively). Conversely, moderate or severe PVR occurred more frequently in the Portico group than in the SAPIEN 3 group (6.1% vs. 1.6%, P=0.016), but no difference was observed when compared with the Evolut R/PRO group (4.0%, P=0.42) (Table 21).
SCOPE I
SCOPE I is an investigator-initiated randomized trial designed to compare the early safety and efficacy of the ACURATE neo self-expanding to the SAPIEN 3 balloon-expandable valve system197. Lanz J, Kim WK, Walther T, Burgdorf C, Mollmann H, Linke A, Redwood S, Thilo C, Hilker M, Joner M, Thiele H, Conzelmann L, Conradi L, Kerber S, Schymik G, Prendergast B, Husser O, Stortecky S, Heg D, Juni P, Windecker S, Pilgrim T, investigators SI. Safety and efficacy of a self-expanding versus a balloon-expandable bioprosthesis for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: a randomised non-inferiority trial. Lancet. 2019;394(10209):1619-1628. Link. In this trial, 739 patients (aged ≥75 years) with symptomatic severe AS undergoing transfemoral TAVI deemed at increased surgical risk were enrolled. The primary composite safety and efficacy endpoint comprised all-caused death, any stroke, life-threatening or disabling bleeding, major vascular complications, coronary artery obstruction requiring intervention, acute kidney injury (stage 2 or 3), rehospitalization for valve-related symptoms or congestive heart failure, valve-related dysfunction requiring repeat procedure, moderate or severe PVR, or prosthetic valve stenosis within 30 days of the procedure. The study was powered for non-inferiority of the ACURATE neo compared with the SAPIEN 3 THV for the primary endpoint (noninferiority margin 7.7% with significance level 0.05). The primary endpoint occurred in 87 (24%) patients in the ACURATE neo and in 60 (16%) in the SAPIEN 3 group; thus, non-inferiority of the ACURATE neo was not met (P for noninferiority = 0.42). The result was largely driven by a higher rate of acute kidney injury (3% vs. 1%, P=0.034) and moderate or severe PVR (9% vs. 3%) in the ACURATE neo arm. In contrast, the incidence of all-cause death (2% vs. 1%, P=0.09) and stroke (2% vs. 3%, =0.33) did not differ between the groups. The incidence of new PPI was low and similar in both groups (10% vs. 9%, P=0.76). In terms of hemodynamic outcomes, the ACURATE neo THV was associated with larger effective orifice area (1.73 cm2 vs. 1.47 cm2, P<0.001) and lower transvalvular gradients (7 mmHg vs. 11 mmHg, P<0.001) compared with the SAPIEN 3 THV (Table 21).
SCOPE II
SCOPE II is another investigator-initiated randomized clinical trial comparing the ACURATE neo to the Evolut R/PRO self-expanding valve system198. Tamburino C, Bleiziffer S, Thiele H, Scholtz S, Hildick-Smith D, Cunnington M, Wolf A, Barbanti M, Tchetche D, Garot P, Pagnotta P, Gilard M, Bedogni F, Van Belle E, Vasa-Nicotera M, Chieffo A, Deutsch O, Kempfert J, Sondergaard L, Butter C, Trillo-Nouche R, Lotfi S, Mollmann H, Joner M, Abdel-Wahab M, Bogaerts K, Hengstenberg C, Capodanno D. Comparison of Self-Expanding Bioprostheses for Transcatheter Aortic Valve Replacement in Patients With Symptomatic Severe Aortic Stenosis: SCOPE 2 Randomized Clinical Trial. Circulation. 2020;142(25):2431-2442. Link. A total of 796 patients (aged ≥75 years) with an indication for transfemoral TAVI were enrolled in the trial. The primary endpoint, powered for non-inferiority of the ACURATE neo THV, was the composite of all-cause death or stroke at 1 year (non-inferiority margin 6% with significance level 0.05). The key secondary endpoint, powered for superiority of the ACURATE neo THV, was new PPI at 30 days. At 1 year, the primary endpoint occurred in 59 (15.8%) in the ACURATE neo and in 52 (13.9%) in the Evolut R/PRO group, with an absolute risk difference of 1.8% and a one-sided 95% upper confidence limit of 6.1% that did not meet non-inferiority of the ACURATE neo compared with the Evolut R/PRO THV (P for non-inferiority = 0.0549). No significant differences were observed in the components of the primary endpoint. However, cardiac death at 30 days (2.8% vs. 0.8%, P=0.03) and 1 year (8.4% vs. 3.9%, P=0.01), and moderate or severe PVR (10% vs. 3%, P=0.002) were increased in the ACURATE neo group. Conversely, the rate of new PPI was lower in the ACURATE neo than the Evolut R/PRO group both at 30 days (11% vs. 18%, P=0.003) and 1 year (11% vs. 18%, P=0.004). At 1 year, also new LBBB occurred less frequently in the ACURATE neo compared with the Evolut R/PRO group (14% vs. 19%, P=0.048). Of note, after these two trials (SCOPE I and II), a new iteration of the ACURATE neo (ACURATE neo 2) with an annular sealing technology was developed and now being used in clinical practice in European countries.
Emerging Indications
Valve-in-Valve
The use of bioprosthetic aortic valves in a younger population has been increasingly observed owing to the bleeding and thromboembolic risks related to the thrombogenicity of mechanical valves and life-long OAC199. Dunning J, Gao H, Chambers J, Moat N, Murphy G, Pagano D, Ray S, Roxburgh J, Bridgewater B. Aortic valve surgery: marked increases in volume and significant decreases in mechanical valve use--an analysis of 41,227 patients over 5 years from the Society for Cardiothoracic Surgery in Great Britain and Ireland National database. J Thorac Cardiovasc Surg. 2011;142(4):776-782 e3. Link. The extended durability of the newer bioprostheses as well as the possibility of performing transcatheter valve-in-valve (ViV) procedures further expedite this trend. Clinically relevant SVD of bioprostheses occurs typically at 10-15 years after valve implantation, and then, repeat intervention is typically needed for the failed bioprosthesis. Historically, redo SAVR has been the gold standard for the treatment of failed bioprostheses; however, it carries a particular risk related to the technical difficulty as well as patient’s age and comorbidities. Thus, ViV TAVI has emerged as a less invasive and attractive alternative strategy for patients with failed bioprostheses (Table 22)200. Paradis JM, Del Trigo M, Puri R, Rodes-Cabau J. Transcatheter Valve-in-Valve and Valve-in-Ring for Treating Aortic and Mitral Surgical Prosthetic Dysfunction. J Am Coll Cardiol. 2015;66(18):2019-2037. Link.
Procedural and clinical outcomes after the valve-in-valve procedure for failed surgical bioprostheses (TAV-in-SAV) have been reported from several dedicated registries, such as the VIVID registry, 201. Dvir D, Webb JG, Bleiziffer S, Pasic M, Waksman R, Kodali S, Barbanti M, Latib A, Schaefer U, Rodes-Cabau J, Treede H, Piazza N, Hildick-Smith D, Himbert D, Walther T, Hengstenberg C, Nissen H, Bekeredjian R, Presbitero P, Ferrari E, Segev A, de Weger A, Windecker S, Moat NE, Napodano M, Wilbring M, Cerillo AG, Brecker S, Tchetche D, Lefevre T, De Marco F, Fiorina C, Petronio AS, Teles RC, Testa L, Laborde JC, Leon MB, Kornowski R, Valve-in-Valve International Data Registry I. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA. 2014;312(2):162-70. Link202. Bleiziffer S, Simonato M, Webb JG, Rodes-Cabau J, Pibarot P, Kornowski R, Windecker S, Erlebach M, Duncan A, Seiffert M, Unbehaun A, Frerker C, Conzelmann L, Wijeysundera H, Kim WK, Montorfano M, Latib A, Tchetche D, Allali A, Abdel-Wahab M, Orvin K, Stortecky S, Nissen H, Holzamer A, Urena M, Testa L, Agrifoglio M, Whisenant B, Sathananthan J, Napodano M, Landi A, Fiorina C, Zittermann A, Veulemans V, Sinning JM, Saia F, Brecker S, Presbitero P, De Backer O, Sondergaard L, Bruschi G, Franco LN, Petronio AS, Barbanti M, Cerillo A, Spargias K, Schofer J, Cohen M, Munoz-Garcia A, Finkelstein A, Adam M, Serra V, Teles RC, Champagnac D, Iadanza A, Chodor P, Eggebrecht H, Welsh R, Caixeta A, Salizzoni S, Dager A, Auffret V, Cheema A, Ubben T, Ancona M, Rudolph T, Gummert J, Tseng E, Noble S, Bunc M, Roberts D, Kass M, Gupta A, Leon MB, Dvir D. Long-term outcomes after transcatheter aortic valve implantation in failed bioprosthetic valves. Eur Heart J. 2020. Link, the STS/ACC TVT registry203. Tuzcu EM, Kapadia SR, Vemulapalli S, Carroll JD, Holmes DR, Jr., Mack MJ, Thourani VH, Grover FL, Brennan JM, Suri RM, Dai D, Svensson LG. Transcatheter Aortic Valve Replacement of Failed Surgically Implanted Bioprostheses: The STS/ACC Registry. J Am Coll Cardiol. 2018;72(4):370-382. Link, the PARTNER 2 ViV registry, 204. Webb JG, Mack MJ, White JM, Dvir D, Blanke P, Herrmann HC, Leipsic J, Kodali SK, Makkar R, Miller DC, Pibarot P, Pichard A, Satler LF, Svensson L, Alu MC, Suri RM, Leon MB. Transcatheter Aortic Valve Implantation Within Degenerated Aortic Surgical Bioprostheses: PARTNER 2 Valve-in-Valve Registry. J Am Coll Cardiol. 2017;69(18):2253-2262. Link205. Webb JG, Murdoch DJ, Alu MC, Cheung A, Crowley A, Dvir D, Herrmann HC, Kodali SK, Leipsic J, Miller DC, Pibarot P, Suri RM, Wood D, Leon MB, Mack MJ. 3-Year Outcomes After Valve-in-Valve Transcatheter Aortic Valve Replacement for Degenerated Bioprostheses: The PARTNER 2 Registry. J Am Coll Cardiol. 2019;73(21):2647-2655. Link, and the CoreValve US Expanded Use study206. Deeb GM, Chetcuti SJ, Reardon MJ, Patel HJ, Grossman PM, Schreiber T, Forrest JK, Bajwa TK, O’Hair DP, Petrossian G, Robinson N, Katz S, Hartman A, Dauerman HL, Schmoker J, Khabbaz K, Watson DR, Yakubov SJ, Oh JK, Li S, Kleiman NS, Adams DH, Popma JJ. 1-Year Results in Patients Undergoing Transcatheter Aortic Valve Replacement With Failed Surgical Bioprostheses. JACC Cardiovasc Interv. 2017;10(10):1034-1044. Link. Across these studies, overall mortality ranged from 2.1% to 7.6% at 30 days and 11.7% to 16.8% at 1 year among elderly patients (mean age 77-79 years) at an increased surgical risk (mean STS-PROM 7-10%). In a recent meta-analysis including 5,553 patients from 24 studies who underwent TAV-in-SAV (mean STS-PROM 7.84 ± 5.14)207. Mahmoud AN, Gad MM, Elgendy IY, Mahmoud AA, Taha Y, Elgendy AY, Ahuja KR, Saad AM, Simonato M, McCabe JM, Reisman M, Kapadia SR, Dvir D. Systematic review and meta-analysis of valve-in-valve transcatheter aortic valve replacement in patients with failed bioprosthetic aortic valves. EuroIntervention. 2020;16(7):539-548. Link, the procedure was successful in 95%. At 30 days, all-cause death occurred in 5%, stroke in 2%, myocardial infarction in 1%, new PPI in 6%, and significant PVR in 7%. At 1 year, the incidence of all-cause death was 12%. Interestingly, in the PARTNER 2 ViV registry, a remarkable reduction in mortality from the initial registry to the continued access registry at 30 days (8.3% vs. 0.7%, P<0.0001) and at 1 year (19.8% vs. 9.8%, P=0.006) was observed, potentially due to a learning curve and patient selection204. Webb JG, Mack MJ, White JM, Dvir D, Blanke P, Herrmann HC, Leipsic J, Kodali SK, Makkar R, Miller DC, Pibarot P, Pichard A, Satler LF, Svensson L, Alu MC, Suri RM, Leon MB. Transcatheter Aortic Valve Implantation Within Degenerated Aortic Surgical Bioprostheses: PARTNER 2 Valve-in-Valve Registry. J Am Coll Cardiol. 2017;69(18):2253-2262. Link. The PARTNER 2 ViV registry recently reported 3-year follow-up data with favourable survival (32.7%), sustained improved hemodynamic status (mean transvalvular gradients:16.6 mmHg, mean effective orifice area: 1.15 cm2, moderate or severe PVR: 2.5%), and good functional (NYHA I or II: 86%) and quality-of-life (average increase in the KCCQ-OS score: 30.0) outcomes up to 3 years205. Webb JG, Murdoch DJ, Alu MC, Cheung A, Crowley A, Dvir D, Herrmann HC, Kodali SK, Leipsic J, Miller DC, Pibarot P, Suri RM, Wood D, Leon MB, Mack MJ. 3-Year Outcomes After Valve-in-Valve Transcatheter Aortic Valve Replacement for Degenerated Bioprostheses: The PARTNER 2 Registry. J Am Coll Cardiol. 2019;73(21):2647-2655. Link.
Comparative data between TAV-in-SAV versus redo SAVR for the treatment of failed bioprostheses remain scarce. In a meta-analysis including 227 TAV-in-SAV patients and 262 redo SAVR patients from four observational studies, clinical outcomes at 30 days were similar between the groups in terms of mortality (5% vs. 4%, OR 1.08, 95% CI 0.44 to 2.62), stroke (2% vs. 2%, OR 1.00, 95% CI 0.28 to 3.59), and acute kidney injury requiring dialysis (7% vs. 10%, OR 0.80, 95% CI 0.36 to 1.77)208. Neupane S, Singh H, Lammer J, Othman H, Yamasaki H, Rosman HS, Bossone E, Mehta RH, Eggebrecht H. Meta-Analysis of Transcatheter Valve-in-Valve Implantation Versus Redo Aortic Valve Surgery for Bioprosthetic Aortic Valve Dysfunction. Am J Cardiol. 2018;121(12):1593-1600. Link. Similarly, in a propensity-matched cohort including 78 matched pairs209. Spaziano M, Mylotte D, Theriault-Lauzier P, De Backer O, Sondergaard L, Bosmans J, Debry N, Modine T, Barbanti M, Tamburino C, Sinning JM, Grube E, Nickenig G, Mellert F, Bleiziffer S, Lange R, de Varennes B, Lachapelle K, Martucci G, Piazza N. Transcatheter aortic valve implantation versus redo surgery for failing surgical aortic bioprostheses: a multicentre propensity score analysis. EuroIntervention. 2017;13(10):1149-1156. Link, the incidence of all-cause death (3.9% vs. 6.4%, P=0.49 at 30 days; 12.3% vs. 13.1%. P=0.80 at 1 year) and stroke (1.3% vs. 0%, P=1.0 at 30 days) were comparable between TAV-in-SAV and redo SAVR. Acute kidney injury requiring dialysis was numerically lower (3.8% vs. 11.5%, P=0.13) and the length of hospital stay was significantly shorter (9 days vs. 12 days, P=0.001) after TAV-in-SAV. More recently, TAV-in-SAV was associated with a lower risk of in-hospital adverse composite outcome of all-cause death, myocardial infarction, stroke, and acute kidney injury compared with redo SAVR (14.1% vs. 25.4%, P=0.018) in another propensity-matched study including 710 matched pairs210. Malik AH, Yandrapalli S, Zaid S, Shetty SS, Aronow WS, Ahmad H, Tang GHL. Valve-in-Valve Transcatheter Implantation Versus Redo Surgical Aortic Valve Replacement. Am J Cardiol. 2020;125(9):1378-1384. Link. In-hospital mortality was numerically lower after TAV-in-SAV than redo SAVR (<1% vs. 4.9%, P=0.064).
The correct identification of the type and size of the bioprosthesis is the most important step when performing TAV-in-SAV. This information is usually obtained from previous operation records or valve identification cards provided by the manufacturers. A dedicated smartphone application will guide the decision in terms of type and size of a THV for the ViV procedure. The operator should acknowledge particular risks related to the individual bioprosthesis design, such as coronary obstruction in externally mounted stented valves or stent-less valves, valve malapposition or dislocation in stent-less valves, and residual gradients in stented small valves, , 211. Webb JG, Dvir D. Transcatheter aortic valve replacement for bioprosthetic aortic valve failure: the valve-in-valve procedure. Circulation. 2013;127(25):2542-50. Link212. Dvir D, Leipsic J, Blanke P, Ribeiro HB, Kornowski R, Pichard A, Rodes-Cabau J, Wood DA, Stub D, Ben-Dor I, Maluenda G, Makkar RR, Webb JG. Coronary obstruction in transcatheter aortic valve-in-valve implantation: preprocedural evaluation, device selection, protection, and treatment. Circ Cardiovasc Interv. 2015;8(1). Link213. Duncan A, Moat N, Simonato M, de Weger A, Kempfert J, Eggebrecht H, Walton A, Hellig F, Kornowski R, Spargias K, Mendiz O, Makkar R, Guerrero M, Rihal C, George I, Don C, Iadanza A, Bapat V, Welsh R, Wijeysundera HC, Wood D, Sathananthan J, Danenberg H, Maisano F, Garcia S, Gafoor S, Nombela-Franco L, Cobiella J, Dvir D. Outcomes Following Transcatheter Aortic Valve Replacement for Degenerative Stentless Versus Stented Bioprostheses. JACC Cardiovasc Interv. 2019;12(13):1256-1263. Link. As with TAVI for the native aortic valve, pre-procedural MDCT plays a pivotal role in determining the THV size and identifying a risk of coronary obstruction in TAV-in-SAV. Virtual valve to coronary ostial distance (VTC), as measured on MDCT, < 4mm is deemed to be at intermediate risk and VTC < 3mm is at high risk of coronary obstruction in patients with low lying coronary arteries, and preventative measures such as coronary protection and BASILICA should be considered212. Dvir D, Leipsic J, Blanke P, Ribeiro HB, Kornowski R, Pichard A, Rodes-Cabau J, Wood DA, Stub D, Ben-Dor I, Maluenda G, Makkar RR, Webb JG. Coronary obstruction in transcatheter aortic valve-in-valve implantation: preprocedural evaluation, device selection, protection, and treatment. Circ Cardiovasc Interv. 2015;8(1). Link. In patients where residual high gradients post-TAV-in-SAV are considered unavoidable (stented valves with small internal diameter), intentional fracture of the bioprosthesis with a non-compliant balloon may be performed before or after the THV implantation, 214. Chhatriwalla AK, Allen KB, Saxon JT, Cohen DJ, Aggarwal S, Hart AJ, Baron SJ, Dvir D, Borkon AM. Bioprosthetic Valve Fracture Improves the Hemodynamic Results of Valve-in-Valve Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2017;10(7). Link215. Allen KB, Chhatriwalla AK, Cohen DJ, Saxon JT, Aggarwal S, Hart A, Baron S, Davis JR, Pak AF, Dvir D, Borkon AM. Bioprosthetic Valve Fracture to Facilitate Transcatheter Valve-in-Valve Implantation. Ann Thorac Surg. 2017;104(5):1501-1508. Link.
Valve-in-valve for transcatheter bioprostheses
As the indication for TAVI expands to younger and low-risk patients, the number of patients who require repeat intervention for failed transcatheter bioprostheses is expected to grow. Inspired by the favourable outcomes of TAV-in-SAV, repeat transcatheter aortic valve implantation (TAV-in-TAV) is now considered a reasonable and effective treatment option for failed transcatheter bioprostheses, and performed in clinical practice (Table 22), , , 216. Barbanti M, Webb JG, Tamburino C, Van Mieghem NM, Makkar RR, Piazza N, Latib A, Sinning JM, Won-Keun K, Bleiziffer S, Bedogni F, Kapadia S, Tchetche D, Rodes-Cabau J, Fiorina C, Nombela-Franco L, De Marco F, de Jaegere PP, Chakravarty T, Vaquerizo B, Colombo A, Svensson L, Lange R, Nickenig G, Mollmann H, Walther T, Della Rosa F, Elhmidi Y, Dvir D, Brambilla N, Imme S, Sgroi C, Gulino S, Todaro D, Pilato G, Petronio AS, Tamburino C. Outcomes of Redo Transcatheter Aortic Valve Replacement for the Treatment of Postprocedural and Late Occurrence of Paravalvular Regurgitation and Transcatheter Valve Failure. Circ Cardiovasc Interv. 2016;9(9). Link217. Schmidt T, Frerker C, Alessandrini H, Schluter M, Kreidel F, Schafer U, Thielsen T, Kuck KH, Jose J, Holy EW, El-Mawardy M, Allali A, Richardt G, Abdel-Wahab M. Redo TAVI: initial experience at two German centres. EuroIntervention. 2016;12(7):875-82. Link218. Landes U, Webb JG, De Backer O, Sondergaard L, Abdel-Wahab M, Crusius L, Kim WK, Hamm C, Buzzatti N, Montorfano M, Ludwig S, Schofer N, Voigtlaender L, Guerrero M, El Sabbagh A, Rodes-Cabau J, Guimaraes L, Kornowski R, Codner P, Okuno T, Pilgrim T, Fiorina C, Colombo A, Mangieri A, Eltchaninoff H, Nombela-Franco L, Van Wiechen MPH, Van Mieghem NM, Tchetche D, Schoels WH, Kullmer M, Tamburino C, Sinning JM, Al-Kassou B, Perlman GY, Danenberg H, Ielasi A, Fraccaro C, Tarantini G, De Marco F, Witberg G, Redwood SR, Lisko JC, Babaliaros VC, Laine M, Nerla R, Castriota F, Finkelstein A, Loewenstein I, Eitan A, Jaffe R, Ruile P, Neumann FJ, Piazza N, Alosaimi H, Sievert H, Sievert K, Russo M, Andreas M, Bunc M, Latib A, Govdfrey R, Hildick-Smith D, Sathananthan J, Hensey M, Alkhodair A, Blanke P, Leipsic J, Wood DA, Nazif TM, Kodali S, Leon MB, Barbanti M. Repeat Transcatheter Aortic Valve Replacement for Transcatheter Prosthesis Dysfunction. J Am Coll Cardiol. 2020;75(16):1882-1893. Link219. Landes U, Sathananthan J, Witberg G, De Backer O, Sondergaard L, Abdel-Wahab M, Holzhey D, Kim WK, Hamm C, Buzzatti N, Montorfano M, Ludwig S, Conradi L, Seiffert M, Guerrero M, El Sabbagh A, Rodes-Cabau J, Guimaraes L, Codner P, Okuno T, Pilgrim T, Fiorina C, Colombo A, Mangieri A, Eltchaninoff H, Nombela-Franco L, Van Wiechen MPH, Van Mieghem NM, Tchetche D, Schoels WH, Kullmer M, Tamburino C, Sinning JM, Al-Kassou B, Perlman GY, Danenberg H, Ielasi A, Fraccaro C, Tarantini G, De Marco F, Redwood SR, Lisko JC, Babaliaros VC, Laine M, Nerla R, Castriota F, Finkelstein A, Loewenstein I, Eitan A, Jaffe R, Ruile P, Neumann FJ, Piazza N, Alosaimi H, Sievert H, Sievert K, Russo M, Andreas M, Bunc M, Latib A, Godfrey R, Hildick-Smith D, Chuang MA, Blanke P, Leipsic J, Wood DA, Nazif TM, Kodali S, Barbanti M, Kornowski R, Leon MB, Webb JG. Transcatheter Replacement of Transcatheter Versus Surgically Implanted Aortic Valve Bioprostheses. J Am Coll Cardiol. 2021;77(1):1-14. Link. In a dedicated multinational registry218. Landes U, Webb JG, De Backer O, Sondergaard L, Abdel-Wahab M, Crusius L, Kim WK, Hamm C, Buzzatti N, Montorfano M, Ludwig S, Schofer N, Voigtlaender L, Guerrero M, El Sabbagh A, Rodes-Cabau J, Guimaraes L, Kornowski R, Codner P, Okuno T, Pilgrim T, Fiorina C, Colombo A, Mangieri A, Eltchaninoff H, Nombela-Franco L, Van Wiechen MPH, Van Mieghem NM, Tchetche D, Schoels WH, Kullmer M, Tamburino C, Sinning JM, Al-Kassou B, Perlman GY, Danenberg H, Ielasi A, Fraccaro C, Tarantini G, De Marco F, Witberg G, Redwood SR, Lisko JC, Babaliaros VC, Laine M, Nerla R, Castriota F, Finkelstein A, Loewenstein I, Eitan A, Jaffe R, Ruile P, Neumann FJ, Piazza N, Alosaimi H, Sievert H, Sievert K, Russo M, Andreas M, Bunc M, Latib A, Govdfrey R, Hildick-Smith D, Sathananthan J, Hensey M, Alkhodair A, Blanke P, Leipsic J, Wood DA, Nazif TM, Kodali S, Leon MB, Barbanti M. Repeat Transcatheter Aortic Valve Replacement for Transcatheter Prosthesis Dysfunction. J Am Coll Cardiol. 2020;75(16):1882-1893. Link including 212 patients undergoing TAV-in-TAV, device success was achieved in 180 patients (85.1%). Overall hemodynamic outcomes were favourable with mean transvalvular gradients of 12.6 ± 7.5 mmHg, mean effective orifice area of 1.63 ± 0.61 cm2 at 30 days, and ≤mild PVR in 91%, all of which sustained at 1 year. Kaplan-Meier estimated survival was 97.2% at 30 days and 86.5% at 1 year. In a subsequent study219. Landes U, Sathananthan J, Witberg G, De Backer O, Sondergaard L, Abdel-Wahab M, Holzhey D, Kim WK, Hamm C, Buzzatti N, Montorfano M, Ludwig S, Conradi L, Seiffert M, Guerrero M, El Sabbagh A, Rodes-Cabau J, Guimaraes L, Codner P, Okuno T, Pilgrim T, Fiorina C, Colombo A, Mangieri A, Eltchaninoff H, Nombela-Franco L, Van Wiechen MPH, Van Mieghem NM, Tchetche D, Schoels WH, Kullmer M, Tamburino C, Sinning JM, Al-Kassou B, Perlman GY, Danenberg H, Ielasi A, Fraccaro C, Tarantini G, De Marco F, Redwood SR, Lisko JC, Babaliaros VC, Laine M, Nerla R, Castriota F, Finkelstein A, Loewenstein I, Eitan A, Jaffe R, Ruile P, Neumann FJ, Piazza N, Alosaimi H, Sievert H, Sievert K, Russo M, Andreas M, Bunc M, Latib A, Godfrey R, Hildick-Smith D, Chuang MA, Blanke P, Leipsic J, Wood DA, Nazif TM, Kodali S, Barbanti M, Kornowski R, Leon MB, Webb JG. Transcatheter Replacement of Transcatheter Versus Surgically Implanted Aortic Valve Bioprostheses. J Am Coll Cardiol. 2021;77(1):1-14. Link, 434 TAV-in-TAV including bailout valve-in-valve procedures were compared with 624 TAV-in-SAV using propensity score matching. In the propensity-matched cohort including 165 matched pairs, TAV-in-TAV was associated with higher procedural success (72.7% vs. 62.4%, P=0.045), and similar procedural safety (70.3% vs. 72.1%, P=0.715) and mortality at 30 days (3.0% vs. 4.4%, P=0.570) and at 1 year (11.9% vs. 10.2%, P=0.633). Although early safety and effectiveness of TAV-in-TAV are favourable in these retrospective studies, more data particularly on long-term valve durability are needed. Furthermore, the risk of coronary obstruction and the potential difficulties in coronary access after TAV-in-TAV (Figure 7) remain concerns that need further investigation.
Pure Native Valve Aortic regurgitation
Pure native valve aortic regurgitation has been considered a relative contraindication to TAVI due to specific anatomic features characterized by the absence of aortic valve calcification, large aortic annulus size and frequent coexistence with dilatation of the aortic root. The Euro Heart Survey on Valvular Heart Disease reported that 7.8% of patients with severe aortic regurgitation requiring surgical treatment had no intervention mainly due to advanced age and multiple comorbidities yielding an excessive risk of peri-operative mortality. Thus, TAVI for pure aortic regurgitation is explored as treatment alternative to surgery (Table 23), , , , , , , , , 220. Roy DA, Schaefer U, Guetta V, Hildick-Smith D, Mollmann H, Dumonteil N, Modine T, Bosmans J, Petronio AS, Moat N, Linke A, Moris C, Champagnac D, Parma R, Ochala A, Medvedofsky D, Patterson T, Woitek F, Jahangiri M, Laborde JC, Brecker SJ. Transcatheter aortic valve implantation for pure severe native aortic valve regurgitation. J Am Coll Cardiol. 2013;61(15):1577-84. Link221. Seiffert M, Bader R, Kappert U, Rastan A, Krapf S, Bleiziffer S, Hofmann S, Arnold M, Kallenbach K, Conradi L, Schlingloff F, Wilbring M, Schafer U, Diemert P, Treede H. Initial German experience with transapical implantation of a second-generation transcatheter heart valve for the treatment of aortic regurgitation. JACC Cardiovasc Interv. 2014;7(10):1168-74. Link222. Wendt D, Kahlert P, Pasa S, El-Chilali K, Al-Rashid F, Tsagakis K, Dohle DS, Erbel R, Jakob H, Thielmann M. Transapical transcatheter aortic valve for severe aortic regurgitation: expanding the limits. JACC Cardiovasc Interv. 2014;7(10):1159-67. Link223. Testa L, Latib A, Rossi ML, De Marco F, De Carlo M, Fiorina C, Oreglia J, Petronio AS, Ettori F, De Servi S, Klugmann S, Ussia GP, Tamburino C, Panisi P, Brambilla N, Colombo A, Presbitero P, Bedogni F. CoreValve implantation for severe aortic regurgitation: a multicentre registry. EuroIntervention. 2014;10(6):739-45. Link224. Schofer J, Nietlispach F, Bijuklic K, Colombo A, Gatto F, De Marco F, Mangieri A, Hansen L, Bruschi G, Ruparelia N, Riess FC, Maisano F, Latib A. Transfemoral Implantation of a Fully Repositionable and Retrievable Transcatheter Valve for Noncalcified Pure Aortic Regurgitation. JACC Cardiovasc Interv. 2015;8(14):1842-9. Link225. Sawaya FJ, Deutsch MA, Seiffert M, Yoon SH, Codner P, Wickramarachchi U, Latib A, Petronio AS, Rodes-Cabau J, Taramasso M, Spaziano M, Bosmans J, Biasco L, Mylotte D, Savontaus M, Gheeraert P, Chan J, Jorgensen TH, Sievert H, Mocetti M, Lefevre T, Maisano F, Mangieri A, Hildick-Smith D, Kornowski R, Makkar R, Bleiziffer S, Sondergaard L, De Backer O. Safety and Efficacy of Transcatheter Aortic Valve Replacement in the Treatment of Pure Aortic Regurgitation in Native Valves and Failing Surgical Bioprostheses: Results From an International Registry Study. JACC Cardiovasc Interv. 2017;10(10):1048-1056. Link226. Yoon SH, Schmidt T, Bleiziffer S, Schofer N, Fiorina C, Munoz-Garcia AJ, Yzeiraj E, Amat-Santos IJ, Tchetche D, Jung C, Fujita B, Mangieri A, Deutsch MA, Ubben T, Deuschl F, Kuwata S, De Biase C, Williams T, Dhoble A, Kim WK, Ferrari E, Barbanti M, Vollema EM, Miceli A, Giannini C, Attizzani GF, Kong WKF, Gutierrez-Ibanes E, Jimenez Diaz VA, Wijeysundera HC, Kaneko H, Chakravarty T, Makar M, Sievert H, Hengstenberg C, Prendergast BD, Vincent F, Abdel-Wahab M, Nombela-Franco L, Silaschi M, Tarantini G, Butter C, Ensminger SM, Hildick-Smith D, Petronio AS, Yin WH, De Marco F, Testa L, Van Mieghem NM, Whisenant BK, Kuck KH, Colombo A, Kar S, Moris C, Delgado V, Maisano F, Nietlispach F, Mack MJ, Schofer J, Schaefer U, Bax JJ, Frerker C, Latib A, Makkar RR. Transcatheter Aortic Valve Replacement in Pure Native Aortic Valve Regurgitation. J Am Coll Cardiol. 2017;70(22):2752-2763. Link227. De Backer O, Pilgrim T, Simonato M, Mackensen GB, Fiorina C, Veulemanns V, Cerillo A, Schofer J, Amabile N, Achkouty G, Schafer U, Deutsch MA, Sinning JM, Rahman MS, Sawaya FJ, Hildick-Smith D, Hernandez JM, Kim WK, Lefevre T, Seiffert M, Bleiziffer S, Petronio AS, Van Mieghem N, Taramasso M, Sondergaard L, Windecker S, Latib A, Dvir D. Usefulness of Transcatheter Aortic Valve Implantation for Treatment of Pure Native Aortic Valve Regurgitation. Am J Cardiol. 2018;122(6):1028-1035. Link228. Anwaruddin S, Desai ND, Szeto WY, Hermiller JB, Jr., Sorajja P, Kodali S, Popma JJ, Giri J, Herrmann HC, Tang GHL, Rame JE, McCarthy FH, Zhang AQ, Reardon MJ. Self-Expanding Valve System for Treatment of Native Aortic Regurgitation by Transcatheter Aortic Valve Implantation (from the STS/ACC TVT Registry). Am J Cardiol. 2019;124(5):781-788. Link229. Purita PAM, Tahoces LS, Fraccaro C, Nai Fovino L, Kim WK, Espada-Guerreiro C, De Backer O, Seiffert M, Nombela-Franco L, Gomez RM, Mangieri A, Franzone A, Bedogni F, Castriota F, Attisano T, Sondergaard L, Antolin RH, Tarantini G. Transcatheter treatment of native aortic valve regurgitation: Results from an international registry using the transfemoral ACURATE neo valve. Int J Cardiol Heart Vasc. 2020;27:100480. Link.
Table 23
TAVI for pure native valve aortic valve regurgitation
Self-expanding THVs have been preferred over balloon-expandable THVs in patients with pure native valve aortic regurgitation for the possibility to oversize the prosthesis while preserving a low risk of annular rupture through relying on its radial force to ensure anchoring even in the absence of calcification. The first report of TAVI for pure aortic regurgitation included 43 high-risk patients (mean STS-PROM 10.2%) at 14 centres220. Roy DA, Schaefer U, Guetta V, Hildick-Smith D, Mollmann H, Dumonteil N, Modine T, Bosmans J, Petronio AS, Moat N, Linke A, Moris C, Champagnac D, Parma R, Ochala A, Medvedofsky D, Patterson T, Woitek F, Jahangiri M, Laborde JC, Brecker SJ. Transcatheter aortic valve implantation for pure severe native aortic valve regurgitation. J Am Coll Cardiol. 2013;61(15):1577-84. Link. The CoreValve THV was used for all the cases, and procedural success was achieved in 97.7%. Second valve implantation was required in 18.6% of the cases during the index procedure, and 79% of patients had ≤mild PVR. At 30 days, the incidence of stroke and all-cause death were 4.7% and 9.3%, respectively. In a systematic review including 237 patients from 13 reports230. Franzone A, Piccolo R, Siontis GC, Lanz J, Stortecky S, Praz F, Roost E, Vollenbroich R, Windecker S, Pilgrim T. Transcatheter Aortic Valve Replacement for the Treatment of Pure Native Aortic Valve Regurgitation: A Systematic Review. JACC Cardiovasc Interv. 2016;9(22):2308-2317. Link, self-expanding THVs were predominantly used (79%) and device success ranged from 75% to 100%. Second valve implantation was needed in 17 patients (7%) and conversion to SAVR was reported in 6 patients (2.5%). The incidence of moderate or severe PVR was 9% (95% CI 0 to 28%, I2 = 90%). At 30 days, all-cause death occurred in 7% (95% CI 3 to 13, I2 = 37%). The occurrences of cerebrovascular events, major bleeding, and vascular complications were relatively low.
The JenaValve (JenaValve Technology, Munich, Germany) is a dedicated self-expanding valve system for pure aortic regurgitation, that features a clipping mechanism that anchors positioning feelers into the native aortic annulus (Figure 11). It gained Conformité Européenne approval for use in patients with isolated aortic regurgitation in 2013 by demonstrating safety and feasibility of implantation through a transapical approach in 31 patients included in the JUPITER registry221. Seiffert M, Bader R, Kappert U, Rastan A, Krapf S, Bleiziffer S, Hofmann S, Arnold M, Kallenbach K, Conradi L, Schlingloff F, Wilbring M, Schafer U, Diemert P, Treede H. Initial German experience with transapical implantation of a second-generation transcatheter heart valve for the treatment of aortic regurgitation. JACC Cardiovasc Interv. 2014;7(10):1168-74. Link. Procedural success was achieved in 96.7% with only one patient requiring conversion to SAVR because of device embolization. At discharge, no moderate or severe PVR was documented. Overall mortality was 10% and 20% at 1 and 2 years, respectively. More recently, a transfemoral delivery system for the Jena Valve has been developed and is under clinical investigation.
In a multicentre study including 254 patients from 46 centres227. De Backer O, Pilgrim T, Simonato M, Mackensen GB, Fiorina C, Veulemanns V, Cerillo A, Schofer J, Amabile N, Achkouty G, Schafer U, Deutsch MA, Sinning JM, Rahman MS, Sawaya FJ, Hildick-Smith D, Hernandez JM, Kim WK, Lefevre T, Seiffert M, Bleiziffer S, Petronio AS, Van Mieghem N, Taramasso M, Sondergaard L, Windecker S, Latib A, Dvir D. Usefulness of Transcatheter Aortic Valve Implantation for Treatment of Pure Native Aortic Valve Regurgitation. Am J Cardiol. 2018;122(6):1028-1035. Link, device success was significantly higher in patients treated with newer generation devices than those with early generation devices (82% vs. 47%, P<0.001). The difference was driven by lower rates of device malpositioning (9% vs. 33%) and ≥moderate PVR (4% vs. 31%) in the newer generation devices. Another multicentre study including 331 patients from 30 centres reported similar results226. Yoon SH, Schmidt T, Bleiziffer S, Schofer N, Fiorina C, Munoz-Garcia AJ, Yzeiraj E, Amat-Santos IJ, Tchetche D, Jung C, Fujita B, Mangieri A, Deutsch MA, Ubben T, Deuschl F, Kuwata S, De Biase C, Williams T, Dhoble A, Kim WK, Ferrari E, Barbanti M, Vollema EM, Miceli A, Giannini C, Attizzani GF, Kong WKF, Gutierrez-Ibanes E, Jimenez Diaz VA, Wijeysundera HC, Kaneko H, Chakravarty T, Makar M, Sievert H, Hengstenberg C, Prendergast BD, Vincent F, Abdel-Wahab M, Nombela-Franco L, Silaschi M, Tarantini G, Butter C, Ensminger SM, Hildick-Smith D, Petronio AS, Yin WH, De Marco F, Testa L, Van Mieghem NM, Whisenant BK, Kuck KH, Colombo A, Kar S, Moris C, Delgado V, Maisano F, Nietlispach F, Mack MJ, Schofer J, Schaefer U, Bax JJ, Frerker C, Latib A, Makkar RR. Transcatheter Aortic Valve Replacement in Pure Native Aortic Valve Regurgitation. J Am Coll Cardiol. 2017;70(22):2752-2763. Link. Newer generation devices were associated with higher device success rate (81.1% vs. 61.3%, P<0.001) due to lower rates of second valve implantation (12.7% vs. 24.4%, P=0.007) and ≥moderate PVR (4.2% vs. 18.8%, P<0.001). At 1 year, the newer generation devices were associated with a lower cardiovascular mortality (9.6% vs. 23.6%< P=0.008). Current evidence indicates the feasibility of TAVI in patients with pure native valve aortic regurgitation, but it should be reserved for inoperable patients.
Conclusion
After nearly 20 years of evolution, TAVI has become the standard of care for symptomatic severe AS alongside SAVR. There continue to remain uncertainties regarding the indications and optimal timing for the intervention, particularly in patients with bicuspid anatomy, moderate AS, or asymptomatic severe AS. Furthermore, the choice between TAVI and SAVR involves a wide range of individual factors (age, gender, previous cardiac surgery, frailty, cardiac and non-cardiac comorbidities, valve and access route anatomy, and patient preferences), and is ultimately left to the discretion of the treating Heart team. The role of the multidisciplinary Heart team is therefore increasingly important for the optimal decision-making. Although the principal TAVI procedure is now well-established, refinements both in technique (e.g., coronary protection, cerebral protection, high prosthesis implantation) and post-procedural care (e.g., antithrombotic management, monitoring for AV conduction disturbances) continue to evolve and may further improve outcomes. Finally, long-term follow-up and thorough assessment of durability will be important to assess differences between devices.
Personal perspective - Taishi Okuno
TAVI has demonstrated superiority/noninferiority compared to SAVR across the entire spectrum of surgical risk in terms of clinical outcomes during mid-term follow-up (1 to 5 years). The less invasive nature of the interventions, lower peri-procedural risks, faster recovery and shorter hospital stay are undeniably attractive for patients. Notwithstanding, there is still a paucity of data, particularly as it relates to long-term durability and clinical outcomes among younger low risk patients. The adverse effects of the higher risk of mild paravalvular regurgitation and AV conduction disturbances after TAVI require careful assessment. Moreover, patients with anatomic features at high risk or unsuitable for TAVI should be considered for SAVR. Further research is indispensable to guide the optimal treatment strategy for younger populations with a longer life expectancy as well as refine the devices and techniques to overcome the current limitations of TAVI.