Department of Cardiology, Inselspital, University of Bern, Bern, Switzerland, Department of Cardiology, Inselspital, University of Bern, Bern, Switzerland, Department of Cardiology, Inselspital, University of Bern, Bern, Switzerland, Department of Cardiology, St. Marianna University School of Medicine, Kanagawa, Japan, Department of Cardiology, Inselspital, University of Bern, Bern, Switzerland
In this chapter
Aortic stenosis (AS) is the most common valvular heart disease leading to intervention. It is characterized by progression from leaflet thickening and calcification to significant haemodynamic stenosis which results in disease-specific symptoms and physical limitations as well as poor prognosis and impaired quality of life if left untreated.
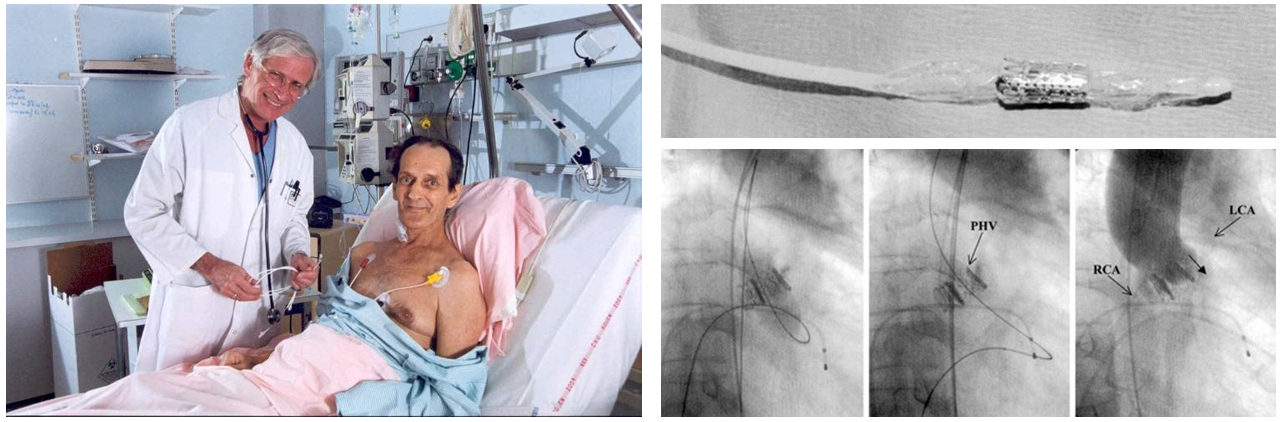
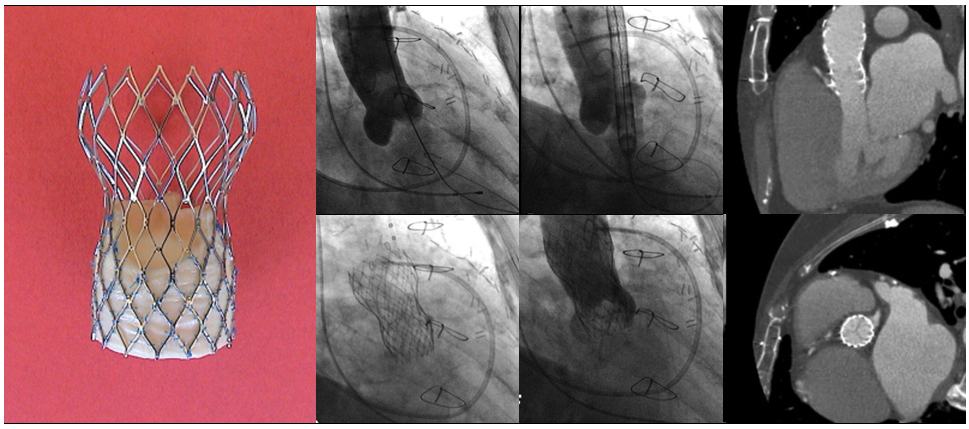
In 1986, Cribier and colleagues introduced balloon aortic valvuloplasty as treatment for inoperable patients with severe AS1. Cribier A, Savin T, Saoudi N, et al. Percutaneous transluminal valvuloplasty of acquired aortic stenosis in elderly patients: an alternative to valve replacement. Lancet. 1986;1:63-67 Link. Although balloon aortic valvuloplasty achieved favourable acute haemodynamic outcomes, restenosis and clinical deterioration occurred frequently within 6-12 months requiring repeat interventions, 2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link3. Lieberman EB, Bashore TM, Hermiller JB, et al. Balloon aortic valvuloplasty in adults: failure of procedure to improve long-term survival. J Am Coll Cardiol. 1995;26:1522-1528 Link. In 2002, Cribier and colleagues performed the first in-human transcatheter aortic valve implantation (TAVI) using a 24 Fr catheter delivery system housing a 23 mm bovine pericardial balloon-expandable stent valve in a 57-year-old critically ill patient presenting with cardiogenic shock due to severe AS who had failed balloon valvuloplasty (Figure 1)4. Cribier A, Eltchaninoff H, Bash A, et al. Percutaneous transcatheter implantation of an aortic valve prosthesis for calcific aortic stenosis: first human case description. Circulation. 2002;106:3006-3008 Link. The intervention was successful in restoring stable haemodynamics leading to subsequent feasibility studies with the balloon-expandable transcatheter heart valve (THV), , 5. Cribier A, Eltchaninoff H, Tron C, et al. Early experience with percutaneous transcatheter implantation of heart valve prosthesis for the treatment of end-stage inoperable patients with calcific aortic stenosis. J Am Coll Cardiol. 2004;43:698-703 Link6. Cribier A, Eltchaninoff H, Tron C, et al. Treatment of calcific aortic stenosis with the percutaneous heart valve: mid-term follow-up from the initial feasibility studies: the French experience. J Am Coll Cardiol. 2006;47:1214-1223 Link7. Walther T, Falk V, Kempfert J, et al. Transapical minimally invasive aortic valve implantation; the initial 50 patients. Eur J Cardiothorac Surg. 2008;33:983-988 Link. In parallel, Grube and colleagues reported the first-in-human results of a self-expanding THV consisting of a nitinol frame and porcine pericardial leaflets (Figure 2), 8. Grube E, Laborde JC, Gerckens U, et al. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-risk patients with aortic valve disease: the Siegburg first-in-man study. Circulation. 2006;114:1616-1624 Link9. Grube E, Schuler G, Buellesfeld L, et al. Percutaneous aortic valve replacement for severe aortic stenosis in high-risk patients using the second- and current third-generation self-expanding CoreValve prosthesis: device success and 30-day clinical outcome. J Am Coll Cardiol. 2007;50:69-76 Link. The early feasibility studies with balloon-expandable or self-expanding THV consistently demonstrated procedural success resulting in significant haemodynamic improvement with favourable short-term clinical outcomes (Table 1), , , , 5. Cribier A, Eltchaninoff H, Tron C, et al. Early experience with percutaneous transcatheter implantation of heart valve prosthesis for the treatment of end-stage inoperable patients with calcific aortic stenosis. J Am Coll Cardiol. 2004;43:698-703 Link6. Cribier A, Eltchaninoff H, Tron C, et al. Treatment of calcific aortic stenosis with the percutaneous heart valve: mid-term follow-up from the initial feasibility studies: the French experience. J Am Coll Cardiol. 2006;47:1214-1223 Link7. Walther T, Falk V, Kempfert J, et al. Transapical minimally invasive aortic valve implantation; the initial 50 patients. Eur J Cardiothorac Surg. 2008;33:983-988 Link8. Grube E, Laborde JC, Gerckens U, et al. Percutaneous implantation of the CoreValve self-expanding valve prosthesis in high-risk patients with aortic valve disease: the Siegburg first-in-man study. Circulation. 2006;114:1616-1624 Link9. Grube E, Schuler G, Buellesfeld L, et al. Percutaneous aortic valve replacement for severe aortic stenosis in high-risk patients using the second- and current third-generation self-expanding CoreValve prosthesis: device success and 30-day clinical outcome. J Am Coll Cardiol. 2007;50:69-76 Link, ushering in a new era in the management of patients with severe AS.
Figure 1
First-in-human transcatheter aortic valve implantation. Figures reproduced and modified from Cribier et al. Circulation 2002;106(24):3006-3008 and PCR Online (https://www.pcronline.com).
First implantation of the self-expanding CoreValve System. Figures reproduced and modified from Grube et al. Catheter Cardiovasc Interv 2005;66(4):465-9.
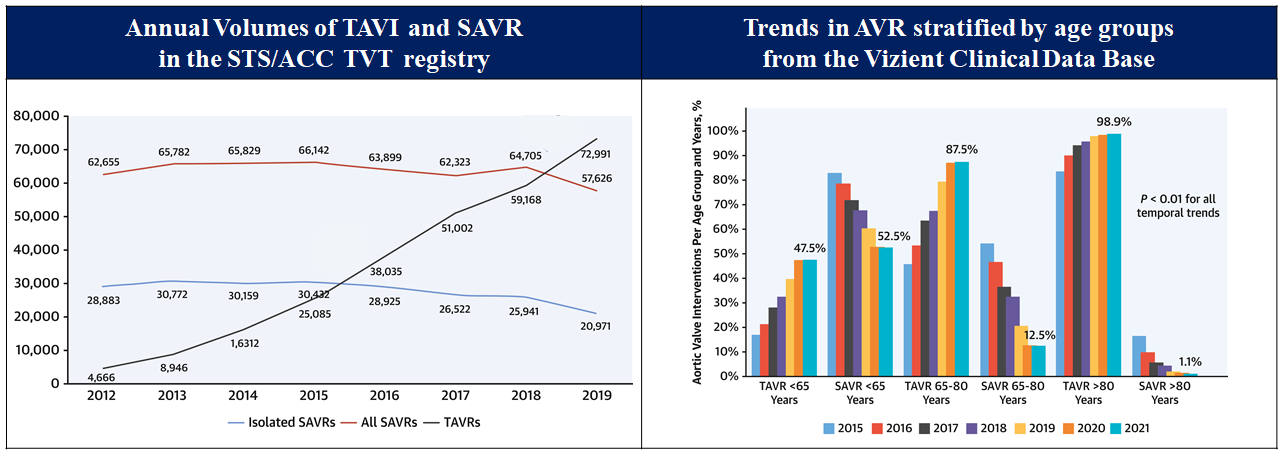
Following the feasibility studies, TAVI has been directly compared with surgical aortic valve replacement (SAVR) in a series of randomized control trials (RCTs) across the spectrum of surgical risk, demonstrating favourable clinical outcomes, , , , , , , , , , , , 10. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607. Link11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link12. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790-1798 Link13. Thyregod HG, Steinbrüchel DA, Ihlemann N, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65:2184-2194 Link14. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374:1609-1620. Link15. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376:1321-1331 Link16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link17. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380:1706-1715 Link18. Siontis GCM, Overtchouk P, Cahill TJ, et al. Transcatheter aortic valve implantation vs surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. 2019;40:3143-3153 Link19. UK TAVI Trial Investigators; Toff WD, Hildick-Smith D, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA. 2022;327:1875-1887. Link20. Ahmad Y, Howard JP, Arnold AD, et al. Transcatheter versus surgical aortic valve replacement in lower-risk and higher-risk patients: a meta-analysis of randomized trials. Eur Heart J. 2023;44:836-852 Link21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link. Following regulatory approval in Europe in 2007 and in the United States in 2011, TAVI has been widely adopted and continues to grow exponentially (Figure 3), , 23. Pilgrim T, Windecker S. Expansion of transcatheter aortic valve implantation: new indications and socio-economic considerations. Eur Heart J. 2018;39:2643-2645 Link24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link25. Sharma T, Krishnan AM, Lahoud R, Polomsky M, Dauerman HL. National Trends in TAVR and SAVR for Patients With Severe Isolated Aortic Stenosis. J Am Coll Cardiol. 2022;80:2054-2056 Link. In this chapter, we will provide a detailed description of current indications, patient selection for TAVI, and the procedural considerations. Furthermore, we will summarize the available evidence and emerging indications in the field of TAVI.
Figure 3
National trend in aortic valve implantation. Figures reproduced and modified from Carroll et al. J Am Coll Cardiol 2020;76(21):2492-2516 and Sharma et al. J Am Coll Cardiol 222;80(21)2054-2056.
AVA = aortic valve area; mPG = mean transvalvular gradient.
Aortic Stenosis
Epidemiology
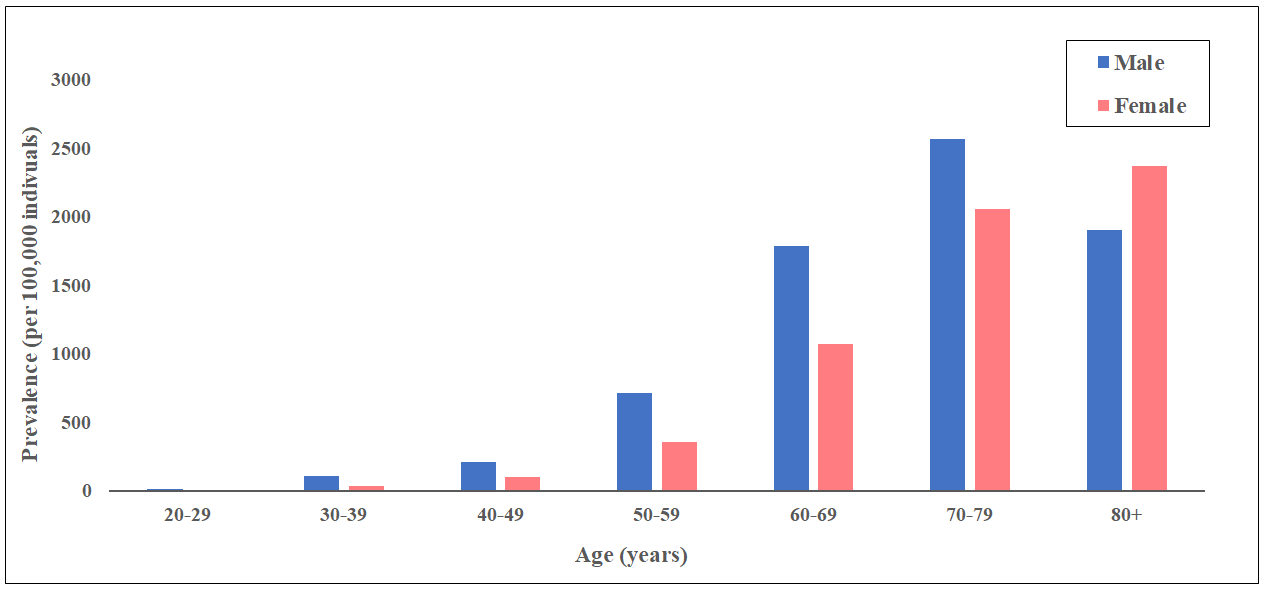
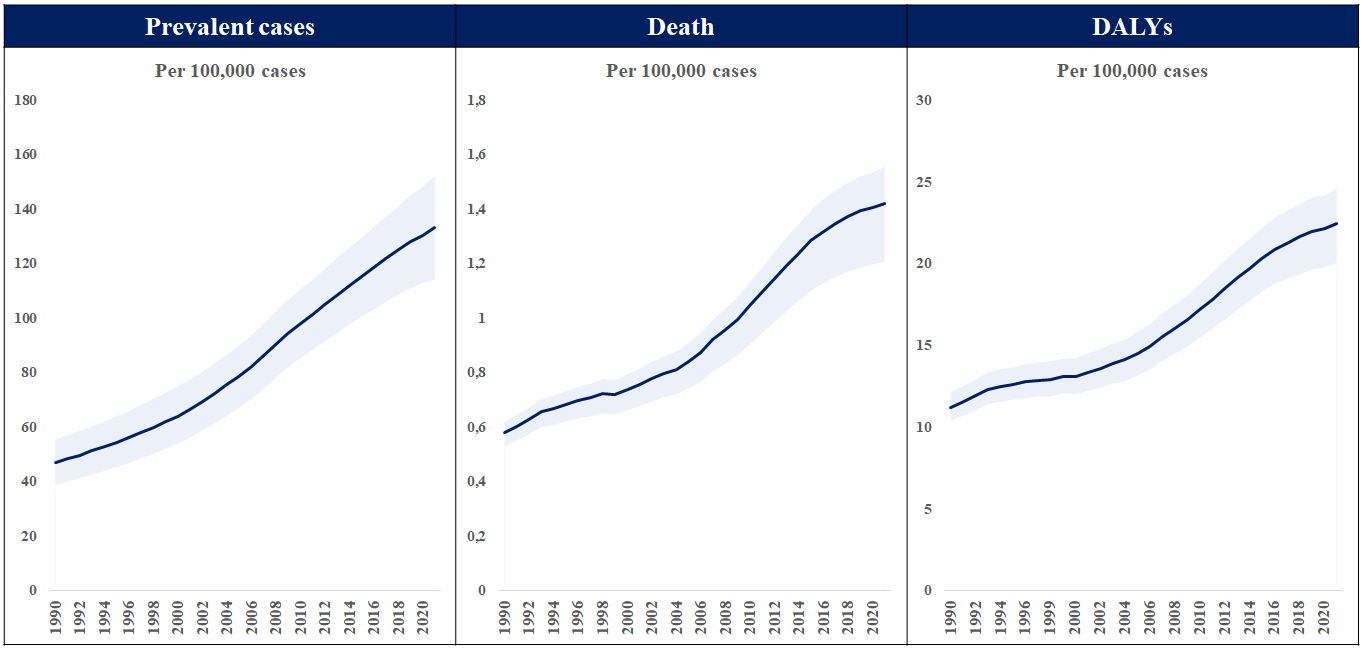
The global burden of calcific aortic valve disease continues to increase due to aging and population growth. In 2021, there were an estimated 13.3 million cases, predominantly observed in the elderly population, and an estimated 151,000 deaths and 2,140,000 disability-adjusted life years attributable to non-rheumatic calcified aortic valve disease (Figure 4andFigure 5), 26. Roth GA, Mensah GA, Johnson CO, et al. Global Burden of Cardiovascular Diseases and Risk Factors, 1990-2019: Update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76:2982-3021 Link27. Yadgir S, Johnson CO, Aboyans V, et al. Global, Regional, and National Burden of Calcific Aortic Valve and Degenerative Mitral Valve Diseases, 1990-2017. Circulation. 2020;141:1670-1680 Link. A pooled analysis of 11,911 adults from three large, national, population-based epidemiological studies, combined with data from 16,501 adults in Olmsted County, demonstrated an age-dependent increase in the prevalence of moderate or severe AS (in population-based studies: 0.02% in 18-44, 0.1% in 45-54, 0.2% in 55-64, 1.3% in 65-74, and 2.8% in ≥75 years; in Olmsted County: 0.1% in 18-44, 0.2% in 45-54, 0.6% in 55-64, 1.4% in 65-74, and 4.6% in ≥75 years, respectively)28. Nkomo VT, Gardin JM, Skelton TN, et al. Burden of valvular heart diseases: a population-based study. Lancet. 2006;368:1005-1011 Link. The actual incidence and prevalence of AS may be underestimated. The OxVALVE Population Cohort Study enrolled 2,500 adults aged ≥65 years from a primary care population and screened for undiagnosed valvular heart disease. In this study, AS was newly diagnosed in 1.3% of participants, and over half of these patients had moderate or severe AS29. d'Arcy JL, Coffey S, Loudon MA, et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur Heart J. 2016;37:3515-3522 Link. This study suggested a substantial increase in the clinical and economic consequences of clinically significant valvular heart disease within the rapidly expanding elderly population. Indeed, recent data from Olmsted County indicate that although the incidence of severe AS has remained stable, the absolute number of AS cases has increased30. Blaser MC, Back M, Luscher TF, Aikawa E. Calcific aortic stenosis: omics-based target discovery and therapy development. Eur Heart J. 2025;46:620-634 Link.
Figure 4
Prevalence of non-rheumatic calcific aortic valve disease in 2021. Data obtained from the Global Burden of Disease Study 2021.
Total number of prevalent cases, death, and disability-adjusted life years (DALYs) to non-rheumatic calcific aortic valve disease between 1990 and 2021. Data obtained from the Global Burden of Disease Study 2021.
The primary etiologies of AS comprise degenerative calcific stenosis (>80% in Europe/US), bicuspid/congenital anomalies (10% in Europe, US), and rheumatic heart disease (<5 in Europe, US). Epidemiological, histopathological, and imaging studies suggest an underlying pathological process with features of both atherosclerosis and elastocalcinosis, including progressive fibro-calcific remodeling and thickening of the aortic valve leaflets caused by genetic factors, lipoprotein deposition and oxidation, chronic inflammation, and osteoblastic transformation of cardiac valve interstitial cells, , 31. Otto CM. Calcific aortic stenosis--time to look more closely at the valve. N Engl J Med. 2008;359:1395-1398 Link32. Carabello BA, Paulus WJ. Aortic stenosis. Lancet. 2009;373:956-966 Link33. Dweck MR, Khaw HJ, Sng GK, et al. Aortic stenosis, atherosclerosis, and skeletal bone: is there a common link with calcification and inflammation. Eur Heart J. 2013;34:1567-1574 Link. Common risk factors for AS include age, male sex, diabetes, hypercholesterolemia, arterial hypertension, obesity, and chronic kidney disease32. Carabello BA, Paulus WJ. Aortic stenosis. Lancet. 2009;373:956-966 Link. Bicuspid aortic valve is the most prevalent congenital heart condition in adults. In the neonatal bicuspid aortic valve, the trilaminar structure is compromised with significant increase in collagen fibers and proteoglycans, as well as fragmentation of elastin fibers, which are associated with early progression of valve deterioration, 34. Yang LT, Ye Z, Wajih Ullah M, et al. Bicuspid aortic valve: long-term morbidity and mortality. Eur Heart J. 2023;44:4549-4562 Link35. Moncla LM, Briend M, Bosse Y, Mathieu P. Calcific aortic valve disease: mechanisms, prevention and treatment. Nat Rev Cardiol. 2023;20:546-559 Link. Rheumatic AS is characterized by non-calcific thickening of the leaflets and fusion of the commissures36. Roberts K, Colquhoun S, Steer A, Remenyi B, Carapetis J. Screening for rheumatic heart disease: current approaches and controversies. Nat Rev Cardiol. 2013;10:49-58 Link. Although there has been a significant reduction in the global burden of disease over the past decades, the health-related burden of rheumatic heart disease remains high particularly in middle-income and low-income countries37. Coffey S, Roberts-Thomson R, Brown A, et al. Global epidemiology of valvular heart disease. Nat Rev Cardiol. 2021 Link. For the same haemodynamic severity of AS, women and men have different pathophysiology of AS: women have less aortic valve calcification and more valvular fibrosis with denser connective tissue than men. These differences may be related to a higher incidence of hypertension in women and poorly understood interactions with sex hormones, although this remains to be elucidated38. Hahn RT, Clavel MA, Mascherbauer J, et al. Sex-Related Factors in Valvular Heart Disease: JACC Focus Seminar 5/7. J Am Coll Cardiol. 2022;79:1506-1518 Link.
Diagnosis and classification of AS
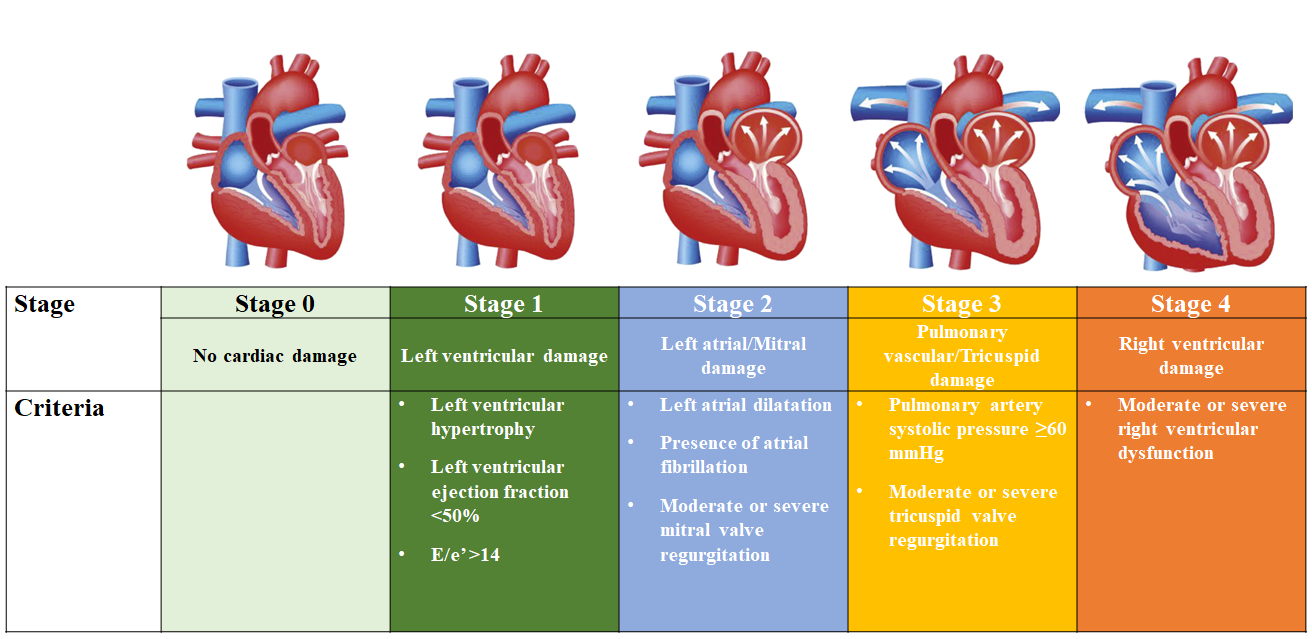
AS is a progressive disease characterized by the presence of aortic valve thickening and calcification, resulting in reduced leaflet motion, haemodynamic left ventricular outflow obstruction, and increased afterload, 31. Otto CM. Calcific aortic stenosis--time to look more closely at the valve. N Engl J Med. 2008;359:1395-1398 Link32. Carabello BA, Paulus WJ. Aortic stenosis. Lancet. 2009;373:956-966 Link. Chronic pressure overload produces various anatomical and physiological changes including left ventricular hypertrophy, left atrial enlargement, and pulmonary arterial hypertension, leading to AS-related and heart failure symptoms, including exertional dyspnea, angina, and syncope. Current American College of Cardiology/American Heart Association (ACC/AHA) and European Society of Cardiology/European Association for Cardio-Thoracic Surgery (ESC/EACTS) guidelines for the management of valvular heart disease base the diagnosis and classification of AS on the integration of clinical symptoms and echocardiographic assessment (Table 2), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. The definition of severe AS, the target of replacement therapy, comprises transaortic velocity ≥4 m/sec, mean transvalvular pressure gradient ≥40 mmHg, or aortic valve area ≤1 cm2, 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. Recently, a staging classification has been proposed to characterize the extent of extra-aortic valve damage (Figure 6), demonstrating that advanced stages of cardiac damage are strongly associated with an increased risk of adverse events after aortic valve replacement (AVR), 41. Genereux P, Pibarot P, Redfors B, et al. Staging classification of aortic stenosis based on the extent of cardiac damage. Eur Heart J. 2017;38:3351-3358 Link42. Genereux P, Pibarot P, Redfors B, et al. Evolution and Prognostic Impact of Cardiac Damage After Aortic Valve Replacement. J Am Coll Cardiol. 2022;80:783-800 Link. This classification has been validated in various independent cohorts, , 43. Fukui M, Gupta A, Abdelkarim I, et al. Association of Structural and Functional Cardiac Changes With Transcatheter Aortic Valve Replacement Outcomes in Patients With Aortic Stenosis. Jama. Cardiol 2019;4:215-222 Link44. Nakase M, Tomii D, Heg D, et al. Long-Term Impact of Cardiac Damage Following Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2024;17:992-1003 Link45. Nakase M, Tomii D, Maznyczka A, et al. Sex-Specific Differences in Upstream Cardiac Damage in Patients With Aortic Stenosis Undergoing TAVR. JACC Cardiovasc Interv. 2024;17:1252-1264 Link, and there is a growing interest in the grading scheme to improve patient management and therapeutic decision-making.
Figure 6
Proposed staging classification to quantify the extent of cardiac damage among patients with aortic stenosis. Figures reproduced and modified from Généreux et al. J Am Coll Cardiol 2022;80:783-800.
Low flow, low gradient AS with reduced ejection fraction#5
D3: Symptomatic severe low-gradient AS with normal LVEF or paradoxical low-flow severe AS
AVA <1 cm2 with a Vmax <4 m/s or mPG <40 mmHg
AND SVI <35 mL/m2 Measured when patient is normotensive (systolic blood pressure <140 mmHg)
Increased LV relative wall thickness Small LV chamber with low stroke volume Restrictive diastolic filling LVEF ≥50%
Low flow, low gradient AS with preserved ejection fraction
#1 ESC/EACTS guidelines adopt criteria for Vmax <2.5 m/s.
#2 ESC/EACTS guidelines adopt criteria for Vmax 2.6-2.9 m/s or mPG <20 mmHg or AVA > 1.5 cm2 or AVAi > 0.85 cm/m2 or Velocity ratio > 0.5.
#3 ESC/EACTS guidelines adopt criteria for Vmax 3-4 m/s or mPG 20-40 mmHg or AVA 1-1.5 cm2 or AVAi 0.6-0.85 cm/m2 or Velocity ratio 0.25-0.5.
#4 ESC/EACTS guidelines adopt criteria for Vmax ≥ 4 m/s or mPG ≥40 mmHg or AVA < 1 cm2 or AVAi < 0.6 cm/m2 or Velocity ratio < 0.25.
#5 Additional criteria of SVI <35 ml/m2.
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; AVA = aortic valve area; AVAi = aortic valve area index to body surface area; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; LV = left ventricular; LVEF = left ventricular ejection fraction; mPG = mean transvalvular gradient; SVI = stroke volume index to body surface area; Vmax = peak transvalvular velocity.
Indications for aortic valve interventions and TAVI
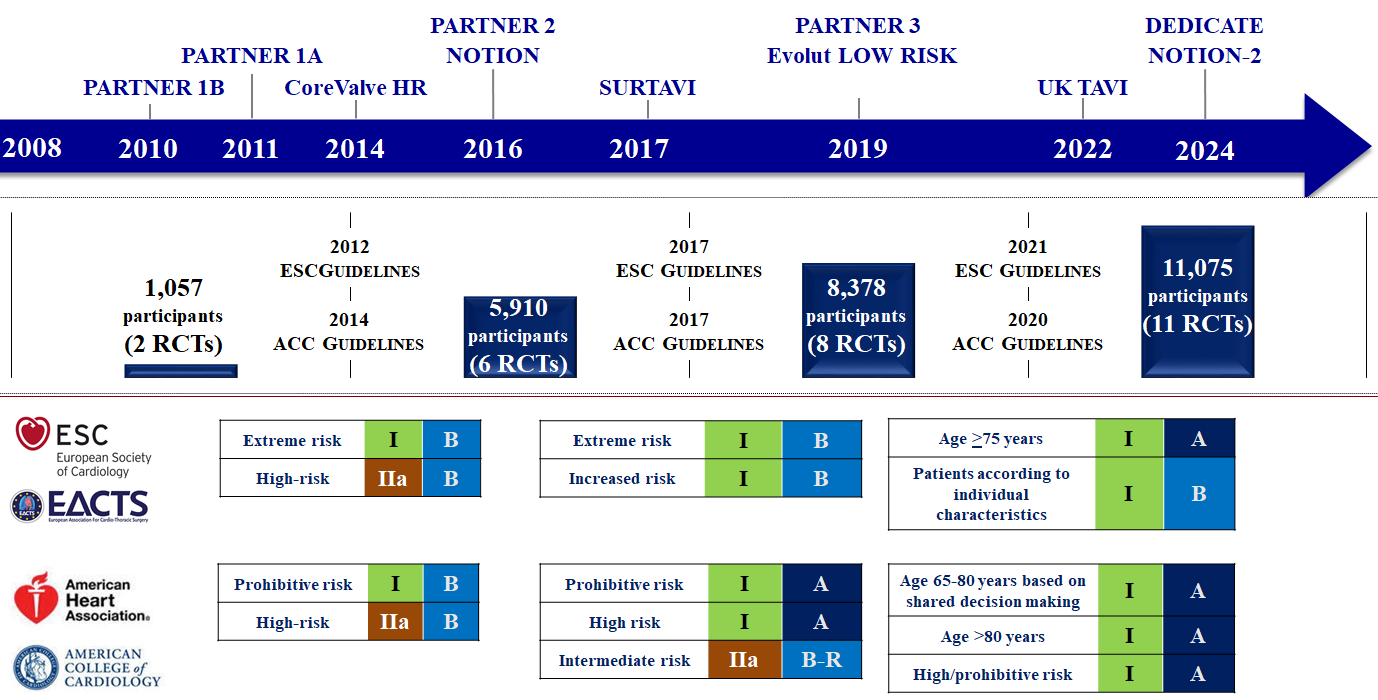
Current ACC/AHA and ESC/EACTS guidelines for the management of valvular heart disease recommend aortic valve intervention (SAVR or TAVI) based on the severity of AS and associated symptoms (Table 3). Although there are differences, both guidelines are generally congruent regarding the timing of AVR, 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. The ACC/AHA guidelines recommend SAVR for patients aged <65 years or with life expectancy >20 years, TAVI for patients aged >80 years or with life expectancy <10 years, and shared decision-making for patients aged 65-80 years39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link. The ESC/EACTS guidelines recommend SAVR in younger patients <75 years of age who are at low surgical risk (society of thoracic surgeons predicted risk of mortality [STS-PROM]/EuroSCORE II <4%) and TAVI in patients ≥75 years of age (Table 4and Figure 7)40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. Since the publication of these guidelines, several trials and updates comparing SAVR and TAVI have become available reporting on longer-term follow-up and new lower risk and younger populations which will impact future guideline recommendations, , , , , , , , , , , , 19. UK TAVI Trial Investigators; Toff WD, Hildick-Smith D, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA. 2022;327:1875-1887. Link21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link46. Makkar RR, Thourani VH, Mack MJ, et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382:799-809 Link47. Jorgensen TH, Thyregod HGH, Ihlemann N, et al. Eight-year outcomes for patients with aortic valve stenosis at low surgical risk randomized to transcatheter vs surgical aortic valve replacement. Eur Heart J. 2021;42:2912-2919 Link48. Leon MB, Mack MJ, Hahn RT, et al. Outcomes 2 Years After Transcatheter Aortic Valve Replacement in Patients at Low Surgical Risk. J Am Coll Cardiol. 2021;77:1149-1161 Link49. Forrest JK, Deeb GM, Yakubov SJ, et al. 2-Year Outcomes After Transcatheter Versus Surgical Aortic Valve Replacement in Low-Risk Patients. J Am Coll Cardiol. 2022;79:882-896 Link50. Van Mieghem NM, Deeb GM, Sondergaard L, et al. Self-expanding Transcatheter vs Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 5-Year Outcomes of the SURTAVI Randomized Clinical Trial. Jama. Cardiol 2022;7:1000-1008 Link51. Forrest JK, Deeb GM, Yakubov SJ, et al. 3-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Low-Risk Patients With Aortic Stenosis. J Am Coll Cardiol. 2023;81:1663-1674 Link52. Forrest JK, Deeb GM, Yakubov SJ, et al. 4-Year Outcomes of Patients With Aortic Stenosis in the Evolut Low Risk Trial. J Am Coll Cardiol. 2023;82:2163-2165 Link53. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement in Low-Risk Patients at Five Years. N Engl J Med. 2023;389:1949-1960 Link54. Thyregod HGH, Jorgensen TH, Ihlemann N, et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. Eur Heart J. 2024;45:1116-1124 Link55. Forrest JK, Yakubov SJ, Deeb GM, et al. 5-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Low-Risk Patients With Aortic Stenosis. J Am Coll Cardiol 2025. [Online ahead of print]. doi: 10.1016/j.jacc.2025.03.004 Link.
Figure 7
Evolution of transcatheter aortic valve implantation through evidence generation and guidelines. Figures reproduced and modified from Windecker et al. Eur Heart J 2024;45(13):1104-1115.
Progressive decrease in LVEF on at least 3 serial imaging studies to <60%
2b
B-NR
/
Severe valve calcification (by CT)*4
/
IIa
B
Indications for other cardiac surgery
1
B-NR
I
C
Moderate AS
Indications for other cardiac surgery
2b
C-EO
IIa
C
*1: AS is the most likely cause of symptoms in ACC/AHA guideline; after careful confirmation that the AS is severe in ESC/EACTS guideline.
*2: A fall in systolic blood pressure of >10 mmHg from baseline during exercise testing in ACC/AHA and >20 mmHg in ESC/EACTS guidelines.
*3: BNP >threefold age- and sex-corrected normal range confirmed by repeated measurements and without other explanation.
*4: Severe AS very likely: (Agatston units): men ≥3000; women ≥1600; Severe AS likely: (Agatston units): men ≥2000; women ≥1200; Severe AS unlikely: (Agatston units): men <1600; women <800
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; BNP = B-type natriuretic peptide; COR = class of recommendation; CT = computed tomography; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; LOE = Level of evidence; LVEF = left ventricular ejection fraction; Vmax = peak transvalvular velocity
Table 4. Guideline recommendations: Mode of intervention
2020 AHA/ACC Valvular Heart Disease Guideline
2021 ESC/EACTS Valvular Heart Disease Guideline
Recommendations
COR
LOE
Recommendations
COR
LOE
Transfemoral TAVI
Patients who are >80 years of age or for younger patients with a life expectancy <10 years and no anatomical contraindication to transfemoral TAVI
1
A
Patients who are age ≥75 years of age, or at a high surgical risk (STS-PROME/EuroScore II >8%), or unsuitable for surgery
I
A
Patients of any age with high or prohibitive surgical risk
1
A
SAVR
Patients who are <65 years of age or have a life expectancy >20 years
1
A
Patients who are <75 years of age and STS-PROME/EuroScore II <4%, operable and unsuitable for transfemoral TAVI
I
B
Asymptomatic patients with severe AS and an abnormal exercise test, very severe AS, rapid progression, or an elevated BNP
1
B-NR
Patients undergoing other cardiac surgery
I
C
Patients in whom a bioprosthetic valve is preferred but valve or vascular anatomy or other factors are not suitable for transfemoral TAVI
1
A
Patients with moderate AS undergoing other cardiac surgery (Heart team decision depending on patient-specific factors)
IIa
C
Transfemoral TAVI or SAVR
Patients who are 65-80 years of age and have no anatomic contraindication to transfemoral TAVI after shared decision making about the balance between expected patient longevity and valve durability
1
A
Remaining patients (Heart team decision depending on patient-specific factors)
I
B
Asymptomatic patients with an LVEF <50% who are 65 to 80 years of age and have no contraindication to transfemoral TAVI
1
B-NR
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; BNP = B-type natriuretic peptide; COR = class of recommendation; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; EuroScore = European System for Cardiac Operative Risk Evaluation; LOE = Level of evidence; LVEF = left ventricular ejection fraction; SAVR = surgical aortic valve replacement; STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality; TAVI = transcatheter aortic valve implantation.
Clinical evidence on TAVI
Randomized controlled trials comparing TAVI vs. SAVR
Evidence generation has been established by comparison of TAVI, mostly with use of a balloon-expandable and a self-expanding THV device with conventional treatments in predominantly elderly patients with symptomatic severe AS across the entire risk spectrum (Figure 7). The cumulative evidence is based on 11 RCTs with more than 11,000 patients (Table 5, Table 6andTable 7).
Table 5. Summary of randomized clinical trials of TAVI versus SAVR/medical treatment.
Clinical Trial Author (year)
Enrolment Year
Number of TAVI cohort (overall)
Age (mean)
STS-PROM (mean)
TAVI Valve
TF access
Primary endpoint
Follow-up
TAVI
SAVR
P value
PARTNER 1A Smith et al. (2011) Mack et al. (2015)
2007-09
348
(699)
83.6 ± 6.8
11.8 ± 3.3
SAPIEN THV
70.1%
All-cause death
1-year
All patients (N = 348)
24.2%
26.8%
P = 0.44 (P = 0.001)#1
Transfemoral cohort (N = 244)
22.2%
26.4%
P = 0.25
(P = 0.002)#1
Transapical cohort (N = 104)
29.0%
27.9%
P = 0.41
5-year
All patients (N = 348)
67.8%
62.4%
P = 0.76
Transfemoral cohort (N = 244)
63%
64%
P = 0.41
Transapical cohort (N = 104)
79%
60%
P = 0.067
PARTNER 1B#2 Leon et al. (2010) Kapadia et al. (2015)
2007-09
179
(358)
83.1 ± 8.6
11.2 ± 5.8
SAPIEN THV
100%
All-cause death
1-year
30.7%
50.7%
P <0.001
5-year
71.8%
93.6%
P <0.0001
CoreValve High risk Adams et al. (2014) Deeb et al. (2016) Gleason et al. (2018)
2011-12
394
(797)
83.2 ± 7.1
7.3 ± 3.0
CoreValve
82.8%
All-cause death
1-year
13.9%
18.7%
P = 0.04
(P<0.001)#1
3-year
32.9%
39.1%
P = 0.068
5-year
55.3%
55.4%
P = 0.50
PARTNER 2A Leon et al. (2016) Makker et al. (2019)
2011-13
1011
(2032)
81.5 ± 6.7
5.8 ± 2.1
SAPIEN XT
76.7%
Composite of all-cause death or disabling stroke
2-year
All patients (N = 1011)
14.5%
16.4%
P = 0.25
(P = 0.001)#1
Transfemoral cohort (N = 775)
16.8%
20.4%
P = 0.05
Transthoracic cohort (N = 236)
27.7%
23.4%
P = 0.31
5-year
All patients (N = 1011)
47.9%
43.4%
P = 0.21
Transfemoral cohort (N = 775)
44.5%
42.0%
P = 0.80
Transthoracic cohort (N = 236)
59.3%
48.3%
P = 0.03
2 to 5 years
Landmark analysis (N = 1011)
36.3%
29.5%
(1.27 [1.06, 1.53])#3
SURTAVI Reardon et al. (2017) Van Mieghem et al. (2022)
2012-16
864
(1660)
79.9 ± 6.2
4.4 ± 1.5
CoreValve, Evolut R
100%
All-cause death or disabling stroke
2-year
12.6%
14.0%
(95% credible interval [Bayesian analysis] for difference -5.2, 2.3])
posterior probability of non-inferiority >0.999
5-year
31.3%
30.8%
P = 0.85
NOTION Thyregod et al. (2015) Thyregod et al. (2019) Jorgense et al. (2021) Thyregod et al. (2024)
2009-13
145
(280)
79.2 ± 4.9
2.9 ± 1.6
CoreValve
96.5%
All-cause death, stroke, myocardial infarction
1-year
13.1%
16.3%
P = 0.43
5-year
38.0%
36.3%
P = 0.86
8-year
54.5%
54.8%
P = 0.94
10-year
65.5%
65.5%
P = 0.9
UK-TAVI Trial Toff et al.(2022)
2014-2018
458
(913)
81 (79-84)
2.6 (2.0-3.5)
Any CE-mark devices
92.0%
All-cause death
1-year
4.6%
6.6%
P <0.001#1
DEDICATE Blankenberg et al. (2024)
2017-2022
701
(1414)
74.3 ± 4.6
1.8 (1.2-2.4)
Any CE-mark devices
97.3%
All-cause death, stroke
1-year
5.4%
10%
P <0.001#1
PARTNER 3 Mack et al. (2019) Mack et al. (ACC 2020)
2016-17
496
(1000)
73.3 ± 5.8
1.9 ± 0.6
SAPIEN 3
100%
All-cause death, stroke, rehospitalization
1-year
8.5%
15.1%
P<0.001
(P = 0.001)#1
2-year
11.5%
17.4%
P = 0.007
5-year
22.8%
27.2%
P = 0.07
Evolut low risk Popma et al. (2019) Forrest et al. (2023) Forrest et al. (2023) Forret et al. (2025)
2016-18
734
(1468)
74.0 ± 5.9
1.9 ± 0.7
CoreValve, Evolut R/PRO
99.6%
All-cause death, disabling stroke
2-year
5.0%
6.6%
(-1.5[-4.9, 1.8])#4
posterior probability of non-inferiority >0.999
3-year
7.4%
10.4%
P = 0.051
4-year
10.7%
14.1%
P = 0.05
5-year
15.5%
16.4%
P = 0.47
NOTION-2 Jorgensen et al. (2024)
2016-2023
187
(370)
71.1 ± 3.1
1.1 (0.9-1.5)
Any CE-mark devices
100%
All-cause mortality, stroke, rehospitalization
1-year
All patients (N = 187)
10.2%
7.1%
P = 0.3
Tricuspid cohort (N = 138)
8.7%
8.3%
P = 0.9
Bicuspid cohort (N = 49)
14.3%
3.9%
P = 0.07
The results provided are from the intention-to-treat analysis except for NOTION trial at 1 year with as-treated analysis.
Numbers, mean age, and mean STS score are of TAVI cohorts.
Blue indicates results with non-inferiority of TAVI versus SAVR or no significant difference between TAVI and SAVR. Yellow indicates results with statistically better outcomes of TAVI over SAVR or superiority of TAVI over SAVR. Red indicates results with statistically better outcomes of SAVR over TAVI.
#1: P value for non-inferiority test.
#2: Results are provided with differences between TAVI and standard treatment.
#3: Results are provided with hazard ratio and 95% confidence intervals (CI).
#4: Results are provided with differences (TAVI-SAVR) and 95% Bayesian credible interval (BCI).
STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality; TA=transapical; TAVI = transcatheter aortic valve implantation; SAVR = surgical aortic valve replacement.
Table 6. Short-term echocardiographic and clinical outcomes comparing TAVI and SAVR in randomized clinical trials.
Trial
Echocardiographic outcomes
30-day Clinical outcomes
AVA (cm2)
mPG (mmHg)
PVR (≥moderate)
All-cause death
Major stroke
Major bleeding
Permanent pacemaker
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
PARTNER 1A Smith et al. (2011)
1.7 ± 0.5
1.5 ± 0.4
9.9 ± 4.8
10.8 ± 5.0
12.2%
0.9%
3.4%
6.5%
11.0%
3.2%
9.3%
19.5%
3.8%
3.6%
P = 0.001
P = 0.004
P<0.001
P = 0.07
P = 0.20
P<0.001
P = 0.89
PARTNER 1B#1 Leon et al. (2010)
1.5 ± 0.4
0.8 ± 0.2
11.4 ± 7.0
33.1 ± 12.6
12%
0%
5.0%
2.8%
5.0%
1.1%
16.8%
3.9%
3.4%
5.0%
NA
NA
NA
P = 0.41
P = 0.06
P<0.001
P = 0.60
CoreValve High risk Adams et al. (2014)
1.95 ± 0.56
1.60 ± 0.51
8.88 ± 3.87
11.71 ± 5.71
9.0%
1.0%
3.3%
4.5%
3.9%
3.1%
28.1%
34.5%
19.8%
7.1%
P<0.001
P<0.001
P<0.001
P = 0.43
P = 0.55
P = 0.05
P<0.001
PARTNER 2A Leon et al. (2016)
1.7 ± 0.5
1.5 ± 0.4
9.7 ± 3.5
10.9 ± 4.3
3.7%
0.6%
3.9%
4.1%
3.2%
4.3%
10.4%
43.4%
8.5%
6.9%
<0.001
<0.001
P<0.001
P = 0.78
P = 0.20
P<0.001
P = 0.17
SURTAVI#2 Reardon et al. (2017)
2.1 ± 0.6
1.8 ± 0.6
8. 9± 4.1
12.4 ± 5.7
3.4%
0.3%
2.2%
1.7%
1.2%
2.5%
12.1%
9.3%
25.9%
6.6%
NA
NA
NA
95%CI [-0.9, 1.8]
95%CI [-2.6, 0.6]
95%CI [-0.1, 5.9]
95%CI [15.9, 22.7]
NOTION#3 Thyregod et al. (2015)
1.7
1.4
8.3
12.2
15.7%
0.9%
2.1%
3.7%
1.4%+
3.0%+
11.3%
20.9%
34.1%
1.6%
P<0.001
P<0.001
P<0.001
P = 0.43
P = 0.37
P = 0.03
P<0.001
UK-TAVI Trial Toff et al.#4, 5 (2022)
1.53 ± 0.48
1.51 ± 0.48
10.36 ± 4.82
10.01 ± 5.12
2.4%
0.9%
1.8%
0.9%
2.4%
2.3%
5.5%
19.5%
11.0%
6.7%
0.04 [-0.02, 0.09]a
0.31 [-0.53, 1.15]a
5.37 [3.86, 7.46]a
1.91 [0.52-7.03]
1.05 [0.35-3.17]
0.27 [0.19-0.37]
1.72 [1.13-2.61]
DEDICATE#5 Blankenberg et al. (2024)
1.8 (1.5-2.1)
1.7 (1.4-2.0)
11.0 (8.0-14.9)
11.0 (8.0-14.2)
1.7%
0.7%
0.7%
1.5%
0.6%
1.7%
3.5%
12.7%
8.3%
4.1%
-0.1 [-0.1, 0.0]b
0.0 [-0.5, 0.6]b
NA
0.55 [0.18-1.50]
0.35 [0.11-0.97]
0.26 [0.16-0.40]
2.09 [1.35-3.32]
PARTNER 3#5 Mack et al. (2019)
1.7
1.8
12.8
11.2
0.8%
0%
0.4%
1.1%
0%
0.4%
3.6%
24.5%
6.5%
4.0%
NA
NA
NA
0.37 [0.07, 1.88]
0.00 [NA]
0.12 [0.07, 0.21]
1.66 [0.93, 2.96]
Evolut low risk#2 Popma et al. (2019)
2.2 ± 0.6
2.0 ± 0.6
8.4 ± 3.5
10.5 ± 4.0
3.4%
0.4%
0.5%
1.3%
0.5%
1.7%
2.4%
7.5%
17.4%
6.1%
NA
NA
NA
-0.8 [-1.9, 0.2]
-1.2 [-2.4, -0.2]
-5.1 [-7.5, -2.9]
11.3 [8.0, 14.7]
NOTION-2#5 Jorgensen et al. (2024)
1.8
1.6
10.6
12.6
4.7%
0%
0.5%
1.1%
0.5%
1.1%
3.7%
16.9%
12.8%
4.6%
NA
NA
P = 0.005
0.5 [0.04-5.9]
0.5 [0.04-5.3]
0.2 [0.1-0.5]
2.9 [1.3-6.6]
The results of PARTNER 1A, PARTNER 2A, PARTNER 2B, PARTNER 3, SURTAVI, UK-TAVI Trial, DEDICATE, PARTNER 3, and NOTION-2 are provided from intention-to-treat analyses.
The results of U.S. CoreValve High risk, NOTION, and Evolut low risk are provided from as-treated analyses.
Blue indicates results with no significant difference between TAVI and SAVR. Yellow indicates results with statistically better outcomes of TAVI over SAVR. Red indicates results with statistically better outcomes of SAVR over TAVI.
#1: Results are provided with differences between TAVI and standard treatment.
#2: Results are provided with differences (TAVI-SAVR) and 95% Bayesian credible interval (BCI).
#3: Echocardiographic data at discharge or 30 days was not provided. The echocardiographic results are at 3-month follow-up.
#4: Echocardiographic data at discharge or 30 days was not provided. The echocardiographic results are at 6-week follow-up.
#5: Results are provided with hazard ratios and 95% confidence intervals (CI).
a: Treatment effect and 95% confidence intervals (CI) (TAVI vs. SAVR).
b: median difference and 95% confidence intervals (CI) (TAVI vs. SAVR).
Table 7. Long-term clinical outcomes comparing TAVI and SAVR in randomized clinical trials.
Period
1-year
Longest follow-up
Clinical outcome
All-cause death
Cardiovascular death
Rehospitalization
Major stroke
Reintervention
All-cause death
Cardiovascular death
Rehospitalization
Major stroke
Reintervention
TAVI vs. SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
TAVI
SAVR
PARTNER 1A Smith et al. (2011) Mack et al. (2015)
24.2%
26.8%
14.3%
13.0%
18.2%
15.5%
5.1%
2.4%
/
67.8%
62.4%
53.1%
47.6%
42.3%
34.2%
10.4%
11.3%
/
P = 0.44
P = 0.63
P = 0.38
P = 0.07
P = 0.76
P = 0.67
P = 0.17
P = 0.61
PARTNER 1B#1 Leon et al. (2010) Kapadia et al. (2015)
30.7%
49.7%
19.6%
41.9%
22.3%
44.1%
7.8%
3.9%
/
71.8%
93.6%
71.8%
92.7%
47.6%
87.3%
16.0%+
18.2%+
/
P<0.001
P<0.001
P<0.0001
P = 0.18
P<0.0001
P<0.0001
P<0.0001
P = 0.555
CoreValve High risk Adams et al. (2014) Gleason et al. (2018)
14.2%
19.1%
10.4%
12.8%
16.5%
13.9%
5.8%
7.0%
1.9%
0.0%
55.3%
55.4%
39.7%
39.5%
37.5%
31.5%
12.3%
13.2%
3.0%
1.1%
P = 0.04
P = 0.31
NA
P = 0.59
P = 0.01
P = 0.50
P = 0.80
P = 0.08
P = 0.49
P = 0.04
PARTNER 2A Leon et al. (2016) Makkar et al. (2020)
12.3%
12.9%
7.1%
8.1%
14.8%
14.7%
5.0%
5.8%
1.2%
0.5%
46.0%
42.1%
29.4%
27.8%
33.3%
25.2%
9.8%
8.6%
3.2%
0.8%
P = 0.69
P = 0.40
P = 0.92
P = 0.46
P = 0.10
HR 1.09 [0.95-1.25]
HR 1.02 [0.85-1.23]
HR 1.28 [1.07-1.53]
HR 1.05 [0.77-1.44]
HR 3.28 [1.32-8.13]
SURTAVI Reardon et al. (2017) Van Mieghem et al. (2022)
7.0%
6.8%
4.8%
5.5%
9.0%
8.7%
2.2%
3.7%
2.0%
0.5%
30.0%
28.7%
17.8%
17.4%
23.9%
20.8%
4.1%
5.8%
3.5%
1.9%
95% credible interval for the difference -2.3, 2.7
95% credible interval for the difference -2.9, 1.5
95% credible interval for the difference -2.6, 3.1
95% credible interval for the difference -3.2, 0.2
95% credible interval for the difference 0.3, 2.6
P = 0.55
P = 0.84
P = 0.13
P = 0.11
P = 0.02
NOTION Thyregod et al. (2015) Thyregod et al. (2024)
4.9%
7.5%
4.3%
7.5%
/
2.9%+
4.6%+
/
62.7%
64.0%
49.5%
51.2%
/
9.7%+
16.4%+
4.3%
2.2%
P = 0.38
P = 0.25
P = 0.44
P = 0.8
P = 0.7
P = 0.1
P = 0.3
UK-TAVI Trial Toff et al. (2022)
4.6%
6.6%
2.8%
3.3%
/
5.2%+
2.6%+
2.2%
1.1%
/
Adjusted HR 0.69 [0.38-1.26]
Adjusted HR 0.86 [0.40-1.83]
Adjusted HR 1.98 [0.95-4.11]
Adjusted HR 1.98 [0.72-5.42]
DEDICATE Blankenberg et al. (2024)
2.6%
6.2%
2.0%
4.4%
12.2%
13.3%
1.3%
3.1%
0.6%
0.3%
/
HR 0.43 (0.24-0.73)
HR 0.47 (0.24-0.86)
HR 0.89 (0.66-1.20)
HR 0.42 (0.19-0.88)
HR 1.70 (0.38-9.78)
PARTNER 3 Mack et al. (2019) Mack et al. (2023)
1.0%
2.5%
0.8%
2.0%
7.3%
11.0%
0.2%
0.9%
0.6%
0.5%
10.0%
8.2%
5.5%
5.1%
13.7%
17.4%
2.9%
2.7%
2.6%
3.0%
HR 0.41 (0.14-1.17)
HR 0.40 (0.12-1.30)
HR 0.65 (0.42-1.0)
HR 0.22 (0.03-2.0)
HR 1.33 (0.22-7.95)
HR 1.23 (0.79-1.90)
HR 1.08 (0.61-1.92)
HR 0.75 (0.54-1.05)
HR 1.03 (0.46-2.30)
HR 0.86 (0.39-1.92)
Evolut low risk Popma et al. (2019) Forrest et al. (2023)
2.4%
3.0%
1.7%
2.6%
3.2%
6.5%
0.8%
2.4%
0.7%
0.6%
13.5%
14.9%
7.2%
9.3%
13.9%
15.1%
3.6%
4.0%
3.3%
2.5%
Difference -0.6 95% BCI [-2.6, 1.3]
Difference -0.9 95% BCI [-2.7, 0.7]
Difference -3.4 95% BCI [-5.9, -1.0]
Difference -1.6 95% BCI [-3.1, -0.3]
Difference 0.0 95% BCI [-1.0, 0.9]
P = HR 0.88 (0.66-1.17)
P = HR 0.75 (0.51-1.11)
P = HR 0.89 (0.67-1.19)
P = HR 0.85 (0.49-1.49)
HR 1.30 (0.66-2.56)
NOTION-2 Jorgensen et al. (2024)
2.1%
1.1%
2.1%
1.1%
3.7%
4.9%
1.6%
1.1%
1.1%
2.2%
/
HR 2.0 (0.4-10.7)
HR 2.0 (0.4-10.7)
HR 0.7 (0.3-2.0)
HR 1.5 (0.2-8.8)
HR 0.5 (0.1-2.7)
Only 1-year results are shown in the UK-TAVI, DEDICATE, and NOTION-2 trials.
1- and 5-year results are shown in the PARTNER 1A and 1B, PARTNER 2, PARTNER 3, CoreValve High Risk, SURTAVI, and Evolut low risk trials.
1- and 10-year results are shown in the NOTION trial.
Results of the CoreValve High risk, NOTION, and Evolut low risk trials are provided from as-treated analyses.
Blue indicates results with no significant difference between TAVI and SAVR. Yellow indicates results with statistically better outcomes of TAVI over SAVR. Red indicates results with statistically better outcomes of SAVR over TAVI.
#1: Results are provided with differences between TAVI and standard treatment.
The PARTNER 1 trial consisted of 2 randomized cohorts: Cohort A, which compared transfemoral/transapical TAVI with the Edwards SAPIEN balloon-expandable valve system (N = 348) or SAVR (N = 351) in high-risk patients11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link; and Cohort B, which randomized inoperable patients to either conservative treatment – including balloon aortic valvuloplasty (N = 179) or transfemoral TAVI (N = 179)10. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607. Link. The primary endpoint was all-cause death at 1 year.
In Cohort B (mean age: 83 years, STS-PROM: 11.2%), TAVI was associated with a 20% absolute risk reduction in all-cause mortality compared with conservative treatment at 1 year (30.7% vs. 50.7%, hazard ration [HR] 0.55, 95% confidence interval [CI] 0.40-0.74, P <0.001) (NNT=5)10. Leon MB, Smith CR, Mack M, et al. Transcatheter aortic-valve implantation for aortic stenosis in patients who cannot undergo surgery. N Engl J Med. 2010;363:1597-1607. Link. The follow-up data reported up to 5 years showed TAVI to maintain superiority over medical treatment. At the end of 5-year follow-up, overall mortality was 71.8% in the TAVI group compared with 93.8% in the medical treatment group (HR 0.50, 95% CI 0.39-0.65, P <0.001)56. Kapadia SR, Leon MB, Makkar RR, et al. 5-year outcomes of transcatheter aortic valve replacement compared with standard treatment for patients with inoperable aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2485-2491 Link.
In cohort A (mean age: 84 years, STS-PROM: 11.8%), TAVI was non-inferior to SAVR in terms of all-cause death at 1 year (24.2 vs. 26.8%, Pnon-inferiority = 0.001)11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link. At 5-year follow-up, the risk of all-cause death remained similar between TAVI and SAVR (67.8% vs. 62.4%, HR 1.04, 95% CI 0.86-1.24)57. Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2477-2484 Link. In a stratified analysis by access site, there was no difference in mortality between transfemoral TAVI and SAVR (63% vs. 64%, P = 0.41), while transapical TAVI was associated with a numerically higher risk of mortality (79% vs. 60%, P = 0.067) compared with SAVR at 5 years. The risk of repeat hospitalization (42.3% vs. 34.2%, P = 0.17), stroke (10.4% vs. 11.3%, P = 0.61), and myocardial infarction (2.9% vs. 5.9%, P = 0.15), and functional status (New York Heart Association [NYHA] class I or II: 85% vs. 81%, P = 0.57) were comparable between the groups up to 5 years. Major vascular complications were more frequent after TAVI (11.9% vs. 4.7%, P = 0.0002), while major bleeding more frequently occurred after SAVR (26.6% vs. 34.4%, P = 0.003)57. Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2477-2484 Link.
CoreValve US High Risk
The CoreValve US High Risk trial was the first trial comparing SAVR with TAVI using the self-expanding CoreValve system in 795 high-risk patients (mean age: 83 years, STS-PROM: 7.3%). The primary endpoint was all-cause death at 1 year. TAVI was predominantly performed via transfemoral access (82.8%). TAVI was associated with a significantly lower risk of all-cause death at 1 year than SAVR (14.2% vs. 19.1%, Pnon-inferiority <0.001, Psuperiority = 0.04)12. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790-1798 Link. At 5 years, both TAVI and SAVR resulted in similar survival outcomes (all-cause death: 55.3% vs. 55.4%, HR 0.93, 95% CI 0.77 to 1.14, P = 0.5). The risk of repeat hospitalization (37.5% vs. 31.5%, P = 0.08), major stroke (12.3% vs. 13.2%, P = 0.49), and myocardial infarction (3.1% vs. 3.3%, P = 0.93), and functional status (NYHA class mean of 1.3 in both groups) were comparable between the groups up to 5 years, while major vascular complications (7.1% vs. 2.0%, P = 0.001) and repeat aortic valve intervention (3.0% vs. 1.1%, P = 0.04) occurred more frequently in the TAVI group and major bleedings was more frequently observed (35.9% vs. 43.3%, P = 0.05) in the SAVR group throughout 5-year follow-up58. Gleason TG, Reardon MJ, Popma JJ, et al. 5-Year Outcomes of Self-Expanding Transcatheter Versus Surgical Aortic Valve Replacement in High-Risk Patients. J Am Coll Cardiol. 2018;72:2687-2696 Link.
PARTNER 2
The PARTNER 2 trial randomly assigned 2,032 intermediate-risk patients (mean age: 82 years, STS-PROM: 5.8%) to SAVR or TAVI with the balloon-expandable SAPIEN XT system. Patients were stratified in cohorts according to access route (transfemoral 76.3% or transthoracic 23.7%). The primary endpoint was the composite of all-cause death or disabling stroke and TAVI was non-inferior to SAVR in terms of the primary endpoint at 2 years (19.3% vs. 21.1%, Pnon-inferiority = 0.001). In the transfemoral access cohort, TAVI resulted in a lower rate of death or disabling stroke than SAVR (HR 0.79, 95% CI 0.62-1.00, P = 0.05), while in the transthoracic access cohort, outcomes were similar between the two groups (HR 1.21, 95% CI 0.84-1.74, P = 0.31)14. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374:1609-1620. Link. At 5-year follow-up, no significant difference was observed in the primary endpoint between the TAVI group and the SAVR group (47.9% vs. 43.4%, HR 1.09. 95% CI 0.95-1.25, P = 0.21). Results were similar for the transfemoral access cohort (44.5% vs. 42.0%, HR 1.02, 95% CI 0.87-1.20), while TAVI was associated with an increased risk of the primary endpoint compared to SAVR in the transthoracic-access cohort (59.3% vs. 48.3%, HR 1.32, 95% CI 1.02-1.71). Improvements in health status (NYHA class I or II: 89.0% vs. 92.7%; average increase in the Kansas City Cardiomyopathy Questionnaire [KCCQ] Overall Summary score: 19.6 points and 20.5 points) were also similar at 5 years. More patients in the TAVI group than in the SAVR group had aortic-valve reintervention (3.2% vs. 0.8%, HR 3.28, 95% CI 1.32-8.13) and repeat hospitalization (33.3% vs. 25.2%, HR 1.28, 95% CI 1.07-1.53) at 5 years46. Makkar RR, Thourani VH, Mack MJ, et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382:799-809 Link.
SURTAVI
The SURTAVI trial (N = 1,746) was a randomized trial designed to compare the safety and efficacy of TAVI with the CoreValve (84%) or the Evolut R (16%) self-expanding valve system and SAVR in intermediate-risk patients (mean age: 80 years, STS-PROM: 4.4%). TAVI was predominantly performed via transfemoral access (94%), while subclavian (2%) or direct aortic (4%) approaches were used in patients with unsuitable iliofemoral anatomy. The primary endpoint was the composite of all-cause death or disabling stroke at 2 years. Consistent with prior studies, TAVI was non-inferior to SAVR for the primary endpoint (12.6% vs. 14.0%, difference -1.4 percentage points, 95% Bayesian credible interval for difference [BCI] -5.2 to 2.3%, posterior probability of non-inferiority >0.999)15. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376:1321-1331 Link. At 5 years, rates of all-cause death (30.0% vs. 28.7%, P = 0.55), rehospitalization (23.9% vs. 20.8%, P = 0.13), and major stroke (4.1% vs. 5.8%, P = 0.11) were similar between the TAVI and SAVR groups, while repeat aortic valve intervention occurred more frequently in the TAVI group (3.5%vs. 1.9%, P = 0.02)50. Van Mieghem NM, Deeb GM, Sondergaard L, et al. Self-expanding Transcatheter vs Surgical Aortic Valve Replacement in Intermediate-Risk Patients: 5-Year Outcomes of the SURTAVI Randomized Clinical Trial. Jama. Cardiol 2022;7:1000-1008 Link.
NOTION
The NOTION I trial randomized patients with severe AS (age ≥70 years and no evidence of significant coronary artery disease) irrespective of surgical risk to TAVI with the self-expanding CoreValve valve system or SAVR. A total of 280 patients (mean age 79 years, STS-PROM: 2.9%) were included, and the majority of patients (81.8%) were considered low-risk patients. The primary endpoint was the composite of all-cause death, stroke, or myocardial infarction at 1 year. There were no differences between TAVI and SAVR for the primary endpoint (13.1% vs. 16.3%, Psuperiority = 0.43) or any of its components at 1 year13. Thyregod HG, Steinbrüchel DA, Ihlemann N, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65:2184-2194 Link. At 10 years of follow-up, the risk of the composite primary outcome of all-cause mortality, stroke, or myocardial infarction was 65.5% in the TAVI group and 65.5% in the SAVR group with no significant difference (HR = 1.0, 95% CI 0.7-1.3, P = 0.9). Although there was no difference in the rate of the components of the primary endpoint, TAVI was associated with a higher rate of new permanent pacemaker implantation (44.7% vs. 14.0, P <0.01) and SAVR had higher rate of new-onset atrial fibrillation (52.0% vs. 74.1%, P <0.01). The rate of aortic valve reintervention was low and similar for the two types of AVR (TAVI 4.3% and SAVR 2.2%, P = 0.3)54. Thyregod HGH, Jorgensen TH, Ihlemann N, et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. Eur Heart J. 2024;45:1116-1124 Link.
UK-TAVI
The UK-TAVI trial was an investigator-initiated, multicenter, RCT involving all National Health Service hospitals performing TAVI in the UK, including 913 patients aged 70 years or older with severe, symptomatic AS and moderately increased operative risk due to age or comorbidity (median age: 81, STS-PROM: 2.6%). TAVI was performed using any valve with a CE mark (balloon expandable valves 57.3%, self-expanding valves: 31.6%, mechanically-expanding valve: 9.6%) and via any access route (transfemoral access: 92.0%). At 1 year, the primary endpoint of all-cause mortality was 4.6% in the TAVI group and 6.6% in the SAVR group (Pnon-inferiority <0.001). TAVI was associated with a reduced risk of major bleeding (7.2% vs. 20.2%), whereas vascular complications (10.3% vs. 2.4%), conduction disturbances requiring pacemaker implantation (14.2% vs. 7.3%), and mild or moderate aortic regurgitation (2.3% vs. 0.6%) were more frequently observed in the TAVI group19. UK TAVI Trial Investigators; Toff WD, Hildick-Smith D, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA. 2022;327:1875-1887. Link.
PARTNER 3
The PARTNER 3 trial was a randomized trial (N = 1,000) that compared transfemoral TAVI using the balloon-expandable SAPIEN 3 valve system with SAVR in low-risk patients (mean age: 73 years, STS-PROM: 1.9%). The primary endpoint was the composite of all-cause death, any stroke, or repeat hospitalization at 1 year. The rate of the primary endpoint was lower in the TAVI group than in the SAVR group (8.5% vs. 15.1%, absolute difference -6.6 percentage points, 95%CI -10.8 to -2.5, Pnon-inferiority <0.001, HR 0.54, 95% CI 0.37 to 0.79, Psuperiority = 0.001). TAVR resulted in a lower rate of stroke (0% vs. 0.4%, P <0.001) and new-onset atrial fibrillation (5.0% vs. 39.5%, P <0.001) at 30 days, while there were no significant between-group differences in major vascular complications, new permanent pacemaker insertions, or moderate or severe paravalvular regurgitation (PVR)16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link. At 5-year follow-up, rates of the composite clinical outcome (22.8% vs. 27.2%, HR 0.79, 95% CI 0.61-1.02) and its components (all-cause death: 10.0% vs. 8.2%, HR 1.23, 95% CI 0.79-1.90; any stroke: 5.8% vs. 6.4%, HR 0.87, 95% CI 0.51-1.48, rehospitalization: 13.7% vs. 17.4%, HR 0.75, 95% CI 0.54-1.05) were similar among patients assigned to TAVI and SAVR, respectively. The rate of aortic valve reintervention (2.6% in the TAVI group and 3.0% in the SAVR group) and the proportion of patients who were alive with a KCCQ Overall Summary score of 75 or higher (indicative of being well) were similar in the two groups (71.0% in the TAVI group and 71.9% in the SAVR group), while valve thrombosis according to the Valve Academic Research Consortium (VARC)-3 definition was higher in the TAVR group (2.5% vs. 0.2%, HR 10.52, 95% CI 1.37-80.93). This trial is planned to be followed for 10 years53. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement in Low-Risk Patients at Five Years. N Engl J Med. 2023;389:1949-1960 Link.
Evolut Low Risk
The Evolut Low Risk trial was a randomized trial (N = 1,468) that compared TAVI with the self-expanding CoreValve (3.6%), Evolut R (74.1%), or Evolut PRO (22.3%) system with SAVR in low-risk patients (mean age: 73 years, STS-PROM: 1.9%). The primary endpoint was the composite of all-cause death or disabling stroke at 2 years. TAVI was performed predominantly using transfemoral access (99.0%). When 850 patients had reached 1-year follow-up, data were analysed using Bayesian methods. At 2 years, TAVI met non-inferiority compared to SAVR in terms of the primary endpoint (5.3% vs. 6.7%, difference -1.4 percentage points, 95% BCI -4.0 to 2.1, posterior probability of non-inferiority >0.999). TAVI resulted in a lower incidence of disabling stroke (0.5% vs. 1.7%, difference -1.2, 95% BCI -2.4 to -0.2), bleeding complications (7.7% vs. 35.4%. difference -5.1, 95% BCI -7.5 to -2.9), acute kidney injury (0.9% vs. 2.8%, difference -1.8, 95% BCI -3.4 to -0.5), and new-onset atrial fibrillation (7.7% vs. 35.4%, difference -27.7, 95% BCI -31.8 to -23.6) at 30 days, as compared to SAVR. Conversely, the rates of new permanent pacemaker implantation (17.4% vs. 6.1%, difference 11.3, 95% BCI 8.0 to 14.7) were higher in the TAVI group than in the SAVR group17. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380:1706-1715 Link. At 5 years, there was no significant difference in the primary endpoint (15.5% vs. 16.4%; HR: 0.90; 95% CI: 0.69-1.18; P = 0.47) and its components (all-cause death: 13.5% vs. 14.9%; HR: 0.88; 95% CI: 0.66-1.17; P = 0.39; disabling stroke: 3.6% vs. 4.0%; HR: 0.85; 95% CI: 0.49-1.49; P = 0.57) between groups. Valve reintervention was required in 3.3% and 2.5% of patients in the TAVI and SAVR groups, respectively (HR 1.30, 95% CI 0.66-2.56, P = 0.44), while the incidence of clinical and subclinical valve thrombosis was low in both groups (0.3% vs. 0.2%, HR 1.84, 95% CI 0.17-20.24, P = 0.61, and 0.6% vs. 0.5%, HR 1.20, 95% CI 0.27-5.37, P = 0.81, respectively). The proportion of patients who were alive and well (alive and KCCQ summary score >75) were similar between the TAVI and surgery groups (70.6% and 69.3%, respectively)55. Forrest JK, Yakubov SJ, Deeb GM, et al. 5-Year Outcomes After Transcatheter or Surgical Aortic Valve Replacement in Low-Risk Patients With Aortic Stenosis. J Am Coll Cardiol 2025. [Online ahead of print]. doi: 10.1016/j.jacc.2025.03.004 Link.
DEDICATE-DZHK6
The DEDICATE trial was an investigator-initiated RCT comparing SAVR with TAVI using any CE-marked devices in patients with severe symptomatic AS who were at low or intermediate surgical risk (N = 1,414, mean age of 74 years, STS-PROM 1.8%). The primary outcome was a composite of death from any cause or fatal or nonfatal stroke at 1 year. The Kaplan–Meier estimate of the primary outcome at 1 year was 5.4% in the TAVI group and 10.0% in the SAVR group (HR 0.53; 95% CI 0.35-0.79; Pnon-inferiority <0.001). The incidence of death from any cause was 2.6% in the TAVI group and 6.2% in the SAVR group (HR 0.43; 95% CI 0.24-0.73); the incidence of stroke was 2.9% and 4.7%, respectively (HR 0.61; 95% CI 0.35-1.06). At 1 year, TAVI was associated with an increased risk of new-onset conduction disturbances (left bundle branch block [LBBB]: 32.0% vs. 17.5%; HR 2.03; 95% CI 1.63-2.54; and permanent pacemaker implantation: 11.8% vs. 6.7%; HR 1.81; 95% CI 1.27-2.61, respectively) and vascular access-site complications (7.9% vs. 0.7%; HR 10.64; 95% CI 4.84-28.94), while SAVR was associated with a higher risk of new-onset atrial fibrillation (12.4% vs. 30.8%; HR 0.36; 95% CI 0.28-0.46) and major or life-threatening or disabling bleeding (4.3% vs. 17.2%; HR 0.24; 95% CI 0.16-0.35)21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link.
NOTION-2
The NOTION-2 trial randomized 370 low-risk patients aged ≤75 years with severe symptomatic AS to TAVI or SAVR, including both tricuspid and bicuspid AS (mean age of 71.1 years and a median STS-PROM of 1.1%). The primary endpoint was a composite of all-cause mortality, stroke, or rehospitalization (related to the procedure, valve, or heart failure) at 12 months. The rate of the primary endpoint in the overall cohort was 10.2% in the TAVI group and 7.1% in the surgery group (absolute risk difference 3.1%; 95% CI -2.7% to -8.8%; HR 1.4; 95% CI, 0.7-2.9; P = 0.3). Patients undergoing TAVI had a lower risk of major or life-threatening bleeding (4.8% vs. 17.5%, HR 0.3, 95% CI 0.1-0.5) and new-onset atrial fibrillation (3.2% vs. 41.7%, HR 0.06, 95% CI 0.03-0.2) and a higher risk of non-disabling stroke (3.7% vs. 0.5%, HR 7.0, 95% CI 0.9-56.5), permanent pacemaker implantation (15.1% vs. 8.0%, HR 2.0, 95% CI 1.1-3.8), and moderate or greater PVR (4.7% vs. 0%, P = 0.005) compared to SAVR. The risk of the primary composite endpoint was similar in patients with tricuspid AS (8.7% in the TAVI group vs. 8.3% in the SAVR group, HR 1.0; 95% CI 0.5-2.3), while in patients with bicuspid AS, TAVI showed a trend towards a higher risk of the primary composite endpoint (14.3% vs. 3.9%, HR 3.8; 95% CI 0.8-18.5). Of note, the risk of stroke (4.1% vs. 0%, HR 4.1, 95% CI -1.5 to -9.6) and moderate or greater PVR (9.1% vs. 0%, HR 9.1, 95% CI 0.6-17.6) was more pronounced in bicuspid patients undergoing TAVI compared with SAVR22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link.
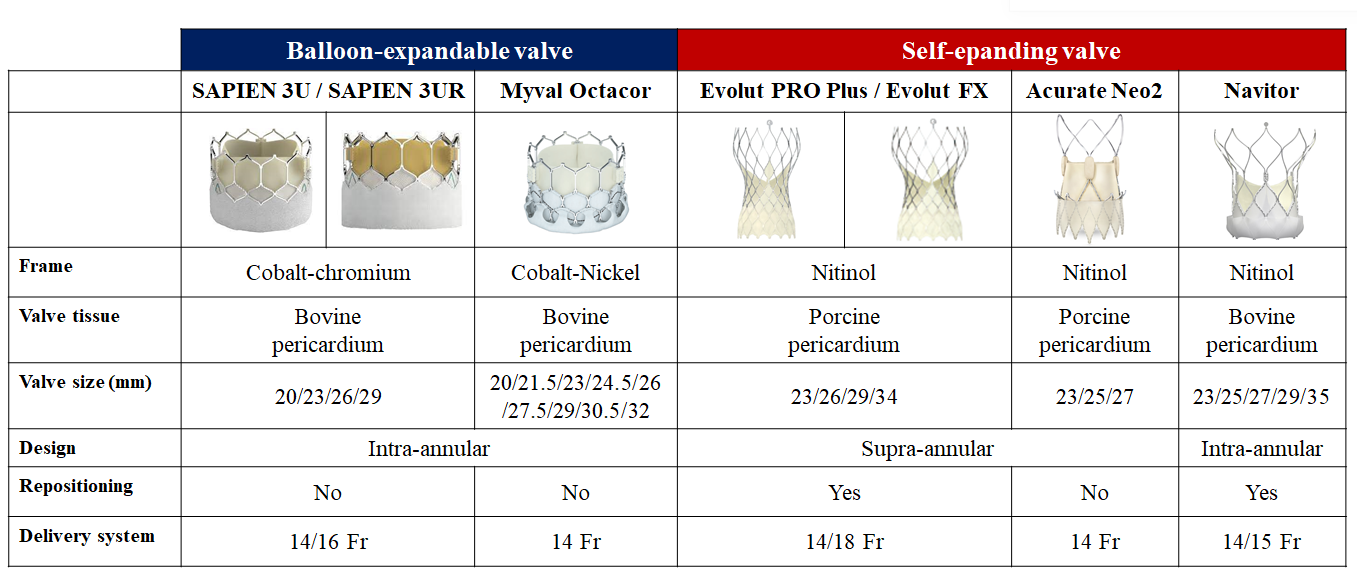
The evidence base for TAVI is dominated by two landmark THV devices, the balloon-expandable SAPIEN and the self-expanding CoreValve/Evolut family of devices. In parallel, there have been prolific efforts to develop novel TAVI devices, which are being evaluated in direct head-to-head device comparisons59. Windecker S, Tomii D. Myval transcatheter heart valve system: a new TAVI contender and remaining uncertainties. EuroIntervention. 2025;21:e97-e99. Link. In this section, we review RCTs comparing TAVI devices which are relevant to inform device selection for individual patients (Table 8 andFigure 8).
Figure 8
Contemporary transcatheter aortic valve implantation devices for the treatment of severe aortic stenosis.
Table 8. Device comparisons in randomized clinical trials.
Clinical Trial Author (year)
Study design
N
Valve performance at 30d
PPI at 30d
Primary endpoint
Main result
mPG (mmHg)
≥mod PVR
CHOICE Abdel-Wahab et al. (2014)
SAPIEN XT vs. CoreValve
121 vs. 120
8.9 vs. 6.6 (P<0.01)
0% vs. 7.2% (P = 0.03)
17.3% vs. 37.6% (P = 0.001)
Device success as defined by the VARC criteria$
95.9% vs. 77.5% (P<0.001)
SCOPE I Lanz et al. (2019)
ACURATE neo vs. SAPIEN 3
372 vs. 367
7 vs. 11 (P<0.0001)
9.4% vs. 2.8% (P<0.0001)
10% vs. 9% (P = 0.76)
Combination of two VARC-2-derived endpoints (early safety and clinical efficacy) at 30 days*
24% vs. 16% (Pnon-inferiority = 0.42)
PORTICO IDE Makkar et al. (2020)
Portico vs. Commercial Valve
381 vs. 369
8.36 vs. 7.31 (P = 0.012)
6.1% vs. 1.6% (P = 0.008)
27.7% vs. 11.6% (P<0.0001)
Safety endpoint: composite of all-cause mortality, disabling stroke, life-threatening or disabling bleeding requiring transfusion, acute kidney injury requiring dialysis, or major vascular complication at 30 days.
13.8% vs. 9.6% (Pnon-inferiority=0.034)
Efficacy endpoint: composite of all-cause mortality or disabling stroke at 1 year.
14.8% vs. 13.4% (Pnon-inferiority=0.0058)
SCOPE II Tamburino et al. (2020)
ACURATE neo vs. Evolut R/PRO
398 vs. 398
6.3 vs. 6.4 (P = 0.70)
10% vs. 3% (P = 0.002)
11% vs. 18% (P = 0.0027)
Powered for non-inferiority of the ACURATE neo THV, was the composite of all-cause death or stroke at 1 year
15.8% vs. 13.9% (Pnon-inferiority = 0.0549)
SOLVE-TAVI Thiele et al. (2019)
Evolut R vs. SAPIEN 3
219 vs. 219
3.4% vs. 1.5% (P = 0.0002)
23.0% vs. 19.2% (P = 0.06)
The efficacy composite endpoint of all-cause mortality, stroke, moderate/severe PVR, and permanent pacemaker implantation at 30 days
28.4% vs. 26.1% (Pequivalence = 0.04)
LANDMARK Baumbach et al. (2024)
Myval/Myval Octaor vs. SAPIEN 3/SAPIEN 3 Ultra or Evolut R/PRO/PRO Plus/FX
384 vs. 384
8.2 vs. 7.9
3% vs. 5% (P = 0.58)
15% vs. 17% (P = 0.49)
Composite of all-cause mortality, all stroke, bleeding (types 3 and 4), acute kidney injury (stages 2–4), major vascular complications, moderate or severe prosthetic valve regurgitation, and conduction system disturbances resulting in a permanent pacemaker implantation at 30 days
25% vs. 27% (Pnon-inferiority <0.0001)
ACURATE IDE Reardon (2024)
Acurate Neo 2 vs. SAPIEN 3/SAPIEN 3 Ultra or Evolut R/PRO/PRO Plus/FX
752 vs. 748
8.0 vs. 12.0 (SAPIEN) or 7.0 (Evolut)
1.1% vs. 0% (SAPIEN) or 0.8% (Evolut)
12.0% vs.12.8%
(HR 0.83, 95% CI 0.69-1.26)
Composite of all-cause mortality, stroke, or rehospitalization (hospitalization for valve related symptoms or worsening congestive heart failure [NYHA class III or IV]; per VARC 2 definition) at 1 year
16.2% vs. 9.5%
(Posterior Median Difference
and 95% BCI: 6.63% [3.04%, 10.2%])
COMPARE-TAVI 1 Terkelsen et al. (2025)
Myval/Myval Octaor vs. SAPIEN 3/SAPIEN 3 Ultra
514 vs. 517
9 vs. 11 (P<0.001)
2.2% vs. 0.6% (P = 0.031)
19.3% vs. 10.5% (P<0.001)
Composite of all-cause mortality, stroke, moderate or severe aortic regurgitation, or moderate or severe haemodynamic valve deterioration at 1 year
13.8% vs. 13.0% (Pnon-inferiority = 0.02)
Reintervention: valve-related, procedural related dysfunction requiring repeat procedure
Rehospitalization: valve-related, procedure-related, or heart failure-related rehospitalization.
The results of SCOPE 1, PORTICO IDE, SCOPE 2, SOLVE-TAVI, LANDMARK, ACURATE IDE, and COMPARE-TAVI 1 trials are provided from intention-to-treat analyses.
Blue indicates results with no significant difference between devices. Yellow indicates results with significant difference between devices.
$: Composite endpoint including (1) successful vascular access, delivery, and deployment of the device and successful retrieval of the delivery system; (2) correct position of the device in the proper anatomical location; (3) intended performance of the prosthetic heart valve (AVA >1.2 cm2, mean aortic valve gradient <20 mmHg, or peak velocity <3 m/s, without moderate or severe prosthetic valve aortic regurgitation); and (4) only 1 valve implanted in the proper anatomical location.
*: Composite of all-cause death, any stroke, life-threatening or disabling bleeding, major vascular complications, coronary artery obstruction requiring intervention, acute kidney injury (stage 2 or higher), rehospitalization for valve-related symptoms or congestive heart failure, valve-related dysfunction requiring repeat procedure, and valve-related dysfunction determined by echocardiography (mean aortic valve gradient ≥20 mm Hg and either effective orifice area ≤0.9–1.1 cm² [depending on body surface area] or Doppler velocity index <0.35; or moderate or severe prosthetic valve regurgitation as defined by VARC-2).
CHOICE was an investigator-initiated trial in high-risk patients with severe AS and an anatomy suitable for transfemoral TAVI. One hundred twenty-one patients were randomly assigned to receive a balloon-expandable SAPIEN XT device and 120 were assigned to receive a self-expandable CoreValve device. The primary endpoint was device success, a composite end point including successful vascular access and deployment of the device and retrieval of the delivery system, correct position of the device, intended performance of the heart valve without moderate or severe regurgitation, and only 1 valve implanted in the proper anatomical location. Device success was observed in 95.9% of patients in the balloon-expandable valve group and 77.5% of patients in the self-expandable valve group (relative risk 1.24, 95% CI 1.12-1.37, P <0.001), with differences attributed to a significantly lower frequency of residual more-than-mild aortic regurgitation (4.1% vs. 18.3%; relative risk 0.23; 95% CI 0.09-0.58; P <0.001) and the less frequent need for implanting more than 1 valve (0.8% vs. 5.8%, P = 0.03) in the balloon-expandable valve group60. Abdel-Wahab M, Mehilli J, Frerker C, et al. Comparison of balloon-expandable vs self-expandable valves in patients undergoing transcatheter aortic valve replacement: the CHOICE randomized clinical trial. JAMA. 2014;311:1503-1514 Link. Clinical outcomes between groups were similar throughout 5-year follow-up, including all-cause death (53.4% vs. 47.6%, P = 0.38), cardiovascular death (31.6% vs. 21.5%, P = 0.12), all strokes (17.5% vs. 16.5%, P = 0.73), and repeat hospitalization for heart failure (28.9% vs. 22.5%, P = 0.75), while new pacemaker implantation was more frequent in the self-expanding group61. Abdel-Wahab M, Landt M, Neumann FJ, et al. 5-Year Outcomes After TAVR With Balloon-Expandable Versus Self-Expanding Valves: Results From the CHOICE Randomized Clinical Trial. JACC Cardiovasc Interv. 2020;13:1071-1082 Link.
SOLVE-TAVI
The SOLVE-TAVI trial was an investigator-initiated RCT of 447 patients with symptomatic severe AS undergoing transfemoral TAVI comparing the self-expanding Evolut R with the balloon-expandable SAPIEN 3 transcatheter valve systems. The primary efficacy composite endpoint included all-cause death, stroke, moderate or severe PVR, and new permanent pacemaker implantation at 30 days. The study was powered for equivalence of the primary endpoint (equivalence margin 10% with significance level 0.05). At 30 days, the primary endpoint occurred in 28.4% of the Evolut R arm and 26.1% of the SAPIEN 3 arm, meeting the prespecified criteria of equivalence (Pequivalence = 0.04). There was a numerically higher stroke rate in the SAPIEN arm (4.7% vs. 0.5%), while the rate of moderate or severe PVR was numerically higher in the Evolut R arm (3.4% vs. 1.5%). The rate of new permanent pacemaker implantation was higher than expected in both arms (23.0% vs. 19.2%)62. Thiele H, Kurz T, Feistritzer HJ, et al. Comparison of newer generation self-expandable vs balloon-expandable valves in transcatheter aortic valve implantation: the randomized SOLVE-TAVI trial. Eur Heart J. 2020;41:1890-1899 Link. At 5 years, there was no significant difference in rates of the composite primary endpoint between the Evolut R and SAPIEN 3 arms (67.7% vs. 63.4%, P = 0.34), while stroke was more common in the SAPIEN 3 arm (2.2% vs. 9.6%, P = 0.002)63. Feistritzer HJ, Kurz T, Vonthein R, et al. Effect of Valve Type and Anesthesia Strategy for TAVR: 5-Year Results of the SOLVE-TAVI Trial. J Am Coll Cardiol. 2025;85:74-82 Link.
SCOPE I
SCOPE I was an investigator-initiated RCT designed to compare the early safety and efficacy of the self-expanding ACURATE neo device to the balloon-expandable SAPIEN 3 system. In this trial, 739 patients (aged ≥75 years) with symptomatic severe AS undergoing transfemoral TAVI deemed at increased surgical risk were enrolled. The primary composite safety and efficacy endpoint comprised all-caused death, any stroke, life-threatening or disabling bleeding, major vascular complications, coronary artery obstruction requiring intervention, acute kidney injury (stage 2 or 3), rehospitalization for valve-related symptoms or congestive heart failure, valve-related dysfunction requiring repeat procedure, moderate or severe PVR, or prosthetic valve stenosis within 30 days of the procedure. The study was powered for non-inferiority of the ACURATE neo compared with the SAPIEN 3 THV for the primary endpoint (non-inferiority margin 7.7% with significance level 0.05). The primary endpoint occurred in 87 (24%) patients in the ACURATE neo and in 60 (16%) patients in the SAPIEN 3 group; non-inferiority of the ACURATE neo was not met (Pnon-inferiority = 0.42). The result was largely driven by a higher rate of acute kidney injury (3% vs. 1%, P = 0.034) and moderate or severe PVR (9% vs. 3%) in the ACURATE neo arm. In terms of haemodynamic outcomes, the ACURATE neo THV was associated with larger effective orifice area (1.73 cm2 vs. 1.47 cm2, P<0.001) and lower transvalvular gradients (7 mmHg vs. 11 mmHg, P <0.001) compared with the SAPIEN 3 THV64. Lanz J, Kim WK, Walther T, et al. Safety and efficacy of a self-expanding versus a balloon-expandable bioprosthesis for transcatheter aortic valve replacement in patients with symptomatic severe aortic stenosis: a randomised non-inferiority trial. Lancet. 2019;394:1619-1628 Link. However, early differences between ACURATE neo and SAPIEN 3 did not translate into significant differences in clinical outcomes or bioprosthetic valve failure throughout 3 years of follow-up (all-cause death: 24.3% vs. 25.0%, HR 0.98, 95% CI 0.73-1.33; cardiovascular death: 16.8% vs. 16.8%, HR 1.01, 95% CI 0.70-1.45; stroke: 6.1% vs. 5.8%, HR 1.04, 95% CI 0.56-1.92; rehospitalization for valve-related symptoms or congestive heart failure: 13.9% vs. 18.1%, HR 0.74, 95% CI 0.51-1.07, new permanent pacemaker implantation: 15.6% vs. 16.4%, HR 0.92, 95% CI 0.62-1.37, respectively). Of note, the incidence of moderate or severe haemodynamic valve deterioration (HVD) according to the VARC-3 criteria (0.4% vs. 2.9%, subhazard ratios [sHR] 0.19, 95% CI 0.02-1.76) and valve thrombosis (0.3% vs. 1.8%, sHR 0.16, 95% CI 0.02-1.35) was numerically lower in the ACURATE neo group compared with that in the SAPIEN 3 group65. Lanz J, Mollmann H, Kim WK, et al. Final 3-Year Outcomes of a Randomized Trial Comparing a Self-Expanding to a Balloon-Expandable Transcatheter Aortic Valve. Circ Cardiovasc Interv. 2023;16:e012873 Link.
SCOPE II
SCOPE II was another investigator-initiated RCT comparing the ACURATE neo to the Evolut R/PRO self-expanding valve system enrolling 796 patients (aged ≥75 years) with an indication for transfemoral TAVI66. Tamburino C, Bleiziffer S, Thiele H, et al. Comparison of Self-Expanding Bioprostheses for Transcatheter Aortic Valve Replacement in Patients With Symptomatic Severe Aortic Stenosis: SCOPE 2 Randomized Clinical Trial. Circulation. 2020;142:2431-2442 Link. The primary endpoint, powered for non-inferiority of the ACURATE neo THV, was the composite of all-cause death or stroke at 1 year (non-inferiority margin 6% with significance level 0.05). The key secondary endpoint, powered for superiority of the ACURATE neo THV, was new permanent pacemaker implantation at 30 days. At 1 year, the primary endpoint occurred in 59 (15.8%) in the ACURATE neo and in 52 (13.9%) in the Evolut R/PRO group, with an absolute risk difference of 1.8% and a one-sided 95% upper confidence limit of 6.1% that did not meet non-inferiority of the ACURATE neo compared with the Evolut R/PRO THV (Pnon-inferiority = 0.0549). No significant differences were observed in the components of the primary endpoint. However, cardiac death at 30 days (2.8% vs. 0.8%, P = 0.03) and 1 year (8.4% vs. 3.9%, P = 0.01), and moderate or severe PVR (10% vs. 3%, P = 0.002) were higher in the ACURATE neo group. Conversely, the rate of new permanent pacemaker implantation was lower in the ACURATE neo than the Evolut R/PRO group both at 30 days (11% vs. 18%, P = 0.003) and 1 year (11% vs. 18%, P = 0.004). At 1 year, also new-onset LBBB occurred less frequently in the ACURATE neo compared with the Evolut R/PRO group (14% vs. 19%, P = 0.048).
ACURATE IDE
Following the assessment of ACURTAE neo in SCOPE I and II, a new iteration - ACURATE neo 2 - with an annular sealing technology was developed which is used in clinical practice in Europe. The ACURATE IDE trial (NCT03735667) directly compared the ACURATE neo2 THV with the two established landmark devices (SAPIEN and Evolut). In this trial, 1,500 patients with tricuspid severe symptomatic AS were randomly assigned 1:1 to ACURATE neo 2 (N = 752) or the control group (SAPIEN [N = 504] or Evolut [N = 244]). The primary hypothesis was non-inferiority of ACURATE neo 2 to the control group for the primary endpoint of all-cause mortality, stroke, or hospitalization for valve-related symptoms or worsening congestive heart failure at 1 year. At 1 year, the primary endpoint occurred in 16.2% (95% BCI 13.4% to 19.1%) of patients receiving ACURATE neo 2 and in 9.5% (95% BCI 7.5% to 11.9%) of patients receiving SAPIEN/Evolut, with between-group difference of 6.6% (95% BCI, 3.0% to 10.2%) and posterior probability of treatment difference of >0.999, failing to establish non-inferiority of ACURATE neo 2 compared to the contemporary devices. Patients in the ACURATE neo 2 group had a higher rate of cardiovascular death, stroke, and spontaneous myocardial infarction than those in the control groups, while clinically evident valve thrombosis occurred less frequently with ACURATE neo 2 than with control valves (0.7% vs. 2.6%, HR 0.26, 95% CI 0.10-0.71) and this difference was more pronounced when compared with the SAPIEN device (clinically evident valve thrombosis: 3.3% in the SAPIEN group and 1.3% in the Evolut group, respectively)67. Makkar R, Ramanna R, Gnall E, et al. Open-cell self-expanding supra-annular ACURATE neo2 valve versus commercially available transcatheter heart valves in patients with severe aortic stenosis (ACURATE IDE): a randomised, controlled, non-inferiority trial. Lancet 2025. In Press. Link. A post-hoc analysis suggested that valve under-expansion may have had an impact on 1-year clinical outcomes. More than 1 in 5 patients assigned to ACURATE neo 2 had evidence of under-expanded valve frames, defined as non-parallel commissural posts on angiographic imaging, and under-expansion was associated with an increased risk of the primary endpoint (primary endpoint: 18.8% vs. 12.4%, P = 0.050; death: 7.4% vs. 3.7%, P = 0.054; stroke: 11.0% vs. 3.5%, P <0.001; rehospitalization: 2.7% vs. 5.9%, P = 0.131; respectively). Patients with well-expanded ACURATE neo2 valves had a similar rate of death and stroke at 1 year compared to controls in this post-hoc analysis (3.7% vs. 3.6% and 3.5% vs. 3.4%, respectively)68. Reardon M. One year Outcomes of ACURATE neo2 vs Approved TAVR Devices in All risk Patients with Severe AS: the ACURATE IDE Trial. TCT 2024 October 30, 2024. Washington, DC Link.
PORTICO IDE
PORTICO IDE was a non-inferiority RCT to evaluate the safety and efficacy of the Portico intra-annular self-expanding THV compared with any commercially available THV (SAPIEN: 1.4%, SAPIEN XT: 7.2%, SAPIEN 3: 57.1%, CoreValve: 3.9%, Evolut R: 24.7%, and Evolut PRO: 5.8%)69. Makkar RR, Cheng W, Waksman R, et al. Self-expanding intra-annular versus commercially available transcatheter heart valves in high and extreme risk patients with severe aortic stenosis (PORTICO IDE): a randomised, controlled, non-inferiority trial. Lancet. 2020;396:669-683. Link. The primary safety endpoint was a composite of all-cause death, disabling stroke, life-threatening bleeding requiring transfusion, acute kidney injury requiring dialysis, or major vascular complication at 30 days. The primary efficacy endpoint was all-cause death or disabling stroke at 1 year. The non-inferiority margin was 8.5% for primary safety and 8.0% for primary efficacy endpoints. The Portico THV met non-inferiority criteria for the primary safety endpoint, which occurred in 13.8% of the Portico and in 9.6% of the commercial valve group (Pnon-inferiority = 0.034). At 1 year, the Portico THV also met non-inferiority criteria for the primary efficacy endpoint (14.8% vs. 13.4%, Pnon-inferiority = 0.006). At 2 years, rates of all-cause death (22.3% vs. 20.2%, P = 0.40) or disabling stroke (3.1% vs. 5.0%, P = 0.32) were similar between groups. In terms of valve performance, the Portico THV was associated with similar mean transvalvular gradients (8.1 mmHg vs. 7.4 mmHg, P = 0.18) and effective orifice area (1.86 cm2 vs. 1.76 cm2, P = 0.16) as the Evolut R/PRO THV, and lower gradients and larger effective orifice area than the SAPIEN 3 THV (11.5 mmHg, P <0.001; and 1.62 cm2, P <0.001; respectively). Conversely, moderate or severe PVR occurred more frequently in the Portico group than in the SAPIEN 3 group (6.1% vs. 1.6%, P = 0.016), but no difference was observed when compared with the Evolut R/PRO group (4.0%, P = 0.42)69. Makkar RR, Cheng W, Waksman R, et al. Self-expanding intra-annular versus commercially available transcatheter heart valves in high and extreme risk patients with severe aortic stenosis (PORTICO IDE): a randomised, controlled, non-inferiority trial. Lancet. 2020;396:669-683. Link.
The ENVISION trial (NCT05932615) is currently underway to compare the Navitor THV, a successor to the Portico THV, to the established landmark devices in a head-to-head randomized comparison.
LANDMARK
The LANDMARK trial was a prospective, multinational, randomized, open-label, non-inferiority trial that compared the balloon-expandable Myval THV with the contemporary SAPIEN or Evolut series. The Myval THV is characterized by smaller sizing increments of 1.5 mm compared with the usual 3 mm increments in valve size. Out of 5,109 screened patients, 768 patients deemed eligible for all three devices were randomly assigned 1:1 to Myval (N = 384) or contemporary THV (N = 384) with subsequent stratification and equal allocation (1:1) of patients to the SAPIEN (N = 192 [SAPIEN 3: 55.4% and SAPIEN 3 Ultra: 44.6%]) or Evolut (N = 192 [Evolut R: 37.0%, Evolut PRO: 55.2%, Evolut PRO Plus: 5.2%, and Evolut FX: 2.6%]) devices using a covariate-adaptive randomization process. The primary early safety and effectiveness composite endpoint at 30-day follow-up included all-cause mortality, stroke, bleeding type 3 & 4, acute kidney injury stage 2-4, moderate or severe PVR, new permanent pacemaker implantation, or major vascular complications. The study was powered for non-inferiority of the primary endpoint (non-inferiority margin 10.44% at a significance level of 0.05). The trial established non-inferiority of the Myval THV (25%) compared with contemporary THV (27%) for the primary endpoint with a risk difference of -2.3% (one-sided upper 95% CI 3.8, Pnon-inferiority <0.0001)70. Baumbach A, van Royen N, Amat-Santos IJ, et al. LANDMARK comparison of early outcomes of newer-generation Myval transcatheter heart valve series with contemporary valves (Sapien and Evolut) in real-world individuals with severe symptomatic native aortic stenosis: a randomised non-inferiority trial. Lancet. 2024;403:2695-2708 Link. There were no significant differences for the individual components of the primary composite endpoint. For the individual head-to-head comparisons, this trial performed a prespecified analysis assuming an event rate of 26.1% for the primary endpoint and a non-inferiority margin of 10.4% the sample size provided 80% power at a one-sided alpha of 0.05 to establish non-inferiority. At 30 days, Myval was found to be non-inferior for the composite primary endpoint as compared to each comparator device (24.7% vs. 24.1% for SAPIEN; risk difference: 0.6%, one-sided upper 95% CI: 8.0%, Pnon-inferiority: 0.0033; and 24.7% vs. 30.0% for Evolut; risk difference: -5.3%, one-sided upper 95% CI: 2.5%, Pnon-inferiority: <0.0001). In terms of echocardiographic outcomes as assessed at an independent Core Laboratory, Myval was associated with lower mean transprosthetic gradients and larger effective orifice area and a similar rate of moderate or greater prosthetic valve regurgitation compared to SAPIEN. As compared with Evolut, Myval was associated with higher mean transprosthetic gradients and smaller effective orifice area and a lower rate of moderate or greater prosthetic valve regurgitation. However, a similar rate of moderate or greater prosthetic valve regurgitation was observed for Myval and Evolut THV after excluding Evolut R prostheses71. Royen NV, Amat-Santos IJ, Hudec M, et al. Early outcomes of the novel Myval THV series compared to SAPIEN THV series and Evolut THV series in individuals with severe aortic stenosis. EuroIntervention. 2025;21:e105-e118 Link.
COMPARE-TAVI 1
The COMPARE-TAVI 1 trial was an investigator-initiated, all-comers, non-inferiority trial comparing two balloon-expandable THV Out of 1,335 patients undergoing transfemoral TAVI at three high-volume centers in Western Denmark (defined as more than 75 TAVI procedures per year), 1,031 patients were randomized 1:1 to treatment with SAPIEN 3 (29 mm) / SAPIEN 3 Ultra (20, 23, or 26 mm) THV or Myval/Myval Octacor THV (median age: 81 years; female: 40.3%; median STS-PROM: 2.3%; bicuspid anatomy: 9.5%; and valve-in-valve procedure: 4.0%). The primary endpoint was a composite of all-cause death, stroke, moderate or severe aortic regurgitation, or moderate or severe HVD at 1 year according to the VARC-3 criteria. The non-inferiority margin was adjusted based on the actual event rate, and a non-inferiority margin of 5.3% with an upper limit of one-sided 95% CI of 4.4% was selected. At 1 year, the primary composite endpoint occurred in 13.0% of patients treated with SAPIEN THV and 13.8% of patients treated with Myval THV, demonstrating non-inferiority of Myval THV to SAPIEN THV (risk difference -0.9%, one-sided upper 95% CI -4.4%, Pnon-inferiority = 0.02). For the components of the primary endpoint, there was no significant difference in the rates of mortality, stroke, and moderate or severe HVD, while moderate or severe aortic regurgitation occurred more frequently in the Myval group compared with the SAPIEN group (3.9% vs. 1.2%, P = 0.005). In addition, the Myval group had a higher incidence of new permanent pacemaker implantation (20.9% vs. 12.0%, P <0.001), newly diagnosed atrial fibrillation (13.5% vs. 8.1%, P = 0.003) and VARC-3 type 2 bleeding (14.8% vs. 7.9%, P <0.001) compared with the SAPIEN group. However, Myval THV had a larger effective orifice area and smaller transprosthetic gradient across all THV sizes and across the total range of annulus areas. Of note, there was a wide range in the rate of predilatation (Myval: 20.2%, Myval Octacor: 59.0%, and SAPIEN: 20.7%, respectively), which may influence valve haemodynamics and the occurrence of conduction disturbances. A prespecified CT substudy is currently underway to evaluate the relationship between actual valve deployment and valve performance or the occurrence of conduction disturbances72. Terkelsen CJ, Freeman P, JS Dahl, et al. SAPIEN 3 versus Myval transcatheter heart valves for transcatheter aortic valve implantation (COMPARE-TAVI 1): a multicentre, randomised, non-inferiority trial. Lancet. 2025;405:1362-1372. Link.
Patient selection for TAVI
Following a series of RCTs demonstrating similar clinical outcomes with the less invasive TAVI intervention compared with SAVR, current ACC/AHA and ESC/EACTS guidelines for the management of valvular heart disease recommend TAVI as an alternative to SAVR across the spectrum of surgical risk among elderly patients who are candidates for bioprostheses (Figure 7), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. Although most of the evidence supporting TAVI compared with SAVR has been generated in carefully selected patient populations with predominantly two valve types, the favourable outcomes of TAVI have been corroborated in investigator-initiated trials with broader inclusion criteria (NOTION, NOTION-2, DEDICATE, UK-TAVI) more closely resembling clinical practice. Notwithstanding, each treatment strategy has its own strengths and limitations, which should be considered by interdisciplinary Heart Teams to provide the best possible care for each individual patient. The following sections highlight key considerations that should be taken into account to inform the individual decision between TAVI and SAVR (Table 9).
Table 9. A framework of factors favouring SAVR, TAVI, or conservative therapy (2020 ACC/AHA guideline).
Favours SAVR
Favours TAVI
Favors Conservative Therapy
Age/life expectancy
-Younger age/longer life expectancy
-Older age/fewer expected remaining years of life
-Limited life expectancy
Valve morphology
-Bicuspid aortic valve
-Left ventricular outflow tract calcification
-Rheumatic valve disease
-Small or large aortic annulus
-Calcific AS of a tri-leaflet valve
Prosthetic valve preference
-Mechanical or surgical bioprosthetic valve preferred
-Concern for prosthesis–patient mismatch (annular enlargement might be considered)
-Bioprosthetic valve preferred
-Favourable ratio of life expectancy to valve durability
-TAVI provides larger valve area than same size SAVR
-Previous cardiac surgery with at-risk coronary grafts
-Previous chest irradiation
-Valve anatomy, annular size, or coronary ostial height precludes TAVI
-Vascular access does not allow transfemoral TAVI
Goals of Care and patient preferences and values
-Less uncertainty about valve durability
-Avoid repeat intervention
-Lower risk of permanent pacer
-Life prolongation
-Symptom relief
-Improved long-term exercise capacity and QOL
-Avoid vascular complications
-Accepts longer hospital stay, pain in recovery period
-Accepts uncertainty about valve durability and possible repeat intervention
-Higher risk of permanent pacer
-Life prolongation
-Symptom relief
-Improved exercise capacity and QOL
-Prefers shorter hospital stay, less postprocedural pain
-Life prolongation not an important goal
-Avoid futile or unnecessary diagnostic or therapeutic procedures
-Avoid procedural stroke risk
-Avoid possibility of cardiac pacer
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; AVR = aortic valve replacement; QOL = quality of life; SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
Age
Current guidelines for the management of valvular heart disease recommend TAVI in patients with severe AS aged ≥65 years (ACC/AHA guidelines) or ≥75 years (ESC/EACTS guidelines), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. Although most patients undergoing TAVI or SAVR are >75 years of age, a non-negligible proportion of patients require intervention before 70 years of age73. Hamm CW, Mollmann H, Holzhey D, et al. The German Aortic Valve Registry (GARY): in-hospital outcome. Eur Heart J. 2014;35:1588-1598 Link. As TAVI is expanding to younger patients with longer life-expectancy, it is important to anticipate lifetime management issues beyond the first 10 years after the index procedure, namely the need for reintervention. The available evidence comparing TAVI with SAVR is limited to 5-10 years with the majority of participants aged >70 years, even in the low-risk trials (PARTNER 3: mean age of 73 years, Evolut Low Risk: mean age of 74 years), , , , , , , , 11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link12. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790-1798 Link13. Thyregod HG, Steinbrüchel DA, Ihlemann N, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65:2184-2194 Link14. Leon MB, Smith CR, Mack MJ, et al. Transcatheter or Surgical Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2016;374:1609-1620. Link15. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376:1321-1331 Link16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link17. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380:1706-1715 Link19. UK TAVI Trial Investigators; Toff WD, Hildick-Smith D, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA. 2022;327:1875-1887. Link21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link. The NOTION-2 trial compared TAVI with SAVR exclusively in patients aged ≤75 years (mean age of 71.1 years and a median STS-PROM of 1.1%) and reported a similar incidence of the primary composite endpoint of all-cause mortality, stroke, or rehospitalization between the treatment strategies. However, the follow-up period is limited to 1-year so far22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link. Although previous surgical studies reported that clinically relevant deterioration of surgical bioprostheses typically occurs after >10 years, data on durability of THV is currently limited up to 10 years54. Thyregod HGH, Jorgensen TH, Ihlemann N, et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. Eur Heart J. 2024;45:1116-1124 Link, as will be discussed in a later section.
Sex
Previous surgical studies have suggested that women compared to men have impaired clinical outcomes due to later disease presentation and more advanced comorbid status at the time of intervention, 38. Hahn RT, Clavel MA, Mascherbauer J, et al. Sex-Related Factors in Valvular Heart Disease: JACC Focus Seminar 5/7. J Am Coll Cardiol. 2022;79:1506-1518 Link74. Chaker Z, Badhwar V, Alqahtani F, et al. Sex Differences in the Utilization and Outcomes of Surgical Aortic Valve Replacement for Severe Aortic Stenosis. J Am Heart Assoc. 2017;6:e006370 Link. Early data from the STS/ACC TVT registry (11,808 women and 11,844 men between 2011 and 2014) reported more procedural complications including major vascular complications, VARC-2 major bleeding, and more frequent surgical conversion in female than male patients, while female patients had a lower 1-year all-cause death compared with male patients (adjusted HR 0.73, 95% CI 0.63-0.85). Of note, more than 30% of patients in this study underwent non-transfemoral TAVI and all TAVI devices adopted a large bore sheath (>20 Fr)75. Chandrasekhar J, Dangas G, Yu J, et al. Sex-Based Differences in Outcomes With Transcatheter Aortic Valve Therapy: TVT Registry From 2011 to 2014. J Am Coll Cardiol. 2016;68:2733-2744 Link. Due to technical and device improvements, increased operator experience, and improved patient selection, sex-specific differences in clinical outcomes have been less pronounced. In the SOURCE 3 registry of 1,649 patients undergoing transfemoral TAVI with the balloon-expandable SAPIEN3 device (49.2% women, age 81.7 ± 6.7 years), no sex-related difference was observed in terms of procedural outcomes and mortality throughout 4-year follow-up76. Tarantini G, Baumgartner H, Frank D, et al. Four-year mortality in women and men after transfemoral transcatheter aortic valve implantation using the SAPIEN 3. Catheter Cardiovasc Interv. 2021;97:876-884 Link.
Several studies have suggested that TAVI may be more effective than SAVR in female patients with severe AS. However, data were limited to subgroup analyses from registry or RCTs, , 16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link77. Siontis GC, Praz F, Pilgrim T, et al. Transcatheter aortic valve implantation vs surgical aortic valve replacement for treatment of severe aortic stenosis: a meta-analysis of randomized trials. Eur Heart J. 2016;37:3503-3512 Link. The RHEIA trial was the first trial directly comparing SAVR with TAVI in female patients with symptomatic severe AS. In this study, 443 female patients with symptomatic severe AS (mean age 73 years and mean STS-PROM 2%) were randomly assigned to SAVR or TAVI with the SAPIEN 3 or SAPIEN 3 Ultra THV. At 1 year, the primary composite endpoint of all-cause mortality, stroke, and rehospitalization for valve- or procedure-related symptoms or worsening heart failure was higher in the SAVR compared with the TAVI group (15.6% vs. 8.9%, difference -6.8%, upper 95% confidence limit -1.5%, Pnon-inferiority <0.001, two-sided 95% CI -13.0% to -0.5%, Psuperiority = 0.034), predominantly driven by a higher rehospitalization rate in the SAVR group (11.4% vs. 4.8%) without differences in terms of mortality (2.0% vs. 0.9%) and stroke (3.0% vs. 3.3%). Although the majority of the study participates represented with small aortic annulus dimensions defined as aortic annulus area <430 mm2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link, favourable bioprosthetic haemodynamics were achieved with both treatment approaches in this population78. Tchetche D, Pibarot P, Bax J, et al. Transcatheter vs. surgical aortic valve replacement in women: the RHEIA trial. Eur Heart J. 2025. Online ahead of print. doi: 10.1093/eurheartj/ehaf133. Link.
Patient morbidities and frailty
A considerable proportion of patients with clinically relevant AS have relevant comorbidities when referred for AVR. These factors must be taken into careful consideration during the decision-making process on treatment selection. Current ACC/AHA guidelines indicate high or prohibitive surgical risk when patients have one or more major organ systems compromised and not to be improved postoperatively (Table 10).
Low surgical risk (must meet all criteria in this column)
High surgical risk (any 1 criterion in this column)
Prohibitive surgical risk (any 1 criterion in this column)
STS-PROM
< 3%
> 8%
Predicted risk of death or major morbidity (all-cause) > 50% at 1 y
Frailty+
None
≥ 2 indices (moderate to severe)
≥ 2 indices (moderate to severe)
Major organ system compromise not to be improved postoperatively++
None
1 to 2 organ systems
≥ 3 organ systems
Procedure-specific impediment+++
None
Possible procedure-specific impediment
Severe procedure-specific impediment
+ Seven frailty indices: Katz Activities of Daily Living (independence in feeding, bathing, dressing, transferring, toileting, and urinary continence) plus independence in ambulation (no walking aid or assistance required, or completion of a 5-m walk in < 6 s). Other scoring systems can be applied to calculate no, mild, or moderate to severe frailty. ++ Examples of major organ system compromise include cardiac dysfunction (severe left ventricular systolic or diastolic dysfunction or right ventricular dysfunction, fixed pulmonary hypertension); kidney dysfunction (chronic kidney disease, stage 3 or worse); pulmonary dysfunction (FEV1 < 50% or DLCO2 < 50% of predicted); central nervous system dysfunction (dementia, Alzheimer’s disease, Parkinson’s disease, cerebrovascular accident with persistent physical limitation); gastrointestinal dysfunction (Crohn’s disease, ulcerative colitis, nutritional impairment, or serum albumin < 3.0); cancer (active malignancy); and liver dysfunction (any history of cirrhosis, variceal bleeding, or elevated international normalized ratio in the absence of vitamin K antagonist therapy). +++ Examples of procedure-specific impediments include presence of tracheostomy, heavily calcified (porcelain) ascending aorta, chest malformation, arterial coronary graft adherent to posterior chest wall, and radiation damage. ACC/AHA = American College of Cardiology/American Heart Association; DLCO2 = diffusion capacity for carbon dioxide; FEV1 = forced expiratory volume in 1 second; STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality.
Although RCTs excluded highly morbid patients, TAVI is more attractive than SAVR in this population as long as life expectancy exceeds 1 year due to the less invasive nature of the intervention and faster recovery, 79. Ando T, Adegbala O, Akintoye E, et al. Is Transcatheter Aortic Valve Replacement Better Than Surgical Aortic Valve Replacement in Patients With Chronic Obstructive Pulmonary Disease? A Nationwide Inpatient Sample Analysis. J Am Heart Assoc. 2018;7:e008408 Link80. Alqahtani F, Aljohani S, Ghabra A, et al. Outcomes of Transcatheter Versus Surgical Aortic Valve Implantation for Aortic Stenosis in Patients With Hepatic Cirrhosis. Am J Cardiol. 2017;120:1193-1197 Link. However, patients with severe morbidities, such as end-stage renal disease, end-stage liver disease, chronic obstructive pulmonary disease, and advanced cancer, have worse prognosis compared with those without, even after successful TAVI and discussion regarding futility may be considered, , , 81. Mok M, Nombela-Franco L, Dumont E, et al. Chronic obstructive pulmonary disease in patients undergoing transcatheter aortic valve implantation: insights on clinical outcomes, prognostic markers, and functional status changes. JACC Cardiovasc Interv. 2013;6:1072-1084 Link82. Ullah W, DiMeglio M, Sana MK, et al. Outcomes After Transcatheter Aortic Valve Implantation in Patients Excluded From Clinical Trials. JACC Adv. 2023;2:100271 Link83. Demirel C, Tomii D, Heg D, et al. Incidental detection of malignancy during preprocedural workup for transcatheter aortic valve implantation: A longitudinal cohort study. Am Heart J. 2023;261:51-54 Link84. Liao YB, He ZX, Zhao ZG, et al. The relationship between chronic obstructive pulmonary disease and transcatheter aortic valve implantation--A systematic review and meta-analysis. Catheter Cardiovasc Interv. 2016;87 Suppl 1:570-578 Link.
Frailty is a multidimensional geriatric syndrome defined as slowness, weakness, exhaustion, wasting and malnutrition, poor endurance and inactivity, and loss of independence85. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol A Biol Sci Med Sci. 2001;56:M146-56. Link. The prevalence of frailty in patients undergoing AVR varies widely between studies due to differences in patient populations and varying definitions (Table 11).
Table 11. Frailty Assessment.
Parameters
Tests
Scales
Fried
Fried+
SPPB
Rockwood
Bern
Columbia
EFT
Slow gait speed
Time to walk 5 meters at a comfortable pace (3 trials)
Time to stand 5 times from a chair without using arms
✓
✓
Poor balance
Time able to stand with feet in tandem or side-by-side positions (up to 10 sec)
✓
Weight loss
Self-reported unintentional weight loss ≥10 lbs over the past year
✓
✓
Exhaustion
Self-reported “could not get going” or “everything was an effort” most days of the week
✓
✓
✓
Inactivity
Paffenbarger questionnaire (expanded version) <2000 kilocalories of weekly activity
✓
✓
✓
Anaemia
Haemoglobin <13.0 g/dL in men and <12.0 g/dL in women
✓
Hypoalbuminemia
Serum albumin <3.5 g/dL in men and women
✓
✓
Malnutrition
Mini-Nutritional Assessment
✓
Cognitive impairment
Mini-Mental State Examination
✓
✓
✓
Depressed mood
Short-Form Geriatric Depression Scale
✓
ADL disability
Inability to independently perform basic activities such as eating and dressing
✓
✓
✓
IADL disability
Inability to independently perform instrumental activities such as cooking and shopping
✓
✓
ADL = Activities of Daily Living; EFT = Essential Frailty Toolset; IADL = Instrumental Activities of Daily Living; SPPB = Short Physical Performance Battery.
The prospective FRAILTY-AVR study assessed frailty in patients with severe AS undergoing TAVR or SAVR using 7 different frailty scales and observed that prevalence ranged from 35-74% in the TAVR group and 12-56% in the SAVR group, depending on the definition used. The Essential Frailty Toolset, integrating lower-extremity weakness, cognitive impairment, anaemia, and hypoalbuminemia, outperformed the other scales and was recommended for use in this setting86. Afilalo J, Lauck S, Kim DH, et al. Frailty in Older Adults Undergoing Aortic Valve Replacement: The FRAILTY-AVR Study. J Am Coll Cardiol. 2017;70:689-700 Link. Despite varying prevalence, frailty has been consistently associated with worse health status and overall prognosis compared to non-frail patients after AVR, , , , 87. Green P, Arnold SV, Cohen DJ, et al. Relation of frailty to outcomes after transcatheter aortic valve replacement (from the PARTNER trial). Am J Cardiol. 2015;116:264-269 Link88. Okoh AK, Chauhan D, Kang N, et al. The impact of frailty status on clinical and functional outcomes after transcatheter aortic valve replacement in nonagenarians with severe aortic stenosis. Catheter Cardiovasc Interv. 2017;90:1000-1006 Link89. Bendayan M, Messas N, Perrault LP, et al. Frailty and Bleeding in Older Adults Undergoing TAVR or SAVR: Insights From the FRAILTY-AVR Study. JACC Cardiovasc Interv. 2020;13:1058-1068 Link90. Arnold SV, Zhao Y, Leon MB, et al. Impact of Frailty and Prefrailty on Outcomes of Transcatheter or Surgical Aortic Valve Replacement. Circ Cardiovasc Interv. 2022;15:e011375 Link91. Sundermann SH, Back C, Bischoff-Ferrari HA, et al. Preinterventional frailty assessment in patients scheduled for cardiac surgery or transcatheter aortic valve implantation: a consensus statement of the European Association for Cardio-Thoracic Surgery (EACTS) and the European Association of Preventive Cardiology (EAPC) of the European Society of Cardiology (ESC). Eur J Cardiothorac Surg. 2023;64:ezad181. Link. A significant proportion of frail patients can achieve a similar extent of improvement in patient-reported outcome as non-frail patients, which may justify invasive treatment strategies in patients with reduced health status and frailty at baseline, even in the absence of an effect on mortality. In a post-hoc analysis of the SCOPE I trial, patients with frailty demonstrated similar improvement in KCCQ overall score after TAVI, while frailty was associated with an increased risk of VARC-3 unfavourable outcomes throughout 3 years of follow-up (48.0% vs. 34.7%, risk ratio 1.38, 95% CI 1.09-1.75), suggesting that TAVI may be futile in some frail patients92. Tomii D, Lanz J, Heg D, et al. The Impact of Frailty on VARC-3 Integrated Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Adv. 2025;4:101594 Link. Current guidelines allocate frailty as key consideration in the decision-making process between SAVR and TAVI (Table 10). However, recent analyses from the PARTNER trials and pooled outcomes of the CoreValve High Risk and SURTAVI trials suggest that frailty is not associated with a differential impact with respect to treatment modality on mortality and disease-specific health status, 90. Arnold SV, Zhao Y, Leon MB, et al. Impact of Frailty and Prefrailty on Outcomes of Transcatheter or Surgical Aortic Valve Replacement. Circ Cardiovasc Interv. 2022;15:e011375 Link93. Strom JB, Xu J, Orkaby AR, et al. Role of Frailty in Identifying Benefit From Transcatheter Versus Surgical Aortic Valve Replacement. Circ Cardiovasc Qual Outcomes. 2021;14:e008566 Link. Furthermore, frailty status may improve with initial relief of mechanical obstruction and improved patient care during subsequent follow-up. The PERFORM-TAVR trial randomized elder frail patients undergoing TAVI to protein oral supplementation and exercise therapy (85 patients) or usual care (95 patients)94. Fountotos R, Lauck S, Piazza N, et al. Protein and Exercise to Reverse Frailty in Older Men and Women Undergoing Transcatheter Aortic Valve Replacement: Design of the PERFORM-TAVR Trial. Can J Cardiol. 2024;40:267-274 Link. At 3 months after TAVR, patients in the intervention group demonstrated better physical performance compared to the control group by an improvement of 1.02 points in the SPPB score95. Afilalo J. Protein and exercise to reverse frailty in older men and women undergoing transcatheter aortic valve replacement: The PERFORM-TAVR Trial. ACC 2024. April 8, 2024 Atlanta, GA Link. Of note, a nationwide Danish study reported an important and ongoing increase in frailty and comorbidity burden from the time of TAVI to the end of life in TAVI recipients96. Strange JE, Holt A, Christensen DM, et al. End of Life After Transcatheter Aortic Valve Replacement: A Danish Nationwide Cohort Study. JACC Cardiovasc Interv. 2024;17:2936-2946 Link. These results underline the importance of a comprehensive approach to all phases of care for elder frail patients undergoing TAVI.
Surgical risk
Surgical risk is usually assessed using STS-PROM and EuroSCORE II, 97. O'Brien SM, Shahian DM, Filardo G, et al. The Society of Thoracic Surgeons 2008 cardiac surgery risk models: part 2--isolated valve surgery. Ann Thorac Surg. 2009;88:S23-42 Link98. Nashef SA, Roques F, Sharples LD, et al. EuroSCORE II. Eur J Cardiothorac Surg. 2012;41:734-744; discussion 744-735 Link. According to these scores, patients have been stratified into three risk categories: high (>8%), intermediate (4%-8%), and low (<4%) surgical risk. Of note, the risk scores have been developed in cohorts of patients undergoing cardiac surgery, and their predictive performances in TAVI population have been limited99. Wang TKM, Wang MTM, Gamble GD, Webster M, Ruygrok PN. Performance of contemporary surgical risk scores for transcatheter aortic valve implantation: A meta-analysis. Int J Cardiol. 2017;236:350-355 Link. Several TAVI-specific risk prediction models have been investigated, , , , , 100. Iung B, Laouenan C, Himbert D, et al. Predictive factors of early mortality after transcatheter aortic valve implantation: individual risk assessment using a simple score. Heart. 2014;100:1016-1023 Link101. Capodanno D, Barbanti M, Tamburino C, et al. A simple risk tool (the OBSERVANT score) for prediction of 30-day mortality after transcatheter aortic valve replacement. Am J Cardiol. 2014;113:1851-1858 Link102. Schiller W, Barnewold L, Kazmaier T, et al. The German Aortic Valve Score II. Eur J Cardiothorac Surg. 2017;52:881-887 Link103. Edwards FH, Cohen DJ, O'Brien SM, et al. Development and Validation of a Risk Prediction Model for In-Hospital Mortality After Transcatheter Aortic Valve Replacement. Jama. Cardiol 2016;1:46-52 Link104. Pilgrim T, Franzone A, Stortecky S, et al. Predicting Mortality After Transcatheter Aortic Valve Replacement: External Validation of the Transcatheter Valve Therapy Registry Model. Circ Cardiovasc Interv. 2017;10:e005481 Link105. Wolff G, Shamekhi J, Al-Kassou B, et al. Risk modeling in transcatheter aortic valve replacement remains unsolved: an external validation study in 2946 German patients. Clin Res Cardiol. 2021;110:368-376 Link. However, their predictive performance was not superior to conventional surgical risk scores (Table 12), maintaining STS-PROM and EuroSCORE II as preferred risk prediction models in current guidelines, 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link.
Table 12. Risk Scores.
Criterion
ES I
ES II
STS
FRANCE-2
OBSERVANT
STS/ACC TVT
German AV Score II
Publication year
1999/2003
2012
2009
2014
2014
2016
2017
Cohort size (Development/Validation)
13,302/1,479
16,828/5,553
65,855/43,904
2,552/1,281
1,256/622
13,718/6,868
9,027/9,027
Procedure
Cardiac surgery
Cardiac surgery
Cardiac valve surgery
TAVI
TAVI
TAVI
55% SAVR
45% TAVI
Discrimination performance (C statics in validation cohort)
0.76
0.81
0.80
0.59
0.71
0.66
0.74
Risk factor
Age
✓
✓
✓
✓
✓
✓
Sex
✓
✓
✓
✓
✓
Body physique
✓
✓
✓
Race
✓
✓
Left ventricular function
✓
✓
✓
✓
✓
Cardiac symptoms
✓
✓
✓
✓
Myocardial infarction
✓
✓
✓
NYHA class
✓
✓
✓
✓
✓
✓
Rhythm
✓
✓
Hypertension
✓
Endocarditis
✓
✓
✓
✓
Coronary artery disease
✓
✓
Previous cardiac surgery
✓
✓
✓
✓
Tricuspid valve disease
✓
Mitral valve disease
✓
Chronic lung disease
✓
✓
✓
✓
✓
✓
Pulmonary hypertension
✓
✓
✓
✓
✓
Cerebrovascular disease
✓
✓
Peripheral artery disease
✓
✓
✓
✓
Renal function
✓
✓
✓
✓
✓
✓
✓
Diabetes
✓
✓
✓
✓
Mobility
✓
Immunocompromise
✓
Status
✓
✓
✓
✓
✓
✓
✓
Previous balloon aortic valvuloplasty
✓
Approach
✓
✓
Pulmonary oedemas during the last year
✓
ES I = EuroSCORE I; ES II = EuroSCORE II; German AV Score II = German Aortic Valve Score II; STS = Society of Thoracic Surgeons score; STS/ACC TVT = Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry TAVI in-hospital mortality risk score.
More recently, artificial intelligence-based predictive models for TAVI outcomes have been developed. The TAVI Risk Machine (TRIM) scores is a machine learning-based model for predicting 30-day survival after TAVI. The algorithm was trained and cross-validated on data from 22,283 patients within the nationwide GARY registry and validated on data from 6,693 patients within the nationwide SwissTAVI registry. The model outperformed STS-PROM (TRIM: C-statistic 0.79, 95% CI 0.74-0.83; STS-PROM: C-statistic 0.69, 95% CI 0.65-0.74 in the deviation set and TRIM: C-statistic 0.75, 95% CI 0.72-0.79; STS-PROM: C-statistic 0.67, 95% CI 0.63-0.70 in the validation set)106. Leha A, Huber C, Friede T, et al. Development and validation of explainable machine learning models for risk of mortality in transcatheter aortic valve implantation: TAVI risk machine scores. Eur Heart J. Digit Health 2023;4:225-235 Link.
Coronary artery disease
AS and coronary artery disease (CAD) often coexist and share pathophysiological mechanisms. Therefore, screening for significant CAD prior to AVR is important to determine the need for coronary revascularization. Current ACC/AHA and ESC/EACTS guidelines recommend invasive coronary angiography to screen for CAD and limit coronary computed tomography angiography (CTA) to exclude obstructive CAD in patients with a low pretest probability of CAD. However, CTA is increasingly used to simultaneously assess the valvular apparatus and exclude significant stenoses of the proximal coronary artery segments, circumventing the need for invasive coronary angiography, , 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link107. Tomii D, Pilgrim T, Borger MA, et al. Aortic Stenosis and Coronary Artery Disease: Decision-Making Between Surgical and Transcatheter Management. Circulation. 2024;150:2046-2069 Link.
While SAVR and concomitant coronary artery bypass grafting has been the traditional and established standard of care for patients with AS and significant CAD, a complete percutaneous strategy (i.e. TAVI and percutaneous coronary intervention [PCI]) has been suggested as a reasonable treatment alternative in this population. However, the prognostic impact of concomitant CAD and the role of PCI remain unresolved in TAVI population, largely related to varying definitions of CAD107. Tomii D, Pilgrim T, Borger MA, et al. Aortic Stenosis and Coronary Artery Disease: Decision-Making Between Surgical and Transcatheter Management. Circulation. 2024;150:2046-2069 Link. In the NOTION-3 trial, 455 patients (median age of 82 years; median STS-PROM 3.0) with at least one high-grade coronary artery stenosis defined as fractional flow reserve ≤0.80 or diameter stenosis ≥90% in a coronary artery ≥2.5 mm diameter were randomly assigned to PCI with complete revascularization or to conservative treatment. The majority of PCI procedures were performed prior to TAVI and complete revascularization was achieved in 89% of patients in the PCI group. At a median follow-up of 2 years, the primary composite endpoint of death from any cause, myocardial infarction, or urgent revascularization was lower in the PCI group than in the conservative treatment group (26% vs. 36%, P = 0.04), driven by lower rates of spontaneous myocardial infarction or urgent revascularization. Of note, the benefit of PCI on adverse cardiac events was more pronounced among patients with ≥90% diameter stenosis as compared to fractional flow reserve <0.80108. Lonborg J, Jabbari R, Sabbah M, et al. PCI in Patients Undergoing Transcatheter Aortic-Valve Implantation. N Engl J Med. 2024;391:2189-2200 Link.
TAVI has the advantage of deferring treatment of concomitant CAD, allowing treatment to be prioritized according to disease severity, complexity and clinical presentation. PCI before TAVI has been proposed to reduce ischemic adverse events and to facilitate coronary access. However routine PCI prior to TAVI may be associated with an increased risk of periprocedural adverse events109. Patterson T, Clayton T, Dodd M, et al. ACTIVATION (PercutAneous Coronary inTervention prIor to transcatheter aortic VAlve implantaTION): A Randomized Clinical Trial. JACC Cardiovasc Interv. 2021;14:1965-1974 Link. Staged PCI after TAVI may provide advantages in terms of procedural safety and adequate physiological assessment of coronary lesion severity, , 110. Lunardi M, Venturi G, Del Sole PA, et al. Optimal timing for percutaneous coronary intervention in patients undergoing transcatheter aortic valve implantation. Int J Cardiol. 2022;365:114-122 Link111. Ochiai T, Yoon SH, Flint N, et al. Timing and Outcomes of Percutaneous Coronary Intervention in Patients Who Underwent Transcatheter Aortic Valve Implantation. Am J Cardiol. 2020;125:1361-1368 Link112. Rheude T, Costa G, Ribichini FL, et al. Comparison of different percutaneous revascularisation timing strategies in patients undergoing transcatheter aortic valve implantation. EuroIntervention. 2023;19:589-599 Link. A TAVI-first approach followed by deferred PCI as necessary may emerge as strategy in TAVI patients without high-grade CAD (i.e., 70-90% stenosis) (Figure 9)107. Tomii D, Pilgrim T, Borger MA, et al. Aortic Stenosis and Coronary Artery Disease: Decision-Making Between Surgical and Transcatheter Management. Circulation. 2024;150:2046-2069 Link. Ongoing trials will provide further perspectives into the optimal management strategy in patients with severe AS and CAD referred to TAVI (Table 13).
Figure 9
Treatment algorithm in patients with significant coronary artery disease undergoing aortic valve replacement. Figures reproduced from Tomii et al. Circulation 2024;150(25):2046-2069.
Table 13. Ongoing randomized clinical trials in patients with aortic stenosis and coronary artery disease undergoing TAVI.
Clinical Trial (Unique Identifier)
N
Intervention
CAD definition
Primary outcome
Follow-up period
Estimated Completion
Complete revascularization
COMPLETE-TAVR (NCT04634240)
4000
FFR-guided PCI with complete revascularization vs. Optimal medical therapy
At least one coronary artery lesion with ≥70% visual angiographic diameter stenosis in a native segment ≥2.5 mm in diameter
Composite of cardiovascular death or new myocardial infarction or ischemia-driven revascularization or hospitalization for unstable angina or heart failure
Median follow-up of 3.5 years
2026
Mode of PCI
FAITAVI (NCT03360591)
320
Physiologically-guided PCI vs. Angiographically-guided PCI
Coronary stenosis ≥50% by visual assessment in vessels ≥2.5 mm
Composite of all-cause death, myocardial infarction, stroke, major bleeding, need for target vessel revascularization
1 year
2024
Lesions with FFR ≤0.80
Timing of PCI
TAVI-PCI (NCT04310046)
986
PCI before TAVI vs. PCI after TAVI
Any suitable lesion with ≥70% diameter stenosis on coronary angiography in a coronary artery ≥2.5 mm in diameter
Composite of all-cause death, non-fatal myocardial infarction, ischemia-driven revascularization, rehospitalization for valve- or procedure-related including heart failure, life-threatening/disabling or major bleeding according to VARC-2 criteria
1 year
2026
Need routine PCI / routine coronary artery assessment
PRO-TAVI (NCT05078619)
466
TAVI without routine PCI vs. TAVI with routine PCI
At least 1 stenosis (70-99% diameter stenosis in angiography or 40-70% diameter stenosis in angiography with positive haemodynamic parameters) in epicardial coronary artery (>2.5 mm) or bypass graft
Composite of all-cause mortality, myocardial infarction, stroke and type 2-4 bleeding, in accordance to VARC-3 criteria
1 year
2025
CAT (NCT06559332)
546
No routine angiographic coronary artery assessment vs. routine invasive coronary angiography and PCI
PCI recommended for coronary diameter stenosis of ≥ 80% in coronary segments with a reference vessel diameter of at least 2.5 mm.
Composite of all-cause death, myocardial infarction, any stroke and heart failure hospitalization (VARC-3 criteria)
The presence of moderate or severe mitral regurgitation and tricuspid regurgitation and clinically significant mitral stenosis (mitral valve area ≤1.5 cm2) is not infrequently observed in patients with severe AS and associated with an increased risk of adverse events even after AVR, , 113. Doldi PM, Steffen J, Stolz L, et al. Impact of mitral regurgitation aetiology on the outcomes of transcatheter aortic valve implantation. EuroIntervention. 2023;19:526-536 Link114. Tomii D, Okuno T, Praz F, et al. Potential Candidates for Transcatheter Tricuspid Valve Intervention After Transcatheter Aortic Valve Replacement: Predictors and Prognosis. JACC Cardiovasc Interv. 2021;14:2246-2256 Link115. Asami M, Windecker S, Praz F, et al. Transcatheter aortic valve replacement in patients with concomitant mitral stenosis. Eur Heart J. 2019;40:1342-1351 Link. Therefore, the presence of concomitant valvular heart disease should be carefully evaluated before the intervention (Figure 10)116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link. However, diagnosis of multivalvular disease is challenging since the haemodynamic interdependency between primary and secondary valvular lesions complicates the assessment of the true severity of each valvular lesion. Similarly, treatment strategy and timing of interventions are complex due to lack of prospective studies and uncertainty of best clinical practice. For patients with severe AS and significant primary valvular heart disease, SAVR and concomitant surgical valve repair/replacement is the first-line therapy unless the surgical risk is not high. In turn, secondary/functional valvular disease is more likely to regress after aortic valve intervention, thus TAVI followed by transcatheter intervention for persistent secondary/functional valvular disease is reasonable in this population (Figure 10). Furthermore, the multidisciplinary Heart Team plays a key role to in integrating the plethora of clinical, echocardiographic, haemodynamic, and anatomical data, upon which an optimal management strategy can be planned for each individual117. Khan F, Okuno T, Malebranche D, et al. Transcatheter Aortic Valve Replacement in Patients With Multivalvular Heart Disease. JACC Cardiovasc Interv. 2020;13:1503-1514 Link.
Figure 10
Prevalence of concomitant valve disease in transcatheter aortic valve implantation and potential treatment strategies. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Anatomical risk stratification based on aortic root anatomy is one of the key considerations in patient selection for TAVI or SAVR. In patients with unfavourable aortic root anatomy, the procedural and device success of TAVI may be diminished, leading to unfavourable clinical outcome. Therefore, Heart Team needs to evaluate typical anatomical considerations before the procedure and determine an individual decision-making (Figure 11)116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link.
Figure 11
Unfavorable aortic root anatomy for transcatheter aortic valve implantation. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Aortic valve leaflet and left ventricular outflow tract calcification
Severely calcified device landing zone is an important anatomical consideration that increases the risk of PVR, annular rupture, coronary obstruction, stroke, and conduction disturbances after TAVI, , , , 118. Seiffert M, Fujita B, Avanesov M, et al. Device landing zone calcification and its impact on residual regurgitation after transcatheter aortic valve implantation with different devices. Eur Heart J. Cardiovasc Imaging 2016;17:576-584 Link119. Abramowitz Y, Jilaihawi H, Pibarot P, et al. Severe aortic stenosis with low aortic valve calcification: characteristics and outcome following transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2017;18:639-647 Link120. Kim WK, Blumenstein J, Liebetrau C, et al. Comparison of outcomes using balloon-expandable versus self-expanding transcatheter prostheses according to the extent of aortic valve calcification. Clin Res Cardiol. 2017;106:995-1004 Link121. Okuno T, Asami M, Heg D, et al. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13:1789-1799 Link122. Reddy P, Merdler I, Ben-Dor I, et al. Cerebrovascular events after transcatheter aortic valve implantation. EuroIntervention. 2024;20:e793-e805 Link. Owing to improvements in TAVI technology, the frequency of PVR has declined, , , 123. Forrest JK, Kaple RK, Tang GHL, et al. Three Generations of Self-Expanding Transcatheter Aortic Valves: A Report From the STS/ACC TVT Registry. JACC Cardiovasc Interv. 2020;13:170-179 Link124. Rheude T, Pellegrini C, Lutz J, et al. Transcatheter Aortic Valve Replacement With Balloon-Expandable Valves: Comparison of SAPIEN 3 Ultra Versus SAPIEN 3. JACC Cardiovasc Interv. 2020;13:2631-2638 Link125. Zaid S, Attizzani GF, Krishnamoorthy P, et al. First-in-Human Multicenter Experience of the Newest Generation Supra-Annular Self-Expanding Evolut FX TAVR System. JACC Cardiovasc Interv. 2023;16:1626-1635 Link126. Stinis CT, Abbas AE, Teirstein P, et al. Real-World Outcomes for the Fifth-Generation Balloon Expandable Transcatheter Heart Valve in the United States. JACC Cardiovasc Interv. 2024;17:1032-1044 Link, while the adverse impact of excess leaflet calcification and severe left ventricular outflow tract (LVOT) calcification remains an important consideration even with newer-generation TAVI devices. In a retrospective analysis of 1,635 patients, moderate or severe LVOT calcification conferred an increased risk of annular rupture when treated with balloon-expandable devices, and a higher incidence of PVR irrespective of valve type or generation121. Okuno T, Asami M, Heg D, et al. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13:1789-1799 Link. SAVR should be considered in low-risk surgical patients with excessive calcification in the device implantation zone, as the calcified leaflets and calcium extension into the annulus and LVOT can be removed.
Small aortic root
The presence of a small aortic root, including small aortic annulus, low-take-off of coronary ostium, and shallow sinus of Valsalva poses a clinical challenge in the management of patients with severe AS. A small aortic annulus may be associated with a high residual prosthetic gradient and prosthesis-patient mismatch resulting in reduced exercise capacity. Although there is no established definition of small aortic annulus (aortic annulus area ≤400 or 430 cm2, aortic annulus perimeter ≤73 mm, etc.), up to 40% of patients with severe AS undergoing SAVR or TAVI have this anatomical feature, , 127. Freitas-Ferraz AB, Tirado-Conte G, Dagenais F, et al. Aortic Stenosis and Small Aortic Annulus. Circulation. 2019;139:2685-2702 Link128. Abdelghani M, Mankerious N, Allali A, et al. Bioprosthetic Valve Performance After Transcatheter Aortic Valve Replacement With Self-Expanding Versus Balloon-Expandable Valves in Large Versus Small Aortic Valve Annuli: Insights From the CHOICE Trial and the CHOICE-Extend Registry. JACC Cardiovasc Interv. 2018;11:2507-2518 Link129. Deeb GM, Chetcuti SJ, Yakubov SJ, et al. Impact of Annular Size on Outcomes After Surgical or Transcatheter Aortic Valve Replacement. Ann Thorac Surg. 2018;105:1129-1136 Link. The optimal treatment strategy in this population has not been determined. TAVI with self-expanding valve has been considered the preferred treatment in patients with small aortic annulus due to improved bioprosthetic haemodynamic outcomes compared with balloon-expandable devices, although it remains unclear whether differences in haemodynamic outcomes translate into clinical benefit, 130. Okuno T, Tomii D, Lanz J, et al. 5-Year Outcomes With Self-Expanding vs Balloon-Expandable Transcatheter Aortic Valve Replacement in Patients With Small Annuli. JACC Cardiovasc Interv. 2023;16:429-440 Link131. Scotti A, Sturla M, Costa G, et al. Evolut PRO and SAPIEN ULTRA Performance in Small Aortic Annuli: The OPERA-TAVI Registry. JACC Cardiovasc Interv. 2024;17:681-692 Link. The randomized SMART trial compared balloon-expandable SAPIEN 3/SAPIEN 3 Ultra with self-expanding Evolut PRO/PRO Plus/FX in patients with small aortic annuli (aortic annulus area ≤430 mm2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link by multi-detector computed tomography [MDCT]). In this unblinded trial, patients allocated to a self-expanding valve had a lower rate of bioprosthetic valve dysfunction and haemodynamic structural valve dysfunction (irrespective of definition of bioprosthetic valve dysfunction [BVD]) and better quality-of-life KCCQ ordinal outcomes compared with patients allocated to a balloon-expandable device at 12 months follow-up132. Herrmann HC, Mehran R, Blackman DJ, et al. Self-Expanding or Balloon-Expandable TAVR in Patients with a Small Aortic Annulus. N Engl J Med. 2024;390:1959-1971 Link. The VIVA trial was a RCT comparing SAVR with TAVI in patients with small aortic annuli defined as aortic annulus mean diameter ≤23 mm or minimal diameter <21.5 mm by MDCT (N = 156). In the VIVA trial, there was no significant difference between TAVI and SAVR with respect to valve haemodynamic results (severe prosthesis-patient mismatch or moderate-severe PVR at 60 days: 5.6% vs. 10.3%, P = 0.30) and clinical outcomes (death, stroke, and cardiac hospitalization)133. Rodes-Cabau J, Ribeiro HB, Mohammadi S, et al. Transcatheter or Surgical Aortic Valve Replacement in Patients With Severe Aortic Stenosis and Small Aortic Annulus: A Randomized Clinical Trial. Circulation. 2024;149:644-655 Link.
Another anatomical risk of TAVI related to small aortic root is the risk of coronary obstruction or impaired coronary access in case of low take-off of the coronary ostia in the setting of a shallow sinus of Valsalva, , , 134. Pilgrim T, Tomii D. Predicting Coronary Obstruction After TAVR: Better Safe Than Sorry. JACC Cardiovasc Interv. 2023;16:426-428 Link135. Ibrahim H, Chaus A, Alkhalil A, Prescher L, Kleiman N. Coronary Artery Obstruction After Transcatheter Aortic Valve Implantation: Past, Present, and Future. Circ Cardiovasc Interv. 2024;17:e012827 Link136. Barbanti M, Costa G, Picci A, et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc Interv. 2020;13:2542-2555 Link137. Tarantini G, Nai Fovino L, Scotti A, et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment: The ALIGN-ACCESS Study. Circ Cardiovasc Interv. 2022;15:e011045 Link. Several procedural techniques have been developed to mitigate the risk of coronary obstruction and to maintain coronary access, which will be discussed in a later section. The decision process in small aortic root anatomy should take into account the expected haemodynamic results, the risk of coronary obstruction and feasibility of coronary protection, the need for future coronary access, and lifetime management with respect to potential risks associated with repeat interventions.
Extremely large aortic annulus
Patients with annulus dimensions beyond the recommended range, extremely large aortic annuli, do not allow for optimal THV sizing. Several reports have summarized the feasibility and safety of TAVI with newer-generation devices using overexpansion in patients with extremely large aortic annuli (annulus area ≥683 mm2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link or perimeter ≥94.2 mm), 138. Armijo G, Tang GHL, Kooistra N, et al. Third-Generation Balloon and Self-Expandable Valves for Aortic Stenosis in Large and Extra-Large Aortic Annuli From the TAVR-LARGE Registry. Circ Cardiovasc Interv. 2020;13:e009047 Link139. Sengupta A, Zaid S, Kamioka N, et al. Mid-Term Outcomes of Transcatheter Aortic Valve Replacement in Extremely Large Annuli With Edwards SAPIEN 3 Valve. JACC Cardiovasc Interv. 2020;13:210-216 Link. In a multicenter study, 124 patients with extremely large aortic annulus had a comparable rate of procedural and in-hospital outcomes after TAVI compared with patients with large aortic annulus (annulus area ≥575 mm2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link or perimeter ≥85 mm) (in-hospital death: 0.8% vs. 2.5%, P = 0.337; in-hospital stroke: 4.0% vs. 1.6%, P = 0.076; device success: 93.1% vs. 94.6%, P = 0.672)138. Armijo G, Tang GHL, Kooistra N, et al. Third-Generation Balloon and Self-Expandable Valves for Aortic Stenosis in Large and Extra-Large Aortic Annuli From the TAVR-LARGE Registry. Circ Cardiovasc Interv. 2020;13:e009047 Link. It should be noted that these data are currently limited to 1-year follow-up. A bench study has suggested that excessive overexpansion may affect leaflet integrity and hydrodynamic function including regurgitation and durability140. Sathananthan J, Sellers S, Barlow A, et al. Overexpansion of the SAPIEN 3 Transcatheter Heart Valve: An Ex Vivo Bench Study. JACC Cardiovasc Interv. 2018;11:1696-1705 Link. A newer-generation balloon-expandable Myval device is available with two additional sizes (30.5 and 32.5 mm), covering larger annulus areas up to 840 mm2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link. Future studies will determine whether optimal sizing TAVI in patients with extremely large annulus results in clinical outcomes comparable to SAVR.
Horizontal aorta
Horizontal aorta, defined as aortic angulation, the angle between the horizontal plane and the plane of the aortic annulus in a coronal projection, greater than 70 degrees, is an important anatomical consideration for TAVI, particularly with some self-expanding devices without steerable delivery systems. Although several studies have evaluated the feasibility of TAVI in patients with higher aortic angulation (e.g., >48 degrees), an inadequate number of patients with horizontal aorta was included, 141. Gallo F, Gallone G, Kim WK, et al. Horizontal Aorta in Transcatheter Self-Expanding Valves: Insights From the HORSE International Multicentre Registry. Circ Cardiovasc Interv. 2021;14:e010641 Link142. Medranda GA, Musallam A, Zhang C, et al. The Impact of Aortic Angulation on Contemporary Transcatheter Aortic Valve Replacement Outcomes. JACC Cardiovasc Interv. 2021;14:1209-1215 Link. In a retrospective analysis including 1,214 patients undergoing TAVI with a balloon-expandable SAPIEN 3 or SAPIEN 3 Ultra device, horizontal aorta was observed in 38 patients (3.1%) without apparent impact on procedural and device success and risk of periprocedural complications143. Nakase M, Tomii D, Praz F, et al. Safety and Efficacy of Balloon-Expandable Transcatheter Aortic Valve Implantation in Patients With Extreme Horizontal Aorta. Can J Cardiol. 2024;40:402-404 Link.
Non-calcified aortic valve
Non-calcified aortic valve morphology has been considered a risk factor for valve embolization or dislocation of THV due to insufficient anchoring of the THV. A single-center observational study of 1,358 patients undergoing TAVI for native severe high-gradient AS reported that patients with less calcified aortic valve, defined as aortic valve leaflet calcium volume ≤163 mm3. Lieberman EB, Bashore TM, Hermiller JB, et al. Balloon aortic valvuloplasty in adults: failure of procedure to improve long-term survival. J Am Coll Cardiol. 1995;26:1522-1528 Link quantified on contrast-enhanced MDCT images with a predefined threshold of 850 HU, had a higher prevalence of autoimmune disease, higher body mass index, female sex, hypertension, and tricuspid valve morphology. Although overall procedural success and clinical outcomes were similar in patients with less calcified AS, these results suggest a distinct pathophysiological and clinical entity144. Maznyczka A, Tomii D, Angellotti D, et al. Fibrotic vs Calcific Aortic Stenosis: Characteristics and Outcomes in Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2024;17:2969-2971 Link. Several studies have suggested that the detection of fibrotic tissue provides a more accurate anatomical risk assessment in patients with AS, particularly in those in whom leaflet fibrosis rather than calcification is a major contributor to valve obstruction, , 145. Cartlidge TR, Bing R, Kwiecinski J, et al. Contrast-enhanced computed tomography assessment of aortic stenosis. Heart. 2021;107:1905-1911 Link146. Grodecki K, Tamarappoo BK, Huczek Z, et al. Non-calcific aortic tissue quantified from computed tomography angiography improves diagnosis and prognostication of patients referred for transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2021;22:626-635 Link147. Grodecki K, Olasinska-Wisniewska A, Cyran A, et al. Quantification of Aortic Valve Fibrotic and Calcific Tissue from CTA: Prospective Comparison with Histology. Radiology. 2024;312:e240229 Link. A group from the nationwide POL-TAVI registry proposed a semi-automated method to identify and quantify aortic valve tissue components as calcific and non-calcific and reported that their method correlated well with histopathological quantification, 146. Grodecki K, Tamarappoo BK, Huczek Z, et al. Non-calcific aortic tissue quantified from computed tomography angiography improves diagnosis and prognostication of patients referred for transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2021;22:626-635 Link147. Grodecki K, Olasinska-Wisniewska A, Cyran A, et al. Quantification of Aortic Valve Fibrotic and Calcific Tissue from CTA: Prospective Comparison with Histology. Radiology. 2024;312:e240229 Link. In addition, they reported that non-calcific aortic valve tissue volume was associated with a five-fold increased risk of MACE at 30 days after TAVI146. Grodecki K, Tamarappoo BK, Huczek Z, et al. Non-calcific aortic tissue quantified from computed tomography angiography improves diagnosis and prognostication of patients referred for transcatheter aortic valve implantation. Eur Heart J. Cardiovasc Imaging 2021;22:626-635 Link.
Vascular access
The established evidence for TAVI, particularly in the recent low-risk trials, is predominantly based on transfemoral TAVI, and current guidelines assign a Class I recommendation for transfemoral TAVI, 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. In contrast, the available evidence for non-transfemoral TAVI is limited to observational studies and subgroup analyses in early randomized trials, , , , 11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link12. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790-1798 Link46. Makkar RR, Thourani VH, Mack MJ, et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382:799-809 Link57. Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2477-2484 Link148. Beurtheret S, Karam N, Resseguier N, et al. Femoral Versus Nonfemoral Peripheral Access for Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2019;74:2728-2739 Link. Although several studies have suggested that the benefits of non-transfemoral TAVI are similar to those of transfemoral TAVI, the transfemoral approach is generally the least invasive and standard strategy to perform TAVI. Indeed, in the transthoracic TAVI cohort of the PARTNER 2A trial, TAVI was inferior to SAVR in terms of death or disabling stroke at 5 years (59.3% vs. 48.3%, P = 0.03)46. Makkar RR, Thourani VH, Mack MJ, et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382:799-809 Link. Therefore, the evaluation of iliofemoral access anatomy is important in the choice between SAVR and TAVI and between transfemoral and non-transfemoral access (Figure 12). Recently, a simplified scoring system based on preprocedural MDCT, the Hostile score, has been proposed to quantify the extent of atherosclerosis and assess the risk of complications in patients with peripheral artery disease undergoing TAVR149. Palmerini T, Saia F, Kim WK, et al. Vascular Access in Patients With Peripheral Arterial Disease Undergoing TAVR: The Hostile Registry. JACC Cardiovasc Interv. 2023;16:396-411 Link. The scoring system was validated in a large single-center TAVI registry of 2,023 patients undergoing transfemoral TAVI with a contemporary device and demonstrated that the Hostile score was an independent predictor of non-puncture site vascular complications, whereas its performance in predicting puncture site vascular complications was modest150. Nakase M, Tomii D, Samim D, et al. Impact of Severity and Extent of Iliofemoral Atherosclerosis on Clinical Outcomes in Patients Undergoing TAVR. JACC Cardiovasc Interv. 2024;17:2353-2363 Link.
Figure 12
Unfavorable iliofemoral arterial anatomy for transcatheter aortic valve implantation. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Coronary access after TAVI can be challenging if the native leaflet is longer than the coronary height, particularly in a narrow sinus of Valsalva. If the stent frame of the THV extends above the take-off of the coronary arteries, misalignment of the stent frame with the native commissures (or the take-off of the coronary arteries in case of eccentric coronary take-off) further complicates coronary access (Figure 13), 136. Barbanti M, Costa G, Picci A, et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc Interv. 2020;13:2542-2555 Link151. Sondergaard L, De Backer O. Transcatheter aortic valve implantation: don't forget the coronary arteries. EuroIntervention. 2018;14:147-149 Link. The difficulty is highlighted after valve-in-valve TAVI (TAV-in-SAV or TAV-in-TAV) due to a Neoskirt potentially extending above the coronary ostia or in case of TAV-in-TAV with unfavourable overlap of stent frame struts (Figure 14), , 152. Tomii D, Okuno T, Lanz J, et al. Valve-in-valve TAVI and risk of coronary obstruction: Validation of the VIVID classification. J Cardiovasc Comput Tomogr. 2023;17:105-111 Link153. Tarantini G, Tang G, Nai Fovino L, et al. Management of coronary artery disease in patients undergoing transcatheter aortic valve implantation. A clinical consensus statement from the European Association of Percutaneous Cardiovascular Interventions in collaboration with the ESC Working Group on Cardiovascular Surgery. EuroIntervention 2023;19:37-52 Link154. De Backer O, Landes U, Fuchs A, et al. Coronary Access After TAVR-in-TAVR as Evaluated by Multidetector Computed Tomography. JACC Cardiovasc Interv. 2020;13:2528-2538 Link. The rate of unsuccessful selective coronary cannulation is particularly noteworthy with self-expanding THV with a tall stent frame extending beyond the take-off of the coronary arteries, , 136. Barbanti M, Costa G, Picci A, et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc Interv. 2020;13:2542-2555 Link137. Tarantini G, Nai Fovino L, Scotti A, et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment: The ALIGN-ACCESS Study. Circ Cardiovasc Interv. 2022;15:e011045 Link151. Sondergaard L, De Backer O. Transcatheter aortic valve implantation: don't forget the coronary arteries. EuroIntervention. 2018;14:147-149 Link. Implications of challenging coronary access are accentuated in patients presenting with acute myocardial infarction, although the incidence of ST-segment elevation myocardial infarction after TAVI is low (<1%)155. Faroux L, Lhermusier T, Vincent F, et al. ST-Segment Elevation Myocardial Infarction Following Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2021;77:2187-2199 Link. There is limited data on repeat coronary intervention after AVR but known CAD increases the risk of future interventions, 156. Celik M, Durko AP, Head SJ, et al. Coronary revascularization after surgical aortic valve replacement. JTCVS Open. 2020;3:91-101 Link157. Okuno T, Demirel C, Tomii D, et al. Long-term risk of unplanned percutaneous coronary intervention after transcatheter aortic valve replacement. EuroIntervention. 2022;18:797-803 Link. The integrated assessment of future coronary access after AVR, including AVR modality and type of THV, should be included in the decision-making process of treatment strategies in patients with severe AS.
Figure 13
Coronary access after transcatheter aortic valve implantation. Figures reproduced from Tarantini et al. EuroIntervention 2023;19(1):37-52.
Redo-transcatheter aortic valve implantation: different THV–in–THV combinations. Figures reproduced and modified from De Backer et al. JACC Cardiovasc Interv 2020;13(21):2528-2538.
Multidisciplinary Heart Team and Centres of Excellence
The value of the Multidisciplinary Heart Team has become increasingly apparent, and decisions concerning treatment and intervention should be made by a collaborative Heart Team with expertise in valvular heart disease. Key members of the Multidisciplinary Heart Team include clinical and interventional cardiologists, cardiac surgeons, imaging specialists with expertise in interventional imaging, cardiovascular anaesthesiologists, dedicated cardiovascular nurses, and other specialists if necessary (e.g. heart failure specialists or electrophysiologists). Current guidelines recommend that aortic valve interventions must be performed in Heart Valve Centres that declare their local expertise and outcomes data, have active interventional cardiology and cardiac surgical programmes on site, and a structured collaborative Heart Team approach (Figure 15), , 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link.
Figure 15
Comprehensive heart valve centre. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Pre-procedural planning is of critical importance when considering TAVI. Operators should integrate clinical and imaging data obtained by MDCT, echocardiography, and cardiac catheterization to determine the best procedural strategy. Because various TAVI devices are available (Figure 8), operators need to be familiar with the strengths and limitations of each device, 158. Claessen BE, Tang GHL, Kini AS, Sharma SK. Considerations for Optimal Device Selection in Transcatheter Aortic Valve Replacement: A Review. Jama. Cardiol 2021;6:102-112 Link159. Okuno T, Khan F, Asami M, et al. Prosthesis-Patient Mismatch Following Transcatheter Aortic Valve Replacement With Supra-Annular and Intra-Annular Prostheses. JACC Cardiovasc Interv. 2019.;12:2173-2182 Link. Device sizing should be carefully determined based on the manufacturers’ sizing chart and annulus dimensions derived by MDCT. In patients with unfavourable iliofemoral anatomy, the decision to perform concomitant peripheral interventions (balloon angioplasty, intravascular lithotripsy, use of parallel stiff wire, or surgical cut-down) and the selection of alternative access sites should be determined by patients’ anatomic features and comorbidities as well as local experience. Preventative strategies and management of potential complications should also be discussed before the procedure. If patients are deemed at high-risk of coronary obstruction, operators need to consider coronary protection (more detailed description will be provided in a later section) and emergency coronary revascularization. For patients deemed at high risk of intraprocedural cerebrovascular events, such as excessive aortic valve leaflet calcification, cerebral embolic protection devices may be considered to capture or deflect emboli to the brain (Figure 16), , 160. Haussig S, Mangner N, Dwyer MG, et al. Effect of a Cerebral Protection Device on Brain Lesions Following Transcatheter Aortic Valve Implantation in Patients With Severe Aortic Stenosis: The CLEAN-TAVI Randomized Clinical Trial. JAMA. 2016;316:592-601 Link161. Schmidt T, Schlüter M, Alessandrini H, et al. Histology of debris captured by a cerebral protection system during transcatheter valve-in-valve implantation. Heart. 2016;102:1573-1580 Link162. Stachon P, Kaier K, Heidt T, et al. The Use and Outcomes of Cerebral Protection Devices for Patients Undergoing Transfemoral Transcatheter Aortic Valve Replacement in Clinical Practice. JACC Cardiovasc Interv. 2021;14:161-168 Link. It should be noted, however, that there is no robust evidence that the use of cerebral embolic protection devices reduces the incidence of cerebrovascular events, , 163. Kapadia SR, Kodali S, Makkar R, et al. Protection Against Cerebral Embolism During Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2017;69:367-377 Link164. Nazif TM, Moses J, Sharma R, et al. Randomized Evaluation of TriGuard 3 Cerebral Embolic Protection After Transcatheter Aortic Valve Replacement: REFLECT II. JACC Cardiovasc Interv. 2021;14:515-527 Link165. Kapadia SR, Makkar R, Leon M, et al. Cerebral Embolic Protection during Transcatheter Aortic-Valve Replacement. N Engl J Med. 2022;387:1253-1263 Link.
The TAVI procedure can be performed in a hybrid operating room or cardiac catheterization laboratory under general anaesthesia or local anaesthesia with or without conscious sedation. In the randomized SOLVE-TAVI trial comparing local anaesthesia with conscious sedation versus general anaesthesia in patients undergoing TAVI, local anaesthesia with conscious sedation resulted in lower rates of catecholamine use (62.8% vs. 97.3%, P <0.001) and the primary composite endpoint of all-cause death, stroke, myocardial infarction, infection requiring antibiotic treatment, and acute kidney injury at 30 days was similar between groups (27.2% vs. 26.4%, P for equivalence= 0.015)167. Thiele H, Kurz T, Feistritzer HJ, et al. General Versus Local Anesthesia With Conscious Sedation in Transcatheter Aortic Valve Implantation: The Randomized SOLVE-TAVI Trial. Circulation. 2020;142:1437-1447 Link. As the learning curve of the TAVI procedure continues to improve in addition to the expansion into lower risk patient populations, TAVI under local anaesthesia with or without conscious sedation has become the standard strategy in most institutions. In the STS/ACC TVT registry, the use of conscious sedation has increased from 33% in 2016 to 64% in early 2019, with a wide variability in the use of general anaesthesia, with a few centres using only general anaesthesia168. Butala NM, Chung M, Secemsky EA, et al. Conscious Sedation Versus General Anesthesia for Transcatheter Aortic Valve Replacement: Variation in Practice and Outcomes. JACC Cardiovasc Interv. 2020;13:1277-1287 Link. The shift represents the elimination of routinely used transesophageal echocardiography, orotracheal intubation, and other invasive monitoring techniques24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link. Currently general anaesthesia is typically reserved for non-femoral access TAVI or anticipated complex procedures.
Antithrombotic management during TAVI
Among patients without indication for long-term oral anticoagulation (OAC), pre-procedural loading with low-dose aspirin is adopted and procedural anticoagulation is achieved with administration of unfractionated heparin maintaining an activated clotting time of 250-300 seconds. Bivalirudin or Argatroban can be used alternatively in patients with a history of heparin-induced thrombocytopenia. In a randomized trial comparing bivalirudin and heparin as the procedural anticoagulant agent in patients undergoing transfemoral TAVI, bivalirudin did not meet superiority criteria for major bleeding at 48 hours (6.9% vs. 9.0%, P = 0.27), but was found non-inferior in terms of net adverse cardiovascular events including all-cause death, myocardial infarction, or stroke at 30 days (14.4% vs. 16.1%, Pnon-inferiority <0.01)169. Dangas GD, Lefevre T, Kupatt C, et al. Bivalirudin Versus Heparin Anticoagulation in Transcatheter Aortic Valve Replacement: The Randomized BRAVO-3 Trial. J Am Coll Cardiol. 2015;66:2860-2868 Link.
Haemostasis may not be adequately achieved under the anticoagulant effect of heparin. Heparin reversal by the administration of protamine is routinely used in cardiac surgery to reduce bleeding complications. Accordingly, protamine administration at the time of sheath removal and closure of the arteriotomy site can be considered in patients undergoing transfemoral TAVI. Available data is limited to one RCT and a few observational studies, and potential risks of protamine including allergic reactions, hypotension, bronchospasm, and skin reactions have been reported170. Al-Kassou B, Kandt J, Lohde L, et al. Safety and Efficacy of Protamine Administration for Prevention of Bleeding Complications in Patients Undergoing TAVR. JACC Cardiovasc Interv. 2020;13:1471-1480 Link. The ACE-PROTAVI trial was an investigator-initiated, placebo-controlled randomized clinical investigating of the efficacy and safety of routine protamine administration after transfemoral TAVI. In this trial, 410 patients were randomly assigned to either the protamine or placebo groups. Compared with patients receiving placebo, patients receiving up-front protamine administration had a higher rate of haemostasis success (97.9% vs. 91.6%, P = 0.006), a shorter median time to haemostasis (181 seconds vs. 279 seconds, P = 0.002), and a reduced risk of the composite of all-cause death, major and minor bleeding complications, or major and minor vascular complications at 30 days (5.2% vs. 12.8%, P = 0.01), predominantly driven by the difference in the prevalence of minor vascular complications (2.1% vs. 8.4%, P = 0.01)171. Vriesendorp PA, Nanayakkara S, Heuts S, et al. Routine Protamine Administration for Bleeding in Transcatheter Aortic Valve Implantation: The ACE-PROTAVI Randomized Clinical Trial. JamaCardiol. 2024;9:901-908. Link.
Among patients with indication for long-term OAC, the decision to continue or discontinue OAC during cardiovascular interventions requires balancing the risk between thromboembolic and bleeding complications172. Douketis JD, Spyropoulos AC. Perioperative Management of Anticoagulant and Antiplatelet Therapy. NEJM Evid. 2023;2:EVIDra2200322 Link. In certain cardiac interventions, including catheter ablation for atrial fibrillation, pacemaker implantation, and PCI, continuation of OAC is associated with lower rates of bleeding and similar or even lower rates of embolic complications, , 173. Birnie DH, Healey JS, Wells GA, et al. Pacemaker or defibrillator surgery without interruption of anticoagulation. N Engl J Med. 2013;368:2084-2093 Link174. Hindricks G, Potpara T, Dagres N, et al. 2020 ESC Guidelines for the diagnosis and management of atrial fibrillation developed in collaboration with the European Association for Cardio-Thoracic Surgery (EACTS): The Task Force for the diagnosis and management of atrial fibrillation of the European Society of Cardiology (ESC) Developed with the special contribution of the European Heart Rhythm Association (EHRA) of the ESC. Eur Heart J. 2021;42:373-498 Link175. Venetsanos D, Skibniewski M, Janzon M, et al. Uninterrupted Oral Anticoagulant Therapy in Patients Undergoing Unplanned Percutaneous Coronary Intervention. JACC Cardiovasc Interv. 2021;14:754-763 Link. Recent observational data suggest that there is favourable association between continued OAC and clinical outcomes in TAVI population, 176. Brinkert M, Mangner N, Moriyama N, et al. Safety and Efficacy of Transcatheter Aortic Valve Replacement With Continuation of Vitamin K Antagonists or Direct Oral Anticoagulants. JACC Cardiovasc Interv. 2021;14:135-144 Link177. Mangner N, Brinkert M, Keller LS, et al. Continued non-vitamin K antagonist oral anticoagulants versus vitamin K antagonists during transcatheter aortic valve implantation. EuroIntervention. 2023;18:e1066-e1076 Link. The POPular PAUSE TAVI randomized control trial evaluated the safety and efficacy of periprocedural continuation versus interruption of OAC during TAVI. In this trial, 869 patients with an indication for long-term OAC use undergoing transfemoral or transsubclavian TAVI were randomly assigned to a continued or interrupted OAC strategy. In the interrupted strategy group, OAC regimens were interrupted 48-120 hours before TAVI, depending on the type of OAC, and renal function and heparin bridging was not initiated. At 30 days, the primary composite endpoint of cardiovascular mortality, all stroke, myocardial infarction, major vascular complications, or major bleeding after TAVI was 16.5% in the continued strategy group and 14.8% in the interrupted strategy group, respectively, and the continued strategy did not meet the non-inferiority criteria for the primary endpoint (Pnon-inferiority = 0.18). Although the rate of thromboembolic events was similar between groups, more bleeding complications (all and major bleeding) occurred in the continued strategy group. These results suggest that interruption of OAC is reasonable in patients undergoing TAVI as compared to other cardiac procedures due to their older age, advanced frailty, and comorbidities178. van Ginkel DJ, Bor WL, Aarts HM, et al. Continuation versus Interruption of Oral Anticoagulation during TAVI. N Engl J Med. 2025;392:438-449 Link.
Antibiotic prophylaxis
Patients with prosthetic valves are at increased risk for infective endocarditis. Considering the worse outcomes of patients with prosthetic valve endocarditis as compared to patients with native valve endocarditis, clinical guidelines for the management of infective endocarditis recommend antibiotic prophylaxis (Class I recommendation). During transcatheter valve procedures, staphylococcal and enterococcal species predominate are common, with enterococcal infections being more prevalent periprocedurally, potentially related to the flora colonizing the groin when transfemoral access is used. This underscores the focus on procedural infection prevention, including aseptic measures during the insertion and manipulation of catheters using surgical standards, as well as prophylaxis. With regards to antibiotic prophylaxis, the guidelines recommend antibiotic prophylaxis to cover for Enterococcus spp179. Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44:3948-4042 Link:
A single dose of amoxicillin/clavulanic acid 2.2 g IV within 120 min of vascular access (ideally within 60 min) (a single dose of ampicillin 3 g IV can be used alternatively).
In case of beta-lactam allergy, a single dose of vancomycin 15 mg/kg or teicoplanin 9-12 mg/kg IV.
Procedural step 1: Transfemoral access
The main femoral access (for THV delivery) is established. Because vascular complications of femoral access are related to high or low punctures, multiple punctures, or inadequate haemostasis technique, ultrasound-guided needle puncture is recommended to ensure that the puncture site is in the common femoral segment excluding the femoral bifurcation, and in a segment free of significant calcification180. Vincent F, Spillemaeker H, Kyheng M, et al. Ultrasound Guidance to Reduce Vascular and Bleeding Complications of Percutaneous Transfemoral Transcatheter Aortic Valve Replacement: A Propensity Score-Matched Comparison. J Am Heart Assoc. 2020;9:e014916 Link. Several studies have shown that the use of a micropuncture kit (Cook Medical, Bloomington, IN) containing a 21 G needle followed by insertion of a 4 Fr sheath reduces the rate of access site complications181. Ben-Dor I, Sharma A, Rogers T, et al. Micropuncture technique for femoral access is associated with lower vascular complications compared to standard needle. Catheter Cardiovasc Interv. 2021;97:1379-1385 Link. Although the right femoral artery is generally preferred due to its typically straight course and ease of procedural manipulation, the choice of right or left femoral access should be guided by individual patient factors, including vessel diameter (a minimum lumen diameter of >5 mm), tortuosity, calcification, and prior interventions, such as iliofemoral stents or peripheral artery disease surgery (Figure 12), 116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link150. Nakase M, Tomii D, Samim D, et al. Impact of Severity and Extent of Iliofemoral Atherosclerosis on Clinical Outcomes in Patients Undergoing TAVR. JACC Cardiovasc Interv. 2024;17:2353-2363 Link.
Secondary access sites include the radial artery or contralateral femoral access (ipsilateral femoral access in selected cases). Radial access has the potential to reduce clinically relevant secondary access site-related bleeding, while this approach may not fully address vascular complications at the main femoral access site, necessitating an alternative femoral puncture, 182. Burzotta F, Aurigemma C, Romagnoli E, et al. A less-invasive totally-endovascular (LITE) technique for trans-femoral transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2020;96:459-470 Link183. Junquera L, Urena M, Latib A, et al. Comparison of Transfemoral Versus Transradial Secondary Access in Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2020;13:e008609 Link. A small randomized trial of 238 patients undergoing transfemoral TAVI compared secondary upper- and lower-extremity access. The primary endpoint of Bleeding Academic Research Consortium type 2, 3, or 5 bleeding at the secondary access site occurred less frequently in patients assigned to the upper-extremity approach (4.2% vs. 13.4%, odds ratio 0.28, 95% CI 0.28-0.91), whereas this approach was associated with a higher rate of secondary access failure (11.8% vs. 0.8%; odds ratio 15.73, 95% CI 2.03-121.69) and longer procedure times (60.0 min vs. 48.0 min, P = 0.002)184. Versteeg GAA, Rooijakkers MJP, Hemelrijk KI, et al. Upper- vs Lower-Extremity Secondary Access During Transcatheter Aortic Valve Implantation: A Randomized Clinical Trial. Jama. Netw Open 2024;7:e2438578 Link.
The main access site is pre-closed typically by using one or two suture-based vascular closure devices (ProGlide or ProStyle, Abbott, Abbott Park, Illinois). Alternative closure devices such as plug-based vascular closure device (MANTA, Teleflex, Wayne, Pennsylvania) may also be utilized without pre-close (Figure 17). In the randomized CHOICE-CLOSURE trial (N = 516), patients who received a plug-based device (MANTA) had a higher rate of the primary end point of access site- or access-related major and minor vascular complications during the index hospitalization compared with patients allocated to a suture-based device (ProGlide) (19.4% vs. 12.0%, P = 0.029)185. Abdel-Wahab M, Hartung P, Dumpies O, et al. Comparison of a Pure Plug-Based Versus a Primary Suture-Based Vascular Closure Device Strategy for Transfemoral Transcatheter Aortic Valve Replacement: The CHOICE-CLOSURE Randomized Clinical Trial. Circulation. 2022;145:170-183 Link.
Following establishment of femoral arterial access and preclosure, the TAVI delivery sheath (14-18 Fr) is inserted through the main access site using a stiff guidewire providing support and straightening iliofemoral tortuosity. In patients with extensive iliofemoral vascular disease with stenosis and/or calcification, percutaneous balloon angioplasty or intravascular lithotripsy may be required to facilitate sheath insertion186. Di Mario C, Goodwin M, Ristalli F, et al. A Prospective Registry of Intravascular Lithotripsy-Enabled Vascular Access for Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12:502-504 Link. In patients with hostile iliofemoral artery anatomy, alternative access sites may be explored due to the increased risk of vascular complications, , 149. Palmerini T, Saia F, Kim WK, et al. Vascular Access in Patients With Peripheral Arterial Disease Undergoing TAVR: The Hostile Registry. JACC Cardiovasc Interv. 2023;16:396-411 Link187. Nardi G, De Backer O, Saia F, et al. Peripheral intravascular lithotripsy for transcatheter aortic valve implantation: a multicentre observational study. EuroIntervention. 2022;17:e1397-e1406 Link188. Imran HM, Has P, Kassis N, et al. Characteristics, Trends, and Outcomes of Intravascular Lithotripsy-Assisted Transfemoral Transcatheter Aortic Valve Replacement in United States. JACC Cardiovasc Interv. 2024;17:2367-2376 Link.
Access for insertion of a temporary pacemaker may be the jugular or femoral vein. Instead of right ventricular pacing, left ventricular pacing approach via the left ventricular guidewire eliminates the need for a separate puncture, theoretically reducing the associated risk of pericardial effusion. In the randomized EASY TAVI trial (N = 303, all patients received a SAPIEN XT or SAPIEN 3 THV), left ventricular pacing was associated with significantly reduced procedure duration (48.4 ± 16.9 min vs. 55.6 ± 26.9 min, P = 0.0013), while maintaining similar efficacy and safety compared with right ventricular pacing. Effective stimulation, defined as achievement and maintenance of a systolic blood pressure ≤60 mmHg for more than 30 seconds without loss-of-capture was similar in both groups (84.9 vs. 87.1%, P = 0.60). Procedural success was achieved at similar rates (100% vs. 99.3%, P = 0.99), with comparable risks of major adverse cardiovascular events including all-cause death, major cerebrovascular events, myocardial infarction, cardiac tamponade, bleeding events, and vascular complications (13.9% vs. 17.1%, P = 0.44)189. Faurie B, Souteyrand G, Staat P, et al. Left Ventricular Rapid Pacing Via the Valve Delivery Guidewire in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12:2449-2459 Link. The SavvyWire (Opsens Medical) is a new 0.035" preshaped guidewire with dedicated pacing properties and a distal pressure sensor allowing for continuous haemodynamic pressure monitoring. A prospective observational study evaluated the safety and efficacy of the SavvyWire during TAVI. In this study of 20 patients (12 Evolut PRO Plus and 8 SAPEN 3 Ultra, respectively), appropriate left ventricular pacing (180-220 bpm) with at least a 50% reduction in systolic blood pressure and/or a systolic pressure <60 mmHg was achieved in all patients, and there were no cases of pacing capture failure or adverse events related to the SavvyWire. In addition, accurate pressure recordings, defined as pressure wire measurements similar to those obtained simultaneously with a pigtail catheter (difference <5 mmHg) were achieved in all patients190. Rodes-Cabau J, Ibrahim R, De Larochelliere R, et al. A pressure wire for rapid pacing, valve implantation and continuous haemodynamic monitoring during transcatheter aortic valve implantation procedures. EuroIntervention. 2022;18:e345-e348 Link.
The 3-cusp coplanar view for valve implantation as derived from MDCT is confirmed by aortic root angiography prior to valve placement. The nadirs of the three aortic cusps should lie along a single line in this implantation angle. For self-expanding THV implantation, the cusp-overlap view overlapping the right and left coronary cusps can be used to facilitate deployment (Figure 18)191. Tang GHL, Zaid S, Michev I, et al. "Cusp-Overlap" View Simplifies Fluoroscopy-Guided Implantation of Self-Expanding Valve in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2018;11:1663-1665 Link. The advantages of the cusp overlap view include elongation of the LVOT, and improved visualization of the true implantation depth with respect to the non-coronary sinus during THV deployment, as well as better alignment of both the THV system and the annular plane with the image plane (i.e., without parallax). In a multicentre retrospective study, self-expanding THV implantation using the cusp-overlap view was associated with a lower incidence of new permanent pacemaker implantation, and moderate or severe PVR compared with the standard three-cusp view192. Wienemann H, Maier O, Beyer M, et al. Cusp overlap versus standard three-cusp technique for self-expanding Evolut transcatheter aortic valves. EuroIntervention. 2023;19:e176-e187 Link.
The aortic valve is crossed using an Amplatz left (AL 1) catheter and a standard straight-tipped wire (hydrophilic or metallic). Alternative catheters such as an internal mammary or Judkins right can be used depending on the orientation of the aortic root. Once the wire is across the valve, the catheter is carefully advanced into the left ventricle and the straight-tipped wire is removed for an exchange length J-shaped wire.
A pigtail catheter is placed in exchange for the catheter in the left ventricle and directed toward the left ventricular apex. At this time, simultaneous pressure assessment in the left ventricular aorta allows for measurement and recording of the transvalvular gradient.
A pre-shaped stiff wire is then inserted into the left ventricle through the pigtail catheter. Careful attention should be needed to avoid entrapment of the pigtail catheter or wire in the subvalvular mitral valve apparatus, which is usually facilitated by using a RAO fluoroscopic projection.
Verify that the THV is properly crimped, loaded, and oriented on the delivery catheter. For crimping, loading, and orientation verification for each valve platform, refer to the appropriate instructions for use.
In cases of very severe and calcified aortic valve stenosis, predilation may be performed under rapid pacing (at rates of 180 to 200 bpm for up to 20-30 seconds) to facilitate THV delivery and device expansion. The size of the balloon should not exceed the minimum aortic annulus diameter determined by MDCT. The efficacy of pre-dilation has been investigated in a randomized comparison of the implantation of a self-expanding THV with or without pre-dilation (N = 171). Although pre-dilation was associated with a lower post-dilation rate (15.1% vs. 29.4%, P = 0.03), the rate of device success was similar between both groups (74.4% vs. 76.5%; mean difference 2.1%; 90% CI -8.9% to 13%)193. Toutouzas K, Benetos G, Voudris V, et al. Pre-Dilatation Versus No Pre-Dilatation for Implantation of a Self-Expanding Valve in All Comers Undergoing TAVR: The DIRECT Trial. JACC Cardiovasc Interv. 2019;12:767-777 Link.
Under fluoroscopic guidance, the THV is delivered over the pre-shaped stiff wire with careful attention to the wire positioned in the left ventricular apex. The system is carefully advanced across the aortic arch avoiding direct interaction with the aortic wall by appropriate deflection and/or rotation of the assembly.
Once the TAVI system has passed the aortic arch, the fluoroscopic angle is changed to the 3-cusp coplanar view or the cusp-overlap view (typically for self-expanding devices). Subsequently, the THV is carefully advanced across the aortic valve using a pigtail catheter placed in the non-coronary (or right coronary) cusp for reference. Aortic root angiography is then performed to confirm appropriate position.
Valve alignment on the delivery catheter balloon is performed and confirmed in a straight section of the descending aorta. Once the THV has passed the aortic valve, the balloon lock is disengaged and the tip of the Flex Catheter is retracted to the centre of the three markers, followed by re-engaging the balloon lock. The Flex wheel is used in combination with gentle manipulations of the guidewire and handle to adjust the coaxiality of the THV within the annulus and the fine adjustment wheel serves to fine-tune the position of the THV across the valve. Before deployment, it is ensured that the THV is accurately positioned between the alignment markers. Under rapid ventricular pacing (to decrease systolic pressure to 50 mmHg or less), deployment is performed with slow, controlled inflation until the complete predetermined volume within the indeflator has been administered and maintained for 3 seconds. When the balloon catheter is completely deflated, pacing is discontinued and the delivery system removed.
Once the THV is advanced into appropriate implant position (targeting an implant depth of 1-4 mm), deployment (unsheathing) is performed by rotating the deployment knob. Controlled pacing (90 to 120 bpm) is frequently used during the deployment to stabilize the valve during flaring. Periodic aortic root injections guide proper positioning during deployment, which is generally initiated in a cusp-overlap view. Once blood pressure drops due to temporary occlusion of the aortic valve by the expanding THV, the operator continues to turn the deployment wheel until blood pressure recovers. A tactile indicator provides feedback to indicate that the capsule is nearing the “point of no recapture” (at approximately 2/3 deployed). At this point, the imaging projection should be adjusted to remove the parallax in the valve inflow to determine valve position using aortic root angiography and deployment height at the left coronary sinus should be verified in the 3-cusp coplanar view. If the operators are satisfied with the valve position and performance (aiming for no more than 1-4 mm extension into the LVOT), wire-tension is relieved and the THV is slowly fully released. The detachment of frame paddles must be confirmed under fluoroscopy, and the nose cone centered before the delivery system is withdrawn.
In contrast to other self-expanding THV systems, the ACURATE series THV are released from the top downwards with a 2-step procedure. Due to the moderate radial force of the ACURATE series THV, effective balloon predilatation is recommended to facilitate device expansion. Once the THV has passed the aortic valve, ensure that the THV is correctly positioned as indicated by the radiopaque intersection line (marker band), which is located in the mid-portion of the stent body using the annular plane. In addition, the upper crown should be located right above the tips of the native leaflets. After the proper initial position is achieved, the first step can be initiated by turning knob 1 counter-clockwise until full stop, releasing the upper crown and stabilization arches. This step should be performed in a controlled fashion to detect any inappropriate movement of the device. Aortic root angiography should be used to verify the position of the THV. Even after completing step 1, it is still possible to adjust the position. If the operator is satisfied with the position, knob 2 will be turned counter-clockwise to release the lower crown for full deployment of the THV. The detachment of the frame paddles must be confirmed under fluoroscopy, and the nose cone centred before the delivery system is withdrawn.
Once the THV is advanced across the aortic valve, the radiopaque marker on the FlexNav delivery catheter is aligned with the annular plane. Deployment is then initiated by turning the deployment wheel, typically under controlled pacing (90 to 120 bpm). A clicking sound is heard when the delivery system reaches the partial deployment lock. The deployment mechanism will not re-engage until the deployment lock button is activated. At this point, the imaging projection should be adjusted to eliminate the parallax in the valve inflow and confirm the valve positioning using aortic root angiography. Once proper positioning is confirmed, wire-tension is relieved and the valve completely deployed by pressing the deployment lock button and rotating the deployment wheel in the direction of the arrow on the handle until the valve capsule is fully retracted. Fluoroscopy should be used to confirm release of the retainer tabs before withdrawing the system.
The balloon-expandable Myval series THV is crimped directly onto the balloon catheter delivery system. The correct valve alignment on the balloon needs to be confirmed in a straight section of the descending aorta. Under fluoroscopy, dark and light bands can be identified, which allow the operator to position the THV at its designated landing zone, the middle or second dark band on the balloon catheter from the ventricular end (70-80% in the aorta: 20-30% in the ventricle). In case of a challenging anatomy where the THV cannot cross the stenotic valve, the undeployed Myval can be fully retrieved through the iliofemoral sheath. Once the THV has crossed the aortic valve, deployment is performed under rapid pacing, with slow, controlled inflation until the full predetermined volume is administered and maintained for 3 seconds. When the balloon catheter is completely deflated, turn off the pacemaker and remove the delivery system.
Procedural step 4: Implantation technique
High implantation technique
Conventionally, the implantation depth is aimed at an aortic frame to LVOT ratio of 80:20 for balloon-expandable THV and 1-4 mm below the aortic annulus for self-expanding THV Since implantation depth correlates with conduction disturbances, a high deployment technique has been proposed to achieve a lower risk of conduction system impairment after TAVI. Although several modifications are used, the key features of the implantation technique are consistent: for the balloon-expandable SAPIEN THV, the THV is positioned by aligning the radiolucent line that is located on the superior aspect of the lowest set of stent struts of the crimped valve, at the base of the non-coronary cusp; for the self-expanding CoreValve/Evolut THV, the THV is implanted using the cusp-overlap view with a target implantation depth of 0 to 3 mm, , , , , 194. Husser O, Pellegrini C, Kessler T, et al. Predictors of Permanent Pacemaker Implantations and New-Onset Conduction Abnormalities With the SAPIEN 3 Balloon-Expandable Transcatheter Heart Valve. JACC Cardiovasc Interv. 2016;9:244-254 Link195. Mauri V, Reimann A, Stern D, et al. Predictors of Permanent Pacemaker Implantation After Transcatheter Aortic Valve Replacement With the SAPIEN 3. JACC Cardiovasc Interv. 2016;9:2200-2209 Link196. Jilaihawi H, Zhao Z, Du R, et al. Minimizing Permanent Pacemaker Following Repositionable Self-Expanding Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12:1796-1807 Link197. Piayda K, Hellhammer K, Veulemans V, et al. Navigating the "Optimal Implantation Depth" With a Self-Expandable TAVR Device in Daily Clinical Practice. JACC Cardiovasc Interv. 2020;13:679-688 Link198. Sammour Y, Banerjee K, Kumar A, et al. Systematic Approach to High Implantation of SAPIEN-3 Valve Achieves a Lower Rate of Conduction Abnormalities Including Pacemaker Implantation. Circ Cardiovasc Interv. 2021;14:e009407 Link199. Ochiai T, Yamanaka F, Shishido K, et al. Impact of High Implantation of Transcatheter Aortic Valve on Subsequent Conduction Disturbances and Coronary Access. JACC Cardiovasc Interv. 2023;16:1192-1204 Link. In a single center observational study of 160 and 258 patients treated with Evolut R/PRO/PRO Plus and SAPIEN 3 THV, respectively, high implantation techniques had a lower incidence of new conduction disturbances (new permanent pacemaker implantation and new LBBB) at 30 days after TAVI compared with conventional technique for both THV (pacemaker: 0.0% vs. 10.8%, P = 0.02; LBBB: 4.2% vs. 11.3%, P = 0.22 in the Evolut THV and pacemaker: 2.0% vs. 2.2%, P = 1.0; LBBB: 1.1% vs. 7.0%, P = 0.047 in the SAPIEN 3 THV). However, post-TAVI MDCT showed that risk of sinus sequestration in redo-TAVI was significantly higher in the high implantation group compared with the conventional implantation group (Evolut THV: 64.0% vs. 41.8%; P = 0.009; SAPIEN 3 THV: 17.6% vs. 5.3%; P = 0.002)199. Ochiai T, Yamanaka F, Shishido K, et al. Impact of High Implantation of Transcatheter Aortic Valve on Subsequent Conduction Disturbances and Coronary Access. JACC Cardiovasc Interv. 2023;16:1192-1204 Link.
Proposed standardized definition of commisural alignment from the ALIGN-TAVR consortium. Figures reproduced from Tang et al. JACC Cardiovasc Interv 2022;15(15):1497-1518.
In contrast to SAVR, in which the commissural posts are aligned with the native aortic valve commissures distant from the coronary ostia, TAVI may result in the inadvertent placement of THV commissural posts facing a coronary orifice, which renders coronary access challenging. In the multicentre RE-ACCESS and ALIGN-TAVR registries, commissural misalignment was an independent predictor of unsuccessful coronary cannulation after TAVI, 136. Barbanti M, Costa G, Picci A, et al. Coronary Cannulation After Transcatheter Aortic Valve Replacement: The RE-ACCESS Study. JACC Cardiovasc Interv. 2020;13:2542-2555 Link137. Tarantini G, Nai Fovino L, Scotti A, et al. Coronary Access After Transcatheter Aortic Valve Replacement With Commissural Alignment: The ALIGN-ACCESS Study. Circ Cardiovasc Interv. 2022;15:e011045 Link. In addition, commissural misalignment is associated with changes in the fluid flow patterns, increased leaflet stress, and creating nonphysiological vorticity, leading to faster bioprosthetic degeneration200. Tang GHL, Amat-Santos IJ, De Backer O, et al. Rationale, Definitions, Techniques, and Outcomes of Commissural Alignment in TAVR: From the ALIGN-TAVR Consortium. JACC Cardiovasc Interv. 2022;15:1497-1518 Link. Therefore, achieving proper commissural alignment is important in lifetime management considerations of patients with severe AS. The ALIGN-TAVR Consortium has proposed preprocedural planning and implantation techniques to achieve commissural alignment200. Tang GHL, Amat-Santos IJ, De Backer O, et al. Rationale, Definitions, Techniques, and Outcomes of Commissural Alignment in TAVR: From the ALIGN-TAVR Consortium. JACC Cardiovasc Interv. 2022;15:1497-1518 Link. Based on the CT-derived “3-cusp” and “cusp-overlap” views are used during the deployment. For the CoreValve/Evolut THV, a C-paddle locates at 1 of the commissures and is mounted 90º clockwise from the fluoroscopic “Hat” marker. By inserting the delivery catheter with the flush port at 3 o’clock (away from the operator), the “Hat” marker can be better oriented to the centre front in the cusp overlap view during valve implantation, thus improving commissural alignment. With successful commissural alignment, the C-paddle should end up at the inner curve of the ascending aorta in the cusp overlap view. For the ACURATE THV, the commissures can be identified on fluoroscopy by the presence of 3 commissural posts at the base of the stabilizing arches and 3 “free cells” at the level of the upper crown. By inserting the delivery system with the flush port facing 6 o’clock, fine-tuning adjustment (clockwise or counterclockwise rotation) is applied to optimize alignment. The RE-ACCESS 2 study evaluated the rate of unsuccessful coronary access after TAVI in 127 patients who undergoing TAVI with a self-expanding Evolut or Acurate THV using commissural alignment technique. In this study, only 7 patients (5.5%) had unsuccessful coronary cannulation after TAVI and commissural misalignment affected coronary cannulation after TAVR mostly in Evolut THV201. Costa G, Sammartino S, Strazzieri O, et al. Coronary Cannulation Following TAVR Using Self-Expanding Devices With Commissural Alignment: The RE-ACCESS 2 Study. JACC Cardiovasc Interv. 2024;17:727-737 Link. These results demonstrate the utility of the commissural alignment technique. However, it should be noted that a non-negligible proportion of patients have severely eccentric origins of the coronary arteries, particularly in the right coronary artery (>10% of cases), which may compromise commissural alignment even with commissural alignment techniques202. Vinayak M, Tang GHL, Li K, et al. Commissural vs Coronary Alignment to Avoid Coronary Overlap With THV-Commissure in TAVR: A CT-Simulation Study. JACC Cardiovasc Interv. 2024;17:715-726 Link. Furthermore, there is currently no established straightforward technique to obtain commissural alignment for other types of THV.
Oversizing and undersizing in borderline aortic annuli
In patients with borderline aortic annulus areas that fall in between two valve sizes, the operator is faced with the decision to oversize or undersize the valve prosthesis. In case of balloon-expandable devices, under- or over-filling the delivery catheter balloon volume by a few milliliters with respect to manufacturer’s specifications is frequently used in current TAVI practice. Ex vivo bench studies have reported that over-expansion may be associated with reduced leaflet mobility and variable degrees of leaflet tear140. Sathananthan J, Sellers S, Barlow A, et al. Overexpansion of the SAPIEN 3 Transcatheter Heart Valve: An Ex Vivo Bench Study. JACC Cardiovasc Interv. 2018;11:1696-1705 Link, and that under-expansion may lead to a pinwheeling phenomenon, twisting of the free edges of the leaflets, resulting from excessive leaflet redundancy203. Hatoum H, Lilly S, Maureira P, Crestanello J, Dasi LP. The hemodynamics of transcatheter aortic valves in transcatheter aortic valves. J Thorac Cardiovasc Surg. 2021;161:565-576.e562e2 Link. A prospective study including 565 patients with post-TAVI MDCT reported that non-uniform expansion and under-expansion of TAVI prostheses may result in frame deformation, asymmetric leaflets, and smaller neosinus volume, which has been associated with hypoattenuated leaflet thickening (HALT)204. Fukui M, Bapat VN, Garcia S, et al. Deformation of Transcatheter Aortic Valve Prostheses: Implications for Hypoattenuating Leaflet Thickening and Clinical Outcomes. Circulation. 2022;146:480-493 Link. In a single-centre retrospective study, patients who received a suboptimally sized THV experienced an increased risk of all-cause and cardiovascular death at 1 year compared with those who received an optimally sized THV (adjusted HR 1.42, 95% CI 1.0-2.0, P = 0.047 and adjusted HR 1.59, 95% CI 1.06-2.39, P = 0.026, respectively)205. Okuno T, Heg D, Lanz J, et al. Heart valve sizing and clinical outcomes in patients undergoing transcatheter aortic valve implantation. Catheter Cardiovasc Interv. 2021;98:E768-e779E779 Link. A newer-generation balloon-expandable device (Myval) introduces a sizing strategy with 1.5 mm diameter increments between nominal device sizes, allowing for a more nuanced sizing strategy to match the aortic annulus compared to conventional devices with fixed 3.0 mm diameter increments. However, in the COMPARE TAVI 1 trial, Myval THV had a higher incidence of moderate or greater aortic regurgitation compared with SAPIEN THV72. Terkelsen CJ, Freeman P, JS Dahl, et al. SAPIEN 3 versus Myval transcatheter heart valves for transcatheter aortic valve implantation (COMPARE-TAVI 1): a multicentre, randomised, non-inferiority trial. Lancet. 2025;405:1362-1372. Link.
Transapical TAVI is performed via a left anterolateral intercostal incision followed by needle puncture of the apex through a pledgeted purse-string suture. A dedicated sheath is then placed and the THV is deployed in a similar manner to the transfemoral approach. This approach is typically used for the Edwards SAPIEN platform. Of note, this access site is associated with delayed recovery due to its invasiveness. In the PARTNER IA trial, the risk of all-cause mortality at 5 years was 79% in the transapical TAVI group versus 60% in the SAVR group (P = 0.067)57. Mack MJ, Leon MB, Smith CR, et al. 5-year outcomes of transcatheter aortic valve replacement or surgical aortic valve replacement for high surgical risk patients with aortic stenosis (PARTNER 1): a randomised controlled trial. Lancet. 2015;385:2477-2484 Link. Similarly, in the PARTNER II trial, transthoracic TAVI (including both transapical and transaortic) was associated with a higher rate of death or disabling stroke at 5 years compared with SAVR46. Makkar RR, Thourani VH, Mack MJ, et al. Five-Year Outcomes of Transcatheter or Surgical Aortic-Valve Replacement. N Engl J Med. 2020;382:799-809 Link.
Transaortic access
Transaortic access is performed through the ascending aorta via a right anterior mini-thoracotomy in the second intercostal space. The aorta is inspected to avoid areas of calcification. A purse-string suture is used to obtain a needle puncture and access with a dedicated sheath. The puncture is made with a minimum of 6 cm above the aortic annulus for the CoreValve platform and 8 cm for the SAPIEN platform. The valve is then deployed in the same manner as via the transfemoral approach206. Bapat V, Khawaja MZ, Attia R, et al. Transaortic Transcatheter Aortic valve implantation using Edwards Sapien valve: a novel approach. Catheter Cardiovasc Interv. 2012;79:733-740 Link.
Transsubclavian/axillary access
Transsubclavian/axillary approaches are the most commonly used alternative TAVI access sites in 2018 and 2019 in the STS/ACC TVT registry24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link. Transsubclavian access is typically performed via surgical cut-down, while trans-axillary can be performed percutaneously with pre-closure sutures most frequently into the proximal third of the axillary artery. There is no dedicated sheath available. A left-sided approach is preferred as it provides a more favourable alignment of the THV with the native valve. The presence of the left internal mammary artery graft in patients with coronary artery bypass surgery is considered a relative contraindication in the absence of native coronary artery flow to the left anterior descending artery or other territory that is supplied by the graft. In a retrospective analysis of the STS/ACC TVT registry, transsubclavian/axillary approach was used in 1,249 (34.4%) of 3,628 patients undergoing alternative access. After propensity-matching, trans-subclavian/axillary approach had lower 30-day mortality (5.3% vs. 8.4%, P<0.01), shorter lengths of intensive care unit and hospital stay, but a higher stroke rate (6.3% vs. 3.1%, P <0.05) compared with transthoracic approach207. Dahle TG, Kaneko T, McCabe JM. Outcomes Following Subclavian and Axillary Artery Access for Transcatheter Aortic Valve Replacement: Society of the Thoracic Surgeons/American College of Cardiology TVT Registry Report. JACC Cardiovasc Interv. 2019;12:662-669 Link.
Transcarotid access
Transcarotid access is performed percutaneously under local anaesthesia or via surgical cut-down and requires cerebral oximetry monitoring. Satisfactory vessel size and vessel quality are critical determinants for efficacy and safety as is an anatomically complete Circle of Willis. In a retrospective analysis of a multicentre registry including 329 alternative access TAVI patients (2012-2017), transcarotid TAVI was associated with less new-onset atrial fibrillation (3.2% vs. 19.0%, P = 0.002), acute kidney injury (0% vs. 12.1%, P = 0.002), and shorter median length of hospital stay (6 days vs. 8 days, P <0.001) compared with transthoracic TAVI after propensity-matching208. Chamandi C, Abi-Akar R, Rodes-Cabau J, et al. Transcarotid Compared With Other Alternative Access Routes for Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2018;11:e006388 Link.
Transcaval access
Transcaval access requires a dedicated pre-TAVI planning derived from the preprocedural MDCT. A calcium-free target on the right aortic wall that allows safe passage of the TAVI sheath from the inferior vena cava to the abdominal aorta needs to be identified. The trajectory of the sheath must be free of interposed obstacles (bowel), and the area of aortic entry should avoid important arterial branches, which allows for provisional covered stent bailout if needed. In brief, the femoral vein is accessed and a coronary guidewire (0.014 inch) connected to electrocautery is used to cross from the inferior vena cava into the abdominal aorta where it can be snared and advanced towards the aortic arch. The coronary guidewire is then exchanged for a stiff guidewire (0.035 inch). The TAVI sheath can be introduced via the stiff wire and the procedure can carry on as in the case of transfemoral TAVI. Once the THV has been deployed, a nitinol cardiac occluder (generally an Amplatzer Duct Occluder I) is used to seal the arteriotomy in the abdominal aorta209. Greenbaum AB, Babaliaros VC, Chen MY, et al. Transcaval Access and Closure for Transcatheter Aortic Valve Replacement: A Prospective Investigation. J Am Coll Cardiol. 2017;69:511-521 Link. In a multicentre European study, transcaval TAVI was successful in 49 out of 50 patients suggesting it to be feasible and safe for high-risk AS patients who are not suitable for transfemoral or transsubclavian/axillary access210. Costa G, De Backer O, Pilgrim T, et al. Feasibility and safety of transcaval transcatheter aortic valve implantation: a multicentre European registry. EuroIntervention. 2020;15:e1319-e1324 Link. These findings are supported by a recent meta-analysis from 8 studies with 467 patients undergoing transcaval TAVI211. Salihu A, Ferlay C, Kirsch M, et al. Outcomes and Safety of Transcaval Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-analysis. Can J Cardiol. 2024.;40:2054-2062 Link.
Procedural adverse events
Owing to improvements in TAVI technology and techniques, the rate of procedural complications has decreased over recent years, , 24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link212. Tomii D, Okuno T, Heg D, et al. Validation of the VARC-3 Technical Success Definition in Patients Undergoing TAVR. JACC Cardiovasc Interv. 2022;15:353-364 Link213. Sherwood MW, Xiang K, Matsouaka R, et al. Incidence, Temporal Trends, and Associated Outcomes of Vascular and Bleeding Complications in Patients Undergoing Transfemoral Transcatheter Aortic Valve Replacement: Insights From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapies Registry. Circ Cardiovasc Interv. 2020;13:e008227 Link. Notwithstanding, TAVI-related complications can occur in a non-negligible proportion of patients and may impact patient prognosis (Figure 26).
PVR occurs with incorrectly positioned THV implantation (too high or too low), undersized THV, or the presence of morphologic features that prevent ideal device apposition, such as asymmetric, protruding device landing zone calcification214. Buellesfeld L, Grube E. A permanent solution for a temporary problem: transcatheter valve-in-valve implantation for failed transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2012;5:578-581 Link. PVR is typically assessed by post-procedural aortic root angiography and/or transthoracic or transesophageal echocardiography. Since significant PVR is associated with an increased risk of adverse events after AVR, , , 214. Buellesfeld L, Grube E. A permanent solution for a temporary problem: transcatheter valve-in-valve implantation for failed transcatheter aortic valve replacement. JACC Cardiovasc Interv. 2012;5:578-581 Link215. Athappan G, Patvardhan E, Tuzcu EM, et al. Incidence, predictors, and outcomes of aortic regurgitation after transcatheter aortic valve replacement: meta-analysis and systematic review of literature. J Am Coll Cardiol. 2013;61:1585-1595 Link216. Van Belle E, Juthier F, Susen S, et al. Postprocedural aortic regurgitation in balloon-expandable and self-expandable transcatheter aortic valve replacement procedures: analysis of predictors and impact on long-term mortality: insights from the FRANCE2 Registry. Circulation. 2014;129:1415-1427 Link217. Pibarot P, Hahn RT, Weissman NJ, et al. Association of Paravalvular Regurgitation With 1-Year Outcomes After Transcatheter Aortic Valve Replacement With the SAPIEN 3 Valve. Jama. Cardiol 2017;2:1208-1216 Link, additional procedures should be considered if significant PVR is observed and the expected mechanism is addressable. If the leak is due to underexpansion of the THV, post-dilation should be performed to obtain optimal expansion. In case of THV malposition, a valve-in-valve procedure may be considered. In a multicenter study of 201 patients who underwent transcatheter intervention for the treatment of moderate or greater PVR after TAVI, PVR was successfully reduced to ≤mild in 82.6% of patients, and patients in whom ≤mild PVR was achieved had lower 1-year mortality than those with residual moderate or greater PVR (8.0% vs. 21.4%, P = 0.007)218. Landes U, Hochstadt A, Manevich L, et al. Treatment of late paravalvular regurgitation after transcatheter aortic valve implantation: prognostic implications. Eur Heart J. 2023;44:1331-1339 Link. Although the incidence of significant PVR has decreased, the incidence of mild PVR is still high compared with SAVR, , , , , , , , , 11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link12. Adams DH, Popma JJ, Reardon MJ, et al. Transcatheter aortic-valve replacement with a self-expanding prosthesis. N Engl J Med. 2014;370:1790-1798 Link13. Thyregod HG, Steinbrüchel DA, Ihlemann N, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Severe Aortic Valve Stenosis: 1-Year Results From the All-Comers NOTION Randomized Clinical Trial. J Am Coll Cardiol. 2015;65:2184-2194 Link11. Smith CR, Leon MB, Mack MJ, et al. Transcatheter versus surgical aortic-valve replacement in high-risk patients. N Engl J Med. 2011;364:2187-2198. Link15. Reardon MJ, Van Mieghem NM, Popma JJ, et al. Surgical or Transcatheter Aortic-Valve Replacement in Intermediate-Risk Patients. N Engl J Med. 2017;376:1321-1331 Link16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link17. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380:1706-1715 Link19. UK TAVI Trial Investigators; Toff WD, Hildick-Smith D, et al. Effect of Transcatheter Aortic Valve Implantation vs Surgical Aortic Valve Replacement on All-Cause Mortality in Patients With Aortic Stenosis: A Randomized Clinical Trial. JAMA. 2022;327:1875-1887. Link21. Blankenberg S, Seiffert M, Vonthein R, et al. Transcatheter or Surgical Treatment of Aortic-Valve Stenosis. N Engl J Med. 2024;390:1572-1583 Link22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link. In a single-center TAVI registry of 1,128 patients (568 with no/trace PVR and 560 with mild PVR), patients with mild PVR had a higher risk of mortality than those with none/trace PVR at 5 years (54.6% vs. 43.8%; adjusted HR: 1.26, 95% CI: 1.06-1.50). When applying the 5-class grading scheme, only mild-to-moderate PVR was associated with an increased risk of mortality at five years (mild PVR: adjusted HR: 1.19, 95% CI: 0.99-1.43, mild-to-moderate PVR: adjusted HR: 1.56, 95% CI: 1.20-2.02)219. Okuno T, Tomii D, Heg D, et al. Five-year outcomes of mild paravalvular regurgitation after transcatheter aortic valve implantation. EuroIntervention. 2022;18:33-42 Link.
Annular rupture
Aortic annular rupture is a rare (<1%) but life-threatening complication of TAVI requiring prompt rescue for haemodynamic stabilization. Annular rupture is more common with balloon-expandable THV or following aggressive pre/post balloon dilation of any valve type in the setting of a severely calcified valve with extension into the aortic root and LVOT, 121. Okuno T, Asami M, Heg D, et al. Impact of Left Ventricular Outflow Tract Calcification on Procedural Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2020;13:1789-1799 Link220. Tomii D, Pilgrim T, Okuno T, et al. Strategies for Treatment of Annular Rupture Complicating Transcatheter Aortic Valve Implantation: A Retrospective Analysis of the Bern TAVI Registry. Circ Cardiovasc Interv. 2023;16:e012796 Link. In general, annular rupture is detected by aortic root angiography and/or echocardiography with pericardial effusion. However, in some cases such as infra-annular injury, transesophageal echocardiography may be required for its detection. Furthermore, the clinical manifestations may vary depending on the location and extent of the injury. When rapid haemodynamic collapse occurs and is unexplained, the presence of annular rupture should be considered. Although conservative management (isolated pericardial drainage and/or optimization of the coagulation status) is selected in certain cases, surgical bailout is the default treatment strategy in patients with haemodynamic collapse. However, patients with annular rupture may not be stabilized to undergo surgical bailout in view of rapid clinical deterioration. Recently, rescue TAV-in-TAV has been suggested as rescue strategy to seal the site of annular rupture by increasing apposition of the first THV and extending the skirt-covered frame height by implantation of the second THV. This strategy could prevent further haemodynamic deterioration and may obviate the need for emergent sternotomy in suitable cases220. Tomii D, Pilgrim T, Okuno T, et al. Strategies for Treatment of Annular Rupture Complicating Transcatheter Aortic Valve Implantation: A Retrospective Analysis of the Bern TAVI Registry. Circ Cardiovasc Interv. 2023;16:e012796 Link.
Coronary artery obstruction
The mechanisms of TAVI-related coronary obstruction fall into two categories. Direct coronary obstruction occurs when the THV displaces the degenerated native or bioprosthetic valve leaflets toward the ostia of the coronary arteries; this typically occurs in patients with low coronary take-off combined with a shallow configuration of the sinus of Valsalva. Conversely, indirect coronary obstruction may occur in patients with a low and narrow sinotubular junction through the mechanism of sinus sequestration (Figure 27). This is a rare but a life-threatening complication of TAVI, , 221. Ribeiro HB, Webb JG, Makkar RR, et al. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. J Am Coll Cardiol. 2013;62:1552-1562 Link222. Ojeda S, Gonzalez-Manzanares R, Jimenez-Quevedo P, et al. Coronary Obstruction After Transcatheter Aortic Valve Replacement: Insights From the Spanish TAVI Registry. JACC Cardiovasc Interv. 2023;16:1208-1217 Link223. Jabbour RJ, Tanaka A, Finkelstein A, et al. Delayed Coronary Obstruction After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2018;71:1513-1524 Link. In the nationwide Spanish TAVI registry (13,675 patients between 2009-2021), the incidence of coronary obstruction was 0.68% for native TAVI and 5.7% for valve-in-valve TAVI. Among patients who developed coronary obstruction, rescue coronary revascularization was performed in 90.4% (PCI 86.9% and CABG 3.5%), and 22% of rescue PCI procedures were unsuccessful resulting in higher in-hospital mortality (patients without coronary obstruction: 4.1%; patients with coronary obstruction receiving successful revascularization: 20.7%; and patients with coronary obstruction receiving unsuccessful revascularization: 78.8%)222. Ojeda S, Gonzalez-Manzanares R, Jimenez-Quevedo P, et al. Coronary Obstruction After Transcatheter Aortic Valve Replacement: Insights From the Spanish TAVI Registry. JACC Cardiovasc Interv. 2023;16:1208-1217 Link. Of note, coronary obstruction can develop with delay after the index TAVI procedure with a similar clinical impact as acute obstruction223. Jabbour RJ, Tanaka A, Finkelstein A, et al. Delayed Coronary Obstruction After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2018;71:1513-1524 Link. Therefore, the risk of coronary obstruction must be taken into consideration during pre-procedural planning. Several anatomical risk factors for coronary obstruction have been identified, , 221. Ribeiro HB, Webb JG, Makkar RR, et al. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. J Am Coll Cardiol. 2013;62:1552-1562 Link223. Jabbour RJ, Tanaka A, Finkelstein A, et al. Delayed Coronary Obstruction After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2018;71:1513-1524 Link224. Khan JM, Kamioka N, Lisko JC, et al. Coronary Obstruction From TAVR in Native Aortic Stenosis: Development and Validation of Multivariate Prediction Model. JACC Cardiovasc Interv. 2023;16:415-425 Link. A preprocedural MDCT-based risk prediction model for direct coronary obstruction during native TAVI has been proposed using the data from the CO-TAVR and COBRA registries. This model includes cusp height > coronary artery height and virtual transcatheter valve-to-coronary-ostium (VTC) distance 4 mm or culprit leaflet calcium volume >600 mm3. Lieberman EB, Bashore TM, Hermiller JB, et al. Balloon aortic valvuloplasty in adults: failure of procedure to improve long-term survival. J Am Coll Cardiol. 1995;26:1522-1528 Link and shows a high predictive performance (area under the curve [AUC] of 0.93, a sensitivity of 0.93, and a specificity of 0.84 for the left coronary artery and with an AUC of 0.94, a sensitivity of 0.92, and a specificity of 0.96 for right coronary artery)224. Khan JM, Kamioka N, Lisko JC, et al. Coronary Obstruction From TAVR in Native Aortic Stenosis: Development and Validation of Multivariate Prediction Model. JACC Cardiovasc Interv. 2023;16:415-425 Link. Similarly, the VIVID registry documented that a shorter VTC distance predicted coronary obstruction and proposed a cutoff value of 4 mm in patients requiring a TAV-in-SAV procedure (AUC: 0.943)221. Ribeiro HB, Webb JG, Makkar RR, et al. Predictive factors, management, and clinical outcomes of coronary obstruction following transcatheter aortic valve implantation: insights from a large multicenter registry. J Am Coll Cardiol. 2013;62:1552-1562 Link. Additionally, in TAV-in-SAV patients, the risk of coronary obstruction is related to the surgical prosthesis type in place and considerably higher in stented prostheses with externally mounted leaflets or stentless prostheses than stented prostheses with internally mounted leaflets.
Figure 27
Mechanism of coronary obstruction complicating transcatheter aortic valve implantation. Figures reproduced from Pilgrim and Tomii. JACC Cardiovasc Interv 2023;16(4)426-428.
In patients deemed at high risk for coronary obstruction, coronary protection should be considered (Figure 28). Chimney stenting consists of placing guidewires and an undeployed balloon or stent in the coronary artery. If coronary occlusion is impending or occurs, the stent can be pulled back and deployed in a “chimney” fashion to maintain coronary patency225. Mercanti F, Rosseel L, Neylon A, et al. Chimney Stenting for Coronary Occlusion During TAVR: Insights From the Chimney Registry. JACC Cardiovasc Interv. 2020;13:751-761 Link. BASILICA (Bioprosthetic or native Aortic Scallop Intentional Laceration to Prevent Iatrogenic Coronary Artery Obstruction) is an alternative strategy to prevent coronary obstruction226. Khan JM, Greenbaum AB, Babaliaros VC, et al. The BASILICA Trial: Prospective Multicenter Investigation of Intentional Leaflet Laceration to Prevent TAVR Coronary Obstruction. JACC Cardiovasc Interv. 2019;12:1240-1252 Link. In brief, an electrified guidewire is used to lacerate the aortic valve leaflet that would otherwise obstruct the coronary ostium to preserve coronary inflow. Although the feasibility of the technique has been shown in several studies, the procedures are technically demanding and should be reserved to specialized centres. The ShortCut (Pi-Cardia, Rehovot, Israel) is the first dedicated transcatheter device designed to modify valve leaflets by mechanical splitting227. Dvir D, Leon MB, Abdel-Wahab M, et al. First-in-Human Dedicated Leaflet Splitting Device for Prevention of Coronary Obstruction in Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2023;16:94-102 Link. Briefly, the procedure is performed under general anaesthesia using guidance by transoesophageal echocardiography. The device is introduced under fluoroscopic guidance over a standard 0.035-inch guidewire. After crossing the aortic valve, the device is unsheathed to automatically open the positioning arm above the aortic valve. A deflection mechanism allows the device to centre in the valve. Predefined fluoroscopic views are then used to rotate and advance the positioning arm to accurately split the target leaflet at the base. After confirming positioning arm location, the splitting element is activated to puncture the leaflet base from the ventricular aspect. The catheter is then gently retracted, performing a vertical split of the leaflet upward from base to tip. If required, the positioning arm is then rotated towards a second target leaflet and the splitting procedure is repeated (dual split). Afterwards, the ShortCut device is removed, and TAVI is performed using the same guidewire. In the prospective Shortcut study, 60 patients with failed bioprosthetic aortic valves who were at high risk for coronary obstruction after TAVI underwent leaflet modifications using the ShortCut device. The primary efficacy endpoint was the per-patient leaflet splitting success and was achieved in all patients. The primary safety endpoint of procedure-related mortality or stroke at discharge or 7 days was achieved in 98.3% of patients. At 30 days, freedom from coronary obstruction was 95%228. Dvir D, Tchetche D, Leon MB, et al. Leaflet modification before transcatheter aortic valve implantation in patients at risk for coronary obstruction: the ShortCut study. Eur Heart J. 2024;45:3031-3041 Link. The use of cerebral embolic protection devices is frequent in TAVI procedures involving leaflet modification techniques due to the nature and complexity of such interventions.
Figure 28
Coronary protection techniques. Figures reproduced and modified from Khan et al. JACC Cardiovasc Interv 2018;11(7):677-689, Mercanti et al. JACC Cardiovasc Interv 2020;13(6):751-761, and Dvir et al. JACC Cardiovasc Interv 2023;16(1):94-102; and Prendergast et al. Eur Heart J 2024;45:3042-3044.
Valve dislocation/embolization occurs in <1% and is accentuated in case of non-calcified native aortic valve leaflets, eccentric and asymmetric calcifications, pre-existing AR, and acute aortic angulation. Valve dislocations are either towards the aorta or into the LV cavity. Although it usually occurs immediately during or after THV implantation, late device migration (up to 1 year after TAVI) has been reported229. Nkomo VT, Suri RM, Pislaru SV, et al. Delayed transcatheter heart valve migration and failure. JACC Cardiovasc Imaging. 2014;7:960-962 Link. In an international retrospective registry, valve dislocation/embolization occurred in 273 out of 29,636 patients (0.92%), of which 217 (79.5%) were into the aorta and 56 (20.5%) into the left ventricle. Bailout measures included repositioning attempts using snares or miscellaneous tools, multiple valve implantation (83.2%), and conversion to surgery (19.0%). Of note, successful reposition was achieved in only 51.8% of cases. In a 1:4 propensity score matching analysis, valve dislocation/embolization was associated with an increased risk of stroke at 30 days (10.6% vs. 2.8%, P <0.001) and mortality at 30 days (18.6% vs. 4.9%, P <0.001) and at 1 year (30.5% vs. 16.6%, P <0.001)230. Kim WK, Schafer U, Tchetche D, et al. Incidence and outcome of peri-procedural transcatheter heart valve embolization and migration: the TRAVEL registry (TranscatheteR HeArt Valve EmboLization and Migration). Eur Heart J. 2019;40:3156-3165 Link.
Atrioventricular conduction disturbance and new-onset atrial fibrillation
New conduction disturbances, including LBBB and high-degree atrioventricular block, requiring new permanent pacemaker implantation, are common adverse events in patients undergoing TAVI. In RCTs, the incidence of new permanent pacemaker implantation and LBBB was higher in patients undergoing TAVI than in those undergoing SAVR, and the development of conduction disturbances is usually more frequent among self-expanding TAVI devices18. Siontis GCM, Overtchouk P, Cahill TJ, et al. Transcatheter aortic valve implantation vs surgical aortic valve replacement for treatment of symptomatic severe aortic stenosis: an updated meta-analysis. Eur Heart J. 2019;40:3143-3153 Link. The development of new conduction disturbances usually occurs within 24 hours, while it may be observed later than 48 hours after TAVI or even after discharge. Pre-existing right bundle branch block, short membranous septum length, non-coronary cusp device landing zone calcification, and deep implantation of the THV have been identified as independent predictors of new conduction disturbances231. Maeno Y, Abramowitz Y, Kawamori H, et al. A Highly Predictive Risk Model for Pacemaker Implantation After TAVR. JACC: Cardiovascular Imaging. 2017;10:1139-1147 Link.
New-onset atrial fibrillation is another common rhythm disorder after TAVI. A combination of inflammation, atrial oxidative stress, and increased sympathetic drive may be causal in the development of atrial fibrillation. A recent meta-analysis of 179 studies with 241,712 patients reported that one in ten patients developed new-onset atrial fibrillation after TAVI232. Ryan T, Grindal A, Jinah R, et al. New-Onset Atrial Fibrillation After Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis. JACC Cardiovasc Interv. 2022;15:603-613 Link.
Both rhythm disorders can affect cardiac anatomical and functional remodeling, potentially impacting prognosis. Conduction disturbances may lead to left ventricular dyssynchrony leading to impaired left ventricular function, lead-induced tricuspid regurgitation, and other pacing lead adverse events (fracture and endocarditis) during long-term follow-up233. Glikson M, Nielsen JC, Kronborg MB, et al. 2021 ESC Guidelines on cardiac pacing and cardiac resynchronization therapy. Eur Heart J. 2021;42:3427-3520 Link. New-onset atrial fibrillation is associated with an increased risk of mortality, stroke, major or life-threatening bleeding, and new permanent pacemaker implantation, , 232. Ryan T, Grindal A, Jinah R, et al. New-Onset Atrial Fibrillation After Transcatheter Aortic Valve Replacement: A Systematic Review and Meta-Analysis. JACC Cardiovasc Interv. 2022;15:603-613 Link234. Mentias A, Saad M, Girotra S, et al. Impact of Pre-Existing and New-Onset Atrial Fibrillation on Outcomes After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2019;12:2119-2129 Link235. Brener MI, George I, Kosmidou I, et al. Atrial Fibrillation Is Associated With Mortality in Intermediate Surgical Risk Patients With Severe Aortic Stenosis: Analyses From the PARTNER 2A and PARTNER S3i Trials. J Am Heart Assoc. 2021;10:e019584 Link. Therefore, continued monitoring by telemetry and potential risk assessment is a key to detect the rhythm disorders, , 236. Rodés-Cabau J, Ellenbogen KA, Krahn AD, et al. Management of Conduction Disturbances Associated With Transcatheter Aortic Valve Replacement: JACC Scientific Expert Panel. J Am Coll Cardiol. 2019;74:1086-1106 Link237. Lilly SM, Deshmukh AJ, Epstein AE, et al. 2020 ACC Expert Consensus Decision Pathway on Management of Conduction Disturbances in Patients Undergoing Transcatheter Aortic Valve Replacement: A Report of the American College of Cardiology Solution Set Oversight Committee. J Am Coll Cardiol. 2020;76:2391-2411 Link238. Malebranche D, Bartkowiak J, Ryffel C, et al. Validation of the 2019 Expert Consensus Algorithm for the Management of Conduction Disturbances After TAVR. JACC Cardiovasc Interv. 2021;14:981-991 Link, particularly in younger patients with longer life-expectancy.
The Co-STAR (Colchicine for Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement [NCT04870424]) trial evaluated the efficacy of colchicine to reduce the risk of new-onset arrhythmias after TAVI. In this trial, 120 patients with severe AS undergoing TAVI were randomly allocated in a 1:1 ratio to treatment with colchicine (0.5 mg once daily) or placebo for the duration of 14 days starting the day before TAVI. At 30 days, the primary composite endpoint of new-onset atrial fibrillation or atrioventricular conduction disturbances requiring new permanent pacemaker implantation occurred in 6 patients (10%) in the colchicine group and in 15 patients (25%) in the placebo group (risk difference -15%, 95% CI -23.3 to -1.7, P = 0.031), while there was no significant difference in the incidence of the components between groups. Of note, this trial was prematurely terminated following the recommendation of the Data Safety Monitoring Board after review of the pre-specified interim analysis after complete follow-up of 120 patients, and the the primary outcome event rates were lower than expected. Further studies are warranted to corroborate the effect of anti-inflammatory treatment on the incidence of arrhythmias after TAVI239. Pilgrim T. Colchicine in Patients With Aortic Stenosis Undergoing Transcatheter Aortic Valve Replacement: A Double-Blind Randomized Controlled Trial. In: TCT. Washington, DC, 2024 Link.
Vascular complications
Vascular complications typically include dissection, stenosis, perforation, and pseudoaneurysm or aneurysm. Although the incidence has decreased over time (1.5% to 4% in the recent low-risk trials) due to smaller and more flexible delivery systems and increasing operator experience, major vascular complications are still common and associated with increased morbidity and mortality, , , 16. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement with a Balloon-Expandable Valve in Low-Risk Patients. N Engl J Med. 2019;380:1695-1705 Link17. Popma JJ, Deeb GM, Yakubov SJ, et al. Transcatheter Aortic-Valve Replacement with a Self-Expanding Valve in Low-Risk Patients. N Engl J Med. 2019;380:1706-1715 Link22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link240. Piccolo R, Pilgrim T, Franzone A, et al. Frequency, Timing, and Impact of Access-Site and Non-Access-Site Bleeding on Mortality Among Patients Undergoing Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2017;10:1436-1446 Link. The most frequent cause is closure device failure leading to continued bleeding, stenosis or vessel closure. In addition to the accurate risk assessment during the preprocedural period, familiarity with closure devices and bailout strategies for iliofemoral vascular complications can mitigate the negative impact of vascular complications. Recently, the TAVI-MultiCLOSE study demonstrated the safety and efficacy of a novel algorithm for percutaneous closure of large-bore arterial access241. Rosseel L, Montarello NJ, Nuyens P, et al. A systematic algorithm for large-bore arterial access closure after TAVI: the TAVI-MultiCLOSE study. EuroIntervention. 2024;20:e354-e362. Link. This algorithm includes the reinsertion of a 4-8 Fr sheath following an initial closure with one or two suture-based vascular closure devices, which provides the opportunity to perform an angiographic control and tailor the final vascular closure with either an additional suture- or plug-based vascular closure device, or neither of these. In this study, the reported incidence of minor and major vascular complication with the consecutive use of this algorithm was 2.2% and 0.6%, respectively241. Rosseel L, Montarello NJ, Nuyens P, et al. A systematic algorithm for large-bore arterial access closure after TAVI: the TAVI-MultiCLOSE study. EuroIntervention. 2024;20:e354-e362. Link.
Stroke
Stroke remains one of the most feared complications of TAVI and is associated with significant morbidity and mortality. TAVI-related stroke can be differentiated by aetiology and timing, 242. Stortecky S, Windecker S. Stroke: an infrequent but devastating complication in cardiovascular interventions. Circulation. 2012;126:2921-2924 Link243. Windecker S, Franzone A, Pilgrim T. Deciphering the Unknowns of Stroke After Aortic Valve Interventions. J Am Coll Cardiol. 2018;72:2427-2430 Link. Acute stroke, the most common type of TAVI-related stroke, occurs during or within 24 hours of the procedure and is related to dislodged atheroma and aortic valve debris. After the acute phase, new-onset atrial fibrillation and bioprosthetic thrombosis may increase the risk of subacute (24 hours to 30 days) and early (>30 days to 1 year) stroke. In the late period (>1 year after TAVI), the risk of stroke is dominated by atherosclerotic burden rather than procedural features, and the incidence of late stroke in the TAVI population is comparable to that in the general population244. Okuno T, Alaour B, Heg D, et al. Long-Term Risk of Stroke After Transcatheter Aortic Valve Replacement: Insights From the SwissTAVI Registry. JACC Cardiovasc Interv. 2023;16:2986-2996 Link. Although there is no robust evidence that cerebral embolic protection devices prevent cerebrovascular events during the procedure, their use may be considered in patients with high-risk TAVI, such as calcified aortic valve and valve-in-valve TAVI with leaflet modification techniques (BASILICA and ShortCut). In addition, optimal anticoagulation during and after the procedure is essential to prevent stroke. Once neurological events are suspected, patients should be promptly evaluated by a neurologist and undergo diagnostic imaging whenever indicated. Neurointervention, including mechanical thrombectomy and thrombolytic therapy may be required245. Levi A, Linder M, Seiffert M, et al. Management and Outcome of Acute Ischemic Stroke Complicating Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2022;15:1808-1819 Link.
Patient management after TAVI
Antithrombotic management after TAVI
Patients undergoing TAVI are predominantly elderly and feature both thromboembolic and bleeding risks. Optimal antithrombotic therapy after TAVI has been debated for the past decade (Table 14). In patients with no indication for anticoagulation therapy, lifelong single antiplatelet therapy (SAPT) is the standard treatment recommendation, as dual antiplatelet therapy (DAPT) is associated with an increased risk of bleeding complications without benefit in terms of thromboembolic event protection, , , 246. Ussia GP, Scarabelli M, Mulè M, et al. Dual antiplatelet therapy versus aspirin alone in patients undergoing transcatheter aortic valve implantation. Am J Cardiol. 2011;108:1772-1776 Link247. Stabile E, Pucciarelli A, Cota L, et al. SAT-TAVI (single antiplatelet therapy for TAVI) study: a pilot randomized study comparing double to single antiplatelet therapy for transcatheter aortic valve implantation. Int J Cardiol. 2014;174:624-627 Link248. Rodés-Cabau J, Masson JB, Welsh RC, et al. Aspirin Versus Aspirin Plus Clopidogrel as Antithrombotic Treatment Following Transcatheter Aortic Valve Replacement With a Balloon-Expandable Valve: The ARTE (Aspirin Versus Aspirin + Clopidogrel Following Transcatheter Aortic Valve Implantation) Randomized Clinical Trial. JACC Cardiovasc Interv. 2017;10:1357-1365 Link249. Brouwer J, Nijenhuis VJ, Delewi R, et al. Aspirin with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;383:1447-1457 Link.
Table 14. Randomized clinical trials on antithrombotic therapy after TAVI.
Trial
First author
Strategy
Population
Primary end point
Period
Main Result
No indication for anticoagulant therapy
Antiplatelet therapy
Ussia et al. (2011)
3 mo DAPT (clopidogrel + aspirin) vs. SAPT (aspirin)
79 patients without underlying indication for OAC or recent stent implantation
Composite of death, MI, major stroke, life-threatening or major bleeding, or urgent conversion to surgery
6 mo
No significant difference for SAPT vs. DAPT (15% vs. 18% respectively; P = 0.85)
SAT-TAVI Stabile et al. (2014)
6 mo DAPT (clopidogrel or ticlopidine + aspirin) vs. SAPT (aspirin)
120 patients without underlying indication for OAC or recent stent implantation
VARC-2 safety end points
30 d
No difference on the primary endpoint. Composite of major and minor vascular complication more frequent with DAPT (13.3% vs. 5%; P<0.05)
ARTE Rodés-Cabau et al. (2017)
3 mo DAPT (clopidogrel + aspirin or acetylsalicylic acid) vs. SAPT (aspirin or acetylsalicylic acid)
222 patients without underlying indication for OAC or recent stent implantation
Composite of death, MI, stroke or TIA, or life-threatening or major bleeding
3 mo
15.3% vs. 7.2% for DAPT and SAPT respectively (OR 2.31, 95% CI 0.95 to 5.62, P = 0.065)
POPular TAVI cohort A Brouwer et al. (2020)
SAPT (aspirin) vs. 3 mo DAPT (aspirin + clopidogrel)
665 patients without an indication for long-term anticoagulation
The two primary end point were all bleeding and non–procedure-related bleeding
12 mo
Both all bleeding and non-procedure bleeding more frequent with DAPT (26.6% vs. 15.1%; P = 0.001, 24.9% vs. 15.1%; P = 0.005, respectively). The composite of bleeding or thromboembolic events were significantly less frequent with SAPT
Oral anticoagulation
GALILEO Dangas et al. (2020)
Rivaroxaban group (rivaroxaban + 3 mo aspirin vs. Antiplatelet group (aspirin + 3 mo clopidogrel)
1,644 patients without indication for long-term OAC
Composite of death or thromboembolic events.
24 mo
Rivaroxaban group had higher rates of death or thromboembolic events (HR 1.35, 95% CI 1.01 to 1.81; P = 0.04)
Major, disabling, or life-threatening bleeding
Rivaroxaban group hadhigher rates of bleeding event (HR 1.50, 95% CI 0.95 to 2.37, P = 0.08)
Low Risk Trial 2.0 Rogers et al. (2021)
Warfarin + Aspirin for 30 days vs. Aspirin
94 patients without indication for OAC
Composite of HALT, at least moderate RLM, haemodynamic dysfunction (mean aortic valve gradient ≥20 mmHg, effective orifice area ≤1.0 cm2, dimensionless valve index <0.35, or moderate or severe aortic regurgitation), stroke, or TIA
30 days
7.0% vs. 26.5% for Warfarin + Aspirin and Aspirin alone, respectively (OR 4.8, 95% CI 1.3 to 18.3, P = 0.014)
ATLANTIS stratum 2 Collet et al. (2022)
Apixaban vs. SAPT or DAPT for 12 mo
1049 without indication for long-term OAC
Composite of death, MI, stroke or TIA, systemic embolism, intracardiac or bioprosthesis thrombosis, DVT or PE and life-threatening, disabling, or major bleeding
12 mo
16.9% vs. 19.3% (HR 0.88, 95% CI 0.66 to 1.17)
Major, disabling, or life-threatening bleeding
7.8% vs. 7.3% (HR 1.09, 95% CI 0.70 to 1.69)
ADAPT-TAVR Park et al. (2022)
Edoxaban vs. DAPT
229 patients without indication for long-term OAC
Leaflet thrombosis on 4-dimensional computed tomography
6 mo
9.8% vs. 18.4% (absolute difference −8.5%; 95% CI −17.8% to 0.8%; P = 0.076)
Indication for anticoagulant therapy
POPular TAVI cohort B Nijenhuis et al. (2020)
OAC vs. OAC + 3 mo clopidogrel
326 patients with indication for long-term OAC
All bleeding and non–procedure-related bleeding
12 mo
Both all bleeding and non-procedure bleeding more frequent with OAC with clopidogrel (34.6% vs. 21.7%; P = 0.01, 34.0% vs. 21.7%, P = 0.02, respectively)
OAC alone was non-inferior in terms of the thromboembolic composite endpoint of cardiovascular death, ischemic stroke, or myocardial infarction (13.4% vs. 17.3%, difference -3.9 percentage points, 95% CI for non-inferiority -11.9 to 4.0)
ENVISAGE-TAVI AF Van Mieghem et al. (2021)
Edoxaban vs. Vitamin K antagonist
1426 patients with indication for long-term OAC
Death, MI, stroke, systemic thromboembolic event valve thrombosis, or major bleeding
Median 554 and 530 days
17.3 per 100 person-years vs. 16.5 per 100 person-years (HR 1.05, 95% CI 0.85 to 1.31)
Major bleeding
9.7 per 100 person-years vs. 7.0 per 100 person-years (HR 1.40, 95% CI 1.03 to 1.91)
ATLANTIS stratum 1 Collet et al. (2022)
Apixaban vs. Vitamin K antagonist
451 patients with indication for long-term OAC
Composite of death, MI, stroke or TIA, systemic embolism, intracardiac or bioprosthesis thrombosis, DVT or PE, and life-threatening, disabling, or major bleeding
12 mo
22% vs. 21.9% (HR 1.02, 95% CI 0.69 to 1.51)
Major, disabling, or life-threatening bleeding
10.3% vs. 11.4% (HR 0.91, 95% CI 0.52 to 1.60)
CI = confidence interval; DAPT = dual antiplatelet therapy; DVT = deep vein thrombosis; HALT = hypoattenuated leaflet thickening; HR = hazard ratio; MI = myocardial infarction; OAC = oral anticoagulation; OR = odds ratio; PE = pulmonary embolism; RLM = reduced leaflet motion; SAPT = single antiplatelet therapy; TIA = transient ischemic attack ; VARC =valve academic research criteria.
Therefore, temporal DAPT is considered only in patients at low risk of bleeding or in those with recent coronary stenting (Table 15), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link.
Table 15. Guideline recommendations: Antithrombotic therapy after TAVI.
2020 AHA/ACC Valvular Heart Disease Guideline
2021 ESC/EACTS Valvular Heart Disease Guideline
Recommendations
COR
LOE
Recommendations
COR
LOE
No indication for oral anticoagulant
Single antiplatelet therapy with aspirin (75-100mg daily).
2a
B-R
Lifelong single antiplatelet therapy.
I
A
For patients at low risk of bleeding, DAPT (aspirin and clopidogrel) may be reasonable for 3-6 months after TAVI.
2b
B-NR
If recent coronary stenting (<3 months), consider DAPT (aspirin and clopidogrel) for 1-6 months, and then single antiplatelet therapy (aspirin or clopidogrel) lifelong.
NA
For patients at low risk of bleeding, OAC with VKA may be reasonable for at least 3 months after TAVI.
2b
B-NR
Routine use OAC is not recommended after TAVI.
III
B
Concomitant indication for oral anticoagulant
No recommendation made in ACC/AHA guidelines.
Lifelong OAC therapy.
I
B
If recent coronary stenting (<3 months) continue OAC lifelong and consider a single antiplatelet drug (aspirin or clopidogrel) for 1-6 months.
NA
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; COR = class of recommendation; DAPT = dual antiplatelet therapy; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; OAC = Oral anticoagulant; TAVI = transcatheter aortic valve implantation; VKA = vitamin K antagonist.
If there is an established indication for DAPT, the antithrombotic management should follow the recommendations for this indication. The NAPT (Non-antithrombotic Therapy After Transcatheter Aortic Valve Implantation [NCT06007222]) trial is currently underway to evaluate the feasibility of no antiplatelet therapy after successful TAVI in patients without an indication for OAC and an indication for antiplatelet therapy other than TAVI. Of note, the study duration will limit mid-term follow-up (up to 3 years) and assessment of valve function, including the presence of subclinical valve thrombosis, is only planned at 6 months and 1 year250. Inohara T, Otsuka T, Watanabe Y, et al. Rationale and design of Non-antithrombotic Therapy After Transcatheter Aortic Valve Implantation (NAPT) Trial. Contemp Clin Trials. 2023;134:107358. Link.
Patients with THV have a lifelong risk for bioprosthetic thrombosis. Subclinical leaflet thrombosis after TAVI, which can manifest as HALT and/or reduced leaflet motion (RLM) has been the focus of intense clinical research251. Makkar RR, Fontana G, Jilaihawi H, et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med. 2015;373:2015-2024 Link. Although there are conflicting data regarding the incidence, natural history, and clinical impact of subclinical leaflet thrombosis, the prevention of subclinical leaflet thrombosis has been emphasized as it may impact bioprosthetic durability and the risk of stroke, , , , , , , , 251. Makkar RR, Fontana G, Jilaihawi H, et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N Engl J Med. 2015;373:2015-2024 Link252. Jilaihawi H, Asch FM, Manasse E, et al. Systematic CT Methodology for the Evaluation of Subclinical Leaflet Thrombosis. JACC Cardiovasc Imaging. 2017;10:461-470 Link253. Sondergaard L, De Backer O, Kofoed KF, et al. Natural history of subclinical leaflet thrombosis affecting motion in bioprosthetic aortic valves. Eur Heart J. 2017;38:2201-2207 Link254. Blanke P, Leipsic JA, Popma JJ, et al. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75:2430-2442 Link255. Makkar RR, Blanke P, Leipsic J, et al. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75:3003-3015 Link256. Garcia S, Fukui M, Dworak MW, et al. Clinical Impact of Hypoattenuating Leaflet Thickening After Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2022;15:e011480 Link257. Hein M, Schoechlin S, Schulz U, et al. Long-Term Follow-Up of Hypoattenuated Leaflet Thickening After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2022;15:1113-1122 Link258. Choi Y, Ahn JM, Kang DY, et al. Frequency, Predictors, and Clinical Impact of Valvular and Perivalvular Thrombus After Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2023;16:2967-2981 Link259. Waksman R, Bhogal S, Gordon P, et al. Transcatheter Aortic Valve Replacement and Impact of Subclinical Leaflet Thrombosis in Low-Risk Patients: LRT Trial 4-Year Outcomes. Circ Cardiovasc Interv. 2023;16:e012655 Link. Several studies have reported that OAC is associated with a reduced risk of subclinical leaflet thrombosis, , 260. De Backer O, Dangas GD, Jilaihawi H, et al. Reduced Leaflet Motion after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382:130-139 Link261. Montalescot G, Redheuil A, Vincent F, et al. Apixaban and Valve Thrombosis After Transcatheter Aortic Valve Replacement: The ATLANTIS-4D-CT Randomized Clinical Trial Substudy. JACC Cardiovasc Interv. 2022;15:1794-1804 Link262. Park DW, Ahn JM, Kang DY, et al. Edoxaban Versus Dual Antiplatelet Therapy for Leaflet Thrombosis and Cerebral Thromboembolism After TAVR: The ADAPT-TAVR Randomized Clinical Trial. Circulation. 2022;146:466-479 Link. In the CT substudy of the GALILEO trial, rivaroxaban added to aspirin was associated with a lower incidence of RLM grade ≥3 and leaflet thickening at 90-day CT follow-up compared with clopidogrel plus aspirin (2.1% vs. 10.9%, P = 0.01, and 12.4% vs. 32.4%)260. De Backer O, Dangas GD, Jilaihawi H, et al. Reduced Leaflet Motion after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382:130-139 Link. Similarly, a CT-substudy of the ATLANTIS trial reported that apixaban reduced the risk of subclinical obstructive valve thrombosis (defined as ≥1 prosthetic valve leaflet with grade 3 or 4 RLM or grade 3 or 4 HALT) compared with antiplatelet therapy (odds ratio: 0.51, 95% CI 0.30-0.86) but not compared with vitamin K antagonists (VKAs) (odds ratio: 1.80; 95% CI: 0.62-5.25)261. Montalescot G, Redheuil A, Vincent F, et al. Apixaban and Valve Thrombosis After Transcatheter Aortic Valve Replacement: The ATLANTIS-4D-CT Randomized Clinical Trial Substudy. JACC Cardiovasc Interv. 2022;15:1794-1804 Link. However, RCTs comparing OAC with antiplatelet therapy have consistently shown that OAC is associated with an increased risk of bleeding and death compared with antiplatelet therapy, 263. Dangas GD, Tijssen JGP, Wöhrle J, et al. A Controlled Trial of Rivaroxaban after Transcatheter Aortic-Valve Replacement. N Engl J Med. 2020;382:120-129 Link264. Collet JP, Van Belle E, Thiele H, et al. Apixaban vs standard of care after transcatheter aortic valve implantation: the ATLANTIS trial. Eur Heart J. 2022;43:2783-2797 Link. Therefore, current ESC/EACTS guidelines do not recommend routine use of OAC in patients with no indication for OAC (Class III) (Table 15)40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link.
In patients with an established indication for OAC, OAC should be continued after TAVI and additional antiplatelet therapy is generally not recommended. In the POPular TAVI trial cohort B, the addition of clopidogrel to OAC was associated with an increased risk of both all bleeding and non-procedure bleeding (34.6% vs. 21.7%; P = 0.01, 34.0% vs. 21.7%; P = 0.02, respectively), and OAC alone was non-inferior with respect to the thromboembolic composite endpoint of cardiovascular death, ischemic stroke, or myocardial infarction (13.4% vs. 17.3%, difference -3.9 percentage points, 95% CI for non-inferiority -11.9 to 4.0)265. Nijenhuis VJ, Brouwer J, Delewi R, et al. Anticoagulation with or without Clopidogrel after Transcatheter Aortic-Valve Implantation. N Engl J Med. 2020;382:1696-1707 Link. Whether these patients should be treated with DOACs or VKA remains a subject of debate. In the ENVISAGE-TAVI AF trial, edoxaban was non-inferior to VKAs in terms of the primary efficacy composite outcome of death from any cause, myocardial infarction, ischemic stroke, systemic thromboembolism, valve thrombosis, or major bleeding (HR 1.05; 95% CI 0.85-1.31, Pnon-inferiority = 0.01). However, the primary safety endpoint of major bleeding occurred more frequently in the edoxaban group compared with VKA (HR 1.40, 95% CI 1.03-1.91)266. Van Mieghem NM, Unverdorben M, Hengstenberg C, et al. Edoxaban versus Vitamin K Antagonist for Atrial Fibrillation after TAVR. N Engl J Med. 2021;385:2150-2160 Link. Similarly, the ATLANTIS trial Stratum 1 reported no difference in the primary composite endpoint of death, myocardial infarction, stroke or transient ischaemic attack, systemic embolism, intracardiac or bioprosthesis thrombosis, deep vein thrombosis or pulmonary embolism, and life-threatening, disabling, or major bleeding at 1 year and in the primary safety endpoint of major, disabling, or life-threatening bleeding (HR 0.91; 95% CI 0.52-1.60) between patients treated with apixaban and those receiving VKA264. Collet JP, Van Belle E, Thiele H, et al. Apixaban vs standard of care after transcatheter aortic valve implantation: the ATLANTIS trial. Eur Heart J. 2022;43:2783-2797 Link.
Bioprosthetic valve dysfunction
Structural valve deterioration and bioprosthetic valve failure
Data on the durability of THV have been reported from the randomized clinical trials and large scale real-world registries. However, the durability data for THV are currently limited to 10-year follow-up and are mainly derived from elderly populations, , , , 53. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement in Low-Risk Patients at Five Years. N Engl J Med. 2023;389:1949-1960 Link54. Thyregod HGH, Jorgensen TH, Ihlemann N, et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. Eur Heart J. 2024;45:1116-1124 Link267. O'Hair D, Yakubov SJ, Grubb KJ, et al. Structural Valve Deterioration After Self-Expanding Transcatheter or Surgical Aortic Valve Implantation in Patients at Intermediate or High Risk. JAMA Cardiol 2023;8:111-119. doi: 10.1001/jamacardio.2022.4627 Link268. Pibarot P, Herrmann HC, Wu C, et al. Standardized Definitions for Bioprosthetic Valve Dysfunction Following Aortic or Mitral Valve Replacement: JACC State-of-the-Art Review. J Am Coll Cardiol. 2022;80:545-561 Link269. Yakubov SJ, Van Mieghem NM, Oh JK, et al. Impact of Transcatheter or Surgical Aortic Valve Performance on 5-Year Outcomes in Patients at ≥ Intermediate Risk. J Am Coll Cardiol. 2025;85:1419-1430. Link. Among surgical studies monitoring durability, structural valve deterioration (SVD) has mainly occurred more than 10 years after implantation although these studies used clinical rather than echocardiographic follow-up (Figure 29). The available evidence on the durability of THV is somewhat confounded due to varying definitions and surrogates of BVD, and a substantial competitive risk of death especially in the cohorts of early TAVI trials and registries, which has variably been accounted for in previous studies. The definition of SVD and BVD has changed over time to incorporate the underlying pathology, haemodynamic significance, and clinical sequelae. Several pathologies can lead to BVD, which have been clustered into SVD and non-SVD etiologies, in addition to two additional entities including thrombosis and endocarditis according to the European Association of Percutaneous Cardiovascular Interventions (EAPCI) and the VARC definitions, 270. Capodanno D, Petronio AS, Prendergast B, et al. Standardized definitions of structural deterioration and valve failure in assessing long-term durability of transcatheter and surgical aortic bioprosthetic valves: a consensus statement from the European Association of Percutaneous Cardiovascular Interventions (EAPCI) endorsed by the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2017;38:3382-3390 Link271. VARC-3 WRITING COMMITTEE; Genereux P, Piazza N, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J 2021;42:1825-1857. doi: 10.1093/eurheartj/ehaa799 Link. The key difference between the definitions is the need for haemodynamic criteria for the assessment of BVD severity. VARC-3 stratifies BVD according to the haemodynamic significance into morphological (without significant haemodynamic valve deterioration), and haemodynamically significant valve deterioration: moderate (Stage 2) and severe (Stage 3) HVD. Contrary to previous definitions, VARC-3 incorporates temporal dynamic changes of the echocardiographic haemodynamic parameters of the aortic valve prosthesis rather than using fixed reference values as diagnostic cut-off thresholds for HVD. Furthermore, the VARC-3 definition considers three stages of BVF: Stage 1 includes any BVD with clinically expressive criteria such as new-onset or worsening symptoms, left ventricular dilatation/hypertrophy/dysfunction, or pulmonary hypertension, or irreversible Stage 3 HVD; Stage 2 includes aortic valve reintervention; and Stage 3 includes valve-related death (Table 16)271. VARC-3 WRITING COMMITTEE; Genereux P, Piazza N, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J 2021;42:1825-1857. doi: 10.1093/eurheartj/ehaa799 Link.
Figure 29
Valve durability according to the type of surgical bioprosthesis. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Table 16. Definitions of structural valve deterioration and bioprosthetic valve failure.
ESC/EAPCI/EACTS
VARC-3
Structural valve deterioration (SVD)
Any of following:
Leaflet integrity abnormality (i.e. torn or flail causing intra-frame regurgitation);
Leaflet structure abnormality(i.e. pathological thickening and/or calcification causing valvular stenosis or central regurgitation);
Leaflet function abnormality (i.e. impaired mobility resulting in stenosis and/or central regurgitation);
Strut/frame abnormality (i.e. fracture)
Morphological SVD
Morphological valve deterioration
Intrinsic permanent changes to the prosthetic valve, including leaflet tear, disruption, flail leaflet, leaflet fibrosis and/or calcification without significant haemodynamic changes.
Any of following:
Mean transprosthetic gradient ≥20mmHg and <40 mmHg;
Mean transprosthetic gradient ≥10 and <20 mmHg change from baseline;
Moderate intra-prosthetic aortic regurgitation, new or worsening (>1+/4+) from baseline
Moderate haemodynamic SVD
Moderate haemodynamic valve deterioration
Morphological valve deterioration AND: Increase in mean transvalvular gradient ≥10 mmHg resulting in mean gradient ≥20 mmHg‡ with concomitant decrease in AVA ≥0.3 cm2 or ≥25% and/or decrease in Doppler velocity index ≥0.1 or ≥20% compared to echocardiographic assessment performed 1 to 3 months post-procedure (or discharge if not available), OR new occurrence or increase of ≥1 grade of transvalvular AR resulting in moderate transvalvular AR.
Any of following:
Mean transprosthetic gradient ≥40 mmHg;
Mean transprosthetic gradient ≥20 mmHg change from baseline;
Severe intra-prosthetic aortic regurgitation, new or worsening (>2+/4+) from baseline
Severe haemodynamic SVD
Severe haemodynamic valve deterioration
Morphological valve deterioration AND: Increase in mean transvalvular gradient ≥20 mmHg resulting in mean gradient ≥30 mmHg‡ with concomitant decrease in AVA ≥0.6 cm2 or ≥50% and/or decrease in Doppler velocity index ≥0.2 or ≥40% compared to echocardiographic assessment performed 1 to 3 months post-procedure (or discharge if not available), OR new occurrence, or increase of ≥2 grades, of transvalvular AR resulting in severe AR.
haemodynamic and morphological SVD
Bioprosthetic Valve failure (BVF)
- Autopsy findings of bioprosthetic valve dysfunction, likely related to the cause of death, or valve-related death;
- Repeat intervention following confirmed diagnosis of bioprosthetic valve dysfunction;
- Severe haemodynamic SVD
Stage 1
Any significant bioprosthetic valve dysfunction with clinically expressive criteria (new-onset or worsening symptoms, left ventricular dilation/ hypertrophy/ dysfunction, or pulmonary hypertension) OR Stage 3 haemodynamic valve deterioration related to permanent changes to the prosthetic valve.
Stage 2
Aortic valve reoperation or reintervention
Stage 3
Valve-related death
‡ This criteria for haemodynamic dysfunction assumes normal flow.
† Cardiovascular mortality presumed to be associated with bioprosthetic valve dysfunction.
AR = aortic valve regurgitation; AVA = aortic valve area; EAPCI/ ESC/EACTS =European Association of Percutaneous Cardiovascular Interventions/European Society of Cardiology/European Association for Cardio-Thoracic Surgery; LV = left ventricular; VARC = Valve Academic Research Consortium.
Available data on the durability comparing SAVR with TAVI using the VARC-3 definition are limited, but recent reports from RCTs are increasingly adapting the VARC-3 definition (Figure 30). In the pooled analysis of the PARTNER 2A trial and the SAPIEN 3 registry, the SAPIEN-XT TAVI cohort had a significantly higher 5-year exposure adjusted incidence rates (per 100 patient-years) of SVD (1.61 ± 0.24% vs. 0.63 ± 0.16%), SVD-related BVF (0.58 ± 0.14% vs. 0.12 ± 0.07%), and all-cause (structural or nonstructural) BVF (0.81 ± 0.16% vs. 0.27 ± 0.10%) (P <0.01 for all) compared with SAVR, while there was a similar rate of SVD (0.68 ± 0.18% vs. 0.60 ± 0.17%; P = 0.71), SVD-related BVF (0.29 ± 0.12% vs. 0.14 ± 0.08%; P = 0.25), and all-cause BVF (0.60 ± 0.15% vs. 0.32 ± 0.11%; P = 0.32) between SAPIEN 3 TAVI and SAVR272. Pibarot P, Ternacle J, Jaber WA, et al. Structural Deterioration of Transcatheter Versus Surgical Aortic Valve Bioprostheses in the PARTNER-2 Trial. J Am Coll Cardiol. 2020;76:1830-1843 Link. The PARTNER 3 trial also reported on the durability data of the SAPIEN 3 THV. At 5 years, the Kaplan–Meier estimates of BVF of any cause were 3.3% in the TAVI group and 3.8% in the surgery group and the incidence of SVD-related BVF was 1.4% in the TAVR group and 2.0% in the surgery group53. Mack MJ, Leon MB, Thourani VH, et al. Transcatheter Aortic-Valve Replacement in Low-Risk Patients at Five Years. N Engl J Med. 2023;389:1949-1960 Link. Favourable durability data have also been reported for self-expanding CoreValve/Evolut THV In the pooled data of the CoreValve US High Risk Pivotal (n = 726) and SURTAVI (n = 1,618) RCTs, the cumulative incidence of VARC-3 BVD and SVD (moderate or severe HVD) treating death as a competing risk was lower in patients undergoing TAVI than surgery (BVD: 9.7% vs. 15.3%, sHR 0.57; 95% CI 0.45-0.73, P <0.001; SVD: 2.4% vs. 4.5%, sHR 0.54, 95% CI 0.33-0.88, P = 0.01, respectively)269. Yakubov SJ, Van Mieghem NM, Oh JK, et al. Impact of Transcatheter or Surgical Aortic Valve Performance on 5-Year Outcomes in Patients at ≥ Intermediate Risk. J Am Coll Cardiol. 2025;85:1419-1430. Link. The NOTION trial reported the longest durability data to date on the self-expanding CoreValve THV compared with SAVR. In this trial, severe SVD (VARC-3 severe HVD) was recorded in 1.5% and 10.0% (HR 0.2; 95% CI 0.04–0.7; P = 0.02) of surviving patients after TAVI and SAVR, respectively. The cumulative incidence for severe non-SVD BVD was 20.5% and 43.0% (P <0.001) and for endocarditis 7.2% and 7.4% (P = 1.0) after TAVI and SAVR, respectively, and no patient experienced clinical valve thrombosis. BVF occurred in 9.7% of TAVI and 13.8% of SAVR patients (HR 0.7; 95% CI 0.4–1.5; P = 0.4)54. Thyregod HGH, Jorgensen TH, Ihlemann N, et al. Transcatheter or surgical aortic valve implantation: 10-year outcomes of the NOTION trial. Eur Heart J. 2024;45:1116-1124 Link. Although RCTs have provided high quality data on the durability of THV, comparisons with the durability of SAVR should consider the non-uniform use of surgical bioprostheses and increased post-procedural gradients immediately after implantation. In summary, available data suggest similar durability of THV and surgical bioprostheses up to 10 years after AVR.
Figure 30
Valve durability comparing transcatheter and surgical bioprostheses in ranodomized control trials. Data reproduced from Thyregod et al. Eur Heart J 2024;45:1116-1124; Mack et al. N Nngl J Med 2023;389:1949-1960; Yakubo et al. J Am Coll Cardiol 2025. [Online ahead of print]. doi: 10.1016/j.jacc.2025.02.009; and Pibarot et al. J Am Coll Cardiol 2020;76:1830-1843.
Bioprosthetic valve thrombosis is relatively rare but an important cause of BVD. Traditionally, bioprostheses have been considered less thrombogenic than mechanical heart valves. However, recent evaluations of the performance and durability of bioprostheses and the advent of MDCT as a novel diagnostic modality has highlighted the issue in various types of THV as well as SAVR valves255. Makkar RR, Blanke P, Leipsic J, et al. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75:3003-3015 Link. Bioprosthetic valve thrombosis typically comprises two distinct entities, clinical valve thrombosis and subclinical leaflet thrombosis. Clinical valve thrombosis is defined by the detection of valve dysfunction secondary to thrombosis or a mobile mass detected on the prosthesis typically associated with increased transvalvular gradients. For the treatment of clinical valve thrombosis, current ESC/EACTS and AHA/ACC guidelines for the management of valvular heart disease recommend OAC with VKA or unfractionated heparin as the first-line treatment before considering invasive treatment (Table 17). After a period of 3 to 6 months, OAC may be discontinued if resolution of thrombus and improvement in bioprosthetic function are achieved. In case of unresolved or recurrent clinical valve thrombosis, lifelong OAC should be considered, 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link.
Table 17. Guideline recommendations: Treatment of clinical valve thrombosis.
2020 AHA/ACC Valvular Heart Disease Guideline
2021 ESC/EACTS Valvular Heart Disease Guideline
Recommendations
COR
LOE
Recommendations
COR
LOE
In patients with suspected or confirmed bioprosthetic valve thrombosis who are haemodynamically stable and have no contraindications to anticoagulation, initial treatment with a VKA is reasonable.
2a
B-NR
Anticoagulation using a VKA and/or UFH is recommended in bioprosthetic valve thrombosis before considering re-intervention.
I
C
Anticoagulation should be considered in patients with leaflet thickening and reduced leaflet motion leading to elevated gradients, at least until resolution.
IIa
B
ACC/AHA = American College of Cardiology/American Heart Association; COR = class of recommendation; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; UFH = unfractionated heparin; VKA = vitamin K antagonist.
In contrast to clinical valve thrombosis, subclinical leaflet thrombosis (HALT and RLM) is most often an incidental finding as assessed by MDCT271. VARC-3 WRITING COMMITTEE; Genereux P, Piazza N, et al. Valve Academic Research Consortium 3: updated endpoint definitions for aortic valve clinical research. Eur Heart J 2021;42:1825-1857. doi: 10.1093/eurheartj/ehaa799 Link. The epidemiology and natural history of clinical and subclinical valve thrombosis is not well established. MDCT assessment of bioprostheses in the framework of the RCTs have reported that subclinical leaflet thrombosis occurs in 10-50% of patients after TAVI and may be associated with an increased risk of clinical valve thrombosis. However, subclinical valve thrombosis may also regress spontaneously without changes in antithrombotic therapy, complicating the establishment of a uniform treatment strategy, 254. Blanke P, Leipsic JA, Popma JJ, et al. Bioprosthetic Aortic Valve Leaflet Thickening in the Evolut Low Risk Sub-Study. J Am Coll Cardiol. 2020;75:2430-2442 Link255. Makkar RR, Blanke P, Leipsic J, et al. Subclinical Leaflet Thrombosis in Transcatheter and Surgical Bioprosthetic Valves: PARTNER 3 Cardiac Computed Tomography Substudy. J Am Coll Cardiol. 2020;75:3003-3015 Link. In this context, close clinical and echocardiographic follow-up is recommended with use of OAC being individualized depending on HALT/RLM evolution and bleeding risk273. Adrichem R, Rodes Cabau J, Mehran R, et al. Treatment of Transcatheter Aortic Valve Thrombosis: JACC Review Topic of the Week. J Am Coll Cardiol. 2024;84:848-861 Link.
Bioprosthetic valve endocarditis
Prosthetic valve endocarditis is a rare but serious complication associated with valve failure and mortality after TAVI. The incidence of prosthetic valve endocarditis after TAVI is comparable to that after SAVR. In PARTNER 1 and 2, the incidence of prosthetic valve endocarditis was 5.21 per 1,000 person-years (95% CI, 4.26-6.38) for TAVI and 4.10 per 1,000 person-years (95% CI, 2.33-7.22) for SAVR during a mean follow-up of 2.69 ± 1.55 years (95% CI, 4.19–6.12)274. Summers MR, Leon MB, Smith CR, et al. Prosthetic Valve Endocarditis After TAVR and SAVR: Insights From the PARTNER Trials. Circulation. 2019;140:1984-1994 Link. Similarly, in the pooled analysis from 3 RCTs (CoreValve US High Risk, SURTAVI, and Evolut Low Risk), the cumulative incidence of prosthetic valve endocarditis was 1.01% (95% CI, 0.47%–1.96%) after TAVI and 1.58% (95% CI, 0.97%–2.46%) after SAVR (P = 0.047) at 5 years275. Lanz J, Reardon MJ, Pilgrim T, et al. Incidence and Outcomes of Infective Endocarditis After Transcatheter or Surgical Aortic Valve Replacement. J Am Heart Assoc. 2021;10:e020368 Link. The risk of prosthetic valve endocarditis is most pronounced during the periprocedural period. The nationwide SwissTAVI registry reported that the incidence for periprocedural, early, and late endocarditis after TAVI was 2.59, 0.71, and 0.40 events per 100 person-years, respectively276. Stortecky S, Heg D, Tueller D, et al. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;75:3020-3030 Link. Across studies, prosthetic valve endocarditis confers a higher mortality, , , 274. Summers MR, Leon MB, Smith CR, et al. Prosthetic Valve Endocarditis After TAVR and SAVR: Insights From the PARTNER Trials. Circulation. 2019;140:1984-1994 Link275. Lanz J, Reardon MJ, Pilgrim T, et al. Incidence and Outcomes of Infective Endocarditis After Transcatheter or Surgical Aortic Valve Replacement. J Am Heart Assoc. 2021;10:e020368 Link276. Stortecky S, Heg D, Tueller D, et al. Infective Endocarditis After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;75:3020-3030 Link277. Del Val D, Linke A, Abdel-Wahab M, et al. Long-Term Outcomes After Infective Endocarditis After Transcatheter Aortic Valve Replacement. Circulation. 2020;142:1497-1499 Link, and 20% of TAVI endocarditis cases require cardiac surgery, which is generally complex and associated with morbidity278. Mangner N, del Val D, Abdel-Wahab M, et al. Surgical Treatment of Patients With Infective Endocarditis After Transcatheter Aortic Valve Implantation. J Am Coll Cardiol. 2022;79:772-785 Link. Therefore, optimal antibiotic coverage and procedural infection prevention using surgical standards as well as antibiotic prophylaxis for invasive procedures after TAVI are key to mitigate the risk of prosthetic valve endocarditis with TAVI179. Delgado V, Ajmone Marsan N, de Waha S, et al. 2023 ESC Guidelines for the management of endocarditis. Eur Heart J. 2023;44:3948-4042 Link.
Modern TAVI: Fast-track pathways
With the expansion of TAVI indications, there is an ever increasing demand for TAVI. In a population-level retrospective cohort study of 22,876 referrals for AVR in Toronto, Ontario, there was a significant increase in wait times for AVR between 2012 and 2018 (from a median of 40 days in 2012 to 90 days in 2018), which was more pronounced for TAVI (increase from a median 80 days in 2012 to 110 days in 2018), and associated with increased mortality and heart failure-related hospitalizations while on the waiting list279. Albassam O, Henning KA, Qiu F, et al. Increasing Wait-Time Mortality for Severe Aortic Stenosis: A Population-Level Study of the Transition in Practice From Surgical Aortic Valve Replacement to Transcatheter Aortic Valve Replacement. Circ Cardiovasc Interv. 2020;13:e009297 Link. The UK Valve for Life initiative is a national project to improve the delivery of transcatheter valve therapy. In the national survey of all TAVI centres in England, 52% of centres reported that they could not perform more TAVI due to cath lab/hybrid room capacity limitations, lack of coronary care unit or ward bed capacity, and MDCT scan availability, 280. Ali N, Faour A, Rawlins J, et al. 'Valve for Life': tackling the deficit in transcatheter treatment of heart valve disease in the UK. Open Heart. 2021;8:e001547. Link281. Valve For Life UK: Increasing access to transcatheter heart therapies in the UK. Link.
Against the background of limited space and human resources, several approaches have been developed to improve access to TAVI. The minimalist approach, including local anaesthesia without transesophageal echocardiographic guidance to simplify transfemoral TAVI procedures is now widely used worldwide282. Durand E, Borz B, Godin M, et al. Transfemoral aortic valve replacement with the Edwards SAPIEN and Edwards SAPIEN XT prosthesis using exclusively local anesthesia and fluoroscopic guidance: feasibility and 30-day outcomes. JACC Cardiovasc Interv. 2012;5:461-467 Link. In addition to the minimalist approach, TAVI using fast-track pathways is receiving increasing attention to reduce the length of hospital stay, leading to early discharge after TAVI. The Vancouver 3M (Multidisciplinary, Multimodality, but Minimalist) Clinical Pathway and the FAST-TAVI Pathway, which focused on early and next-day discharge through the use of objective anatomic and functional screening criteria and streamlined, standardized peri-procedural and postprocedural management guidelines, have shown that implementation of the fast-track pathways allow a high rate of next-day or early home discharge after TAVI without increasing the risk of adverse events in carefully selected patients, , 283. Lauck SB, Wood DA, Baumbusch J, et al. Vancouver Transcatheter Aortic Valve Replacement Clinical Pathway: Minimalist Approach, Standardized Care, and Discharge Criteria to Reduce Length of Stay. Circ Cardiovasc Qual Outcomes. 2016;9:312-321 Link284. Barbanti M, van Mourik MS, Spence MS, et al. Optimising patient discharge management after transfemoral transcatheter aortic valve implantation: the multicentre European FAST-TAVI trial. EuroIntervention. 2019;15:147-154 Link285. Wood DA, Lauck SB, Cairns JA, et al. The Vancouver 3M (Multidisciplinary, Multimodality, But Minimalist) Clinical Pathway Facilitates Safe Next-Day Discharge Home at Low-, Medium-, and High-Volume Transfemoral Transcatheter Aortic Valve Replacement Centers: The 3M TAVR Study. JACC Cardiovasc Interv. 2019;12:459-469 Link. More recently, the Cleveland Clinic has reported the safety and feasibility of same-day discharge following transfemoral TAVI compared with next-day discharge in the contemporary TAVI era. The same-day discharge was based on 6 criteria including procedural characteristics and outcomes, patient comfort, and availability of social support after discharge. In 2020, same-day discharge and next-day discharge accounted for 22.1% (n = 114 of 516) and 63.8% (n = 329 of 516) of transfemoral TAVI, respectively, and there was no significant difference in in-hospital clinical outcomes and 30-day readmissions286. Krishnaswamy A, Isogai T, Agrawal A, et al. Feasibility and Safety of Same-Day Discharge Following Transfemoral Transcatheter Aortic Valve Replacement. JACC Cardiovasc Interv. 2022;15:575-589 Link. FAST-TAVI II was a prospective, multicentre, cluster-randomized, controlled trial in patients with severe symptomatic AS to evaluate the efficacy and safety of a dedicated training program aimed at reducing the length of hospital stay after transfemoral TAVI. In this cluster-randomized trial involving 20 French TAVI centres, patients randomized to the intervention group received a dedicated training programme implementing 10 quality of care measures to reduce length of hospital stays, with an implementation phase of eight weeks. The primary endpoint was the proportion of patients discharged early within 3 days which was achieved more frequently in the intervention group than the control group (58.1% vs. 42.3%, P <0.0001)287. Durand E, Beziau-Gasnier D, Michel M, et al. Reducing length of stay after transfemoral transcatheter aortic valve implantation: the FAST-TAVI II trial. Eur Heart J. 2024;45:952-962 Link. In summary, minimalist TAVI with fast-track pathways has demonstrated a reduction in the length of hospital stay after TAVI without increasing the risk of adverse events. Further efforts are warranted to reduce the length of hospital stay and increase the proportion of patients discharged home early after TAVI.
Repeat aortic valve intervention and lifetime strategy
The choice of prosthesis type in patients referred for valve replacement remains a debated issue, particularly in younger patients with a longer life expectancy. Although several studies have consistently shown that mechanical prostheses are associated with a lower risk of reoperation than bioprostheses, the benefit of extended durability intrinsic to mechanical prostheses must be balanced against the lifelong need for OAC and the associated risk of bleeding and the inconvenience of monitoring, dietary restrictions, medication interactions, and the need to restrict participation in some types of athletic activity. Current guidelines recommend mechanical prostheses in younger patients (patients younger than 50 years of age in AHA/ACC guideline and younger than 60 years of age in ESC/EACTS guideline), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. In a recent report from the STS Adult Cardiac Surgery Database comparing isolated mechanical or bioprosthetic SAVR in patients aged 40-75 years (2008-2019), patients 60 years of age or younger treated with mechanical SAVR showed benefit in terms of freedom from risk-adjusted all-cause mortality (40-49 years: stabilized inverse probability weights (sIPW)-adjusted HR 0.69, 95% CI 0.59-0.79; 50-59 years: sIPW-adjusted HR 0.87, 95% CI 0.80-0.94; 60-69 years: sIPW-adjusted HR 0.99, 95% CI 0.91-1.08; and 70-79 years: sIPW-adjusted HR 1.12, 95% CI 0.97-1.29, respectively)288. Bowdish ME, Mehaffey JH, Chang S-C, et al. Bioprosthetic vs Mechanical Aortic Valve Replacement in Patients 40-75 Years. J Am Coll Cardiol. 2025 ;85:1289-1298 Link. However, several studies have reported that the use of mechanical prostheses in surgical procedures has declined over time even in younger patients, and the extended durability of the newer bioprostheses as well as the emergence of TAVI have further expedited this trend, , 289. Hickey GL, Bridgewater B, Grant SW, et al. National Registry Data and Record Linkage to Inform Postmarket Surveillance of Prosthetic Aortic Valve Models Over 15 Years. Jama. Intern Med 2017;177:79-86 Link290. Alkhouli M, Alqahtani F, Kawsara A, et al. National Trends in Mechanical Valve Replacement in Patients Aged 50 to 70 Years. J Am Coll Cardiol. 2020;76:2687-2688 Link291. Tam DY, Rocha RV, Wijeysundera HC, et al. Surgical valve selection in the era of transcatheter aortic valve replacement in the Society of Thoracic Surgeons Database. J Thorac Cardiovasc Surg. 2020;159:416-427 e418 Link. Consequently, the number of failed bioprostheses requiring repeat aortic valve intervention has increased. Traditionally, redo SAVR has been the standard procedure for the treatment of failed bioprostheses; however, multiple open-heart surgeries carry an increased risk related to technical issues of reoperation as well as patient’s age and comorbidities292. Bianco V, Kilic A, Gleason TG, et al. Reoperative Cardiac Surgery Is a Risk Factor for Long-Term Mortality. Ann Thorac Surg. 2020;110:1235-1242 Link. Valve-in-valve TAVI (TAV-in-SAV or TAV-in-TAV) has emerged as a less invasive and preferred treatment option for patients with failed bioprostheses and has markedly increased in use, , 24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link293. Piazza N, Bleiziffer S, Brockmann G, et al. Transcatheter aortic valve implantation for failing surgical aortic bioprosthetic valve: from concept to clinical application and evaluation (part 1). JACC Cardiovasc Interv. 2011;4:721-732 Link294. Piazza N, Bleiziffer S, Brockmann G, et al. Transcatheter aortic valve implantation for failing surgical aortic bioprosthetic valve: from concept to clinical application and evaluation (part 2). JACC Cardiovasc Interv. 2011;4:733-742 Link.
TAV-in-SAV
TAVI for failed surgical bioprosthesis (TAV-in-SAV) is a predominant form of valve-in-valve TAVI24. Carroll JD, Mack MJ, Vemulapalli S, et al. STS-ACC TVT Registry of Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:2492-2516 Link. Several dedicated registries have reported procedural and clinical outcomes of TAV-in-SAV, , , , , , 295. Dvir D, Webb JG, Bleiziffer S, et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA. 2014;312:162-170 Link296. Deeb GM, Chetcuti SJ, Reardon MJ, et al. 1-Year Results in Patients Undergoing Transcatheter Aortic Valve Replacement With Failed Surgical Bioprostheses. JACC Cardiovasc Interv. 2017;10:1034-1044 Link297. Tuzcu EM, Kapadia SR, Vemulapalli S, et al. Transcatheter Aortic Valve Replacement of Failed Surgically Implanted Bioprostheses: The STS/ACC Registry. J Am Coll Cardiol. 2018;72:370-382 Link298. Webb JG, Mack MJ, White JM, et al. Transcatheter Aortic Valve Implantation Within Degenerated Aortic Surgical Bioprostheses: PARTNER 2 Valve-in-Valve Registry. J Am Coll Cardiol. 2017;69:2253-2262 Link299. Webb JG, Murdoch DJ, Alu MC, et al. 3-Year Outcomes After Valve-in-Valve Transcatheter Aortic Valve Replacement for Degenerated Bioprostheses: The PARTNER 2 Registry. J Am Coll Cardiol. 2019;73:2647-2655 Link300. Bleiziffer S, Simonato M, Webb JG, et al. Long-term outcomes after transcatheter aortic valve implantation in failed bioprosthetic valves. Eur Heart J. 2020;41:2731-2742 Link301. Hahn RT, Webb J, Pibarot P, et al. 5-Year Follow-Up From the PARTNER 2 Aortic Valve-in-Valve Registry for Degenerated Aortic Surgical Bioprostheses. JACC Cardiovasc Interv. 2022;15:698-708 Link. In a meta-analysis of 5,553 TAV-in-SAV cases from 24 studies, the procedural success rate was 97% (95% CI 94-98%) with a low 30-day adverse event rate (death: 5% [95% CI 3-6%]; stroke: 2% [95% CI 1-2%]; myocardial infarction: 1% [95% CI 1-2%]; and new permanent pacemaker implantation: 7% [95% CI 5-11%], respectively)302. Mahmoud AN, Gad MM, Elgendy IY, et al. Systematic review and meta-analysis of valve-in-valve transcatheter aortic valve replacement in patients with failed bioprosthetic aortic valves. EuroIntervention. 2020;16:539-548 Link. The PARTNER 2 ViV and continued access registries have reported long-term clinical outcomes up to 5 years of follow-up in patients undergoing TAV-in-SAV at high surgical risk (N = 369, mean age was 78.9 ± 10.2 years, and the mean STS-PROM was 9.1 ± 4.7%). At 5 years, all-cause death and stroke occurred in 50.6% and 10.5% of patients, respectively, and a significant improvement in patient health status was observed compared to baseline. The bioprosthetic haemodynamic properties were sustained over 5 years, and the incidence of VARC-3 SVD-related BVF was low (2.3%)301. Hahn RT, Webb J, Pibarot P, et al. 5-Year Follow-Up From the PARTNER 2 Aortic Valve-in-Valve Registry for Degenerated Aortic Surgical Bioprostheses. JACC Cardiovasc Interv. 2022;15:698-708 Link. The outcome of TAV-in-SAV has been compared to redo SAVR. In a French nationwide propensity-matched analysis of 717 matched pairs (2010-2019), TAV-in-SAV was associated with a lower risk of the composite of all-cause mortality, all-cause stroke, myocardial infarction, and major or life-threatening bleeding at 30 days compared with redo SAVR (odds ratio: 0.62; 95% CI: 0.44-0.88), while the incidence of the combined endpoint was similar between groups during a median follow-up of 516 days, (odds ratio: 1.18; 95% CI: 0.99-1.41)303. Deharo P, Bisson A, Herbert J, et al. Transcatheter Valve-in-Valve Aortic Valve Replacement as an Alternative to Surgical Re-Replacement. J Am Coll Cardiol. 2020;76:489-499 Link. Similarly, in a meta-analysis including a total of 16,207 patients (8,048 TAV-in-SAV and 8,159 redo SAVR) from 35 studies (2015-2020), TAV-in-SAV was associated with lower all-cause mortality and major bleeding at 30 days (odds ratio 0.52, 95% CI: 0.39-0.68; and odds ratio 0.48 95% CI: 0.28-0.80, respectively), but comparable 1-year mortality compared with redo SAVR (odds ratio 0.90, 95% CI: 0.61-1.32). Of note, TAV-in-SAV was associated with a higher rate of severe prosthesis-patient mismatch (OR: 4.63; 95% CI: 3.05-7.03)304. Sa M, Van den Eynde J, Simonato M, et al. Valve-in-Valve Transcatheter Aortic Valve Replacement Versus Redo Surgical Aortic Valve Replacement: An Updated Meta-Analysis. JACC Cardiovasc Interv. 2021;14:211-220 Link. TAV-in-SAV for small surgical bioprostheses, stenotic cause of bioprosthesis failure, and pre-existing prosthesis-patient mismatch, all of which are associated with an increased risk of severe prosthesis-patient mismatch after TAV-in-SAV, are the principal risk factors for redo aortic valve surgery and impaired survival after TAV-in-SAV, 295. Dvir D, Webb JG, Bleiziffer S, et al. Transcatheter aortic valve implantation in failed bioprosthetic surgical valves. JAMA. 2014;312:162-170 Link300. Bleiziffer S, Simonato M, Webb JG, et al. Long-term outcomes after transcatheter aortic valve implantation in failed bioprosthetic valves. Eur Heart J. 2020;41:2731-2742 Link. The use of self-expanding THV and bioprosthetic valve fracture have been suggested to mitigate the risk of prosthesis-patient mismatch after TAV-in-SAV, , 305. Rodes-Cabau J, Abbas AE, Serra V, et al. Balloon- vs Self-Expanding Valve Systems for Failed Small Surgical Aortic Valve Bioprostheses. J Am Coll Cardiol. 2022;80:681-693 Link306. Nuche J, Abbas AE, Serra V, et al. Balloon- vs Self-Expanding Transcatheter Valves for Failed Small Surgical Aortic Bioprostheses: 1-Year Results of the LYTEN Trial. JACC Cardiovasc Interv. 2023;16:2999-3012 Link307. Chhatriwalla AK, Allen KB, Depta JP, et al. Outcomes of Bioprosthetic Valve Fracture in Patients Undergoing Valve-in-Valve TAVR. JACC Cardiovasc Interv. 2023;16:530-539 Link.
TAV-in-TAV (Redo-TAVI)
As TAVI has expanded to low-risk patients with longer life-expectancy, the number of patients with failed THV will increase. Owing to the favourable outcomes of TAV-in-SAV, TAV-in-TAV (redo TAVI) has been considered as a reasonable treatment option for THV failure. In the multicentre Redo-TAVR registry of 63,876 TAVI patients treated at 37 centers in 2019, 212 patients (0.33%) underwent redo TAVI and 138 (64%) were treated 1 year or later after the initial TAVI procedure. Device success according to the VARC-2 definition was achieved in 180 patients (85.1%) with most failures being attributable to high residual gradients (14.1%) or regurgitation (8.9%). Kaplan-Meier survival estimates were 97.2% at 30 days and 86.5% at 1 year, respectively310. Landes U, Webb JG, De Backer O, et al. Repeat Transcatheter Aortic Valve Replacement for Transcatheter Prosthesis Dysfunction. J Am Coll Cardiol. 2020;75:1882-1893 Link. The STS/ACC TVT registry compared procedural and clinical outcomes and bioprosthetic haemodynamics in 1,320 propensity-matched pairs of patients undergoing redo TAVI and native TAVI (redo TAVI cohort: mean age 78 years; 42.3% female; mean STS-PROM 8.1%). Although mean transprosthetic gradient was higher in the redo TAVI group compared with the native TAVI group (15 mmHg vs. 12 mmHg; P <0.0001), there were no between group differences with respect to risk of moderate or severe PVR, procedural complications, and clinical outcomes at 30 days and 1 year (death, stroke, and valve-related admission)311. Makkar RR, Kapadia S, Chakravarty T, et al. Outcomes of repeat transcatheter aortic valve replacement with balloon-expandable valves: a registry study. Lancet. 2023;402:1529-1540 Link.
Challenges for Valve-in-Valve TAVI Procedures
In addition to the risk of increased residual gradients and patient-prosthesis mismatch after the procedure, valve-in-valve TAVI procedures have an increased risk of coronary obstruction and potentially challenging coronary access after the procedure. The incidence of coronary obstruction following valve-in-valve TAVI is considerably higher than that in TAVI for native aortic valve (2.0-3.5% vs. <1.0%), 222. Ojeda S, Gonzalez-Manzanares R, Jimenez-Quevedo P, et al. Coronary Obstruction After Transcatheter Aortic Valve Replacement: Insights From the Spanish TAVI Registry. JACC Cardiovasc Interv. 2023;16:1208-1217 Link312. Ribeiro HB, Rodés-Cabau J, Blanke P, et al. Incidence, predictors, and clinical outcomes of coronary obstruction following transcatheter aortic valve replacement for degenerative bioprosthetic surgical valves: insights from the VIVID registry. Eur Heart J. 2018;39:687-695 Link, due to a Neoskirt potentially extending above the coronary ostia resulting in sinus sequestration. In addition, the risk is pronounced in specific procedures. For example, in TAV-in-SAV procedures, TAVI in failed stentless surgical bioprotheses is more challenging compared with TAVI in failed stented surgical bioprotheses, due to the lack of fluoroscopic markers at the stent frame or sewing ring, and a shorter distance of the prosthetic valve leaflets from the coronary ostia attributable to the supra-annular position. In the VIVID registry, device malposition (10.3% vs. 6.2%, P = 0.014), second THV implantation (7.9% vs. 3.4%, P <0.001), and coronary obstruction (6.0% vs. 1.5%, P <0.001) occurred more frequently in stentless TAV-in-SAV313. Duncan A, Moat N, Simonato M, et al. Outcomes Following Transcatheter Aortic Valve Replacement for Degenerative Stentless Versus Stented Bioprostheses. JACC Cardiovasc Interv. 2019;12:1256-1263 Link. In addition, Redo TAVI is more complex than TAV-in-SAV because of the unique design of THV devices, compatibility issues, and the need for individualized planning based on factors such as implant depth, shape, and coronary artery relationships. Therefore, operators must assess these risks during a detailed preprocedural planning for each individual. Correct identification of the type and size of the implanted bioprosthesis is an important consideration when performing Valve-in-Valve TAVI. This information is usually obtained from previous SAVR/TAVI operative notes or valve identification cards provided by the manufacturers. Similarly, pre-procedural MDCT plays a key role in determining the size of THV and identifying the risk of coronary obstruction in valve-in-valve TAVI (TAV-in-SAV and TAV-in-TAV). A step-by-step assessment of the feasibility of valve-in-valve TAVI, including 1) identification of type and size of initial aortic bioprosthesis, 2) MDCT assessment, 3) selection of THV type and size, and 4) risk assessment of coronary obstruction, should be performed to obtain optimal results of valve-in-valve TAVI. Dedicated smartphone applications will guide the decision in terms of type and size of a THV for the valve-in-valve procedure (https://apps.apple.com/us/app/valve-in-valve/id655683780; https://apps.apple.com/us/app/valve-ppm/id1604258260; https://apps.apple.com/us/app/redo-tav/id6462937010), 314. Bapat V. Valve-in-valve apps: why and how they were developed and how to use them. EuroIntervention. 2014;10 Suppl U:U44-51 Link315. Bapat VN, Fukui M, Zaid S, et al. A Guide to Transcatheter Aortic Valve Design and Systematic Planning for a Redo-TAV (TAV-in-TAV) Procedure. JACC Cardiovasc Interv. 2024;17:1631-1651 Link.
To achieve a better haemodynamic status after valve-in-valve TAVI, bioprosthetic valve fracture has been proposed. Bioprosthetic valve fracture is a technique in which the sewing ring of the failed surgical bioprosthesis is fractured by noncompliant, high-pressure balloon inflation with the goal of optimizing THV expansion and improving haemodynamics after TAV-in-SAV. Although several studies have reported improved bioprosthetic haemodynamics after TAV-in-SAV using bioprosthetic valve fracture, the overall clinical benefit remains uncertain. A report from the STS/ACC TVT registry, which included 2,975 patients who underwent valve-in-valve TAVI between 2020 and 2022 (bioprosthetic valve fracture was performed in 619 patients [21%]), found that attempted bioprosthetic valve fracture was associated with higher in-hospital mortality (odds ratio: 2.51; 95% CI: 1.30-4.84) and life-threatening bleeding (odds ratio: 2.55; 95% CI: 1.44-4.50) compared with no bioprosthetic valve fracture, while the benefits in bioprosthetic haemodynamics were modest (effective orifice area: 1.6 cm2 vs. 1.4 cm2, P <0.01; and mean gradient: 16.3 mmHg vs. 19.2 mmHg, P <0.01, respectively). Of note, when bioprosthetic valve fracture was stratified according to timing (before vs. after THV implantation), patients who underwent bioprosthetic valve fracture after THV implantation had a better haemodynamic status and similar in-hospital mortality to patients who did not undergo bioprosthetic valve fracture307. Chhatriwalla AK, Allen KB, Depta JP, et al. Outcomes of Bioprosthetic Valve Fracture in Patients Undergoing Valve-in-Valve TAVR. JACC Cardiovasc Interv. 2023;16:530-539 Link.
TAVI explant
Depending on the index TAVI procedure and the aortic root anatomy, surgical explantation of the THV may be required for the treatment of TAVI failure. In the EXPLANT-TAVR registry including 269 patients who underwent TAVI explantation between 2009 and 2020, the most common indication for surgical intervention was endocarditis (43.1%), followed by SVD (20.1%), PVR (18.2%) and prosthesis-patient mismatch (10.8%), and more than 25% of patients were considered ineligible for redo TAVI due to unfavourable anatomy316. Bapat VN, Zaid S, Fukuhara S, et al. Surgical Explantation After TAVR Failure: Mid-Term Outcomes From the EXPLANT-TAVR International Registry. JACC Cardiovasc Interv. 2021;14:1978-1991 Link. Of note, explantation of THV is technically more demanding than native valve SAVR due to potential iatrogenic injury to the sinotubular junction, aorta, mitral valve, or membranous septum. In particular, explantation of self-expanding THV requires careful endarterectomy of the endothelialized stent frame, and THV may require detachment from the anterior leaflet of the mitral valve when implanted too low. Indeed, more than half of explantation cases required concomitant procedures as reported in previous studies, including aortic root repair/replacement and mitral valve repair/replacement, which may complicate the operation and perioperative management, 316. Bapat VN, Zaid S, Fukuhara S, et al. Surgical Explantation After TAVR Failure: Mid-Term Outcomes From the EXPLANT-TAVR International Registry. JACC Cardiovasc Interv. 2021;14:1978-1991 Link317. Fukuhara S, Brescia AA, Shiomi S, et al. Surgical explantation of transcatheter aortic bioprostheses: Results and clinical implications. J Thorac Cardiovasc Surg. 2021;162:539-547 e531 Link. The perioperative risk of TAVI explantation is substantial, with reported 30-day mortality rates ranging from 10% to 30%318. Kaneko T, Bapat VN, Alakhtar AM, et al. Transcatheter heart valve explantation for transcatheter aortic valve replacement failure: A Heart Valve Collaboratory expert consensus document on operative techniques. J Thorac Cardiovasc Surg. 2025;169:878-889 Link, which is significantly higher compared with redo TAVI319. Tang GHL, Zaid S, Kleiman NS, et al. Explant vs Redo-TAVR After Transcatheter Valve Failure: Mid-Term Outcomes From the EXPLANTORREDO-TAVR International Registry. JACC Cardiovasc Interv. 2023;16:927-941 Link. Lack of procedural expertise may contribute to adverse outcomes320. Hasan I, Sultan I. Commentary: Transcatheter aortic valve explantation: Surgical strategies for superior outcomes. J Thorac Cardiovasc Surg. 2024;48(4):e70134. Link; in the STS database from 2011 to 2018, the median number of TAVI explantations per surgeon and per institution was 1321. Fukuhara S, Brescia AA, Deeb GM. Surgical Explantation of Transcatheter Aortic Bioprostheses: An Analysis From the Society of Thoracic Surgeons Database. Circulation. 2020;142:2285-2287 Link, and the mean annual volume of aortic root replacements performed at cardiac surgery centres in the US was 5322. Ogami T, Serna-Gallegos D, Arnaoutakis GJ, et al. The impact of reoperative surgery on aortic root replacement in the United States. J Thorac Cardiovasc Surg. 2024;167:1185-1193.e1 Link.
Lifetime strategy
As younger patients have a life-expectancy that may exceed the durability of the bioprosthesis, it becomes increasingly important to anticipate lifetime AVR strategies beyond the 10-15 year timeframe after the index procedure, 116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link323. Yerasi C, Rogers T, Forrestal BJ, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Young, Low-Risk Patients With Severe Aortic Stenosis. JACC Cardiovasc Interv. 2021;14:1169-1180 Link. Given the risks associated with multiple open-heart surgeries292. Bianco V, Kilic A, Gleason TG, et al. Reoperative Cardiac Surgery Is a Risk Factor for Long-Term Mortality. Ann Thorac Surg. 2020;110:1235-1242 Link and challenges of valve-in-valve procedures (e.g., coronary obstruction and suboptimal bioprosthetic haemodynamics), 315. Bapat VN, Fukui M, Zaid S, et al. A Guide to Transcatheter Aortic Valve Design and Systematic Planning for a Redo-TAV (TAV-in-TAV) Procedure. JACC Cardiovasc Interv. 2024;17:1631-1651 Link324. Tarantini G, Dvir D, Tang GHL. Transcatheter aortic valve implantation in degenerated surgical aortic valves. EuroIntervention. 2021;17:709-719 Link, incorporating both SAVR and TAVI in a sequence of lifetime interventions is critical (Figure 31). A SAVR-first strategy with a mechanical prosthesis or a Ross procedure is the most common scenario for young patients at present (<50 years of age). In patients at low surgical, who received a bioprosthesis at young age and require a second intervention when they are in their 60ies, redo SAVR followed by valve-in-valve TAVI as a third intervention in their 70s to 80s may be a plausible treatment strategy (SAVR–SAVR–TAVI). SAVR-TAVI-TAVI is a potentially less invasive strategy with the need for only one open-heart surgery in a lifetime. In this scenario, every effort should be made to implant the largest possible surgical bioprosthesis with/without aortic root enlargement at the index SAVR to optimise haemodynamics after anticipated future valve-in-valve TAVI. A TAVI-first strategies (TAVI-SAVR-TAVI) is another potentially less invasive strategy. This strategy may be beneficial in younger patients who are working, exercising, or wishing to become pregnant, in terms of faster recovery and no need for long-term anticoagulation. If the first THV degenerates, SAVR as a second intervention can be performed on a naive chest. A TAVI only strategy (TAVI-TAVI-TAVI) might be possible in patients with large aortic root anatomy allowing for the treatment with repeated short-frame THV Of note, all these scenarios are hypothetical considerations lacking validation. Current guidelines recommend that valve-in-valve TAVI for the treatment of degenerated bioprostheses should be considered only at a Comprehensive Valve Center (Class 2a Level of Evidence B-NR recommendation)39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link.
Figure 31
Strategies for lifetime management according to patient’s life expectancy. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Current guidelines recommend clinical and echocardiographic follow-up for patients with asymptomatic severe AS in the absence of reduced left ventricular ejection fraction (LVEF), very severe stenosis, positive stress test, elevated biomarkers, pulmonary hypertension, rapid progression or other indications for AVR (Table 3), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link. However, it remains challenging to distinguish between asymptomatic and symptomatic status because symptoms are subjective and can develop insidiously, and patients adapt to symptoms, leading to underestimation of symptoms by both patients and clinicians. Observational studies, , 325. Taniguchi T, Morimoto T, Shiomi H, et al. Initial Surgical Versus Conservative Strategies in Patients With Asymptomatic Severe Aortic Stenosis. J Am Coll Cardiol. 2015;66:2827-2838 Link326. Lancellotti P, Magne J, Dulgheru R, et al. Outcomes of Patients With Asymptomatic Aortic Stenosis Followed Up in Heart Valve Clinics. Jama. Cardiol 2018;3:1060-1068 Link327. Genereux P, Sharma RP, Cubeddu RJ, et al. The Mortality Burden of Untreated Aortic Stenosis. J Am Coll Cardiol. 2023;82:2101-2109 Link and 2 RCTs comparing SAVR with watchful waiting (RECOVERY and AVATAR), 328. Kang DH, Park SJ, Lee SA, et al. Early Surgery or Conservative Care for Asymptomatic Aortic Stenosis. N Engl J Med. 2020;382:111-119 Link329. Banovic M, Putnik S, Penicka M, et al. Aortic Valve Replacement Versus Conservative Treatment in Asymptomatic Severe Aortic Stenosis: The AVATAR Trial. Circulation. 2022;145:648-658 Link indicate benefits of early SAVR in asymptomatic patients with severe AS. Several recent RCTs have evaluated the safety and efficacy of early intervention in patients with asymptomatic severe AS (Table 18 andTable 19).
Table 18. Ongoing randomized clinical trials of early intervention in patients with aortic stenosis.
Clinical Trial (Unique Identifier)
N
Population
Intervention
Primary outcome
Follow-up period
Estimated Completion
Asymptomatic severe AS
ESTIMATE (NCT02627391)
360
Asymptomatic severe AS patients with normal exercise test, LVEF >50%, and low surgical risk
SAVR
All-cause mortality and cardiac morbidity+
1 year
Halted
EASY-AS (NCT04204915)
2844
Asymptomatic severe AS patients with LVEF ≥50%
SAVR/TAVI
Cardiovascular death and heart failure hospitalization
3 years
2029
DANAVR (NCT03972644)
1700
Asymptomatic severe AS and signs of increased left ventricular filling pressure or reduced longitudinal strain
SAVR/TAVI
All-cause death
5 years
2029
Moderate AS
PROGRESS (NCT04889872)
750
Moderate AS with symptoms or evidence of cardiac damage/dysfunction
TAVI
Death, stroke, and unplanned cardiovascular hospitalization
2 years
2029
EXPAND TAVR II (NCT05149755)
650
Moderate AS or evidence of cardiac damage/dysfunction
TAVI
All-cause death or unplanned procedure-related or aortic valve related hospitalization
2 years
2026
+: Any adverse cardiac event requiring hospitalization. Adverse cardiac events include: development of any symptom clearly related to AS (dyspnea, angina, pre-syncope or syncope during exercise); major adverse cardiac events defined as congestive heart failure or acute coronary syndrome; death of any cause, including cardiac death.
AS = aortic stenosis; AVA = aortic valve area; LVEF = left ventricular ejection fraction; SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
Table 19. Results of early intervention in patients with aortic stenosis.
Clinical Trial
N
Population
Intervention
Crossover in the clinical surveillance group
Primary outcome
Median F/U for primary outcome assessment
Early intervention
Clinical surveillance
Asymptomatic severe AS
RECOVERY
145
Asymptomatic very severe AS
SAVR 100%
74%
(median 700 days)
Operative mortality or death from cardiovascular causes
6.2 years
1%
15%
HR (95% CI) 0.09 (0.01-0.67)
AVATAR
157
Asymptomatic severe AS and no symptoms on treadmill stress test
SAVR 100%
44.3%
(median 476 days)
All-cause death, acute myocardial infarction, stroke, or unplanned hospitalization for heart
failure
32 months
15.22%
34.7%
HR (95% CI) 0.46 (0.23-0.90)
EARLY-TAVR
901
Asymptomatic severe AS with age ≥65 years and no symptoms on treadmill stress test
TAVI 100%
87.0%
(median 11.1 months)
All-cause mortality, stroke, and unplanned cardiac hospitalization
3.8 years
26.8%
45.3%
HR (95% CI) 0.50 (0.40-0.63)
EVOLVED-AS
224
Asymptomatic severe AS with evidence of midwall LGE
SAVR 75%
TAVI 25%
77%
(median 20.2 months)
All-cause mortality and unplanned AS-related hospitalization
41 months
18%
23%
HR (95% CI) 0.79 (0.44-1.43)
Moderate AS
TAVR UNLOAD
178
Moderate AS patients with reduced LVEF (<50%) and heart failure
TAVI 100%
43%
(median 12 months)
All-cause mortality, disabling stroke, rehospitalization, and change in KCCQ
23 months
47.6%*
36.6%*
Win ratio (95% CI) 1.31 (0.91-1.88)
*wins of patient pairs
AS = aortic stenosis; CI = confident interval; HR = hazard ratio; KCCQ = Kansas City Cardiomyopathy Questionnaire; LVEF = left ventricular ejection fraction: LGE = late gadolinium enhancement; SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
EARLY-TAVR was a randomized, controlled trial comparing transfemoral TAVI with the SAPIEN 3 or SAPIEN 3 Ultra balloon-expandable device to clinical surveillance in patients with asymptomatic severe AS with indications for clinical surveillance330. Genereux P, Schwartz A, Oldemeyer JB, et al. Transcatheter Aortic-Valve Replacement for Asymptomatic Severe Aortic Stenosis. N Engl J Med. 2025;392:217-227 Link. Asymptomatic status was determined by a negative treadmill stress test in 90.6% of patients. If a patient was unable to perform the stress test, eligibility was confirmed through detailed physician assessment of medical history. Between 2017 and 2021, 1,578 patients were screened and 677 (42.9%) were excluded from this trial. Among excluded patients, 313 (46.2%) were reclassified as having a class 1 indication for AVR, and the majority were confirmed to have symptomatic status by stress testing or more rigorous questioning. A total of 901 patients (mean age 76 years, 69% male, mean STS-PROM 1.8%) were randomly assigned to TAVI (N = 455) or clinical surveillance (N = 446). During a median follow-up of 3.8 years, the primary non-hierarchical composite endpoint of all-cause mortality, any stroke, or unplanned cardiovascular occurred in 122 patients (26.8%) in the TAVI group and in 202 patients (45.3%) in the clinical surveillance group (HR, 0.50; 95% CI, 0.40-0.63; P <0.001), primarily driven by guideline-directed conversions to AVR within 6 months in the clinical surveillance group. In addition, the prespecified secondary endpoint, including favourable outcome (alive and KCCQ overall score ≥75 that did not decrease by >10 points from baseline) at 2 years and the composite of integrated left ventricular health (absolute left ventricular global longitudinal strain ≥ 15%, left ventricular mass index < 115 g/m2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link for men or < 95 g/m2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link for women, and left atrial volume index ≤ 34 mL/m2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link) at 2 years, was higher in the TAVI group than in the clinical surveillance group, suggesting that clinical surveillance was associated with a decline in quality of life and the development of more cardiac damage. Of note, 87.0% of patients in the clinical surveillance group underwent AVR with a median time from randomization to conversion to AVR of 11.1 months (interquartile range: 5.0 to 19.7) and with a median time to the procedure from symptom onset or from the decision to intervene of 32 days (interquartile range: 18 to 58), and there were no apparent differences in procedure-related adverse events between patients in the TAVI group and those in the clinical surveillance group who underwent AVR330. Genereux P, Schwartz A, Oldemeyer JB, et al. Transcatheter Aortic-Valve Replacement for Asymptomatic Severe Aortic Stenosis. N Engl J Med. 2025;392:217-227 Link.
EVOLVED was a multicenter, randomized controlled trial to determine whether early AVR in asymptomatic patients with severe AS and evidence of midwall non-ischemic late gadolinium enhancement (LGE) on cardiac magnetic resonance (CMR) imaging improves prognosis331. Loganath K, Craig NJ, Everett RJ, et al. Early Intervention in Patients With Asymptomatic Severe Aortic Stenosis and Myocardial Fibrosis: The EVOLVED Randomized Clinical Trial. Jama. 2025;333:213-221 Link. The trial recruited asymptomatic patients with severe AS and preserved LVEF. At the screening visit, patients were evaluated for plasma high-sensitivity cardiac troponin I (hsTnI) concentrations and electrocardiogram. If there was evidence of left ventricular hypertrophy with strain or elevated hsTnI (an hsTnI concentration ≥6 ng/L), they proceeded to baseline CMR. A total of 224 patients with midwall LGE were enrolled and randomly allocated to the early intervention (N = 113) or the guideline-directed conservative management group (N = 111). Of 113 patients in the early intervention group, 107 (94%) underwent AVR (SAVR 75% and TAVI 25%) and 6 patients died prior to AVR during a median delay of 5.5 months. In the guideline-directed conservative management group, 85 patients (77%) underwent AVR (55% SAVR and 45% TAVI) at a median of 20.2 months. During a median follow-up of 42 months with a total follow-up of 722 patient-years, the primary composite end point of all-cause death or unplanned AS hospitalization occurred in 20 patients (18%) in the early aortic valve intervention group and 25 (23%) in the guideline-directed conservative management group (HR 0.79 [95% CI 0.44-1.43] between-group difference -4.82% [95% CI -15.31% to 5.66%]). For the secondary endpoints, early intervention was associated with a lower incidence of unplanned aortic stenosis hospitalization (6% vs. 17%, HR 0.37, 95% CI 0.16-0.88) and a lower 12-month rate of NYHA functional class II-IV symptoms than guideline-directed conservative management (19.7% vs. 37.9%; odds ratio 0.37, 95% CI 0.20-0.70). Of note, this trial was halted for 5 months due to the Covid-19 pandemic and the statistical plan was revised in light of the results of the RECOVERY and AVATAR trials331. Loganath K, Craig NJ, Everett RJ, et al. Early Intervention in Patients With Asymptomatic Severe Aortic Stenosis and Myocardial Fibrosis: The EVOLVED Randomized Clinical Trial. Jama. 2025;333:213-221 Link.
A meta-analysis of 4 RCTs investigating the effect of an early intervention strategy in patients with asymptomatic severe AS (1,427 patients and an average follow-up time of 4.1 years) reported that early AVR was associated with a significant reduction in unplanned cardiovascular or heart failure hospitalization (pooled rate 14.6% vs. 31.9%; HR: 0.40; 95% CI: 0.30-0.53; I2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link = 4%; P <0.01) and stroke (pooled rate 4.5% vs. 7.2%; HR: 0.62; 95% CI: 0.40-0.97; I2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link = 0%; P = 0.03), while there were no differences in all-cause (pooled rate 9.7% vs. 13.7%; HR: 0.68; 95% CI: 0.40-1.17; I2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link = 61%; P = 0.17) and cardiovascular mortality (pooled rate 5.1% vs. 8.3%; HR: 0.67; 95% CI: 0.35-1.29; I2. Litvack F, Jakubowski AT, Buchbinder NA, Eigler N. Lack of sustained clinical improvement in an elderly population after percutaneous aortic valvuloplasty. Am J Cardiol. 1988;62:270-275 Link = 50%; P = 0.23) between early AVR and clinical surveillance 332. Genereux P, Banovic M, Kang DH, et al. Aortic Valve Replacement vs Clinical Surveillance in Asymptomatic Severe Aortic Stenosis: A Systematic Review and Meta-Analysis. J Am Coll Cardiol. 2025;85:912-922 Link.
These results suggest that early intervention is not associated with an increased risk of periprocedural complications compared with delayed intervention, improves quality of life, and reduces unplanned hospitalizations in patients with asymptomatic severe AS. Although uncertainty remains regarding valve durability, this concern does not discourage an early intervention strategy in asymptomatic patients with severe AS, given that crossover in the clinical surveillance groups occurred within 1-2 years of randomization in most patients (Table 19). Conversely, a watchful waiting strategy may be justified in the absence of an increased risk of mortality as long as careful surveillance and timely intervention can be assured in the respective health care setting333. Iung B, Pierard L, Magne J, et al. Great debate: all patients with asymptomatic severe aortic stenosis need valve replacement. Eur Heart J. 2023;44:3136-3148 Link.
Moderate AS
Current guidelines recommend aortic valve intervention for moderate AS only in patients with indications for other cardiac surgery (Table 3). Observational data suggest that less than severe AS is associated with impaired prognosis, heart failure hospitalizations, and evidence of cardiac damage compared to patients without AS. In the National Echocardiographic Database of Australia, patients with moderate AS had higher 5-year all-cause and cardiovascular mortality compared with those without AS (61.4% vs. 18.6% and 43.0% vs. 10.4%, respectively). Similarly, data on 1,669,536 echocardiographic reports from 24 US hospitals reported that untreated moderate AS was associated with an increased risk of mortality compared with those without AS (adjusted HR 1.56, 95% CI 1.42-1.71)327. Genereux P, Sharma RP, Cubeddu RJ, et al. The Mortality Burden of Untreated Aortic Stenosis. J Am Coll Cardiol. 2023;82:2101-2109 Link. However, it has not been established whether moderate AS is an independent predictor of adverse outcomes or a surrogate marker for other prognostically relevant comorbidities. In a propensity score matched analysis of 262 pairs of patients with heart failure (LVEF <50%) alone versus heart failure and moderate AS, moderate AS was associated with an increased risk of mortality (HR 2.98; 95% CI: 2.08-4.31) and the composite of heart failure hospitalization and mortality (HR: 2.34; 95% CI: 1.72-3.21) during a median follow-up time of 2.9 years335. Jean G, Van Mieghem NM, Gegenava T, et al. Moderate Aortic Stenosis in Patients With Heart Failure and Reduced Ejection Fraction. J Am Coll Cardiol. 2021;77:2796-2803. Link. Furthermore, the additive negative prognostic value of moderate AS is more pronounced among patients with more advanced cardiac damage336. Amanullah MR, Pio SM, Ng ACT, et al. Prognostic Implications of Associated Cardiac Abnormalities Detected on Echocardiography in Patients With Moderate Aortic Stenosis. JACC Cardiovasc Imaging. 2021;14:1724-1737. Link. A retrospective analysis of 1,245 patients with moderate AS categorized into 5 groups according to the extent of extra-aortic valvular cardiac abnormalities demonstrated that there was a stepwise increase in all-cause mortality at 5 years according to increasing stages of cardiac damage, and advanced cardiac damage was associated with a progressively increasing risk of all-cause mortality compared with no cardiac damage (i.e., cardiac stage 0) 336. Amanullah MR, Pio SM, Ng ACT, et al. Prognostic Implications of Associated Cardiac Abnormalities Detected on Echocardiography in Patients With Moderate Aortic Stenosis. JACC Cardiovasc Imaging. 2021;14:1724-1737. Link. These observations raise the question whether aortic valve intervention for moderate AS may have a prognostic benefit, particularly in patients with impaired cardiac function.
The TAVR UNLOAD trial was the first RCT to evaluate the treatment of moderate AS in patients with reduced LVEF ranging between 20% and 50%337. Van Mieghem NM, Elmariah S, Spitzer E, et al. Transcatheter Aortic Valve Replacement in Patients With Systolic Heart Failure and Moderate Aortic Stenosis: TAVR UNLOAD. J Am Coll Cardiol. 2025;85:878-890 Link. Conducted between January 2017 and December 2022, the trial enrolled 178 patients (mean age: 77 years; 20.8% female; 55.6% in NYHA functional class III or IV). Participants were randomized to early intervention with transfemoral TAVI using a balloon-expandable valve (N = 89) or clinical surveillance (N = 89). The primary endpoint was a hierarchical composite of: 1) all-cause mortality, 2) disabling stroke, 3) disease-related hospitalizations or heart failure equivalents, and 4) changes from baseline in KCCQ overall summary score, analysed using the win ratio. Over a median follow-up of 23 months, 38 patients (43%) in the clinical surveillance group underwent TAVI with a median crossover time of 12 months. For the primary endpoint, early TAVI resulted in wins in 47.6% of patient pairs, compared with 36.6% in the clinical surveillance group, yielding a win ratio of 1.31 (95% CI: 0.91-1.88; P = 0.14) (Table 19). At 1 year, early TAVI demonstrated superiority in the ranked ordinal comparison (48% vs. 30.9%; win ratio: 1.55; 95% CI: 1.04-2.31), primarily driven by improvements in the KCCQ overall summary score. It is noteworthy that the trial design was adapted reducing the initially planned enrolment of 600 patients to 178 due to slow recruitment and funding limitations. Moreover, while the original study design specified a primary analysis at 1 year, the extended follow-up period, combined with a 43% crossover rate in the clinical surveillance arm at a median of 12 months, may have diluted the ability to observe early clinical benefits, 337. Van Mieghem NM, Elmariah S, Spitzer E, et al. Transcatheter Aortic Valve Replacement in Patients With Systolic Heart Failure and Moderate Aortic Stenosis: TAVR UNLOAD. J Am Coll Cardiol. 2025;85:878-890 Link338. Genereux P, Gupta A, Makkar RR. TAVR in Patients With Moderate Aortic Stenosis and Heart Failure. J Am Coll Cardiol. 2025;85:891-893 Link.
Currently, two RCTs - PROGRESS (NCT04889872) and EXPAND TAVR II (NCT05149755) - are ongoing to evaluate whether early intervention by means of TAVI improves clinical outcomes in patients with moderate AS and evidence of heart failure or cardiac damage (Table 18). These trials will determine whether earlier aortic valve intervention can improve clinical outcomes beyond the current strategy of optimal medical therapy alone.
Bicuspid aortic valve
The cumulative evidence of TAVI was obtained in well-selected patients with tricuspid aortic valve stenosis, excluding those with bicuspid aortic valve lesions. Bicuspid aortic valve is the most prevalent congenital heart condition in adults and is associated with early progression of valve deterioration, leading to the development of aortic valve disease requiring intervention in 80% of patients with bicuspid aortic valve over their lifetime, 34. Yang LT, Ye Z, Wajih Ullah M, et al. Bicuspid aortic valve: long-term morbidity and mortality. Eur Heart J. 2023;44:4549-4562 Link339. Vincent F, Ternacle J, Denimal T, et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation. 2021;143:1043-1061 Link. Approximately 20% of patients undergoing SAVR aged 65-79 years and 5% of patients aged 80 years or older have bicuspid morphology340. Mehta CK, Liu TX, Bonnell L, et al. Age-Stratified Surgical Aortic Valve Replacement for Aortic Stenosis. Ann Thorac Surg. 2024;118:430-438 Link, and therefore it is natural that TAVI is increasingly tested also in patients with bicuspid AS (Table 20).
Table 20. TAVI for bicuspid aortic stenosis.
Study
N (total)
Device
Age (years)
Male
STS-PROM
BAV type (Siever classification)
Post procedure ≥mod PVR
Clinical outcomes
Follow-up
All-cause mortality
Stroke
TAVI in bicuspid valve
Wijesinghe et al. (2010)
11
BEV 100%
73.2 ± 12.5
55%
4.4 ± 2.6
NA
27%
30 days
18%
NA
Himbert et al. (2012)
15
SEV 100%
80 ± 10
80%
8 ± 5
Type 0: 13% Type I: 67% Unknown: 20%
13.3%
30 days
7%
0%
Mylotte et al. (2014)
139
BEV 34.5% SEV 65.5%
78.0 ± 8.9
56.1%
4.9 ± 3.4
Type 0: 27% Type I: 68% Type II: 5%
34%
30 days
5.0%
2.2%
1 year
17.5%
NA
Yousef et al. (2015)
108
BEV 56% SEV 44%
75.5 ± 14.4
63.9%
17.2 ± 12.2
Type 0: 12% Type I: 53% Type II: 7% Unknown: 28%
31%
30 days
8.3%
2.8%
1 year
16.9%
NA
Kosek et al. (2015)
7
BEV 29% SEV 71%
77.7 (72–85)
43%
NA
NA
28%
30 days
14%
0%
Perlman et al. (2016)
51
BEV 100%
76.2 ± 9.3
47.1%
5.2 ± 3.7
Type 0: 11.8% Type I: 74.4% Type II: 1.9% Unknown: 11.6%
0%
30 days
3.9%
1.9%
Yoon et al. (2016)
301
BEV 59% SEV 37% MEV 4%
77.0 ± 9.2
57.5%
4.7 ± 5.2
Type 0: 10.3% Type I: 74.4% Type II: 1.7% Unknown: 13.6%
6%
30 days
4.3%
2.3%
1 year
14.4%
NA
Jilaihawi et al. (2016)
130
BEV 54% SEV 46%
76.6 ± 10.4
61.5%
4.7 (3.0-7.3)
Type 0: 20.9% Type I: 54.9% Type II: 0% Unknown: 24.2%
18%
30 days
3.8%
3.3%
Yoon et al. (2017)
108
BEV 100%
74.4 ± 10.6
71.3%
5.2 ± 3.4
Type 0: 6% Type I: 94%
6%
30 days
0.9%
4.6%
1 year
6.9%
NA
Liu et al. (2018)
12
SEV 100%
76 ± 4
67%
6.86 ± 4.27
Type 0: 67% Type I: 33%
0%
30 days
0%
8%
Kim et al. (2018)
144
BEV 63% SEV 32% MEV 5%
NA
NA
NA
Type 0: 4.2% Type I complete raphe: 41.7% Type I partial raphe: 54.1%
11.1%
30 days
4.9%
NA
Mangieri et al. (2018)
353
BEV 68.6% SEV 31.4%
77.8 ± 8.3
64.9%
4.4 ± 3.3
Type 0: 7.1% Type I: 61.8% Type II: 0.9% Unknown: 29.8%
4.0%
30 days
4.3%
1.6%
Attinger-Toler et al. (2019)
79
BEV 100%
76 ± 9
56%
3.8 (2.3–5.5)
Type 0: 6% Type I L-R: 65% Type I R-N: 14% Type I L-N: 2% Type II: 5% Unknown: 8%
5%
30 days
3.8%
1.3%
1 year
7.7%
1.3%
Lei et al. (2019)
71
SEV 77.5% MEV 22.5%
71.9 ± 5.8
45.1%
7.0 ± 3.6
Type 0: 100%
0%
30 days
7.0%
4.2%
1 year
8.5%
NA
Weir-McCall et al. (2019)
44
BEV 100%
75 ± 10
59%
4.3 ± 2.3
Type 0: 5% Type I L-R: 77% Type I R-N: 18% Type I L-N: 0% Type II: 0%
0%
1 year
8.9%
NA
LRT trial Bicuspid Arm (2019)
61
BEV 74% SEV 26%
68.6 ± 7.4
42.6%
1.5 ± 0.6
Type 0: 13.3% Type I: 78.3% Type II: 3.3%
2.0%
30 days
0%
1.6%
Mangieri et al. (2020)
353
BEV 68.6% SEV 31.4%
77.8 ± 8.3
64.9%
4.4 ± 3.3
Type 0: 7.1% Type I: 61.8% Type II: 0.9% Unknown: 29.8%
4.0%
30 days
4.3%
1.6%
Yoon et al. (2020)
1034
BEV 71.6% SEV 23.9% MEV 4.5%
74.7 ± 9.3
59%
3.7 ± 3.3
Type 0: 10.3% Type I: 89.7%
5.2% (≥Mild-moderate)
30 days
2.0%
NA
2 years
12.5%
2.7%
Kochman et al. (2020)
24
MEV 100%
75.3 ± 7.85
50%
13.4 ± 10.39*
Type 0: 8% Type I: 75% Type II: 0% Functional: 8% Unknown: 8%
4%
30 days
4%
4%
2 years
12.5%
4.2%
Attinger-Toller et al. (2020)
79
BEV 100%
76 ± 9
56%
3.8 (2.3–5.5)
Type 0: 6% Type I: 81% Type II: 5% Unknown: 8%
0%
30 days
3.8%
1.3%
1 year
7.7%
1.3%
Gorla et al. (2021)
56
SEV 73.2% MEV 26.8%
75.5 ± 12.4
62%
3.4 ± 2.1
NA
14%
30 days
4%
2%
Ielasi et al. (2021)
243
BEV 70% SEV 30%
80 ± 7.9
67.1%
3.5 ± 4.6
Type 0: 10.3% Type I: 89.7%
4.1%
30 days
4%
1.4%
1 year
9.8%
7.3%
Kumar et al. (2022)
70
BEV 30% SEV 70%
72 ± 8.49
68.6%
6.00 ± 6.54
Type 0: 21% Type I: 78%
0%
30 days
2.86%
0%
2 year
2.86%
0%
Elkoumy et al. (2022, 2023)
68
BEV 100%
72.6 ± 9.4
72%
3.54 ± 2.1
Type 0: 19% Type I: 74% Type II: 7%
3%
30 days
3.0%
0%
1 year
11.3%
3.2%
Tchétché et al. (2023)
149
SEV 100%
78
63.1%
2.6 (1.7-4.2)
Type 0: 10.1% Type I: 72.5% Type II: 3.3%
11.3% (≥Mild-moderate)
1 year
10%
4%
Li et al. (2023)
156
SEV 100%
71.6 ± 6.8
64.7%
2.1 (1.5–3.7)
NA
6.0%
30 days
2.6%
0.6%
Deutsch et al. (2023)
106
BEV 64% SEV 36%
NA
65%
2.6
Type 0: 7.5% Type I: 92.5% Type II: 0%
0%
30 days
0.9%
2.8%
Fiorina et al. (2023)
109
BEV 31.2% SEV 56% MEV 12.8%
78 ± 7.5
49.5%
5.1 ± 4.3
NA
13.1%
4 years
32%
NA
Boiago et al. (2023)
150
BEV 55.3% SEV 44.7%
81.4 ± 7.5
67.3%
5.4 ± 6.4
Type 0: 6.7% Type I: 92.7% Type II: 0.7%
9.9%
30 days
3.4%
2%
3 years
28.1%
9.6%
Evolut Low Risk Bicuspid Study (2020, 2021, 2024)
150
SEV 100%
70.3±5.5
52.0%
1.3 (0.9, 1.7)
Type 0 9.3% Type 1 90.7% Type 2 0%
0%
30 days (N = 50)
0.7%
4.0%
1 year
0.7%
4.7%
2 years
2.1%
6.1%
3 years
2.8%
6.9%
TAVI in bicuspid vs. tricuspid valves
Hayashida et al. (2013)
21 (229)
BEV 52% SEV 48%
82.0 ± 7.0
57.1%
NA
Type I: 86% Type II: 14%
19%
30 days
7.9%
NA
Bauer et al. (2014)
38 (1395)
BEV 32% SEV 68%
80.7 ± 6.6
45%
18 ± 10*
NA
25%
30 days
11%
0%
1 year
13%
0%
Costopoulos et al. (2014)
21 (468)
BEV 38% SEV 62%
76.7 ± 7.1
57%
7.6 ± 4.2
NA
24%
30 days
14%
0%
1 year
32%
NA
Kochman et al. (2014)
28 (112)
BEV 15% SEV 85%
77.6 ± 5.5
46%
19.2 ± 9.0*
NA
32%
30 days
4%
0%
1 year
18%
NA
Liu et al. (2015)
15 (40)
SEV 100%
75.4 ± 5.7
60%
5.6 ± 4.1
Type 0: 73% Type I: 27% Type II: 0%
0%
30 days
6.7%
6.7%
Yoon et al.† (2017)
546 (1092)
BEV 58% SEV 34% MEV 8%
77.2 ± 8.2
62.8%
4.6 ± 4.6
Type 0: 11% Type I: 75% Type II: 1% Unknown: 13%
10%
30 days
3.7%
2.9%
Arai et al. (2017)
10 (153)
BEV 100%
81.3 ± 5.1
43%
19.0 ± 12.5*
Type I: 90% Type II: 10%
0%
30 days
0%
0%
Sannino et al. (2017)
88 (823)
BEV 52% SEV 48%
80.2 ± 8.4
60.2%
7.4 ± 3.9
Type 0: 14% Type I: 85% Type II: 1%
5%
30 days
3.4%
2.3%
1 year
8.5%
NA
Song et al. (2018)
44 (97)
SEV 100%
73.8 ± 5.2
54.5%
5.0 (3.8–8.2)
Type 0: 50% Type I complete raphe: 45% Type I partial raphe: 5%
11.4%
30 days
6.8%
2.3%
2 years
11.4%
NA
Aalaei-Andabili et al. (2018)
32 (128)
BEV 78% SEV 22%
68.59 ± 11.07
66.7%
6.01 ± 3.42
Type 0: 75% Type I: 12.5% Type II: 6.25% Unknown: 6.25%
3%
30 days
6.25%
6.2%
2 years
14%
6.2%
Liao et al. (2018)
87 (157)
SEV 100%
73.4 ± 6.4
57.5%
7.9 ± 4.0
Type 0: 56% Type I: 44%
14%
30 days
9.2%
1.1%
Nagaraja et al.† (2019)
359 (718)
NA
68.01 ± 13.42
34.83%
NA
NA
NA
In-hospital
5.57%
2.79%
Tchetche et al. (2019)
101 (189)
BEV 65.3% SEV 28.8% MEV 9.9%
78.2 ± 10.1
65%
11.3 ± 8.5
Type 0: 12.9% Type I: 86.1% Type II: 1%
20.8% (Mild-moderate)
30 days
0%
2%
Makkar et al.† (2019)
2691 (5382)
BEV 100%
74 (66-81)
60.3%
4.9 ± 4.0
NA
2.0%
30 days
2.6%
2.5%
1 year
10.5%
3.4%
LRT trial Bicuspid Arm† (2019)
50 (100)
BEV 74% SEV 26%
68.6 ± 7.4
42.6%
1.5 ± 0.6
Type 0: 13.3% Type I: 78.3% Type II: 3.3%
2.0%
30 days
0%
1.6%
Harim et al. (2020)
5412 (170959)
BEV 81.1% SEV 18.9%
74.0 (65.0–81.0)
59.1%
3.8 (2.3–6.1)
NA
4.4%
In-hospital
2.0%
2.2%
Forrest et al.† (2020)
929 (1858)
SEV 100%
73.0 ± 10.3
55.1%
5.3 ± 4.2
NA
2.2%
30 days
2.6%
3.4%
1 year
10.4%
3.9%
Pineda et al. (2020)
50 (567)
BEV 38% SEV 62%
70 (64-74)
64%
4.6 (3.0-7.7)
Type 0: 14.0% Type I: 86.0%
4.0%
30 days
6.0%
2.0%
2 years
18.0%
NA
Fu et al. (2020)
44 (118)
SEV 100%
73.57 ± 6.30
52.3%
6.70 ± 2.95
NA
11.4%
30 days
4.5%
2.3%
1 year
13.6%
6.8%
Chodór et al. (2021)
21 (83)
SEV 100%
75.76 ±7.96
66.67%
21.63 ±11.49
NA
14.28%
30 days
4.76%
0%
1 year
28.57%
0%
Makkar et al.† (2021)
3168 (6336)
BEV 100%
68.8 ± 8.7
69.2%
1.7 ± 0.6
NA
1.8%
30 days
0.9%
1.4%
1 year
4.6%
2.0%
Michel et al. (2021)
78 (743)
BEV 100%
77 , 68. Reardon M. One year Outcomes of ACURATE neo2 vs Approved TAVR Devices in All risk Patients with Severe AS: the ACURATE IDE Trial. TCT 2024 October 30, 2024. Washington, DC Link80. Alqahtani F, Aljohani S, Ghabra A, et al. Outcomes of Transcatheter Versus Surgical Aortic Valve Implantation for Aortic Stenosis in Patients With Hepatic Cirrhosis. Am J Cardiol. 2017;120:1193-1197 Link
Type 0: BEV 5.2%, SE 94.8% Type I: BEV 8.9%, SEV 91.1%
Type 0: 73.04 ± 5.97 Type I: 72.51 ± 8.03
Type 0: 62.8% Type I: 62.8%
Type 0: 5.16 ± 3.94 Type I: 4.97 ± 4.41
NA
Type 0: 13.2% Type I: 14.5%
30 days
Type 0: 4.2% Type I: 1.7%
Type 0: 1.0% Type I: 0.9%
1 year
Type 0: 10.0% Type I: 2.3%
Type 0: 1.4% Type I: 1.6%
Magyari et al.† (2023)
52 (104)
BEV 100%
71 ± 7.1
65.4%
5.2 ± 3.3
NA
NA
30 days
0%
1.9%
TAVI vs. SAVR in bicuspid valve
Elbadawi et al.† (2019)
975 (1950)
NA
65.70 ± 16.53
60%
NA
NA
NA
In-hospital
3.1%
2.1%
Soud et al.† (2020)
68 (136)
NA
65.0 ± 14.8
67.6%
NA
NA
NA
In-hospital
5.9%
NA
Mentias et al.† (2020)
699 (1398)
NA
74.7 ± 9.4+
NA
NA
NA
NA
30 days
2.9%
4.0%
1 year
9.0%
4.0%
Tsai et al. (2021)
48 (130)
NA
65.7 ± 7.8
58.3%
6.25 ± 6.4
NA
NA
In-hospital
12.5%
2%
Majmundar et al.† (2022)
1393 (2786)
NA
68.3 ± 10.1
62.2%
NA
NA
NA
30 days
0.3%
0.1%
6 months
0.4%
0.1%
Sanaiha et al.† (2023)
3855 (56331)
NA
69 (62-76)
61.2%
NA
NA
NA
In-hospital
1.6%
0.8%
Chen et al.† (2023)
797 (1594)
NA
73 (69-77)
58.2%
NA
NA
NA
3 years
25.4%
NA
NOTION-2 Bicuspid cohort (2024)
49 (100)
BEV 28.5% SEV 67.3% MEV 4.1%
69.7 ± 3.6
55.1%
1.0 (0.8-1.3)
Type 0: 6.1% Type I: 91.8% Type II: 2.1%
9.1% (at 1 year)
1 year
4.1%
6.1%
Post procedural PVR was evaluated at discharge or 30 days.
†Matched cohort. +Entire cohort. *EuroSCORE.
BEV = balloon expandable valve; MEV = mechanically-expanding valve; PVR = paravalvular regurgitation; SAVR = surgical aortic valve replacement; SEV = self-expanding valve; STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality; TAVI = transcatheter aortic valve implantation.
Bicuspid valve morphology may pose a technical challenge for TAVI due to anatomical specifications, including a non-circular aortic root, more severe and asymmetric distribution of leaflet calcification, presence of 1 or 2 raphes with variable degree of calcification and associated aortopathy (Figure 32), 116. Windecker S, Okuno T, Unbehaun A, et al. Which patients with aortic stenosis should be referred to surgery rather than transcatheter aortic valve implantation. Eur Heart J. 2022;43:2729-2750 Link339. Vincent F, Ternacle J, Denimal T, et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation. 2021;143:1043-1061 Link. Indeed, early experience with TAVI in patients with severe bicuspid AS has highlighted an increased risk of procedural complications and lower device success compared with TAVI in patients with tricuspid AS341. Yoon SH, Bleiziffer S, De Backer O, et al. Outcomes in Transcatheter Aortic Valve Replacement for Bicuspid Versus Tricuspid Aortic Valve Stenosis. J Am Coll Cardiol. 2017;69:2579-2589 Link. Device advances, increasing operator experience, and careful patient selection based on the systematic use of preprocedural MDCT for the assessment of aortic valve and root morphology have improved procedural success and device performance with TAVI in patients with bicuspid AS. The STS/ACC TVT registry reported comparable rates of device success, bioprosthetic valve haemodynamics, and 1-year clinical outcomes using newer-generation devices (balloon-expandable SAPIEN 3 and self-expanding Evolut R or PRO devices) in selected patients with bicuspid compared with tricuspid AS, 342. Makkar RR, Yoon SH, Leon MB, et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. Jama. 2019;321:2193-2202 Link343. Forrest JK, Kaple RK, Ramlawi B, et al. Transcatheter Aortic Valve Replacement in Bicuspid Versus Tricuspid Aortic Valves From the STS/ACC TVT Registry. JACC Cardiovasc Interv. 2020;13:1749-1759 Link. However, even with TAVI using newer-generation devices, bicuspid morphology remained associated with a higher risk of peri-procedural stroke and significant PVR, 342. Makkar RR, Yoon SH, Leon MB, et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke. Jama. 2019;321:2193-2202 Link344. Halim SA, Edwards FH, Dai D, et al. Outcomes of Transcatheter Aortic Valve Replacement in Patients With Bicuspid Aortic Valve Disease: A Report From the Society of Thoracic Surgeons/American College of Cardiology Transcatheter Valve Therapy Registry. Circulation. 2020;141:1071-1079 Link. Furthermore, a core laboratory MDCT analysis in a multinational registry of 1,034 bicuspid AS patients undergoing TAVI, identified calcified raphe and excess leaflet calcification in bicuspid aortic valve as the risk factors for procedural complications and mid-term mortality after TAVI using current-generation devices345. Yoon SH, Kim WK, Dhoble A, et al. Bicuspid Aortic Valve Morphology and Outcomes After Transcatheter Aortic Valve Replacement. J Am Coll Cardiol. 2020;76:1018-1030 Link.
Figure 32
Anatomical risk stratification of bicuspid aortic valve. Figures reproduced from Windecker et al. Eur Heart J 2022;43(29):2729-2750.
Consistent with TAVI for tricuspid AS, evidence has accumulated to support the feasibility of TAVI in low-risk patients with bicuspid AS. The STS/ACC TVT registry provided data from a propensity score-matched analysis of 3,168 bicuspid and tricuspid AS pairs undergoing TAVI with the SAPIEN 3 balloon-expandable device (mean age 69 years; 69.8% men; mean STS-PROM 1.7%) and reported no significant differences in procedural complications, bioprosthetic performance, and clinical outcomes at 30 days and 1 year346. Makkar RR, Yoon SH, Chakravarty T, et al. Association Between Transcatheter Aortic Valve Replacement for Bicuspid vs Tricuspid Aortic Stenosis and Mortality or Stroke Among Patients at Low Surgical Risk. Jama. 2021;326:1034-1044 Link. Similar findings have been reported in the bicuspid registries from the pivotal low-risk randomized clinical trials. In the PARTNER 3 bicuspid registry (N = 148, mean age 71 years; 58.1% men; mean STS-PROM 1.4%), patients with bicuspid AS treated with SAPIEN 3 balloon-expandable device had similar procedural success (100% vs. 99.3%) and 1-year clinical outcomes (death: 0.7% vs. 1.4%; stroke: 2.1% vs. 2.0%; cardiovascular rehospitalization: 9.6% vs. 9.5%) compared to patients with tricuspid AS in a propensity score matching analysis347. Williams MR, Jilaihawi H, Makkar R, et al. The PARTNER 3 Bicuspid Registry for Transcatheter Aortic Valve Replacement in Low-Surgical-Risk Patients. JACC Cardiovasc Interv. 2022;15:523-532 Link. The Evolut Low Risk Bicuspid Study provides the longest-term prospective follow-up data on 150 low-risk patients with bicuspid AS undergoing TAVI with the self-expanding Evolut R or PRO device (mean age: 70.3 years, median STS-PROM: 1.3%). Periprocedural outcomes were favourable with device success rate of 95.3% and no ≥moderate PVR, and 30-day mortality and disabling stroke were rare (both occurred in 1 patient)348. Forrest JK, Ramlawi B, Deeb GM, et al. Transcatheter Aortic Valve Replacement in Low-risk Patients With Bicuspid Aortic Valve Stenosis. Jama. Cardiol 2021;6:50-57 Link. A propensity-score matched comparison of this group with the TAVR cohort of the Evolut Low Risk randomized trial reported no relevant differences in clinical and bioprosthetic haemodynamics at 1 year between the bicuspid and tricuspid anatomies349. Deeb GM, Reardon MJ, Ramlawi B, et al. Propensity-Matched 1-Year Outcomes Following Transcatheter Aortic Valve Replacement in Low-Risk Bicuspid and Tricuspid Patients. JACC Cardiovasc Interv. 2022;15:511-522 Link. At 3 years, the composite of all-cause death or disabling stroke, all-cause death, disabling stroke, and aortic valve hospitalization occurred in 4.1%, 2.8%, 2.1%, and 5.4% of patients, respectively, and bioprosthetic haemodynamic properties were sustained with 15% mild PVR and no moderate or greater PVR350. Zahr F, Ramlawi B, Reardon MJ, et al. 3-Year Outcomes From the Evolut Low Risk TAVR Bicuspid Study. JACC Cardiovasc Interv. 2024;17:1667-1675 Link. These data suggest that TAVI is feasible in younger, low-risk patients with bicuspid aortic valve morphology taking into consideration that the low-risk bicuspid populations were highly selected with strict anatomical exclusion criteria for relevant device landing zone calcification evaluated by a review committee, as well as the exclusion of patients with concomitant relevant valvular or coronary artery disease, , 347. Williams MR, Jilaihawi H, Makkar R, et al. The PARTNER 3 Bicuspid Registry for Transcatheter Aortic Valve Replacement in Low-Surgical-Risk Patients. JACC Cardiovasc Interv. 2022;15:523-532 Link350. Zahr F, Ramlawi B, Reardon MJ, et al. 3-Year Outcomes From the Evolut Low Risk TAVR Bicuspid Study. JACC Cardiovasc Interv. 2024;17:1667-1675 Link351. Waksman R, Craig PE, Torguson R, et al. Transcatheter Aortic Valve Replacement in Low-Risk Patients With Symptomatic Severe Bicuspid Aortic Valve Stenosis. JACC Cardiovasc Interv. 2020;13:1019-1027 Link.
Several uncertainties remain in patients with bicuspid AS who are candidates for TAVI352. Windecker S, Tomii D. Transcatheter Aortic Valve Replacement in Patients With Bicuspid Aortic Stenosis: Cumulative Evidence and Remaining Uncertainties. JACC Cardiovasc Interv. 2024;17:1676-1679 Link: 1) definition of favourable and unfavourable bicuspid aortic valve morphology339. Vincent F, Ternacle J, Denimal T, et al. Transcatheter Aortic Valve Replacement in Bicuspid Aortic Valve Stenosis. Circulation. 2021;143:1043-1061 Link; 2) optimal device selection and sizing strategy353. Tchetche D, de Biase C, van Gils L, et al. Bicuspid Aortic Valve Anatomy and Relationship With Devices: The BAVARD Multicenter Registry. Circ Cardiovasc Interv. 2019;12:e007107 Link; 3) long-term TAVI durability and evolution of aortopathy after TAVI354. Jia Y, Tirado-Conte G, Montarello N, et al. Prognostic Impact of Ascending Aortic Dilatation in Bicuspid TAVR Patients. JACC Cardiovasc Interv. 2023;16:3057-3059 Link. Current clinical guidelines recommend SAVR as the preferred treatment strategy in patients with bicuspid aortic valve morphology (Table 21).
Table 21. Guideline recommendations: Mode of intervention in patients with bicuspid aortic stenosis.
2020 AHA/ACC Valvular Heart Disease Guideline
2021 ESC/EACTS Valvular Heart Disease Guideline
COR
LOE
Recommendation
COR
LOE
2b
B-NR
In patients with bicuspid aortic valve and symptomatic, severe AS, TAVI may be considered as an alternative to SAVR after consideration of patient-specific procedural risks, values, trade-offs, and preferences, and when the surgery is performed at a Comprehensive Valve Center.
Bicuspid aortic valve is an anatomical factor that favors SAVR.
NA
SAVR remains more appropriate in patients with AS affecting a bicuspid valve and in those with associated disease (e.g. aortic root dilatation, complex coronary disease, or severe mitral regurgitation) requiring a surgical approach.
NA
ACC/AHA = American College of Cardiology/American Heart Association; AS = aortic stenosis; COR = class of recommendation; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; LOE = Level of evidence; SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
The available evidence on the safety and efficacy of TAVI comparing SAVR is mainly limited to observational studies, , 355. Elbadawi A, Saad M, Elgendy IY, et al. Temporal Trends and Outcomes of Transcatheter Versus Surgical Aortic Valve Replacement for Bicuspid Aortic Valve Stenosis. JACC Cardiovasc Interv. 2019;12:1811-1822 Link356. Mentias A, Sarrazin MV, Desai MY, et al. Transcatheter Versus Surgical Aortic Valve Replacement in Patients With Bicuspid Aortic Valve Stenosis. J Am Coll Cardiol. 2020;75:2518-2519 Link357. Chen Q, Malas J, Megna D, et al. Bicuspid aortic stenosis: National three-year outcomes of transcatheter versus surgical aortic valve replacement among Medicare beneficiaries. J Thorac Cardiovasc Surg. 2024;168:1035-1044.e17 e1017 Link. The NOTION-2 trial is the only randomized trial comparing TAVR and SAVR in patients aged ≤75 years at low surgical risk that did not exclude patients with bicuspid aortic valve morphology. The bicuspid substudy comprised 100 patients (49 TAVI and 51 SAVR), and patients in the bicuspid arm were younger and less likely to have comorbidities compared to patients in the tricuspid arm. At 1 year, the primary endpoint (death from any cause, stroke, or rehospitalization) was higher in the TAVI group than in the SAVR group (14.3% vs. 3.9%), primarily driven by higher rates of stroke (6.1% vs. 0%)22. Jorgensen TH, Thyregod HGH, Savontaus M, et al. Transcatheter aortic valve implantation in low-risk tricuspid or bicuspid aortic stenosis: the NOTION-2 trial. Eur Heart J. 2024;45:3804-3814 Link. Although the sample size of the bicuspid cohort in the NOTION-2 was small and underpowered to determine the optimal strategy in this population, these data suggest that the results of TAVI in tricuspid AS may not be generalizable to patients with bicuspid AS. Currently, dedicated randomized trials comparing TAVI with SAVR in this specific setting with long-term follow-up are in the preparation phase. These trials will provide evidence-based data to inform future guideline recommendations358. Nuyens P, De Backer O, Sathananthan J, et al. TAVR in Bicuspid Aortic Stenosis: Current Evidence and Proposal for a Randomized Controlled Trial Design. JACC Cardiovasc Interv. 2023;16:1682-1687 Link. In the meantime, Heart Teams need to provide a tailored approach for individual patients with bicuspid AS based on the patient’s risk profile, comorbidities, anatomical considerations, and life expectancy.
Emergent TAVI
Patients with severe AS may present with acute decompensated heart failure or cardiogenic shock, a critical clinical status with poor short-term prognosis. Although SAVR has been considered in these patients, the surgical approach has been associated with an increased risk of perioperative mortality in the emergent and/or acute setting359. Piérard S, de Meester C, Seldrum S, et al. Impact of preoperative symptoms on postoperative survival in severe aortic stenosis: implications for the timing of surgery. Ann Thorac Surg. 2014;97:803-809 Link. As a result, TAVI has gained increasing attention in the emergent/urgent setting (emergent/urgent TAVI) as a viable therapeutic option among patients with acute decompensated heart failure or cardiogenic shock. Results of patients undergoing emergent TAVI have been consistent, indicating technical feasibility but an increased risk of short-term mortality, , , , , , , 360. Tomii D, Pilgrim T, Windecker S. Emergency transcatheter aortic valve implantation: expanding indication and concern of delayed treatment of aortic stenosis. Eur Heart J. Acute Cardiovasc Care 2022;11:887-890 Link361. Frerker C, Schewel J, Schlüter M, et al. Emergency transcatheter aortic valve replacement in patients with cardiogenic shock due to acutely decompensated aortic stenosis. EuroIntervention. 2016;11:1530-1536 Link362. Landes U, Orvin K, Codner P, et al. Urgent Transcatheter Aortic Valve Implantation in Patients With Severe Aortic Stenosis and Acute Heart Failure: Procedural and 30-Day Outcomes. Can J Cardiol. 2016;32:726-731 Link363. Kolte D, Khera S, Vemulapalli S, et al. Outcomes Following Urgent/Emergent Transcatheter Aortic Valve Replacement: Insights From the STS/ACC TVT Registry. JACC Cardiovasc Interv. 2018;11:1175-1185 Link364. Elbadawi A, Elgendy IY, Mentias A, et al. Outcomes of urgent versus nonurgent transcatheter aortic valve replacement. Catheter Cardiovasc Interv. 2020;96:189-195 Link365. Enta Y, Miyasaka M, Taguri M, et al. Patients' characteristics and mortality in urgent/emergent/salvage transcatheter aortic valve replacement: insight from the OCEAN-TAVI registry. Open Heart. 2020;7:e001467 Link366. Masha L, Vemulapalli S, Manandhar P, et al. Demographics, Procedural Characteristics, and Clinical Outcomes When Cardiogenic Shock Precedes TAVR in the United States. JACC Cardiovasc Interv. 2020;13:1314-1325 Link367. Steffen J, Stocker A, Scherer C, et al. Emergency transcatheter aortic valve implantation for acute heart failure due to severe aortic stenosis in critically ill patients with or without cardiogenic shock. Eur Heart J. Acute Cardiovasc Care 2022;11:877-886 Link. A recent analysis from the STS/ACC TVT registry including 309,505 patients undergoing TAVI with a balloon-expandable device reported that 5,006 patients (1.6%) presented with cardiogenic shock (defined according to registry coding data, pre-procedural use of inotropic or mechanical circulatory support, and/or cardiac arrest within 24 hours prior to the procedure) prior to TAVI and that VARC-3 technical success rate was 95%. In a propensity-matched analysis, TAVI in the setting of cardiogenic shock was associated with an increased risk of in-hospital (9.9% vs. 2.7%), 30-day (12.9% vs. 4.9%), and 1-year (29.7% vs. 22.6%) mortality compared with the control cohort. Using landmark analyses, the adverse impact of emergent TAVI associated with the critically ill clinical status was limited to the first 30 days after TAVI, whereas there were no significant differences between groups during the time period between 30 days and 1 year of follow-up. In addition, there was significant improvement in functional status among patients surviving after the procedure368. Goel K, Shah P, Jones BM, et al. Outcomes of transcatheter aortic valve replacement in patients with cardiogenic shock. Eur Heart J. 2023;44:3181-3195 Link. These results suggest that patients with severe AS who are critically ill due to acute decompensation or cardiogenic shock are potential candidates for emergent TAVI in the absence of severe comorbidities.
Native Valve Aortic regurgitation
Aortic regurgitation (AR) is another aortic valve disease entity associated with relevant morbidity and mortality. In the OxVALVE population cohort study of 2,500 individuals aged ≥65 years representing a primary care population, the prevalence of any and moderate or severe AR was 15% and 1.6%, respectively29. d'Arcy JL, Coffey S, Loudon MA, et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur Heart J. 2016;37:3515-3522 Link. Patients with significant AR are asymptomatic for a long period of time, although AR results in severe left ventricular volume and pressure overload, leading to detrimental structural and functional remodeling associated with poor survival, 369. Dujardin KS, Enriquez-Sarano M, Schaff HV, et al. Mortality and morbidity of aortic regurgitation in clinical practice. A long-term follow-up study. Circulation 1999;99:1851-1857 Link370. Genereux P, Amoroso NS, Thourani VH, et al. Mortality Burden for Patients With Untreated Aortic Regurgitation. JACC Adv. 2024;3:101228 Link. Surgical aortic valve repair or replacement is the standard of care for patients with severe symptomatic AR, and current guidelines limit the use of TAVI for the treatment of pure AR to patients who are ineligible for surgery (Table 22), 39. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA Guideline for the Management of Patients With Valvular Heart Disease: A Report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143:e72-e227 Link40. Vahanian A, Beyersdorf F, Praz F, et al. 2021 ESC/EACTS Guidelines for the management of valvular heart disease. Eur Heart J. 2022;43:561-632 Link.
Table 22. Guideline recommendations: Mode of intervention in patients with pure aortic regurgitation
2020 AHA/ACC Valvular Heart Disease Guideline
2021 ESC/EACTS Valvular Heart Disease Guideline
Recommendation
TAVI for isolated chronic AR is challenging because of dilation of the aortic annulus and aortic root and, in many patients, lack of sufficient leaflet calcification. Risks of TAVI for treatment of AR include transcatheter valve migration and significant paravalvular regurgitation. TAVI is rarely feasible, and then only in carefully selected patients with severe AR and heart failure who have a prohibitive surgical risk and in whom valvular calcification and annular size are appropriate for a transcatheter approach.
TAVI may be considered in experienced centres for selected patients with AR and ineligible for SAVR.
ACC/AHA = American College of Cardiology/American Heart Association; AR = aortic regurgitation; COR = class of recommendation; ESC/EACTS = European Society of Cardiology and the European Association for Cardio-Thoracic Surgery; LOE = Level of evidence; SAVR = surgical aortic valve replacement; TAVI = transcatheter aortic valve implantation.
However, there is a non-negligible undertreatment of patients with severe symptomatic AR, and the predominant reasons include advanced age, female sex, high surgical risk, and advanced left ventricular systolic dysfunction, , 371. Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231-1243 Link372. Iung B, Delgado V, Rosenhek R, et al. Contemporary Presentation and Management of Valvular Heart Disease: The EURObservational Research Programme Valvular Heart Disease II Survey. Circulation. 2019;140:1156-1169 Link373. Thourani VH, Brennan JM, Edelman JJ, et al. Treatment Patterns, Disparities, and Management Strategies Impact Clinical Outcomes in Patients with Symptomatic Severe Aortic Regurgitation. Structural Heart. 2021;5:608-618 Link. Accordingly, TAVI for pure AR has been explored as an alternative treatment strategy (Table 23) although it is technically challenging due to anatomical and device-related considerations; dilatation of the ascending aorta and aortic annulus, lack of calcification of the aortic valve leaflets, elliptical and dilated LVOT, increased stroke volume, and lack of large THV sizes and anchoring capability.
Table 23. TAVI for pure native valve aortic regurgitation.
Study
N
Age (years)
STS-PROM
Access
Device
Procedural
success
Post procedure ≥mod PVR
Second Valve
Required
30 days mortality
1 year (6 months) mortality
Roy et al. (2013)
43
75.3 ± 8.8
10.2 ± 5.3%
Femoral (81.4%) Subclavian (9.3%) Direct aortic (7.0%) Carotid (2.3%)
CoreValve
74%*
4.7%
18.6%
9.3%
21.4%
Seiffert et al. (2014)
31
73.8 ± 9.1
5.4 ± 3.6%
Apical
JenaValve
96.8%*
0%
3.2%
12.9%
19.3%
Wendt et al. (2014)
8
72.5 ± 8.4
7.3 ± 3.3%
Apical
ACURATE TA
100%+
0%
0
0
0
Testa et al. (2014)
26
73 ± 10
13.1 ± 2.0%
Femoral (81%) Subclavian (15%) Direct aortic (4%)
CoreValve
76.9%+
88.5%a
19.2%
23%
31%
Schofer et al. (2015)
11
74.7 ± 12.9
8.84 ± 8.9%
Femoral
Direct Flow
100%+
0%
0
9%
/
Sawaya et al. (2017)
78
74 ± 10
6.7 ± 4.8%
Femoral (65%) Subclavian (3%) Direct aortic (3%) Apical (29%)
CoreValve (42%) Evolut R (6%) JenaValve (29%) Direct Flow (8%) Lotus (8%) SAPIEN XT (5%) SAPIEN 3 (1%)
*: Procedural success was defined as the successful transcatheter implantation of a functioning aortic valve according to Valve Academic Research Consortium criteria.
+: Procedural success was defined as the successful transcatheter implantation of a functioning aortic valve according to Valve Academic Research Consortium 2 criteria.
†: Procedural success was defined as the successful transcatheter implantation of a functioning aortic valve according to Valve Academic Research Consortium 3 criteria.
PVR = paravalvular regurgitation; STS-PROM = Society of Thoracic Surgeons Predicted Risk of Mortality; THV = transcatheter heart valve.
Several studies have reported that TAVI using THV devices off-label for the treatment of pure severe AR is associated with a higher risk of procedural complications (valve embolization and need for second valve implantation) and device failure, 374. Yoon SH, Schmidt T, Bleiziffer S, et al. Transcatheter Aortic Valve Replacement in Pure Native Aortic Valve Regurgitation. J Am Coll Cardiol. 2017;70:2752-2763 Link375. Poletti E, De Backer O, Scotti A, et al. Transcatheter Aortic Valve Replacement for Pure Native Aortic Valve Regurgitation: The PANTHEON International Project. JACC Cardiovasc Interv. 2023;16:1974-1985 Link. The PANTHEON International Project evaluated the performance of new-generation THV in patients treated for pure native severe AR. The study included 201 patients who underwent TAVI with currently available devices. The overall technical and device success rates (according to the VARC-3 criteria) were 83.6% and 76.1%, respectively, and the procedural failure were predominantly due to device embolization (12.4%) and residual moderate or greater AR (9.6%). Of note, there were no differences in the complication rates between the balloon-expandable and self-expanding devices375. Poletti E, De Backer O, Scotti A, et al. Transcatheter Aortic Valve Replacement for Pure Native Aortic Valve Regurgitation: The PANTHEON International Project. JACC Cardiovasc Interv. 2023;16:1974-1985 Link.
To overcome the technical challenges, dedicated TAVI systems have been designed. The JenaValve (JenaValve Technology) and J-Valve (JC Medical) are dedicated self-expanding valve systems for the treatment of pure AR. Both THV are designed to provide active anchoring features in noncalcified aortic valve leaflets, via 3 anchoring clips in the JenaValve and 3 anchoring rings in the J-Valve system. Although earlier generation devices were delivered via transapical access, 376. Seiffert M, Bader R, Kappert U, et al. Initial German experience with transapical implantation of a second-generation transcatheter heart valve for the treatment of aortic regurgitation. JACC Cardiovasc Interv. 2014;7:1168-1174 Link377. Wei L, Liu H, Zhu L, et al. A New Transcatheter Aortic Valve Replacement System for Predominant Aortic Regurgitation Implantation of the J-Valve and Early Outcome. JACC Cardiovasc Interv. 2015;8:1831-1841 Link, both systems have been completely redesigned for transfemoral access in current generation of devices (Figure 33).
Figure 33
Dedicated transcatheter aortic valve implantation devices for the treatment of pure aortic regurgitation.
The latest iteration of the JenaValve, the JenaValve Trilogy, consists of a supra-annular porcine pericardial bioprosthetic valve with a nitinol frame. The unique feature of the Trilogy valve is the locator technology that ensures optimal positioning within the native aortic valve and secure anchoring by 3 radial locators that are positioned in each aortic cusp under fluoroscopy or transesophageal echocardiography guidance, ensuring commissural alignment and attachment to the cusps upon valve release. The frame has three large open cells, enabling coronary artery access after implantation. The prosthesis is available in 3 sizes (23 mm, 25 mm, and 27 mm), allowing treatment of annulus diameters up to 28.6 mm, while treatment of bicuspid valves is currently not recommended. A German multicentre study was the first to report the clinical outcomes of the JenaValve Trilogy. In the analysis of 58 patients who underwent TAVI with the JenaValve Trilogy for the treatment of pure AR, device success was achieved in 98% of patients, with no moderate or greater PVR, valve embolization, or conversion to surgery. At 30 days, 92% of the patients were in NYHA functional class I or II, and the 30-day mortality rate was 1.7%378. Adam M, Tamm AR, Wienemann H, et al. Transcatheter Aortic Valve Replacement for Isolated Aortic Regurgitation Using a New Self-Expanding TAVR System. JACC Cardiovasc Interv. 2023;16:1965-1973 Link. The ALIGN-AR trial is the first, prospective, multicentre, single-arm pivotal study of transfemoral TAVI with the JenaValve Trilogy in patients with symptomatic moderate-to-severe or severe AR at high surgical risk. Anatomical exclusion criteria included bicuspid aortic valve morphology, aortic annulus perimeter derived diameter of <21.0 mm or >28.6 mm or perimeter <66 mm or >90 mm, aortic annulus angulation >70 degree, straight length of ascending aorta of <55 mm, and significant disease of ascending aorta (ascending aortic aneurysm defined as maximal luminal diameter of 50 mm or greater or atheroma including if thick [>5 mm], protruding or ulcerated). The primary safety endpoint was all-cause mortality, any stroke, major vascular complication, life-threatening or major bleeding, new pacemaker, acute kidney injury, valve dysfunction and surgery or intervention related to the device at 30 days, and the primary efficacy endpoint was all-cause mortality at 1 year. This study included 180 patients (mean age was 75 years, 47% were female, and mean STS-PROM was 4.1%). Technical success was achieved in 171 (95%) patients, and 30-day all-cause mortality, any stroke, and moderate or greater residual AR occurred in 2.2%, 2.2%, and 0.6%, respectively. The primary safety endpoint was met in 48 patients with a prespecified non-inferiority margin (26.7%, 97.5% CI 19.2-34.0, Pnon-inferiority <0.0001), with new pacemaker implantation in 36 (24%) patients. At 1 year, the primary efficacy endpoint of all-cause mortality was low (7.8%, 97.5% CI 3.3-12.3, Pnon-inferiority <0.0001) and the JenaValve Trilogy demonstrated significant and sustained improvement in functional status and patient-reported outcomes (6-min walk test: from 262.7 m at baseline to 312.5 m at 1 year, P = 0.004; and KCCQ overall score: from 55.3% at baseline to 77.6% at 1 year, P <0.0001)379. Vahl TP, Thourani VH, Makkar RR, et al. Transcatheter aortic valve implantation in patients with high-risk symptomatic native aortic regurgitation (ALIGN-AR): a prospective, multicentre, single-arm study. Lancet. 2024;403:1451-1459 Link. At 2 years, all-cause and cardiovascular death and all-cause stroke occurred in 15.4%, 7.4%, and 6.4% of patients, respectively, and the bioprosthetic haemodynamic properties and improved patient health status were sustained. In addition, echocardiography demonstrated favourable LV remodeling that was sustained over the 2-year follow-up period380. Vahl TP. The ALIGN-AR Trial: Two-Year Outcomes of Transcatheter Aortic Valve Replacement With JenaValve TrilogyTM in High Surgical Risk Patients With Moderate-to-Severe or Severe Native Aortic Regurgitation. TCT 2024. October 29, 2024. Washington, DC. Link. Based on the favourable results of the Trilogy System, a randomized clinical trial is currently ongoing to demonstrate non-inferiority of the Trilogy THV System compared to SAVR for the treatment of patients with clinically significant native AR (ARTIST: Aortic Regurgitation Trial Investigating Surgery Versus Trilogy [NCT06608823]).
The J-Valve consists of 3 bovine pericardial leaflets in a self-expanding, low-profile nitinol frame with 3 U-shaped “anchor rings” and has a similar anchoring concept to that used for the Trilogy prosthesis. The prosthesis is available in 5 sizes (22, 25, 28, 31, and 34 mm) to treat a wide range of anatomies, with an annular diameter of up to 33.1 mm. A compassionate use experience in North America was reported in which 27 patients (median age 81 years, 81% at high surgical risk, 96% in NYHA functional class III or IV) with native valve AR were treated with the J-Valve (2018-2022). Although adverse clinical outcomes were rare at 30 days (1 death, 1 stroke, 3 permanent pacemaker implantations, and no moderate or greater AR), procedural success defined as the J-Valve delivered to the intended location without the need for surgical conversion or a second THV was achieved in 81% (22 of 27 cases), which led to a redesign of the attachment points and bonding methods. After the valve design was modified, the compassionate use experience was successfully continued without surgical conversion or the need for a second THV381. Garcia S, Ye J, Webb J, et al. Transcatheter Treatment of Native Aortic Valve Regurgitation: The North American Experience With a Novel Device. JACC Cardiovasc Interv. 2023;16:1953-1960. Link. The J-Valve TF Early Feasibility Study (JVTF EFS) prospectively evaluated the safety and efficacy of the J-Valve in patients with severe symptomatic AR, high surgical risk, and suitable anatomy for transfemoral access. The study included 15 high-risk patients (mean age 80 years, 73% male, STS-PROM 5.5%). The procedural success rate was 93.5% (14 of 15 cases): one patient required conversion to surgery due to an inability to release the anchor rings after a successful valve deployment, secondary to extreme aortic tortuosity. At 30 days, there were no cardiovascular deaths, strokes, device-related interventions, or new permanent pacemakers. Echocardiographic outcomes showed no or trace residual AR in all patients, and a paired analysis showed an evidence of left ventricular remodeling. The J-Valve Transfemoral Pivotal Study (JOURNEY) is currently ongoing to evaluate the safety and efficacy of the J-Valve Transfemoral System in patients with symptomatic, severe (grade 3 or 4) native AR and AR-dominant mixed aortic valve disease (NCT06455787).