Bifurcation lesions (old)
Summary
Coronary bifurcations are by nature prone to the development of atherosclerosis. They pose technical difficulties for percutaneous interventional treatment and they are associated with higher stent thrombosis and restenosis rates. The optimal approach for true coronary bifurcations is still a subject of debate, especially when the side branch (SB) is large, not easily accessible and narrowed by a long lesion. The general philosophy is: keep it simple and safe, understand and respect the original bifurcation anatomy, optimize flow and function of a bifurcation following percutaneous coronary angioplasty and limit the number of stents which should be well apposed and expanded with limited overlap. The role of dedicated devices in this setting remains unclear. Complex techniques (using two or three stents) should be used only when necessary, because they are associated with a worse outcome. Final kissing balloon (FKB) inflation is strongly recommended when using a complex technique.
The consensus is that main branch (MB) stenting with provisional SB stenting should be the default approach in the majority of cases. This approach is associated with a low risk of failure and complications provided that the following guidelines are implemented: wiring of both branches when starting the procedure, stenting of the MB with a stent diameter adapted to the distal MB, immediate optimization of the proximal stent segment according to Finet’s law using the proximal optimization technique (POT). The procedure can then be stopped at this point, however, if the SB does need attention, then the POT/side/POT technique (Re-POT) or FKB can be used. If SB stenting is necessary T, TAP or Culotte stenting can be performed.
Introduction
For anatomical reasons and due to the distributive function of the coronary tree, bifurcation sites are prone to the development of atherosclerotic lesions, as a result of flow turbulence generating pro-atherogenic low wall sheer stress. For these reasons, bifurcation lesions frequently account for up to 30% of lesions in patients with multivessel disease. The treatment of bifurcation lesions remains a controversial problem in terms of therapeutic indications, interventional strategy and technical considerations.
The challenge posed by bifurcation disease emerged in the early years of percutaneous coronary intervention (PCI) with plain balloon angioplasty and many techniques were developed in order to improve the procedural success and long-term outcome. Over the past 20 years, since the advent of drug-eluting stents (DES), coronary bifurcation lesions have been the subject of intense discussion and debates, fueled by new definitions, classifications, measurement and imaging methods as well as various clinical series, registries or randomized studies and meta-analyses. Numerous new findings with a direct impact on therapeutic strategies have emerged from the experimentation of various stent implantation techniques in bench tests.
The purpose of the present review is to examine the strategies currently implemented in the treatment of coronary bifurcation disease, to highlight the most debated issues and to propose recommendations for an optimal approach. The treatment of distal left main (LM) lesions will be discussed briefly in order to underline differences and similarities with non-left main bifurcation lesions.
Fundamental Aspects
THE THREE DIAMETERS
There is a strong anatomical/functional relationship in the coronary tree , which is constructed according to the hypothesis of minimum energy cost . The epicardial section of the coronary tree has a distributive function and the intramyocardial part has a delivery function. The sum of the vascular areas, as well as mean blood flow velocity, is constant in the distributive part. The total vascular area increases distally and blood flow slows down in order to allow sufficient contact time for capillary exchange. Instantaneous blood flow velocity is maximal during diastole and minimal, or even reversed, during systole. In epicardial arterial segments, coronary artery branching complies with the fractal geometry pattern and its self-similarity principle .
Asymmetric branching is repeated all along the coronary tree following the branching law described in 1923 as Murray’s law :
D³mother = D³daughter1+ D³daughter2.
This law was recently modified by Kassab, with respect to the exponent (2/3 for coronary arteries instead of 3). Finet’s formula, as validated in the coronary arteries by intravascular ultrasound (IVUS), is even easier to use in routine practice in a cathlab:
Dmother = (Ddaughter1 + Ddaughter2) x 0.678.
These formulae are analogous to the flow continuity formula applied to flow across an obstruction. In the coronary tree, linear relationships exist between diameter and flow and between diameter, length, flow and perfused myocardial mass .
The practical implications of this anatomical/functional structure are the following:
- There is no linear decrease from the proximal to the distal diameter of a coronary artery. The diameter is constant between two bifurcations and then diminishes abruptly when the artery branches off into a bifurcation. This makes all undedicated QCA software and methods obsolete, especially for analysing the vicinity of bifurcations.
- A coronary bifurcation is not composed simply of a main vessel and a SB, it has three segments with different diameters and flows (proximal main vessel: PMV, distal main vessel: DMV and SB).
- Following the flow/length/diameter relationship, the DMV should be the largest and/or longest segment.
FLOW, SHEAR STRESS AND ATHEROMA
In non-bifurcated segments, intracoronary flow is linear and exerts friction on the vessel wall, termed wall shear stress (WSS) . A low WSS is a frequently identified factor in atherogenesis . A low WSS is associated with slow, turbulent or reversed flow, especially in coronary bifurcations . In non-bifurcated vessels, it occurs along the internal edge of a curve or behind an obstacle (e.g., atheroma, plaque, stent). In coronary bifurcations, flow remains rapid and linear at the level of the flow divider whereas it is turbulent and recirculating on the side opposite the carina in the PM, DMV and SB (Figure 1). Histopathological analysis and IVUS have confirmed that atheroma is often present in bifurcations and develops in areas with low WSS . In most instances, the carina is free of atheroma (Figure 2). In addition, it has been demonstrated that in-stent restenosis is governed by the same flow laws by means of which the pattern of the initial lesion is reproduced with predominant neo-intimal proliferation . Atheroma progression results from flow disturbances caused by the initial plaque and extends in an anterograde and circular manner . Circular progression of atheroma up to the carina, in cases of large plaque burden, may explain the presence of atheroma at the level of the carina in up to 30% of cases . This phenomenon is crucial to understand late appearance of stenosis proximal to a stent at a bifurcation level.
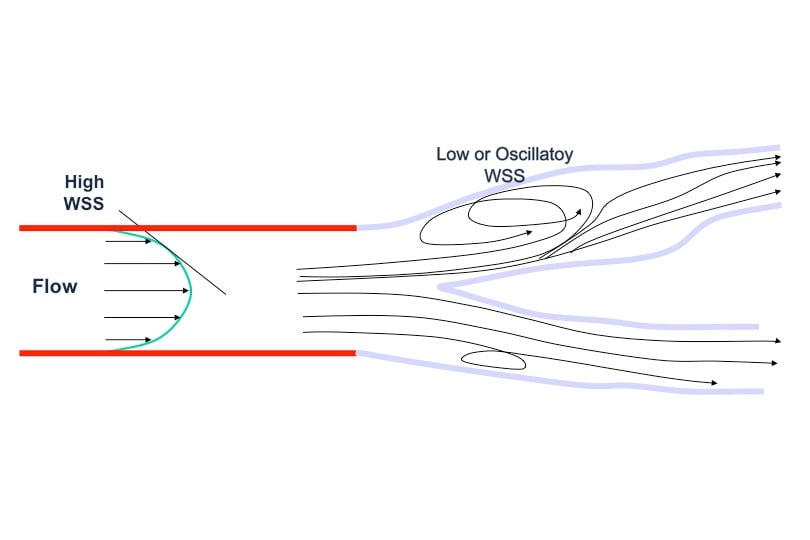
Figure 1
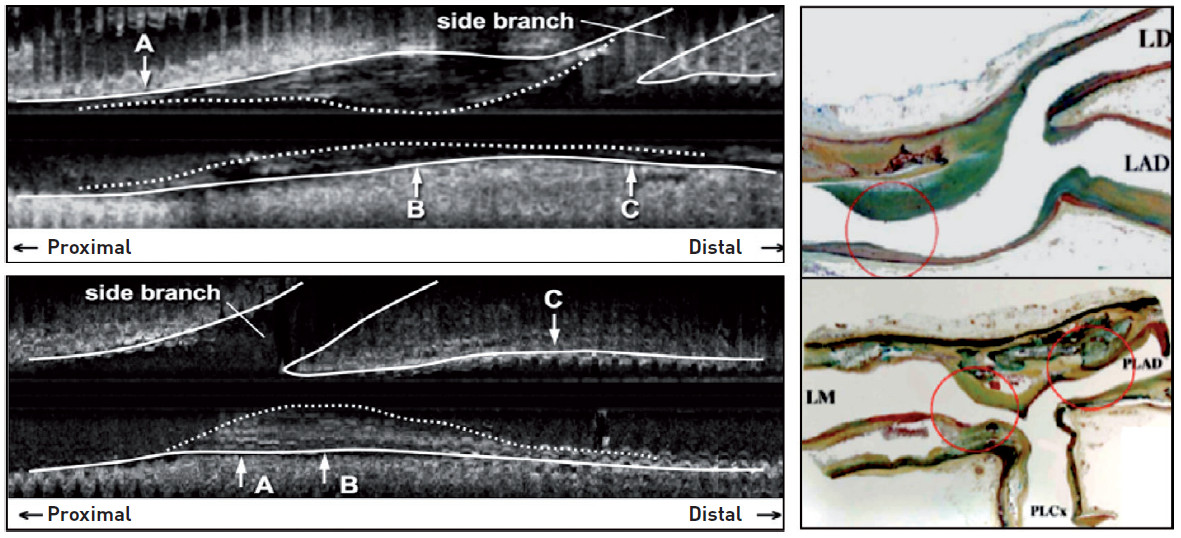
Figure 2
No atheroma at the level of the carena in the majority of cases
Atheroma is developing in areas of low shear, opposite to the flow divider (adapted from Shimada and Virmani)
The fact that there is usually no disease at the level of the carina has many implications that will be elaborated upon in the definition and technical sections.
Historical perspectives
BALLOONS
The first treatment strategies applied to coronary bifurcation lesions date back to the early years of coronary angioplasty, especially the famous kissing balloon inflation technique carried out with two guiding catheters. These balloon angioplasty procedures were associated with a low rate of procedural success, frequent complications and a high rate of restenosis .
BARE METAL STENTS
Following the advent of the first balloon-expandable bare metal stents (BMS) in the early 1990s, several bifurcation stenting techniques were described: kissing stenting, stenting across the SB, T stenting starting with the SB, Y stenting, Culotte stenting, modified T stenting, V stenting, the Skirt technique, Trouser legs and seat, and T stenting starting with the MB . Recognition of the excellent angiographic outcome of FKB after implantation of the MB, even in the presence of a SB lesion, resulted in a progressive acceptance of the “provisional SB stenting” strategy, with SB stent placement being left to operator judgment .
All these techniques designed for a large variety of lesions improved procedural success and safety but there was still a relatively high rate of restenosis and recurrent clinical events. Non-randomised comparisons of a one-stent versus two-stent approach were almost always in favour of the single-stent implantation technique . Very few studies compared the different types of double stenting techniques .
In the modern era, the use of bare metal stent should be absolutely avoided in bifurcation lesions whatever the clinical presentation, bifurcation type and used technique.
DEDICATED BARE METAL STENTS
The first dedicated stents were developed before the drug-eluting stent (DES) era. They were basic (Nir Side® [Medinol Ltd., Jerusalem, Israel], Jomed [Abbott Vascular, Redwood City, CA, USA]) or bifurcated (AVE [Medtronic/AVE, Galway, Ireland], Bard [Bard Ireland Ltd., Galway, Ireland]) and inadequately assessed in small observational studies .
DRUG-ELUTING STENTS
Drug-eluting stents started being used in coronary bifurcations in the early 2000s and clearly improved the mid-term angiographic and clinical outcomes . They levelled out the differences between the various techniques and, because of potentially very low restenosis rates, they generated several new very “metallic” techniques. The best known among these techniques are the Crush technique , the SKS (simultaneous kissing stenting) derived from V stenting whereby a new carina of variable size is created in the PMV .
In 2002-2003, Antonio Colombo conducted the first randomised study comparing the use of a single versus a dual-stent approach using T stenting with the Cypher® stent (Cordis, Johnson & Johnson, Warren, NJ, USA) in the treatment of coronary bifurcations . The results of this study were in favour of the provisional strategy with respect to the rate of restenosis. However, intent-to-treat analysis was compromised by a high rate of crossover from single to dual-stent treatment. After the European Bifurcation Club was created in 2004, numerous teams from both within and outside Europe designed new, single or multi-centre DES studies based on new definitions, classifications and analysis methods .
Definitions, classifications, analysis and treatment techniques
DEFINITION
The issue of an appropriate definition for coronary bifurcation lesions is still being debated. Most proposed definitions are based on the risk of SB occlusion after MB stenting. The risk of SB occlusion was mainly attributed to the "plaque shifting" phenomenon from the MB after balloon angioplasty or stenting . The role of plaque shifting was then disputed in view of the alleged absence of plaque on the carina and the term “plaque shifting” was replaced by “carina shifting”. Currently, the risk of SB occlusion is attributed to both phenomena . However, the main factor contributing to SB occlusion is carina shifting secondary to MB stent oversizing (when sized according to the proximal reference instead of the distal).
Fundamental data have clearly shown the relationship between the SB diameter and the perfused myocardial mass. The SB diameter should be used as an index of the extent of the myocardial area at risk in case of SB occlusion. The degree of biomarker elevation is recognized as a predictor of short-term and mid-term outcome . However, the relationship between the diameter of an occluded SB and biomarker elevation has never been demonstrated in humans.
The European Bifurcation Club (EBC) established a practical definition of the SB that takes into the account the individual characteristics of each patient: “a coronary bifurcation lesion is a coronary narrowing occurring adjacent to, and/or involving the origin of a significant SB”. “A significant SB is a branch that you do not want to lose in the global context of a particular patient (symptoms, location of ischaemia, branch responsible for symptoms or ischemia, viability, collateralising vessel, or left ventricular function)”. This simple definition is still valid while many authors are working in this field in order to develop a more robust definition of what is an important side branch.
CHARACTERISTICS OF CORONARY BIFURCATION LESIONS
Coronary bifurcation lesions have many different characteristics. The characteristics most often described are easily assessed by angiography, especially lesions located in the three segments of a bifurcation. “True” coronary bifurcation lesions are those with stenosis in the main vessel (PMV and/or DM) and in the SB before any treatment has been performed. The term “false” or “pseudo” bifurcation lesions, refers to instances where the SB is free of any lesion before treatment. In most cases, lesion assessment is carried out by visual analysis. False bifurcation lesions are nevertheless considered bifurcation lesions because the treatment of the MB may impact the SB ostium by carena shifting and sometimes plaque shifting whatever the technique.
Coronary bifurcation lesions have other significant characteristics. Visualization of calcifications can be achieved more or less adequately by semi-quantitative angiography, or more accurately by vessel enhancement or MSCT. According to the EBC set of definitions , angle A (Approach) is between the PMV and the SB and may determine access to the SB, angle B (Between) is between the DMV and the SB, and, when acute, may increase the risk of SB occlusion after MB stenting. Reliable visualization of the angles between the various bifurcation segments can only be achieved adequately by MSCT or 3-D angiography . The angle modification between systole and diastole after bifurcation stenting may have some impact on clinical outcome. The SB lesion length within the bifurcation is an important factor to be taken into account for treatment of a bifurcation lesion. When combined with poor accessibility, lesion length may constitute an alleged contra-indication to the provisional SB stenting strategy.
CLASSIFICATIONS OF BIFURCATION LESIONS
A large number of classifications have been reported or published . All of them are expressed via a combination of letters and/or digits describing the angiographic position of the lesions in the bifurcation. The main advantage of the Medina classification proposed in 2006 and adopted immediately by the EBC is its simplicity (Figure 3). Some parameters such as presence or absence of calcifications or SB lesions length can be added in order to add more informations about the complexity of the lesion, but the simple Medina classification is still the preferred classification in 2019.
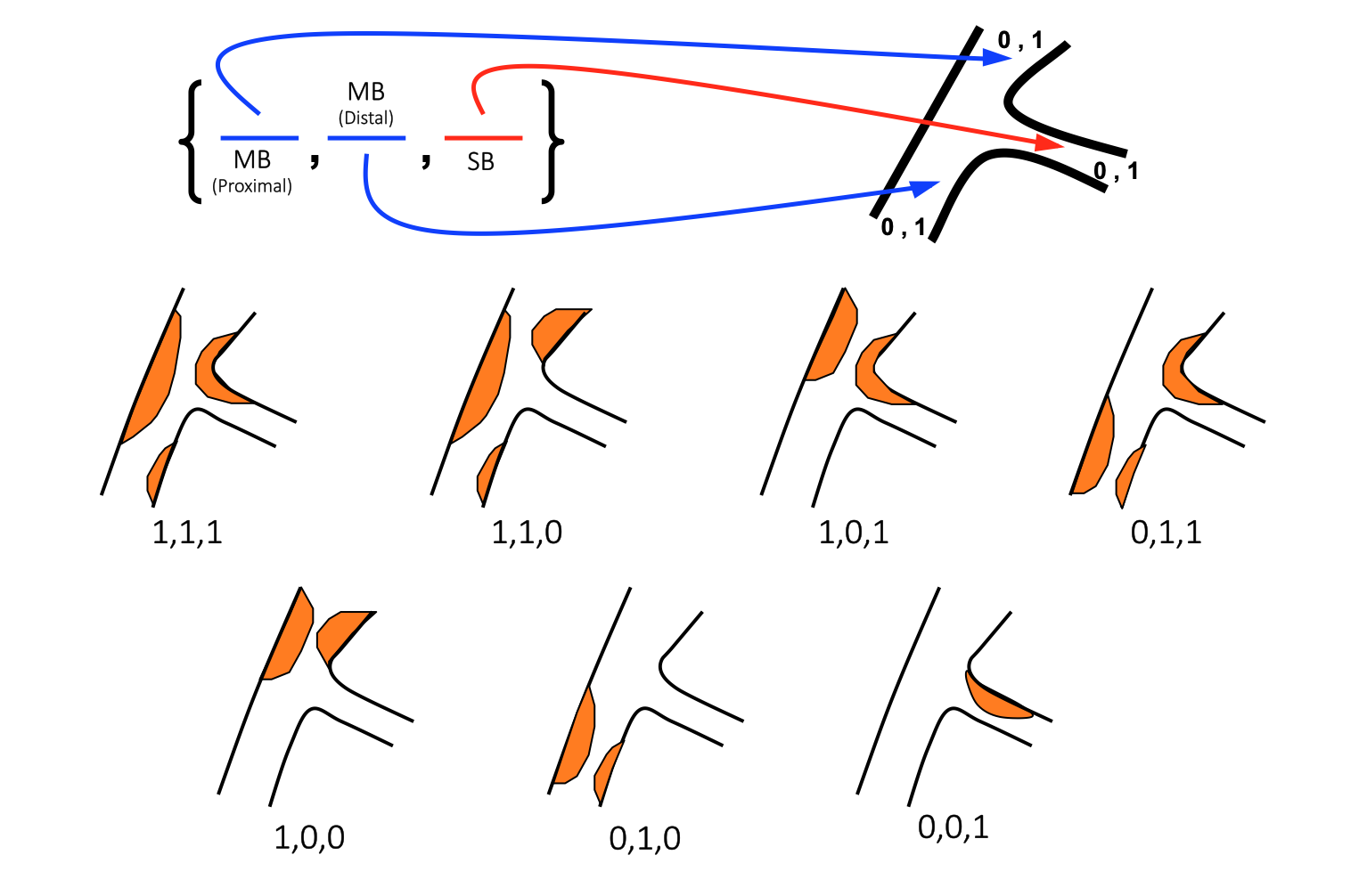
Figure 3
Modified Medina classification
An anatomical-based description of the three components of a bifurcation lesion. Before the first comma, 1 or 0 depending on the presence or not of > 50% stenosis in the proximal main vessel, between the two commas the same for distal main vessel, after the second comma the same for side branch (from A. Medina).
DESIGNATION OF CORONARY BIFURCATION LESIONS
QCA measurement, lesion classification and subsequent accurate definition of the technique used require clear designation of the SB prior to commencing treatment. Changing the DMV into the SB, or vice versa, modifies the Medina classification of the lesion involved, its automated analysis and the description of the technique used. For instance, the standard Culotte technique starting with stent implantation in the PMV towards the DMV becomes an inverted Culotte technique with the first stent being deployed from the PMV towards the SB.
How to define the DMV (and consequently the SB):
- In compliance with fundamental data, the DMV can be defined as the segment with the largest diameter, the longest distal segment and, consequently, with the highest flow volume vascularizing the largest myocardial mass. This generally corresponds to the LAD in relation to the diagonal branches, less frequently the postero-descending coronary artery (PDA) in relation to the postero-lateral coronary artery (PLA) and very rarely the circumflex in relation to a large marginal branch.
- The above rule can be adapted by the operator, not simply in order to define a technique, but also to take into account the presence of a bypass graft on one of the two branches, or major collateral flow, or conversely, in order to reflect the absence of myocardial viability within the territory of one distal branch.
QUANTITATIVE ANGIOGRAPHY OF BIFURCATION LESIONS
As explained above, the reference diameter profile of a normal coronary artery, from the proximal to the distal segment, is not a straight line but a flight of stairs with steps that vary both in length and height at the level of each bifurcation (Figure 4). The reference diameter between two significant bifurcations is almost constant and decreases only at the site where the bifurcation branches off. Any analysis of a bifurcation lesion performed with non-dedicated software is inaccurate with respect to the interpolated reference diameter at the level of the stenosis and to the percentage of stenosis, whatever the technique used. The inaccuracy is proportionate to the proximity of the lesion to the bifurcation and the size of the other distal vessel .
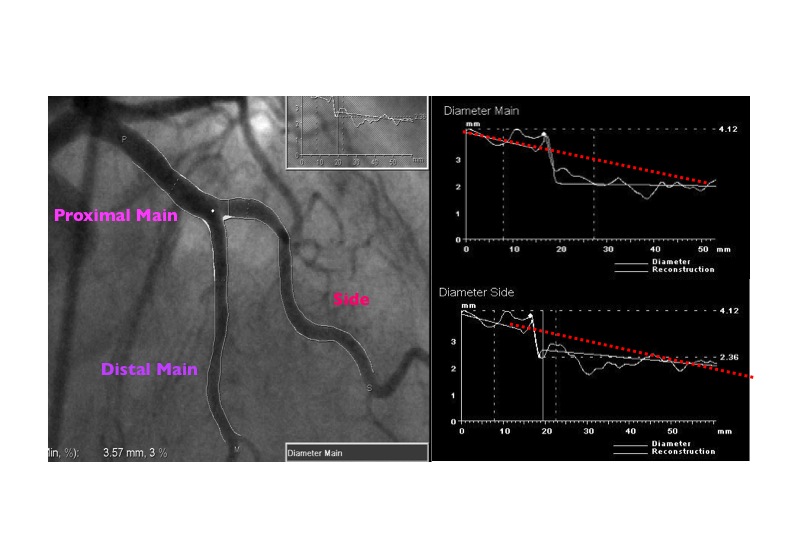
Figure 4
The reference functions from PM to DM and from PM and SB are not linear as usual (red dotted line), but constant proximal and distal to the bifurcation and stepped at the level of the bifurcation (from P. Serruys).
Dedicated software allowing automated analysis of bifurcation lesions has become available providing a simultaneous drawing of the luminal diameter curves in the three segments, an interpolated definition of the theoretical profiles in compliance with the laws of branching, as well as the degree of stenosis . Reproducibility depends on the standardisation of the methods used . In the context of a research study the EBC proposed the simultaneous analysis of the whole bifurcation, both branches, the three segments, the stented segments and their margins, the ostia as well as geographic miss and overlap (Figure 5) . The use of dedicated QCA was recommended by the EBC in order to study accurate indexed management of lesions according to the Medina classification and subsequently developed by Medis and Pie Medical Imaging .
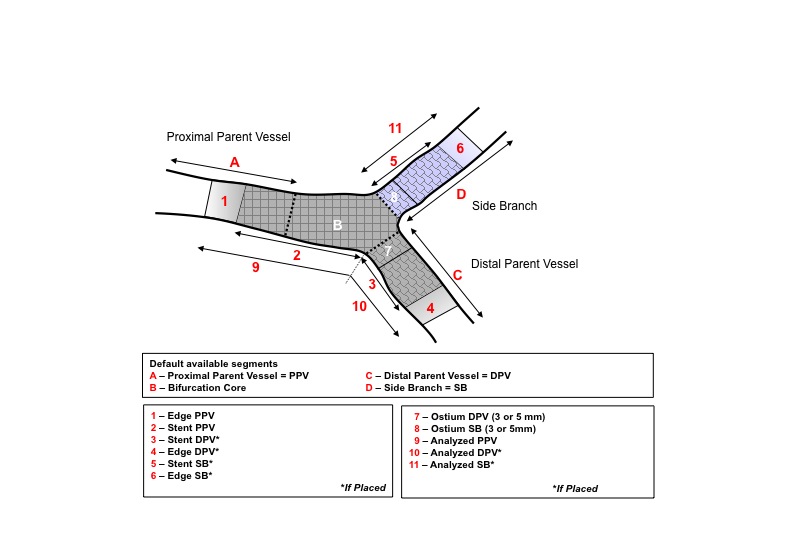
Figure 5
PHYSIOLOGICAL ANALYSIS OF CORONARY BIFURCATION LESIONS
During an intervention for bifurcation lesions, the operator needs to decide whether to intervene on the SB lesions and whether to implant a SB stent after balloon angioplasty. To overcome this complexity, a better understanding of this lesion subset is required. Although various angiographic or flow criteria are currently used to evaluate the severity of SB lesions, none of these has been validated as yet. Moreover, angiographic evaluation alone is sometimes inaccurate and does not reflect the functional severity of lesions, especially ostial lesions.
Fractional flow reserve (FFR) is an easily obtainable lesion-specific parameter for the physiological evaluation of epicardial coronary artery stenosis which takes into account the interaction between the anatomical stenosis and the area of perfusion supplied by a specific coronary artery. Recently, a series of investigations was performed to compare the functional severity and angiographic severity in SB lesions and to evaluate the functional outcomes of jailed SB lesions during follow-up . These studies have shown that FFR-guided provisional SB intervention is feasible and effective, that angiographic evaluation overestimates the functional severity of jailed SB lesions at every step of the provisional strategy for bifurcation lesions and that the functional status of jailed SB lesions after MB DES implantation does not change significantly during follow-up.
Such findings are crucial for understanding what types of SB residual lesions are acceptable not only at the end of the procedure but also at follow-up. Thus, because lesion length is a very important parameter to take into consideration, it is frequent to see a very tight, but short SB ostium stenosis without inducible ischaemia as assessed by FFR. In bifurcation lesions, the correlation between FFR and conventional QCA is poor, whereas it is improved when using three-dimensional QCA analysis of the SB .
ENDOLUMINAL IMAGING
IVUS
Intravascular ultrasound (IVUS) has dramatically changed our understanding of coronary atherosclerotic disease and the response to PCI . Angiography has limitations in assessing the extent of plaque burden and distribution, true luminal size and may provide only very modest information regarding the composition of the coronary lesion. On the other hand, these parameters can be easily obtained by the tomographic cross-sectional format provided by IVUS. In particular, IVUS has revealed that the extent of atherosclerotic disease is significantly more diffuse and localised calcifications are present much more commonly than is revealed by angiography. The information obtained from IVUS has also led to changes in the stent-deployment algorithm, ushering in the “high pressure deployment era” with dual anti-platelet therapy. However, this issue is still controversial because, despite better anatomical understanding, positive meta-analysis of randomised and non randomised studies in non-bifurcation lesions , and a recent positive non randomised studies in bifurcation lesions , no study has shown clearly the benefits of IVUS-guided bifurcation stenting over angiographically-guided stenting. Only one LM study, the Main Compare Study, has shown by post hoc analysis, that not using IVUS for LM stenting was associated with a higher death rate at mid-term follow-up. Today, IVUS should be considered for LM stenting, especially for physicians who do not carry out LM stenting frequently. It should be performed at least at the end of the procedure in order to assess stent apposition and deployment.
FFR is clearly better than IVUS to assess angiographically ambiguous LM disease or SB ostium disease.
For “IVUS” centres, a better insight into plaque configuration with IVUS can diminish the unnecessary use of two-stent procedure by distinguishing “true stenosis” from “pseudo stenosis” caused by artefacts including coronary spasm or calcification at the SB. This may play a role in improving outcomes allowing an appropriate selection of stenting strategy. IVUS is also a very useful tool for research and has shown in the past the limitations of complex stenting techniques. It may also help to improve our understanding of different technologies and the knowledge of the steps needed for appropriate stent or dedicated devices implantation.
Finally, IVUS should be used in all cases where there are some uncertainties either during or at the end of the procedure. In such cases IVUS may provide completely unexpected findings, which may be corrected before ending the procedure. The need for pullback from both branches has recently been pointed-out .
OCT
Optical coherence tomography (OCT) has 10 times higher resolution than IVUS. It produces fewer strut-induced artefacts and offers precise evaluation of strut apposition in a real-life clinical setting. This is currently the best tool to assess and guide stent expansion. Repeated OCT examinations at follow-up may also help to detect the presence and identify the characteristics of strut coverage, a potential predictor of late stent thrombosis . It is also a very useful tool to obtain aid re-crossing into the jailed SB (distal strut), and achieve distal MB rewiring and favourable stent positioning against the SB ostium . More informations are available in the recent consensus paper by Onuma et al. .
CLASSIFICATION OF BIFURCATION LESION TREATMENT TECHNIQUES
Since the advent of coronary stenting, many techniques have been reported or published. A classification by treatment families allows a simplified description of several analogous techniques, especially when they derive from each other. Very few technique classifications have been proposed. The ICPS classification reported first in 1996 was further expanded with the introduction of new techniques in 2004 . The available classifications are either not exhaustive or difficult to memorise. The only way of solving these issues is to keep the classification open. Any classification based on the final positioning of stents in a bifurcation is inadequate because it does not take into account the order in which stents are implanted. For instance, with the Culotte technique the first stent may be implanted from the PMV towards the DMV or the SB and the technical difficulties, acute results and clinical outcome may be different. The combination of a treatment strategy with final stent positioning keeps the classification open. The strategy is defined according to the placement of the first stent. The analogy between techniques classified into a specific type of treatment is not only accounted for by the final position of the stents implanted, but it also involves the gradual technical steps of the procedure. In this respect, the MADS classification proposed by the EBC in 2007 seems to meet the criteria of simplicity and openness. However, this classification cannot reflect the creativity of individual operators as it does not contain a detailed description of all potential balloon and guide manoeuvres.
A perfect description would require an electronic CRF in which all phases of any particular stenting procedure should be entered. All the techniques mentioned in the MADS classification have been reported or published. The four treatment types included in the MADS classification are identified by 4 letters: M (for Main) signifies that the first stent is deployed in the PM, A (for Across) means that the first stent is implanted from the PMV to the DMV across the SB, D (for Double) is used to describe an heterogeneous treatment type whereby one or two stents are delivered on two guidewires via two lumens without recrossing a stent strut and S (for Side) stands for a treatment type with stent placement in the SB first, with or without protrusion in the MB. In each treatment type, the procedure may be completed with the placement of one or two additional stents. The inversion of distal branches (where SB becomes DMV and vice-versa) defines the “inverted techniques”. the updated MADS classification (version 2) will be published in EuroIntervention in 2019 (Figure 6 and Figure 7).
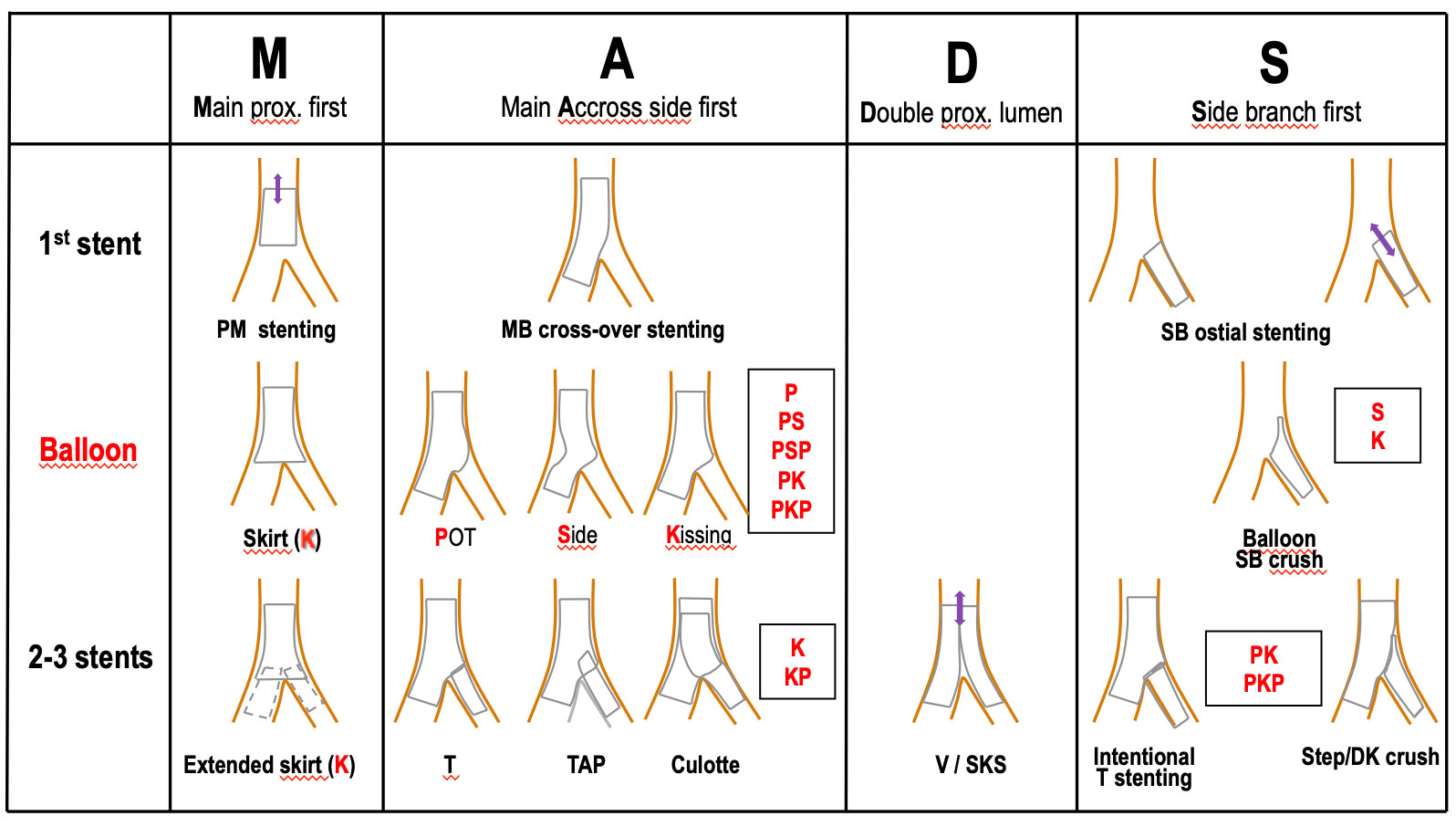
Figure 6
An operational description of the possible permutations when stenting a bifurcation lesion MADS classification (2019)
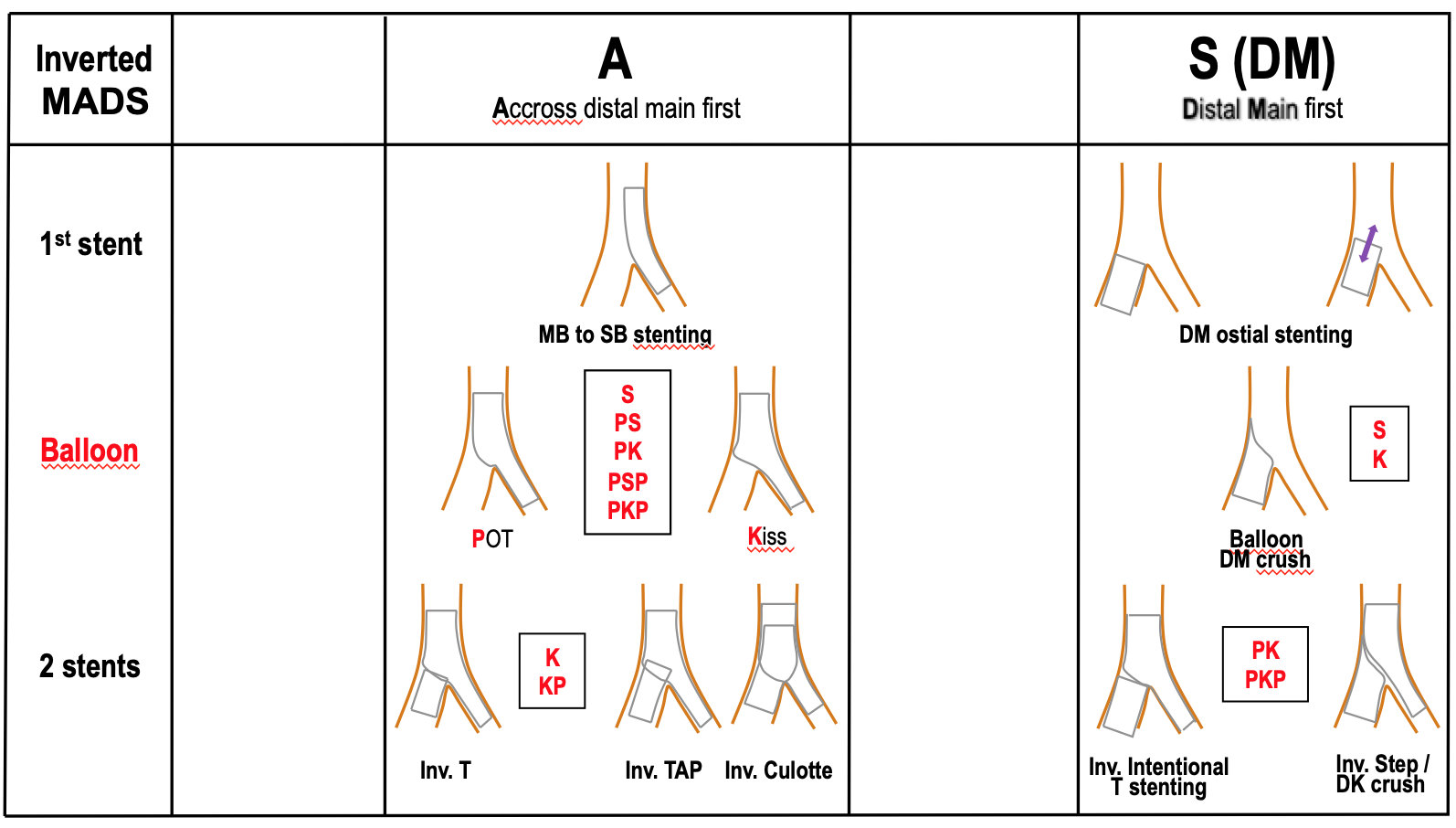
Figure 7
Updated MADS classification of inverted techniques (2019)
BMS and DES studies
ENDPOINTS
The endpoints selected in bifurcation studies are variable. In most instances, they include hard endpoints, such as death, acute myocardial infarction (AMI) and sometimes stroke. These endpoints are combined with bifurcation target lesion revascularisation (TLR) in major adverse cardiac events (MACE) or MACCE when cerebral events are added. Following the academic research consortium (ARC) classification, a better definition is now used for MACE: “device oriented” composite endpoint (DOCE) when a new device is assessed, which includes cardiac death, target-lesion related MI and TLR or “patient oriented” composite endpoint (POCE) for wide analysis, including any death, AMI, re-intervention or stroke.
No clear definition was adopted in the very few studies in which angiographic follow-up was performed and we do not have an accurate description of the restenosis process in this setting. MB and SB restenosis are reported, but restenosis in PMV and DMV corresponds to different restenosis territories. In cases where the SB is not stented, restenosis is assimilated to residual stenosis and both are regarded as target vessel failure (TVF). In the absence of LM lesions, acute events are associated with SB stenosis and long-term events are most often related to MB. However, a large SB may be responsible for symptoms or ischaemia that are seldom reported.
STENT THROMBOSIS
Many retrospective registries have pointed out a relationship between the risk of stent thrombosis and bifurcation lesions stenting . Careful analysis of these data shows that the risk of stent thrombosis seems to be more related to the implementation of a complex approach than to the bifurcation itself. In the prospective Japanese cypher registry (J-Cypher registry), which included 5,115 patients, stent thrombosis at 1 year was 1.17% in coronary bifurcations versus 0.44% in single vessels (p=0.02). However, only dual-stenting, haemodialysis and emergency intervention were found to be associated with stent thrombosis, not bifurcation (FDA, Circulatory System Devices Panel, December 7, 2006). In the J-PMS registry (another prospective Japanese registry with the Cypher® stent), the rate of stent thrombosis was 0.8% in bifurcation lesions treated with one stent, compared to 10.8% in patients treated with 2 stents (p=0.003) . A more recent metanalysis of 3107 patients as shown by intent to treat analysis a lower rate of early stent thrombosis (p=0.021) with the simple approach (0.26%) compared to a two stents technique (1.14%)
RANDOMISED STUDIES WITH FIRST GENERATION DES
There are 8 published randomised trials comparing provisional SB stenting with double stenting in the era of DES . Seven of these studies were conducted with the Cypher® stent and the largest one evaluated the Taxus® stent (Boston Scientific, Natick, MA, USA) . In three of these studies, several techniques were used to implement the dual-stent strategy . Three of the others compared the single stent strategy with only one double-stenting technique .
The results of the earliest study by Colombo et al were weakened by a very high rate of crossover from the single-stent strategy to the dual-stenting strategy which precluded any intention-to-treat analysis. This study reported a better outcome associated with the single-stent strategy . The study by Pan did not report any differences in terms of MACE, and only a trend toward a decrease in the SB restenosis rate when using only one stent in a small cohort of patients . The first significant study was the NORDIC trial, which included a large number of patients with a low crossover rate from one stent technique to a more complex approach. There was no difference in MACE rate at 6 month (Two stents 3.4%, 1 stent 2.9%) and no differences in the rates of definite, probable and possible stent thrombosis (ARC criteria) at 14 months (2 months after clopidogrel discontinuation) . However, the complex strategy was associated with longer procedural time, longer x-ray exposure, higher volume of contrast, and more periprocedural biomarkers elevation. No differences were observed with respect to MB restenosis or SB occlusion in the sub-group of patients who underwent angiographic follow-up. The 5 years follow–up showed a trend for higher MACE rate in the complex group. Ten years follow-up showed a similar non- significant trend in terms of death (Figure 8) in favor of the provisonal approach.
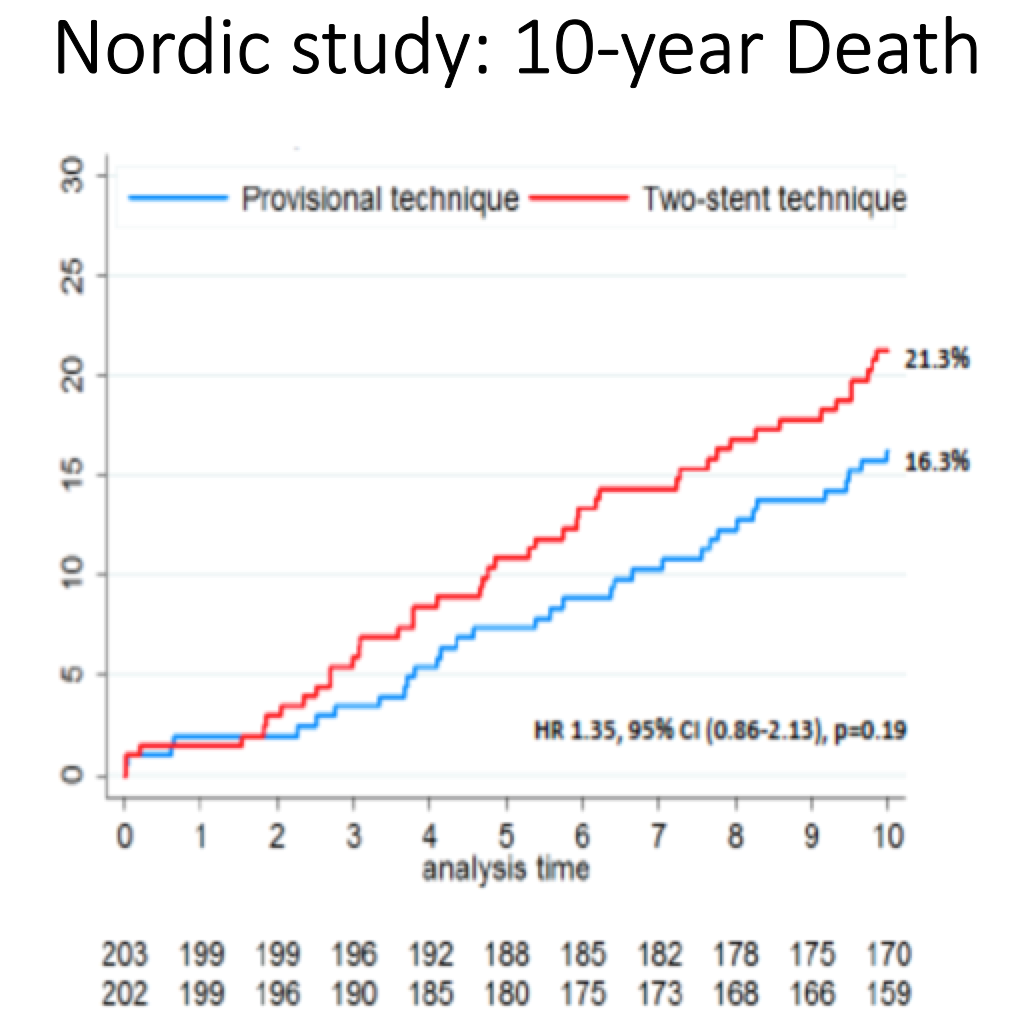
Figure 8
10 years death rate in the Nordic study (Provisional vs 2 systematic stents). From Steigen et al. TCT 2016
The BBK study by Ferenc and colleagues also had a very low rate of crossover. It was characterised by the fact that stent implantation was always performed in the MB first and that patients were randomised to systematic SB T-stenting or provisional SB stenting. The endpoint was angiographic (% diameter stenosis of the SB at 9-month angiographic follow-up). No difference was observed between provisional (23.0±20.2%) and systematic SB T- stenting (27.7± 24.8%, p=0.15). The 5 years follow-up was published recently and showed no difference in clinical outcome except a trend for a higher rate of stent thrombosis in the systematic T- stenting group.
The CACTUS study conducted by Colombo et al compared two technical strategies: provisional SB stenting and Crush-stenting. Crossover rate from provisional to crush was very high (31%). The primary endpoint (MACE) was not different between the two study groups (15% in the provisional vs. 16% in the Crush group). No differences were observed in the rate of restenosis in the MB (provisional 6.7% vs. Crush 4.6%) or the SB (provisional 14.7% vs. Crush 13.2%) . Interestingly, when a two stents technique was use, the MACE rate was significantly lower when FKB was performed.
The BBC one trial conducted by Hildick-Smith et al is the largest and the most recent study with a high proportion (83%) of true bifurcations. The complex strategy group was heterogeneous and both the Crush and Culotte techniques were implemented. The primary endpoint (a composite of death, MI and TVF at 9 months) occurred in 8.0% in the simple approach versus 15.2% in the complex one (p=0.009), a difference mainly driven by peri-procedural MI rates (3.6% versus 11.2%, p=0.001). Procedural time, x-ray exposure and volume of contrast used were lower in recipients of a single stent. At 5 years follow-up, the metanalysis based on individual data of BBC one and Nordic (Figure 9) showed a significant difference in terms of death in favor of the provisional approach (3.8 vs 7.0%, p=0.04).
A randomised study comparing the provisional strategy with the TAP technique was performed in China and showed no clinical difference between the 2 groups despite a higher rate of restenosis in the TAP group . More recently the same group reported the results of a randomised study comparing double kissing crush (DK crush II) to the provisional SB T-stenting strategy. This study showed favourable results associated with the double kissing crush technique with respect to Provisional SB stenting strategy .
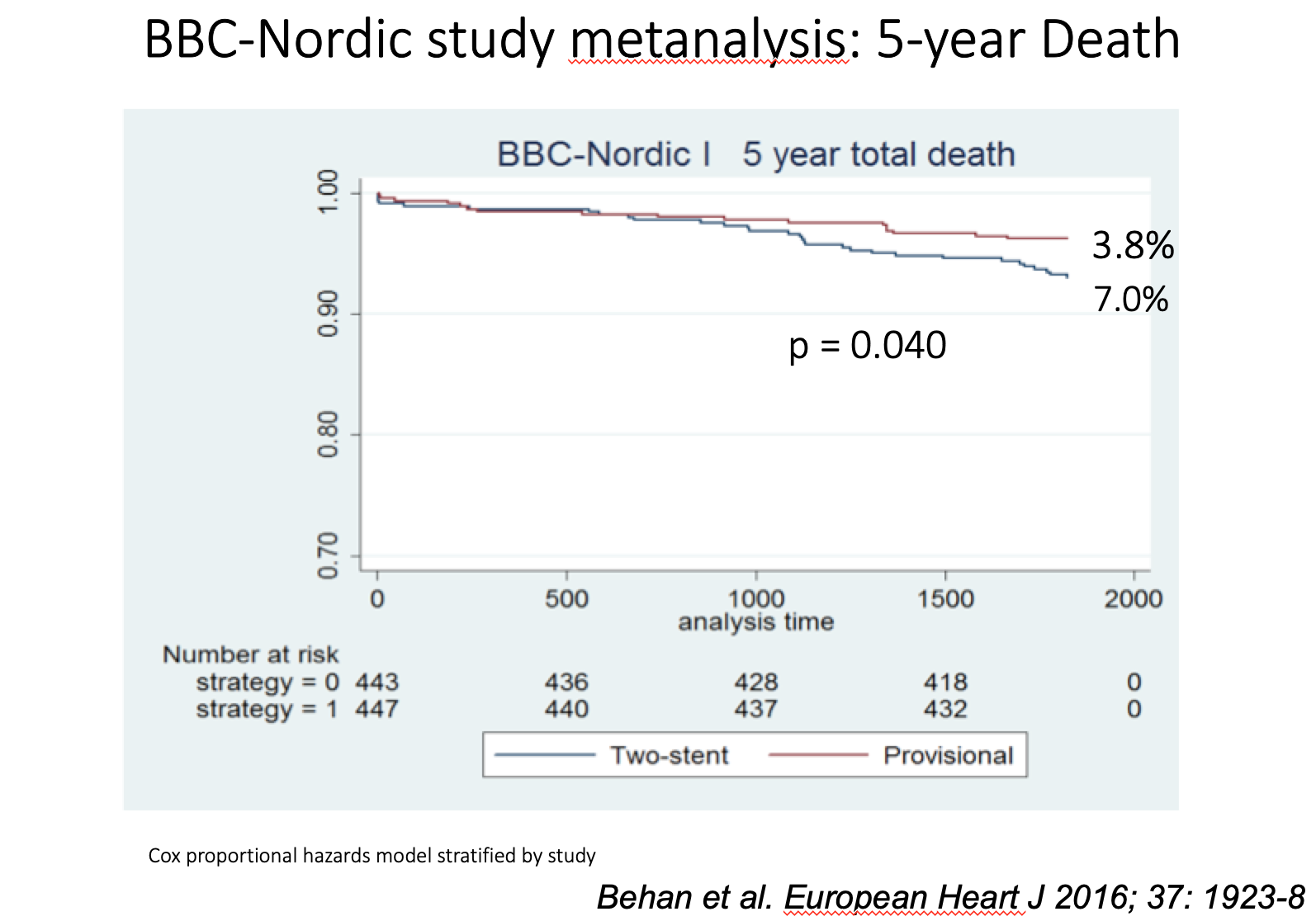
Figure 9
5 years death rate in the BBC-Nordic metanalysis (provisional vs sytematic two stents). From Behan et al. (reference 307)
When two stents are needed: Crush, Culotte or T-stenting?
An attempt at identifying the optimal complex technique when needed was made in the Nordic 2 trial comparing the classical Crush technique to the Culotte technique. The Culotte technique used was the straight Culotte (starting with stent placement in the MB). MACE rates at 6 months were similar (4.3% vs. 3.7%). At 8-month angiographic follow-up, in-stent restenosis was lower following Culotte stenting (MB: 6.6 vs.12.1%, p=0.10; SB: 4.5 vs. 10.5%, p=0.046). It is very difficult to make definitive conclusions. We can speculate that when the bifurcation angle is T-shaped and two stents are needed, a T-stenting technique is probably the best technique. When the bifurcation angle is Y-shaped, the Culotte technique is probably more appropriate than a classical Crush technique. However, the recent data from the DK Crush II study have shown a high rate of FKB and excellent clinical outcome with this technique and therefore further evaluation is needed. T stenting remains the easiest technique. The SB stent can be positioned at the ostium without protrusion in the MB when the SB ostium is covered by the MB stent. If the SB ostium is not covered by the MB stent a TAP or a Culotte is recommended. When a two stents technique is used, FKB is strongly recommended .
After a one-stent technique, do we need a final kissing balloon inflation?
The benefit of final kissing inflation associated with the provisional stenting technique has been assessed in a small randomised study by Pan et al who did not report any differences in clinical outcome despite the MB MLD distal to the carina, as measured by IVUS, being larger . Another small study published by Korn et al did not report any differences in MACE and restenosis rate. The Nordic III study did not show any clinical differences between the two groups at 6 months. At 8-month angiographic follow-up, differences in the rate of restenosis between the two techniques were shown to be in favour of FKB with a binary restenosis rate in the bifurcation lesion of 11.0 vs. 17.3% (p=0.11), in the MV 3.1 vs. 2.5% (p=0.68), and in the SB 7.9 vs. 15.4% (p=0.039). Even in patients with true bifurcation lesions, the SB restenosis rate was lower in the FKB group (7.6 vs. 20.0%, p=0.024).
On the other hand, the COBIS I study has shown that FKB was associated with a higher MACE rate a well as the CROSS and SMART-STRATEGY while COBIS II showed a significant reduction in TVR and MACE after FKB. Today, with the available data, it is still very difficult to conclude on the optimal technique because many other variables may play an important role in the outcome , such as the stent used, the diameter, length and type of the balloon used, the duration of inflation, the sequence of inflation and deflation: SB or MB first.
A new promising alternative is currently evaluated, the POT/Side/POT technique (Figure 10) or “Re-POT” . The technique is very simple. It consists in performing a POT after MB stent deployment in order to appose the proximal part of the MB stent, then access toward the distal strut of the MB stent through the SB, open the SB using a NC compliant balloon with a balloon/artery ratio of 1 and finally correct the MB stent deformation with a final POT. Careful sizing and positioning of the balloon (NC or semi compliant) just proximal to the carena is crucial in order to avoid carena shifting (too distal) or suboptimal proximal stent deployment (too proximal).
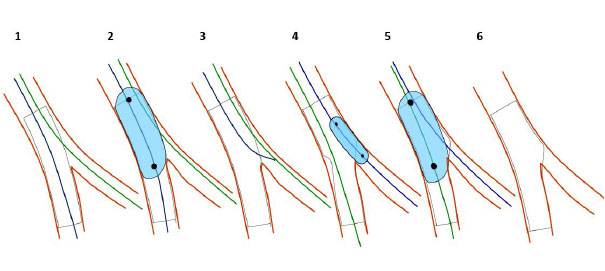
Figure 10
POT/Side/POT technique (RePOT): 1. stent deployment (diameter selected according to the MB distal reference. 2. Proximal optimization technique. 3. SB wiring through a distal strut. 4. SB dilatation with a NC balloon. 5. RePOT to correct the MB stent deformation. 6. Final result.
Role of second generation DES
A recent OCT study has shown less neointimal proliferation with new generation DES while a recent observational study has shown better clinical outcome with second generation DES compared to first generation . Very few clinical studies are available but they all show better clinical outcome with second generation DES.
In the the EBC two study , symptomatic patients with large caliber true bifurcation lesions (SB diameter ≥2.5 mm) and significant ostial disease length (≥5 mm) were randomized to either a provisional T-stent strategy or a dual stent culotte technique. Two hundred patients aged 64±10 years, were randomized in 20 European centers. SB stent diameter (2.7±0.3 mm) and length (20.3±5.9 mm) confirmed the extent of SB disease. Procedural success (provisional 97%, culotte 94%) and kissing balloon inflation (provisional 95%, culotte 98%) were high. Sixteen percent of patients in the provisional group underwent SB T-stenting. The primary end point (a composite of death, myocardial infarction, and target vessel revascularization at 12 months) occurred in 7.7% of the provisional T-stent group versus 10.3% of the culotte group (p=0.53). Procedure time, x-ray dose, and cost all favored the simpler procedure.
META-ANALYSIS
One of the limitations of randomised studies comparing a provisional to a systematic 2 stents approach is the fact that patients included in these studies have bifurcation lesions that were considered technically feasible with the 2 techniques by the operator. Therefore, patients with bifurcation lesions considered feasible only with 2 stents were probably not included in these studies. This may also limit the conclusions obtained from meta-analysis. Nine meta-analyses dedicated to the outcome of coronary bifurcation lesions have been published or reported . The recent DK crush II study was not included in these meta-analyses. Nevertheless, they all reported similar results with respect to the occurrence of mid-term clinical events associated with provisional SB stenting vs. dual-stenting strategies, namely no differences in mortality or TLR, but a small trend for a higher rate of stent thrombosis. The two main randomised studies (Nordic and BBC one) were included in a meta-analysis of individual data . This meta-analysis confirmed the benefit of the simple strategy compared to systematic dual stenting in all pre-specified subgroups: true bifurcations, open angles (>60°), large SB (≥2.75 mm), long SB lesions (>5 mm), ostial SB lesions and lesions with two equivalent distal diameters (difference <0.25 mm). In addition, the single-stent strategy was associated with a significant reduction in procedural time, x-ray exposure and contrast media volume. Two meta-analyses included randomised and non-randomised DES studies without accurately defined selection criteria. One of these two studies showed a higher SB acute gain in the dual-stenting group. However, minimal luminal diameter (MLD), as well as the restenosis rates was not different at follow-up analysis, which clearly showed that placement of a second stent is not required when a satisfactory result is achieved at the SB ostium without stenting.
Another large meta-analysis compared SB stenting with dual-stenting using BMS and DES in 42 studies and a total of 6,825 patients . This study confirmed the superiority of DES over BMS and of the single stent strategy compared to the dual technique as assessed by the MACE rate. These data are illustrated in (Figure 11).
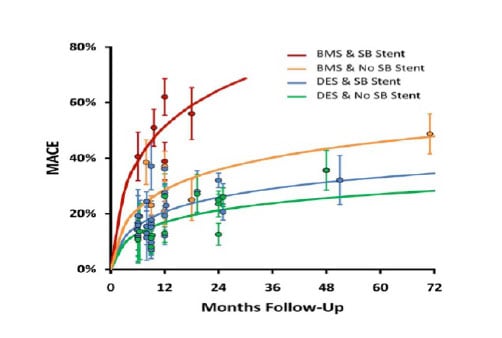
Figure 11
Meta-analysis illustrating the frequency of MACE between different bifurcation strategies.
Description of various treatment techniques
ROLE OF BENCH-TESTING
The first bench-test for stent evaluation was performed by deploying a stent in vitro through a strut or in a model, which was not constructed in compliance with ramification laws. The result was recorded with a video camera, or by means of endoscopy and later by microCT, with digital acquisition allowing precise measurements. Certain very elaborate benches were perfused with microspheres in suspension in order to analyse the relationship between endo-coronary flow and different stenting techniques.
These bench tests allowed also the measurement of the maximal expansion of stents and stent struts and the analysis of stent deformation and coating deterioration. The in vitro reproduction of the most frequently used techniques in compliance with ramification laws permitted the identification of the advantages and flaws of certain techniques and resulted in technical improvements. It also allowed the simulation of complications.
DIGITAL SIMULATION
This has become an increasingly reliable alternative to bench testing. Genuine normal or diseased coronary bifurcations can be captured by 3-D angiography or MSCT. They are subsequently transformed into “finite elements” each being attributed the mechanical properties obtained from autopsy measurements. Similarly, the structure and mechanical features of stents can be simulated as well as their deployment against potential vessel wall resistance .
In addition to stent deployment using simple techniques, it is possible to compare and analyse the ability to recross the stent struts with a wire, or study radial wall stress, or WSS generated by various flow conditions and various stent deployment techniques.
It is highly probable that the reproduction of complex techniques will be feasible in the future, as well as the simulation of the biological activity of DES and prediction of the restenosis risk.
GENERAL CONSIDERATIONS FOR ALL BIFURCATION TECHNIQUES
As a potentially complex PCI, general rules should apply for most of the bifurcations cases:
- Except for emergency PCI, Ad-hoc procedures should be avoided and angio carefully analyzed.
- Good backup support is needed with at least 6 French guiding catheter.
- Monitoring of ACT (objective>300 seconds) is crucial especially for long procedures, complex techniques and use of intra-coronary imaging.
M APPROACH (STENTING OF THE PROXIMAL SEGMENT FIRST)
The technical strategy starting with single stent placement in the PMV was first described as the Skirt technique whereby a stent was crimped manually onto two balloons. It currently consists in stent placement as close as possible to the carina, followed by deployment by means of two balloons towards the two distal branches . In certain lesions where a single stent is not sufficient, implantation of two stents with limited overlapping is required. Simultaneous implantation of two stents seems to be the best option and requires optimal expansion of the proximal stent. The dedicated Axxess stent from Biosensors is used with this M approach.
A APPROACH (PROVISIONAL SB STENTING)
This technique is now considered as the gold standard and used as the default approach in the majority of cases . It will be described step by step (Figure 12):
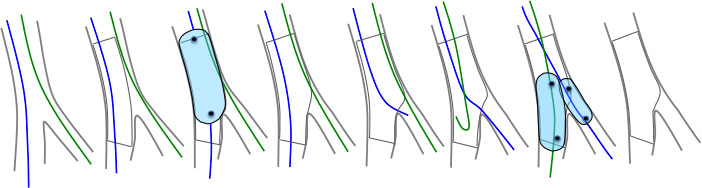
Figure 12
Schematic drawings illustrating provisional bifurcation stenting with the proximal optimisation technique (POT) and final kissing balloon inflation (FKB). Of note the jailed side branch and main branch wires are swapped over after the POT.
Insertion of two guidewires into each distal branch starting with the most difficult branch wired first. The second wire is then inserted by limiting the rotation manoeuvre using a torquer (no more than a wrist rotation to avoid wire wrap). In case of difficult SB access, the “pull-back” technique can be very usefull (Figure 13). Keeping the wires separated and identified outside the patient helps prevent wire wrap. We recommend that hydrophilic polymer wires, such as PT Graphics™ (Boston Scientific, Natick, MA, USA), should not be used in order to avoid rupture of the “jailed” wire during removal. Systematic placement of a wire in the SB helps to open angle A (A for approach: angle between the proximal MB and the SB), which further facilitates access to the SB during guidewire exchange . This wire is used in order to reduce the risk of SB occlusion following MB stenting , the predictors of which have been well identified, especially the acuteness of angle B . In instances of SB occlusion, the “jailed” wire serves as a marker to find the ostium or sometimes, in case of failure to recross the SB through the MB stent as bail-out technique. Wiring the two branches permit also to optimize the visualization of the bifurcation and look for the view with the wider angle between the two wires.
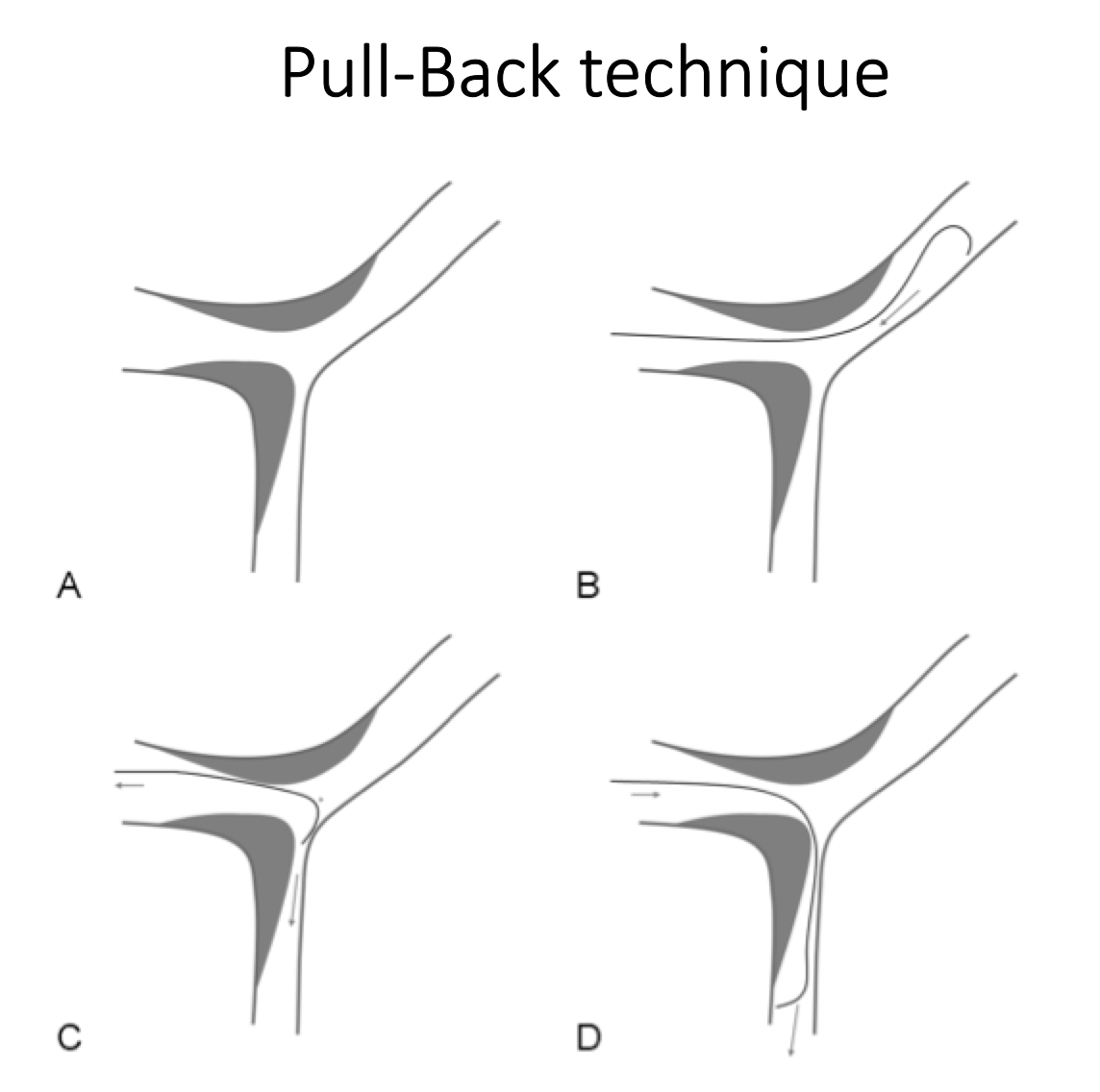
Figure 13
Schematic drawings of the «Pull-back technique» in case of difficult side branch access.
The shape of the two wires must be adapted to their secondary use. The “jailed” wire in the SB will be used to wire the MB when doing guidewire exchange. The tip of the MB wire must be relatively long and angulated in order to reach the SB ostium from the MB through the most distal cell of the MB stent. In cases of failure to insert a wire in the SB, the shape of the wire can be modified according to the diameter of the MB and angle between the MB and the SB. The wire can also be exchanged for a hydrophilic wire or a soft CTO wire with good torque transmission (Fielder FC or Sion wire). In case of proximal tortuosity before the bifurcation, a microcatheter can be used in order to increase control of the wire tip. In case of severe angulation between the MB and the SB and wiring failure, dual-lumen (Fineduo, Twinpass, Sasuke, NHancer Rx) or angulated (Supercross 90 or 120°) microcatheter (Figure 14) can be used. In some cases, the “reverse wire technique” (Figure 15), can be very useful . Rotational atherectomy of the MB may help resolve the issue by removing a calcified plaque in front of the SB (Figure 16). Wire and tool escalation for SB wiring failure before MB stenting is summarized in (Figure 17). In case of very difficult SB wiring, SB stenting first should be considered.
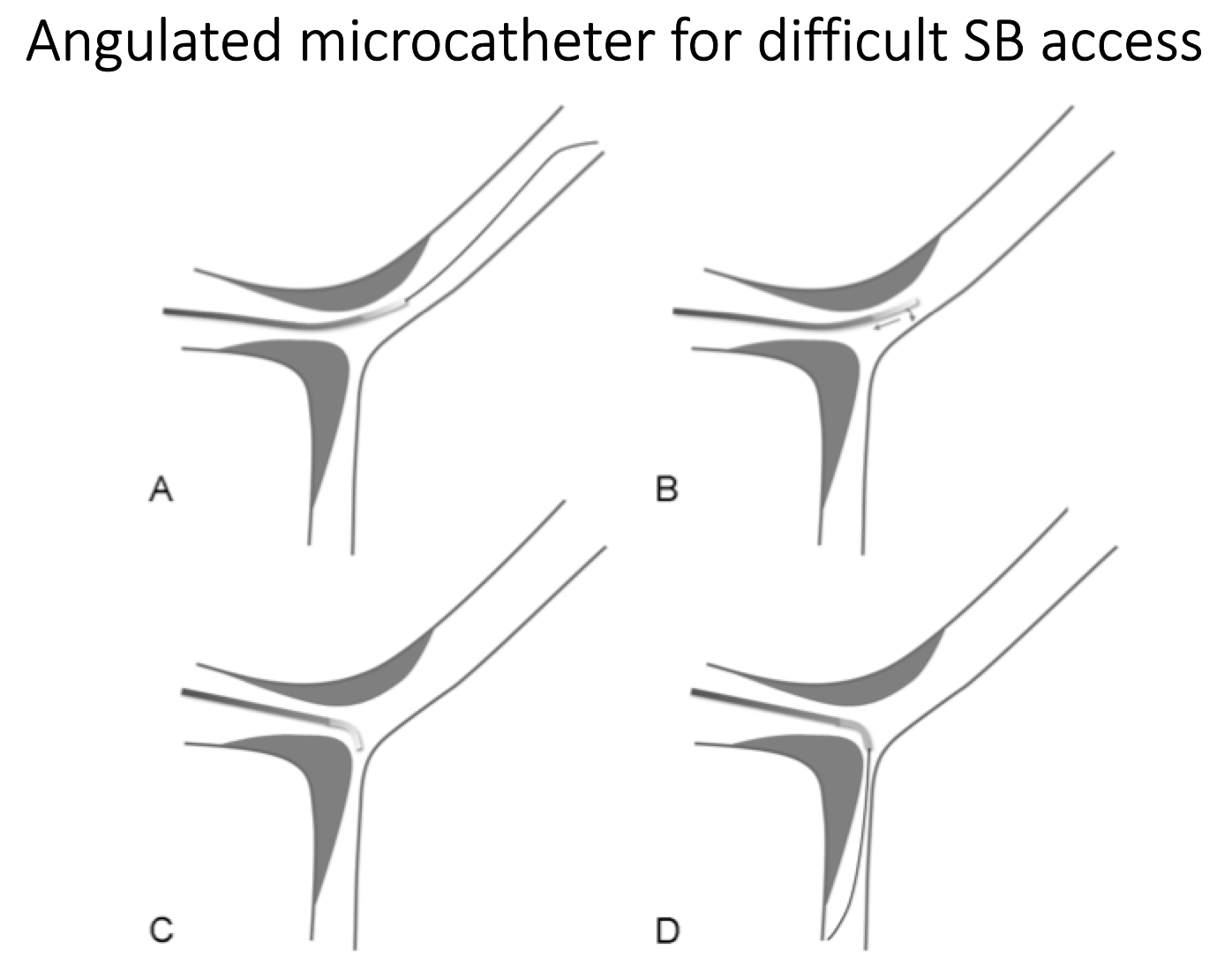
Figure 14
Schematic drawings of the angulated microcatheter approach in case of impossible side branch access.
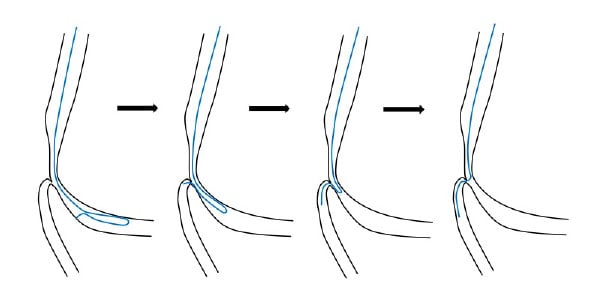
Figure 15
Schematic drawings illustrating the reversed wire technique. This is one of several advanced wire techniques that may be used for traversing an extremely angulated side branch origin.
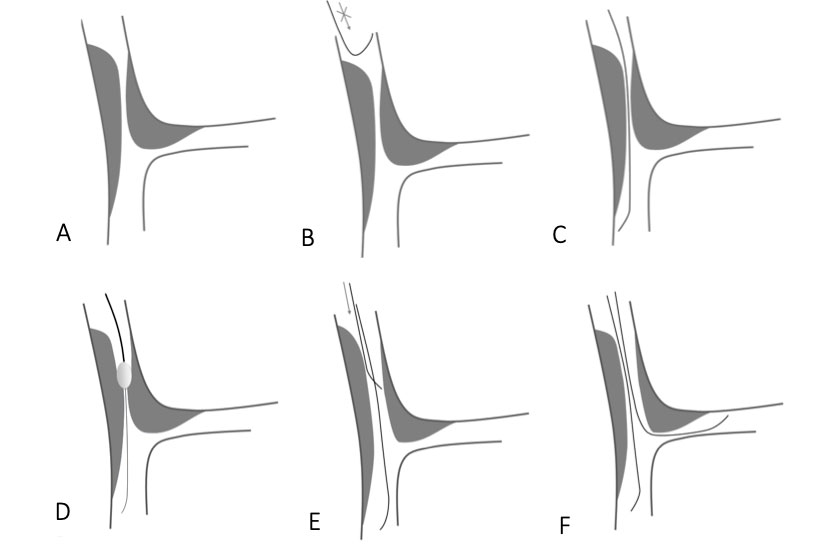
Figure 16
Schematic drawings illustrating the role of Rotablator to facilitate difficult side branch access.
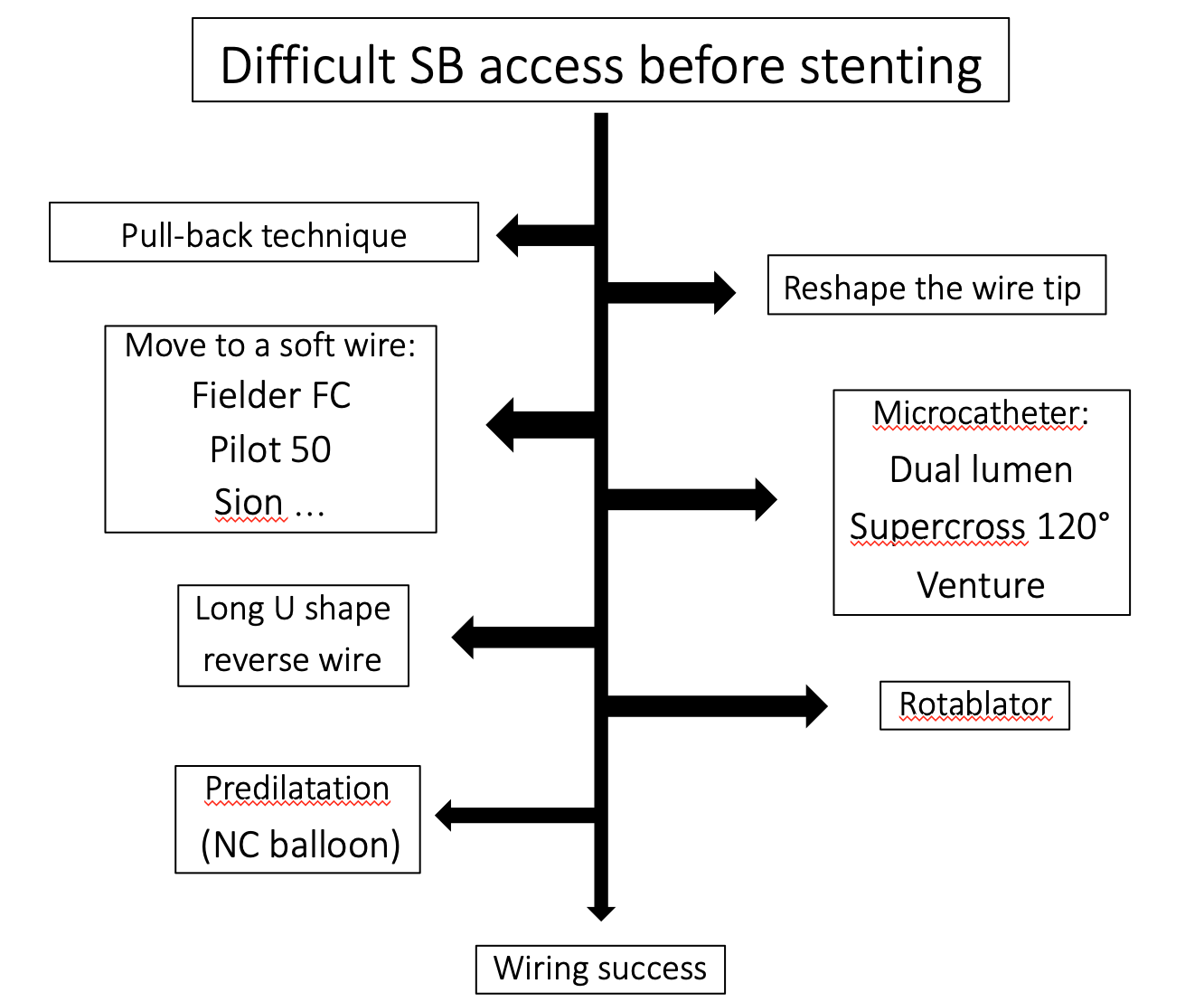
Figure 17
Side branch access technical escalation before stenting
Predilatation of the MB depends on operator’s preference based on clinical and anatomical conditions. Predilatation using kissing balloon inflation is not recommended.
Predilatation of the SB is a controversial topic. When the technique selected requires guidewire exchange for SB treatment further to MB stenting across the SB, it is preferable not to predilate the SB in order to avoid re-crossing through the struts and a dissection which can be created by predilatation. As explained above, penetration into the SB through the struts of the MB stent as close as possible to the carina causes maximal stent distorsion, i.e., the attraction of the stent opposite the SB into the MB lumen, which can have untoward consequences but can be corrected by kissing balloon inflation or “Re-POT”. The positive aspect of stent deformation is the projection of metal in the SB ostium, allowing good SB scaffolding and, when necessary, SB T-stenting without a gap. When SB ostium scaffolding is not optimal and SB lesion needs to be stented, T-stenting will not result in a good result at the SB ostium. In this case another technique such as TAP or Culotte should be used in order to obtain good SB ostium scaffolding. Stent enhancement tools permit generally to see the metal projection at the SB ostium and then choose between T-stenting, TAP or Culotte.
Stent selection for MB stenting may prove essential in large coronary artery bifurcations. The maximal opening ability of the stent cells as well as maximal stent expansion must be taken into account. The diameter of the cell must be at least equal to the diameter of the SB and the maximum expansion ability required depends on the size of the PMV, on angle A, and on the position of the stent struts in relation to the carina, which is impossible to anticipate . The diameter of the stent must be selected according to the diameter of the DM. A stent of a larger diameter, will not only increase the risk of distal dissection, but also the risk of carina shifting which may result in SB occlusion. In addition, this may change the access plan to the SB, which in such a case, becomes parallel to the MB axis rather than perpendicular to the SB axis and may hinder subsequent insertion of balloons and stents (Figure 18 upper panel). Conversely, selection of a MB stent diameter adapted to the DMV always results in stent malapposition in the PMV, with a risk of difficult guidewire exchange and increased risk of stent thrombosis. This, however, can be easily resolved by the POT (Figure 18 lower panel).
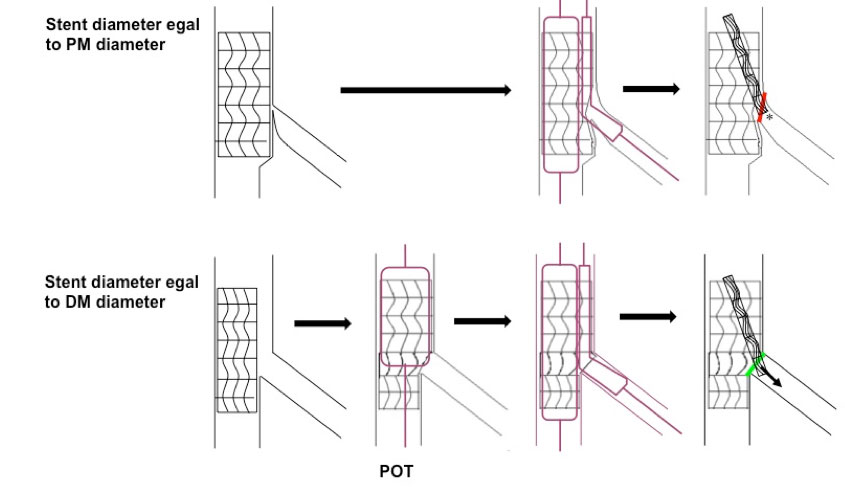
Figure 18
The crucial role of stent diameter
Upper panel: Schematic illustrating the effect of sizing the MB stent to its proximal diameter with subsequent carina shift and more challenging entry for equipment into the SB.
Lower panel: Schematic illustrating the effect of sizing the MB stent to its distal diameter with subsequent preservation of the carina and ostial SB anatomy thus allowing easier access to the SB.
The POT introduced by Darremont in 2007 (Figure 19), enables the main vessel stent positioned in two different segments to have two different diameters. The POT technique is especially useful in the presence of a large SB resulting in a major difference between the PMV and DMV diameters. This simple and very useful approach will probably be carried out with dedicated balloons in the future. However, it currently requires that the stent implanted in the PMV is long enough in order to cover the PMV proximal to the carina by at least 6 or 8 mm, which corresponds to the shortest balloons available in order to avoid geographical miss. The distal marker of the appropriately sized balloon inflated in the PMV must be positioned just proximal to the carina. The implementation of this technique results in the optimisation of the proximal stent segment, strut protrusion into the SB and larger strut opening as well as no or limited carina shifting for easier guidewire exchange.
Minimal stent length for at least a POT and a FKB if needed without geographical miss should be then 15 mm (8 mm for POT before carena and 7 mm for FKB after carena).
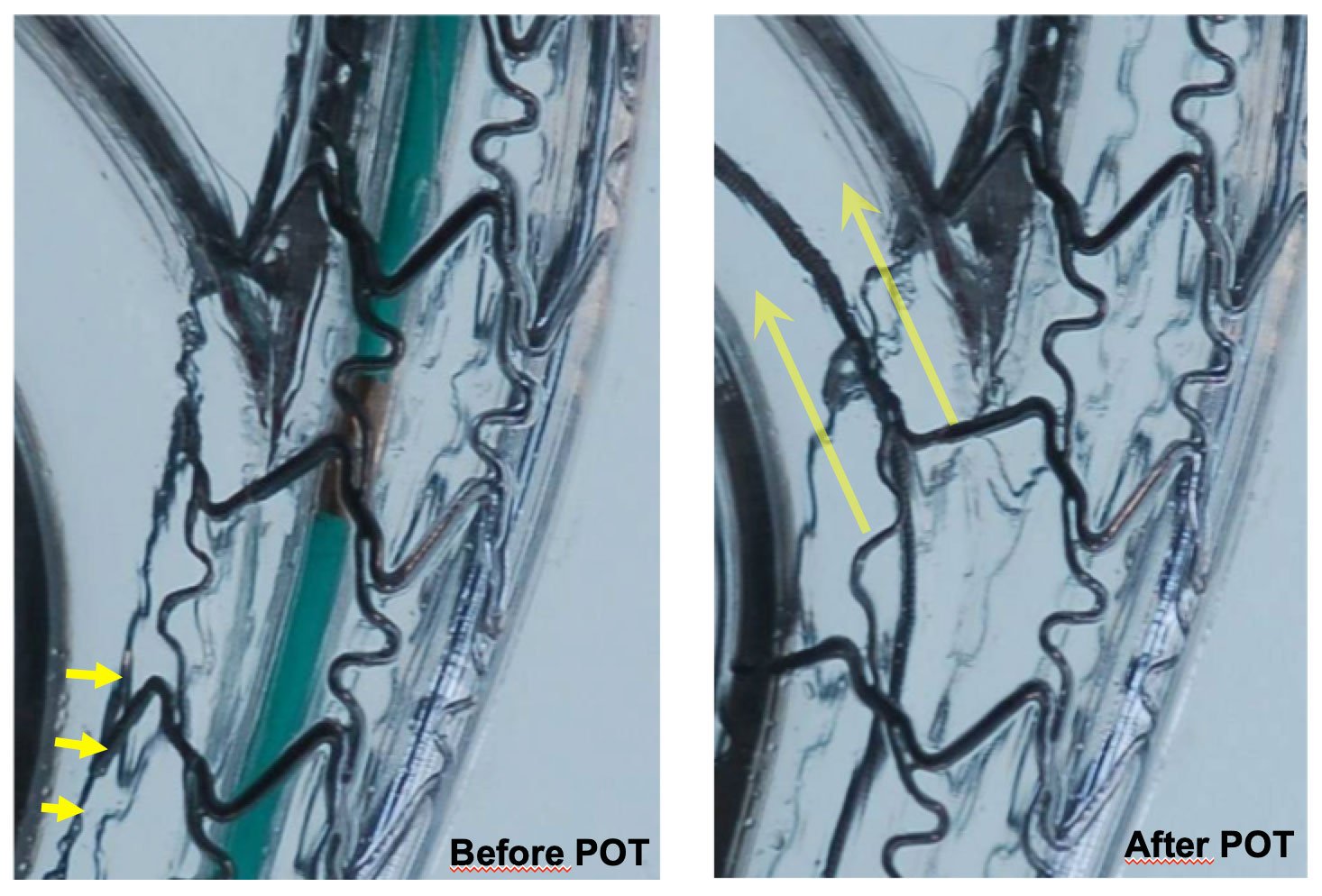
Figure 19
Role of POT
Virtual bench simulation of provisional bifurcation stenting showing the improvement in stent apposition [yellow arrow] and enlargement in cell area across the SB by use of the proximal optimisation technique.
Guidewire exchange: why? and how?
Guidewire exchange or re-crossing of the SB with a free wire is aimed at dilating the SB ostium. SB dilatation may cause MB stent distorsion, which can be corrected using FKB. Some operators are now using the Re-POT, which is very straightforward. The non-inferiority of this technique as compared to FKB has been shown in bench models and has been evaluated in a dedicated non-randomised study .
SB dilatation may be performed only in the presence of inadequate results in the SB ostium (“cross-over technique”). It may also be performed systematically in order to eliminate all stent struts in front of the SB, which may cause flow disruption leading to thrombosis and promoting neo-atherosclerosis. It could also hinder subsequent access to the SB and be a substatum for the creation of bridges of endothelium at the SB ostium creating a false restenosis. The decision not to treat a SB, which is unsuitable for stenting is probably warranted in a patient with normal flow, no angina and no ECG signs. All other settings may be debated.
Guidewire exchange starts by inserting the wire of the stented artery (MB) into the SB (or by using a third wire). Once made into an optimal distal tip shape and correctly orientated, this guidewire facilitates passage into the SB through the most distal strut (Figure 20) next to the carina using the pull-back technique (Figure 21). When removing the “jailed” wire from the SB, care must be taken to avoid guiding catheter deep intubation using the “left hand control” in order to avoid deep intubation of the guide which may lead coronary dissection or stent longitudinal compression (Figure 22). Guidewires with a short and accentuated shape may allow re-crossing through the PMV and preclude passage outside the stent struts (although this has become an unusual problem, thanks to the POT performed immediately after MB stenting). The re-crossing of the MB stent struts towards the SB may prove more difficult in certain instances. A number of tips may be useful in this situation . In most of the cases performing a second POT and/or use of hydrophilic and softer wires will permit to re-wire the SB. In some cases dual-lumen and angulated microcatheter can also be used. In cases where the SB is occluded and cannot be re-crossed, the following bail-out technique may be used (Figure 23): a very small balloon is inserted over the jailed wire and pushed outside the stent and then inflated in order to re-establish flow in the SB and allow passage of the other wire using the conventional approach through the MB stent and then the classical provisional SB stenting approach can be performed. If re-crossing through the strut opposite the SB still proves impossible, the technique may be converted into the inverted Crush technique. A larger balloon is inserted over the “jailed” wire, crushing the MB stent with a wire protection, and a second stent is placed in the PMV towards the SB, followed by kissing inflation . In high-risk settings, protection techniques using a balloon may be implemented in the SB . In cases where removal of the “jailed” wire from the SB may prove difficult, various techniques using small balloons or micro catheter may help to resolve the problem . Strategy escalation for difficult SB access after MB stenting is summarized in (Figure 24).
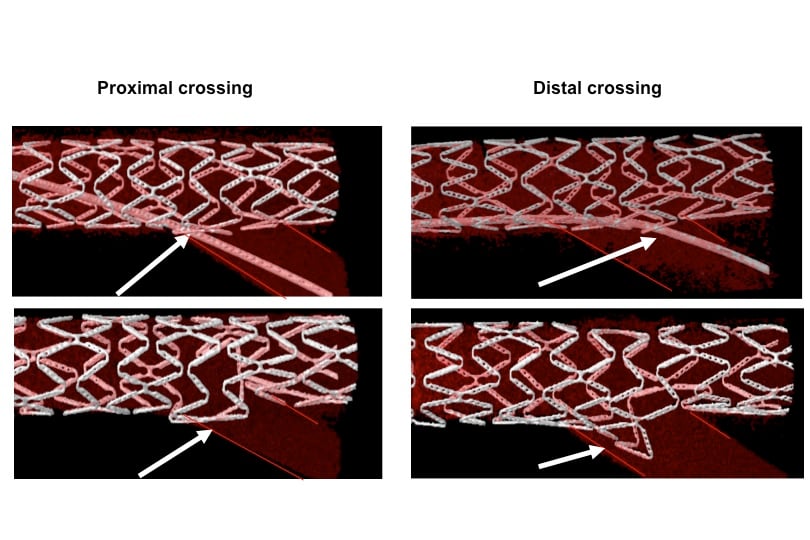
Figure 20
Schematic illustrating that crossing the distal stent strut covering the side branch ostium results in more favourable ostial stent geometry than crossing more proximally.
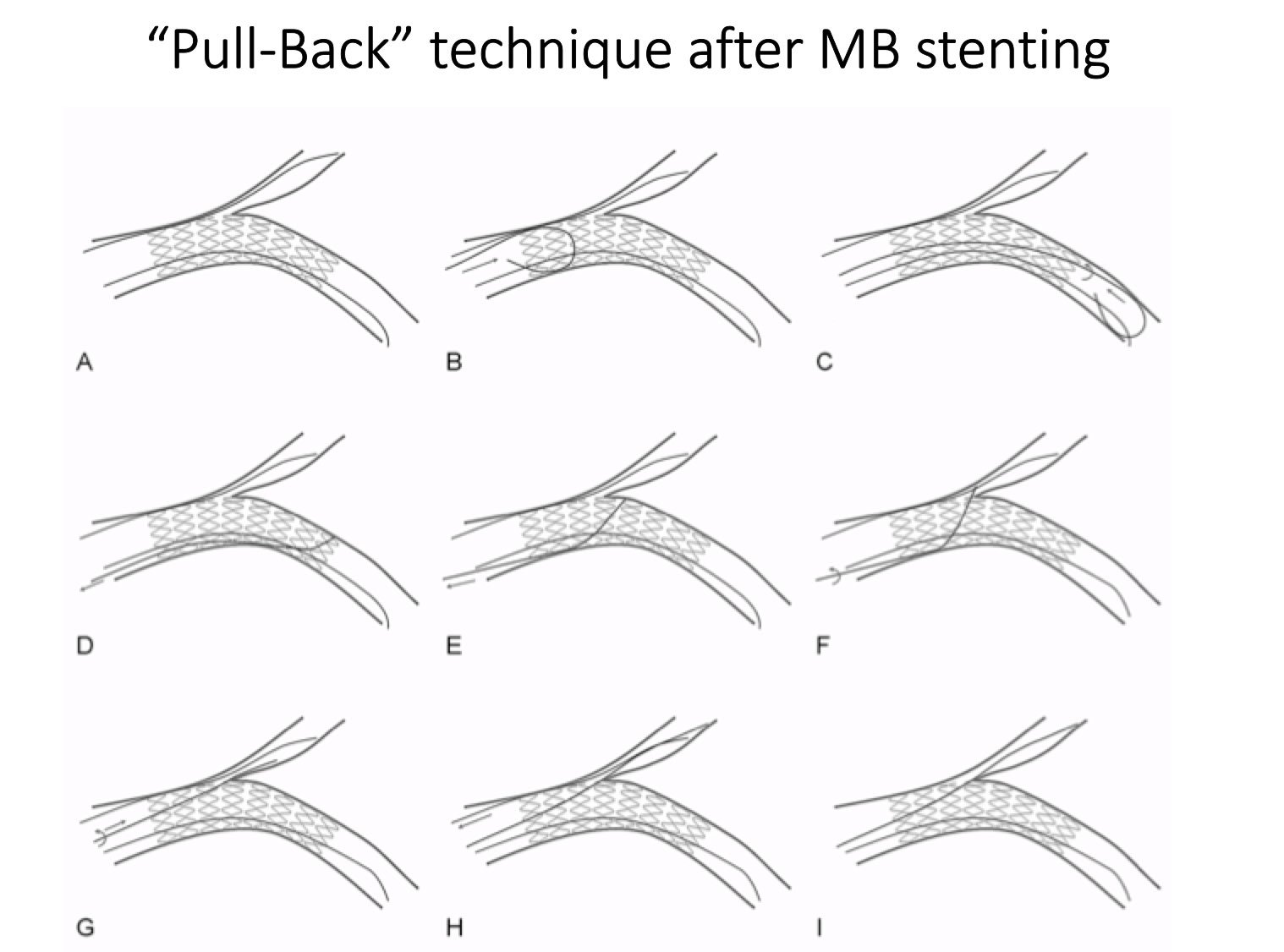
Figure 21
Schematic illustrating the wire pull-back technique to enter the SB after MB stenting and POT. This technique facilitate also crossing tyhroug a distal strut.
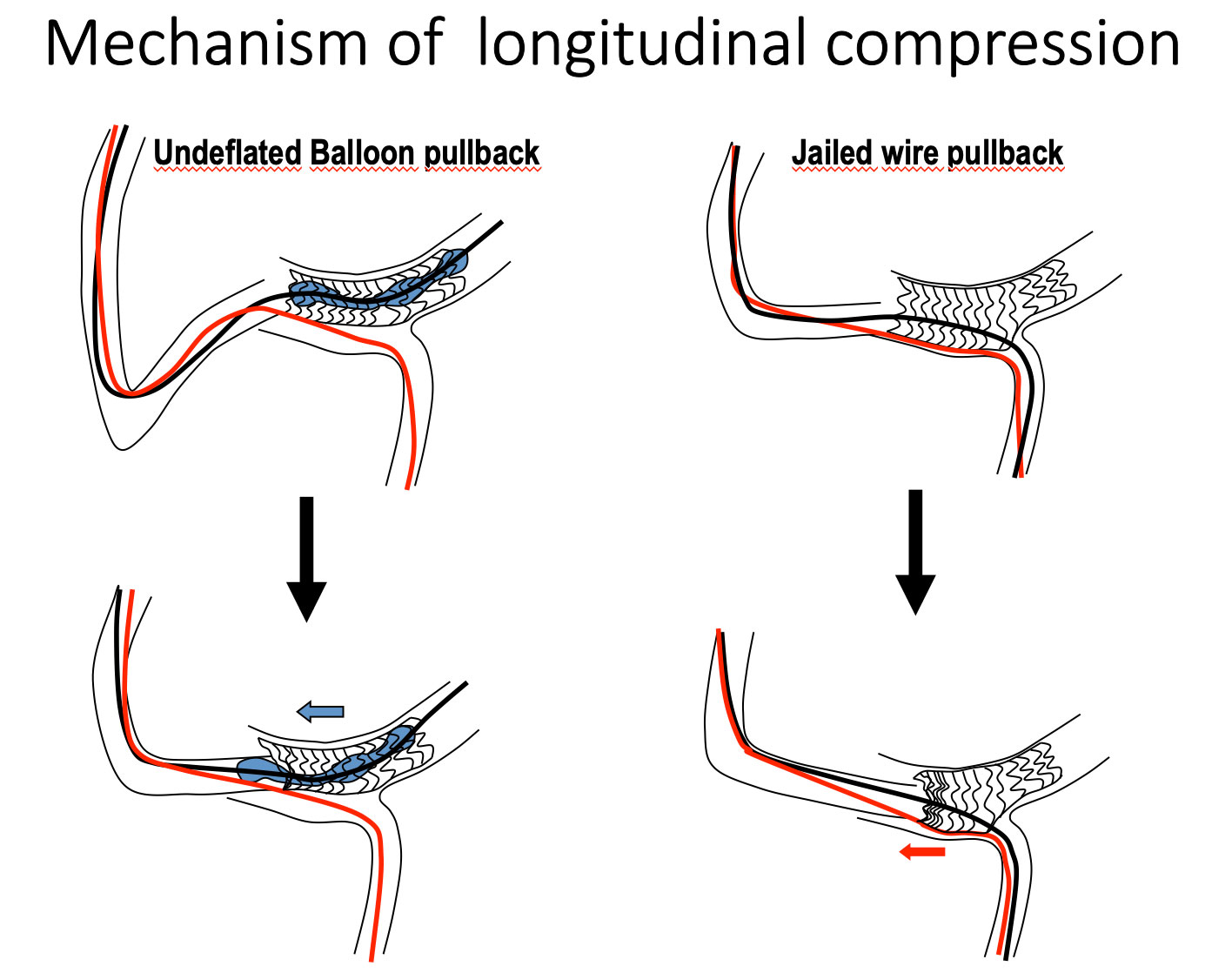
Figure 22
Schematic illustrating the risk of longitudinal compression when pulling-back a non fully deflated balloon (left panel) or a jaide wire without control of the guiding catheter (left hand control).
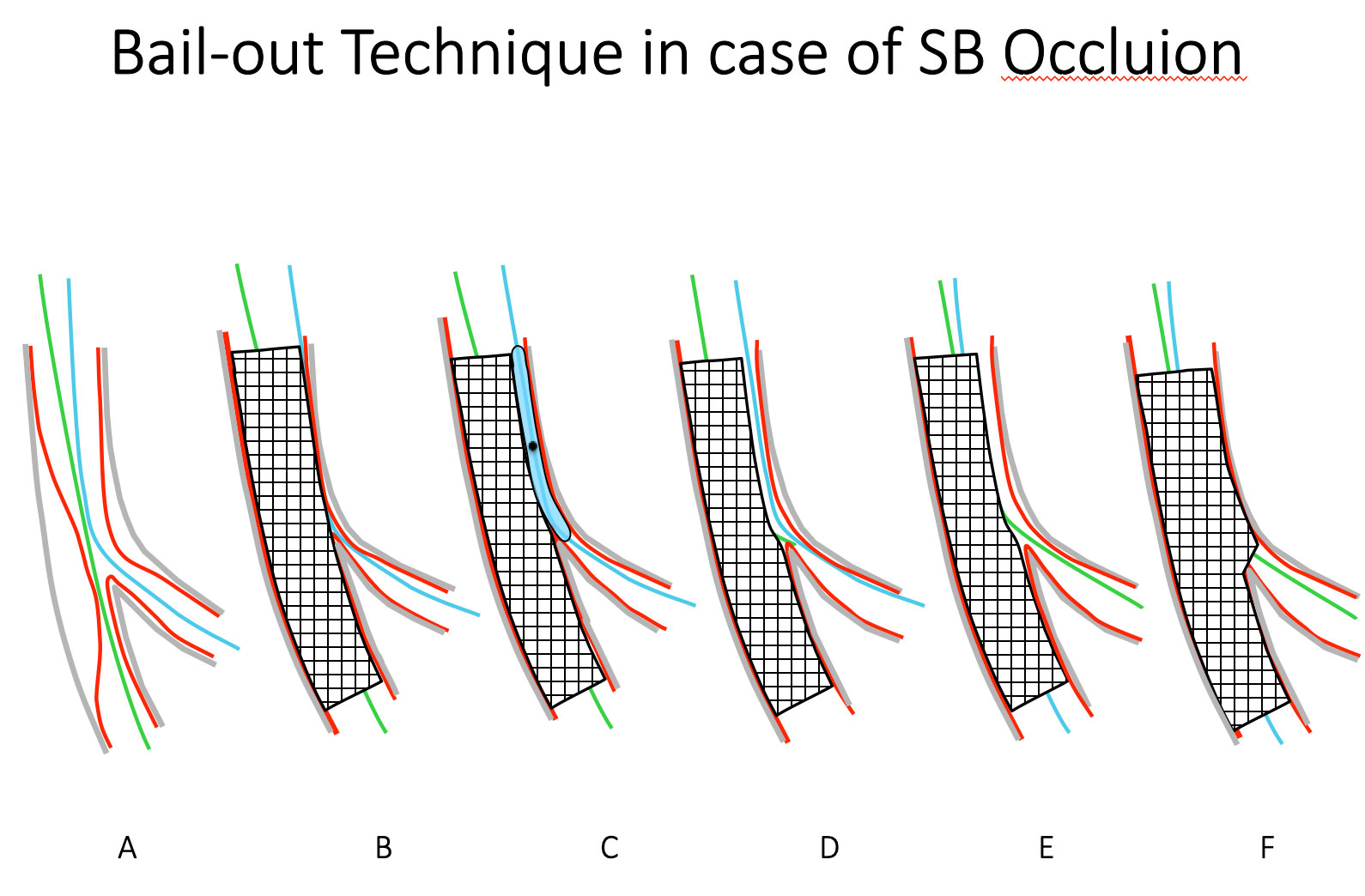
Figure 23
Bailout technique in the case of ostial SB occlusion. Inflating a small diameter balloon on the SB wire behind the MB stent can re-open the SB ostium (left panel). The MB wire or a third wire can be used to cross the MB stent into the side branch.
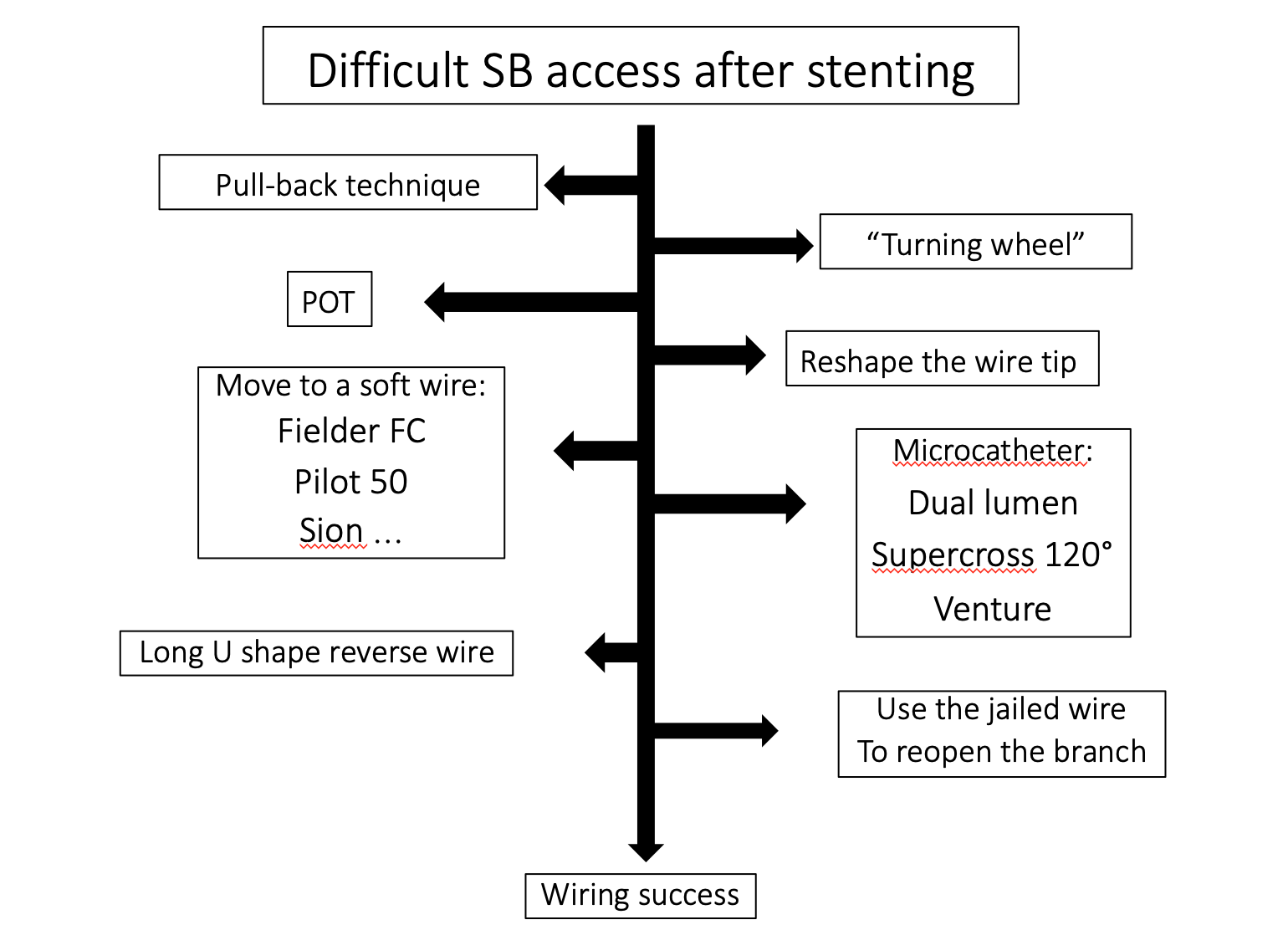
Figure 24
Summary of SB access technical escalation after stenting
Kissing balloon inflation
The benefit of performing final kissing balloon (FKB) inflation after implantation of a single stent has long been a subject of debate . It is possible that the technique used to perform FKB may also play a significant role. FKB should be carried out with balloons selected according to the diameters of the DMV and SB . Short balloons should be used to limit the risk of PMV distorsion (bottleneck effect) and prevent geographical miss. NC balloons may limit the risk of SB ostial dissection . Non-simultaneous FKB inflation (mainly SB first), long inflations and simultaneous deflation has been associated with better anatomical results in in vitro models . When two stents are used, FKB is strongly recommended . A Final POT is recommended in order to correct stent deformation if long balloons are used for FKB .
When a second stent is needed
Provisional SB stenting may be completed by implantation of a second stent. This may become necessary in order to treat a complication or in the presence of <TIMI 3 flow, unstable dissection, chest pain, ST-segment elevation or whan the SB vessel is large and the lesion length is > 5-10 mm. In cases of tight residual SB ostial stenosis, the discrepancy between the angiographic, endoluminal and physiological measurements raises some concern and it is probable that the SB is ‘over stented’ in many cases based on angiographic criteria alone.
Indeed, Koo showed that in cases where the ostial SB stenosis is by QCA < 75% post stenting, FFR nearly always > 0.80. Moreover, when the SB stenosis is greater than 75%, FFR is very infrequently < 0.80. This difference may be explained by the use of a non-dedicated QCA, by specific flow characteristics in the bifurcation (recirculation opposite the carina leading to poor SB angiographic filling), ostium ‘ovalisation’ as assessed by IVUS, combined with the fact that lesions are always angiographically visualised in the worst possible view. The use of dedicated QCA allows a good correlation between QCA and FFR, though this has never been studied in the setting of post stenting SB stenosis .
The implantation of a second stent may be performed using several techniques: T stenting, T and protrusion or straight Culotte (Figure 25). Before implementing the T stenting strategy, the position of the stent should be visualised in at least two views showing the SB ostium as well as the quantity of metal projected in the SB by POT and FKB (Stent enhancement is very useful at this step). The position of the stent on the balloon in relation to the proximal marker should also be taken into account. The decision between T and TAP depends on the appearance of the SB ostium and the quality of visualisation of the carena (Figure 26). TAP is preferred in case of poor visualisation of the carena and/or poor appearance of the SB ostium after FKB or POT/Side/POT. Final POT is recommended when long balloons are used for FKB, but it should be proximal in order to avoid the neocarena created by the TAP which should stay in the center of the vessel (flow divider).
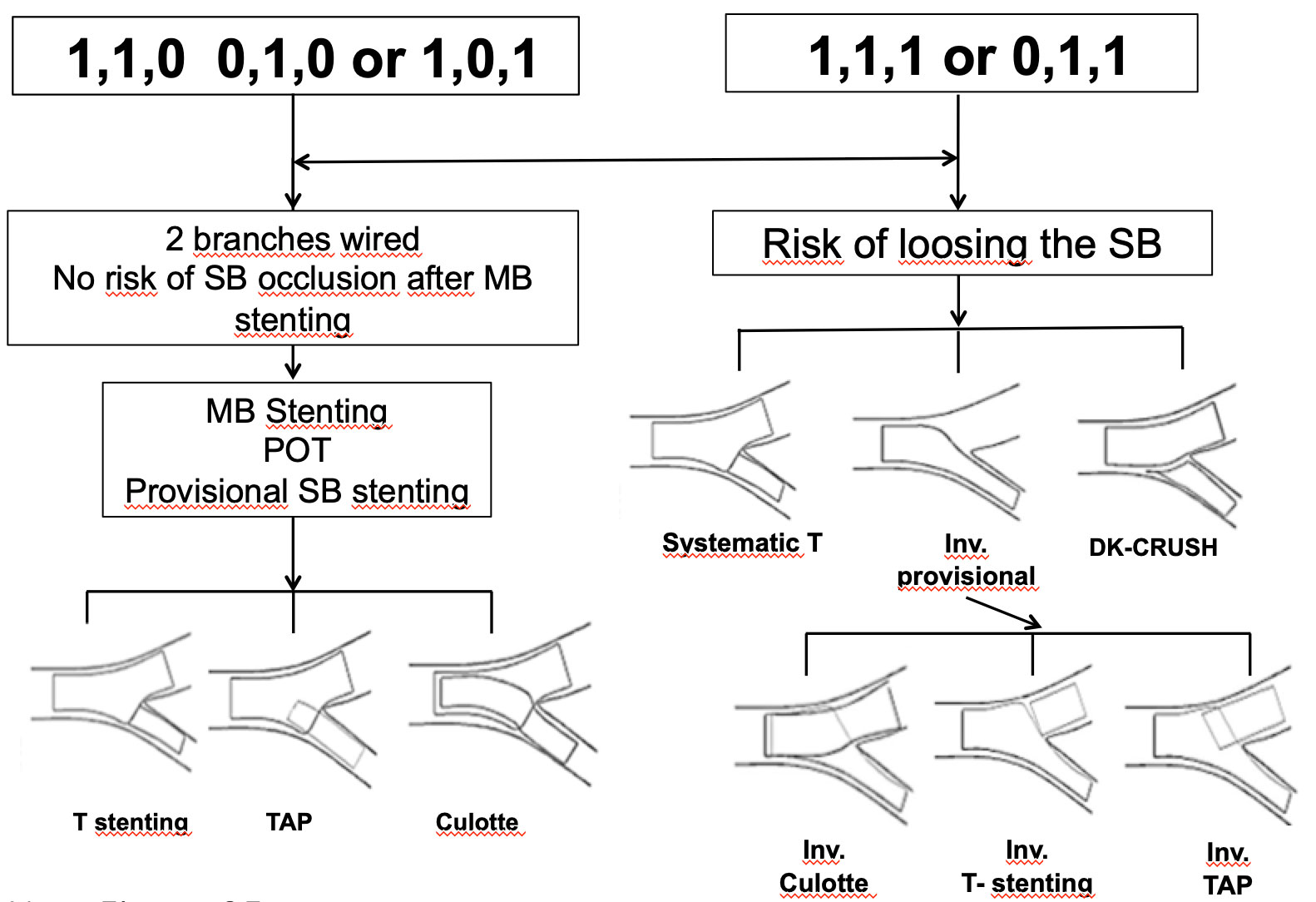
Figure 25
A simplified technical algorythm when treating a bifurcation lesion
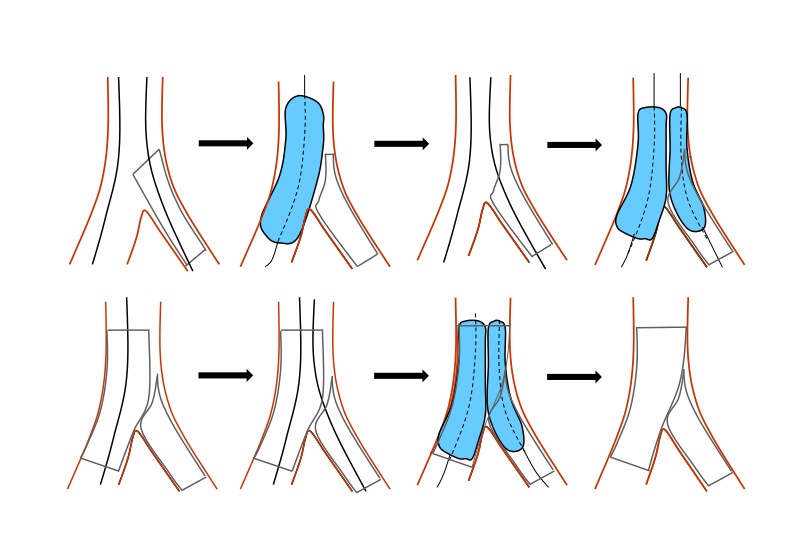
Figure 26
The difference between T and TAP technique. An optimal view of the carena is crucial.
Stent selection is crucial when applying the Culotte technique because of the difference in size between the MB and the SB. Many steps are needed including POT two times and rewiring two times (Figure 27).The Culotte technique is not optimal in the bench in case of T shape angulation .
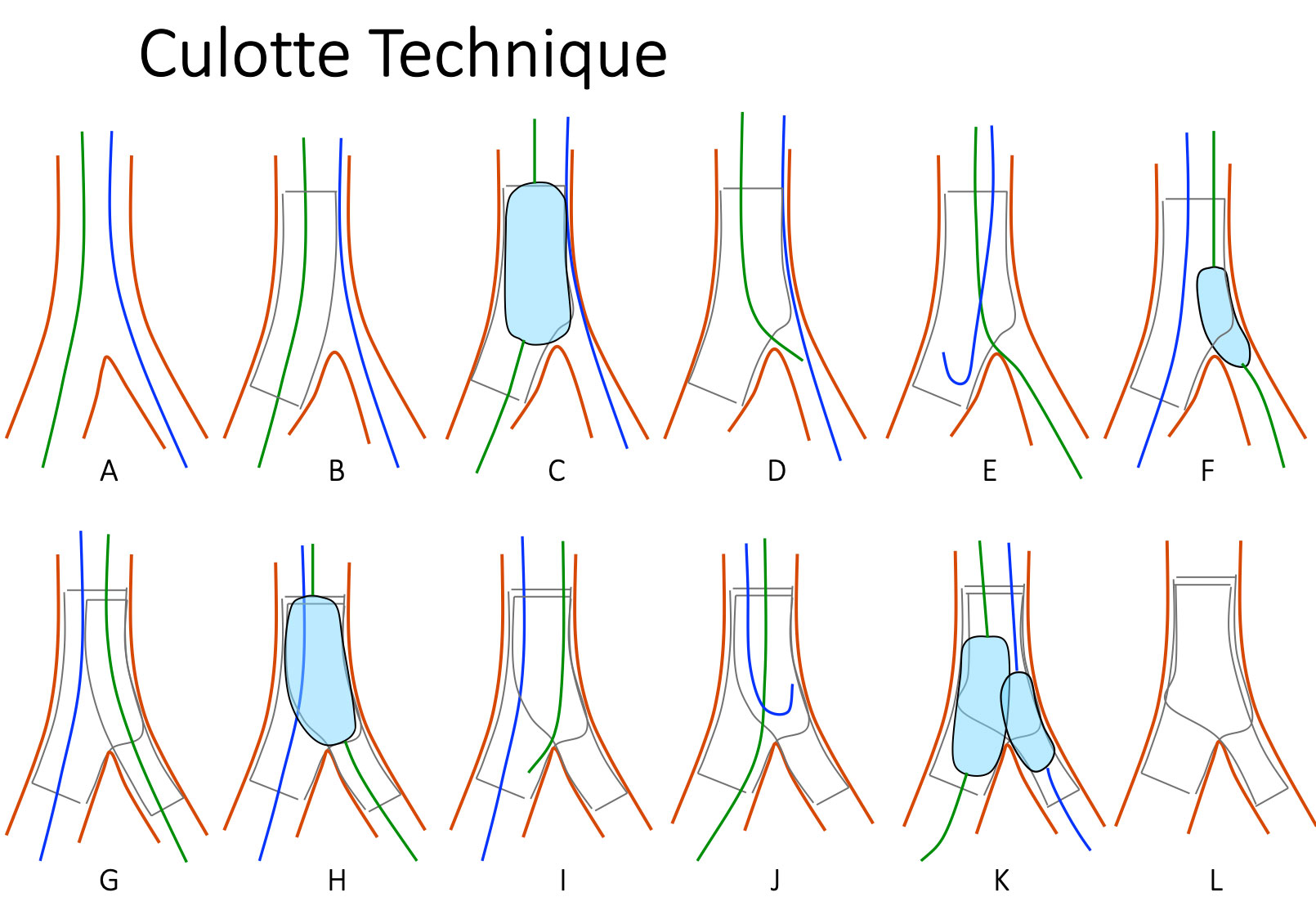
Figure 27
Schematic drawings of the Strait Culotte Technique.
This is a two-stent strategy for bifurcations. After wiring both branches, the first stent is deployed in the MB, POT is performed, SB is rewired and struts are opened, then a second stent from the PMV to the SB. After POT, the MB is rewired and a mandatory FKB is performed.
In cases where the angle or access to the SB are difficult or in 1,0,1 lesions, the provisional strategy may be inverted for technical reasons. In such instances, whether with the “inverted provisional stenting strategy” or the “inverted Culotte” (Figure 7), placement of a first sent in the PMV towards the SB is required . After deployment of the stent from the PMV to the SB, POT is crucial.
D APPROACH (DISTAL FIRST STRATEGY)
One or two stents placed over two wires are implanted in the MB and or SB without re-crossing a stent strut.
All techniques pertaining to this treatment type, which have been published or reported, are heterogeneous. Historically, the first technique to be used in lesions 0,1,1 was the V stenting also known as the “touching stents” technique . However, the mid-term outcome of this technique has proved disappointing . Simultaneous proximal implantation of two stents, whereby a neo-carina of variable length is created, allows treatment of lesions involving the PMV and is defined as SKS . This technique was used for the first time in a spontaneous coronary dissection . The only benefit of this technique lies in the fact that it can be performed easily and rapidly. The circular configuration of the two stents deployed is altered in most cases allowing the creation of an unstented channel which may favor blood stagnation and neutralise the biological effect of the stent . When one of the branches has a sharp angle, the two stents may wrap around one another . Proximal dissection may occur during simultaneous implantation, which can only be corrected by placement of two additional stents or one proximal crushing stent. The outcome of this technique, as reported in the literature, varies from acceptable to very poor (TLR up to 40%) . Certain studies have shown a high rate of stent thrombosis. A membrane growth on the neo-carina complicates the treatment of restenosis as well as any new intervention . All these techniques showed worse outcomes and should be only used without any alternative strategy.
S APPROACH (SB STENTED FIRST)
The procedure starts with stent implantation in the SB. IT should be used only when the SB is significantly diseased, considered important in terms of risk of occlusion (Figure 25), risk of significant residual ischemia or when the SB is potentially difficult to rewire or stent after MB stenting.
Classical T Stenting
The length of the stent must be commensurate with the length of the SB stenosis. The stent can be placed in the vicinity of the ostium, although this may generate a gap or result in protrusion into the MB, especially in the presence of a sharp B Angle. The presence of a gap at the SB ostium following placement of a second stent in the MB is considered the main cause of high restenosis rates in the SB. The predilatation of both branches constitutes the first step of T stenting procedures starting in the SB. In order to avoid a gap between the MB and SB stent, Colombo introduced the modified T-stenting techniques whereby the SB stent is positioned so as to protrude slightly into the MB with a second stent being positioned in the MB. After SB stent deployment, the SB wire is removed and the MB stent is implanted. Then a FKB is performed after SB rewiring. Several variations of this technique have been developed .
Inverted Culotte technique
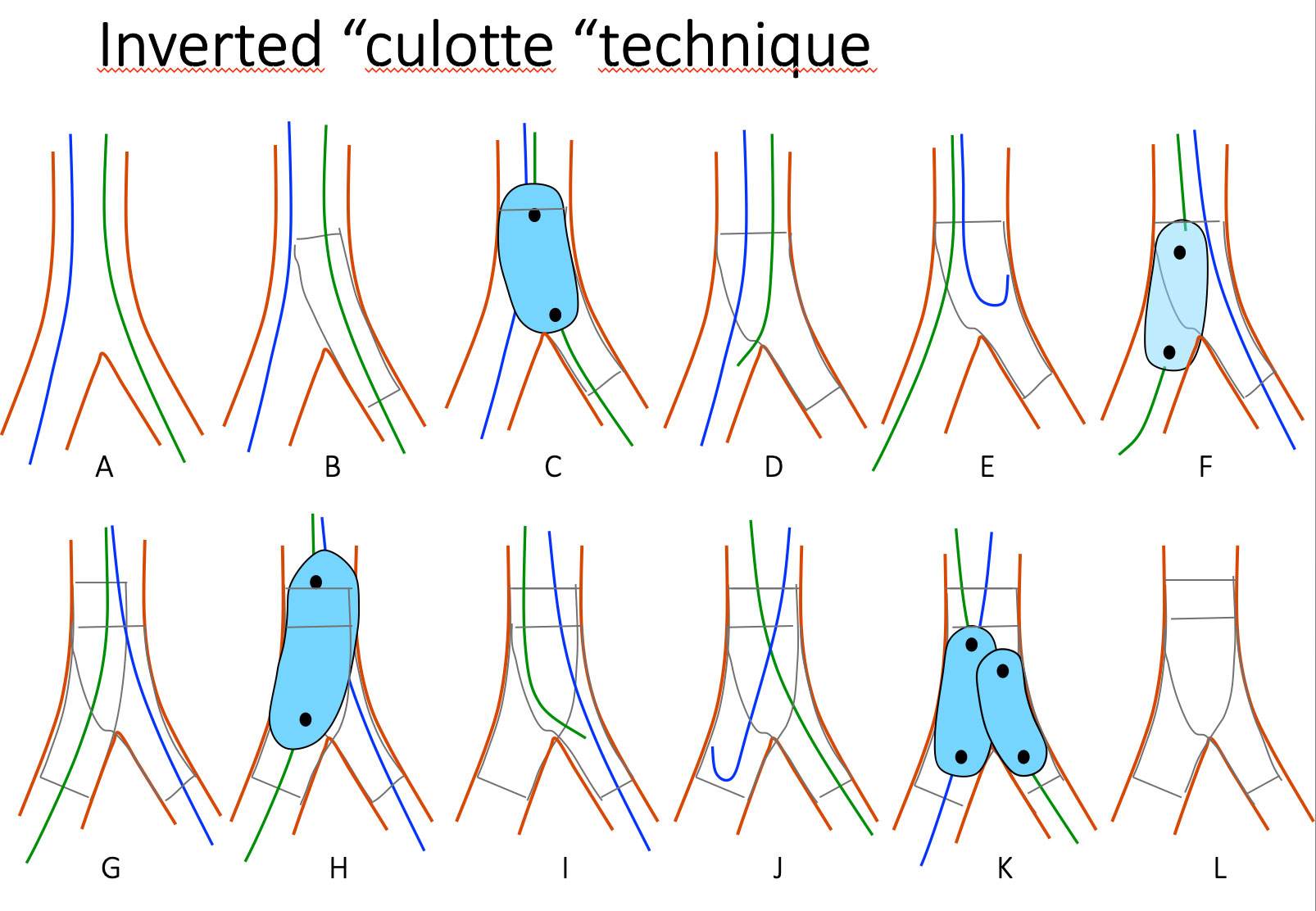
Figure 28
Schematic drawings of the Inverted Culotte Technique.
The first stent is deployed from the PMV to the side branch and simlar steps are performed like for the strait culotte technique.
This technique is part of an inverted provisional SB stenting approach and can be used when the SB is severely diseased and relatively large. After stenting the lesion from the MB to the SB, a first POT is performed. If the MB needs attention, it can be rewired throught the most distal strut and the strut open with balloon dilatation. If the MB is stented, a second POT is needed before rewiring the SB and the procedure should be completed by FKB.
Crush technique
The T-stenting technique has evolved towards a more proximal implantation of the SB stent in the PMV in order to avoid a gap between the MB and the SB stent. The SB stent protruding in the PMV is then crushed just proximal to the carena with a balloon already positioned in the MB at the beginning of the procedure. After SB wire removal, a stent is deployed in the MB stent. Then a FKB is performed after SB rewiring through a proximal strut . According to Ge , FKB is indispensable as it reduces the risk of MACE and TLR by 65% but the risk of failure to perform a FKB is aout 10-20 %. As for the Culotte strategy, a T shape angle is associated with a higher MACE rate with the Crush technique, but not with the provisional stenting strategy .
Mini Crush
The Crush technique has evolved into the mini-crush technique with a reduced length of crushed stent segment in order to reduce the amount of metal and the length of overlapping stents . Several techniques have been derived from the original strategy with only very subtle differences .
DK Crush
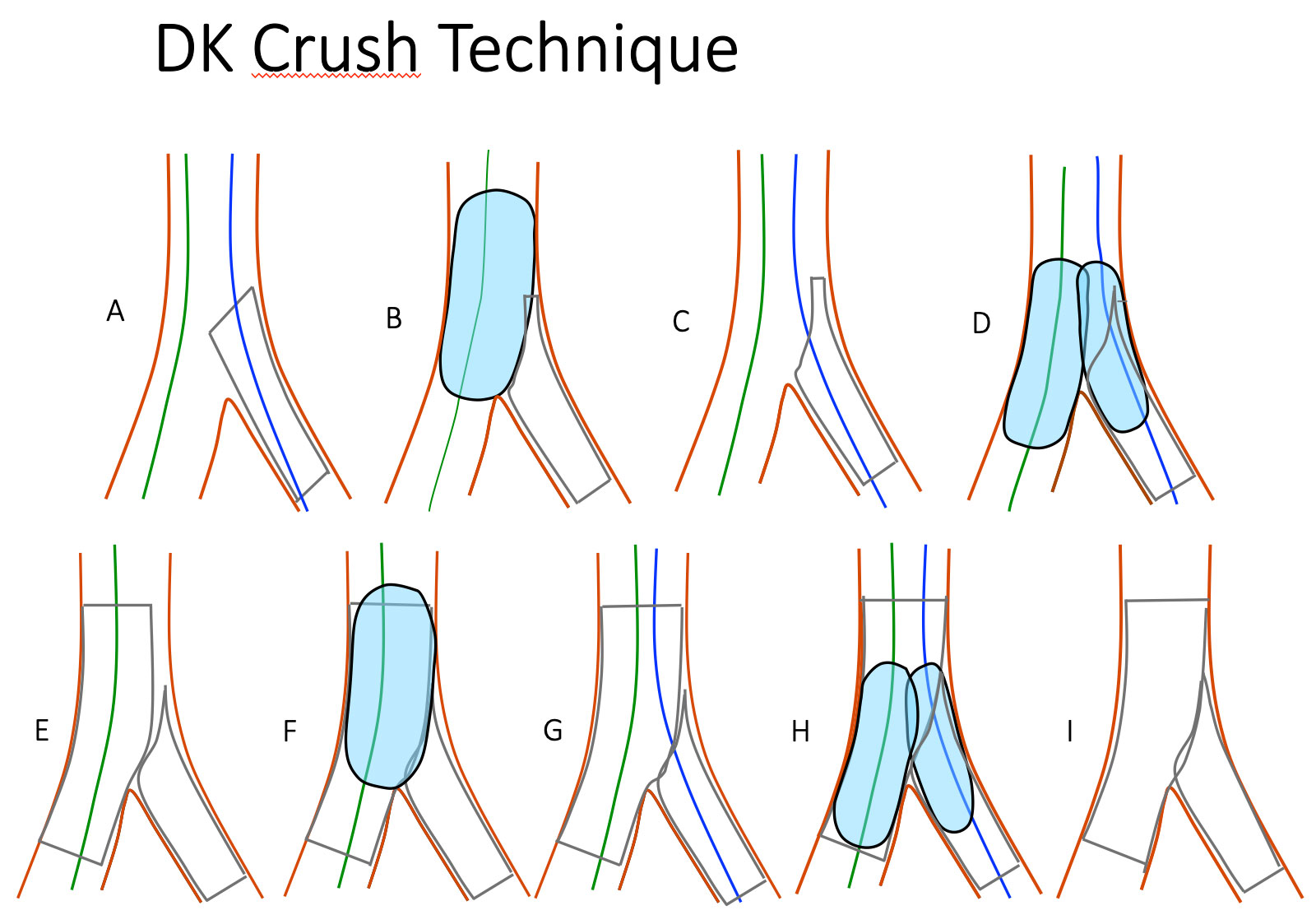
Figure 29
DK-Crush technique step by step (A) SB Stenting with protrusion. (B) SB stent balloon crush. (C) proximal SB wire recrossing. (D) First kissing balloon inflation. (E) MB stenting across the SB. (F) POT. (G) Second SB wire recrossing. (H) Second kissing balloon inflation. (H) Final result. Final POT shoul be performed if long balloons are used for kissing.
More recently Chen has shown that by adding another procedural step by doing a first kissing balloon inflation after crushing the SB stent with a balloon and then a FKB after stenting the MB, “the double kissing technique or DK crush” , the rate of FKB success was increased and the clinical outcome better . This approach is technically demanding but should be preferred compared to the classical crush or Minicrush. The size of the balloon used for crushing must be adapted to the PMV in order to achieve efficient crushing of the SB stent proximal to the carena . Contrary to the provisional SB stenting approach, guidewire re-crossing towards the SB should be carried out through a proximal strut in order to avoid externalising the wire outside the SB stent . A first kissing is performed after crushing, then the MB stent (diameter according to the distal reference) is deployed afer removing the SB wire. The proximal diameter is increased proximal to the carena using POT. The SB is rewired and FKB is performed. In order to be efficient FKB should be preceded by very high-pressure balloon inflation towards the SB, using long inflation time with NC balloons . A final POT can be used if FKB is performed using long balloons. Compared to the classic Crush strategy, the DK Crush seems to be superior in terms of repeat intervention rates as shown in the DK CRUSH 1, 2 and 3 studies , and it is not affected by the angle . Stent fractures may play a role in the occurrence of SB ostial restenosis after the Crush technique .
DEDICATED STENTS
One particular dedicated stent entails a technique whereby the PMV is stented first: the AXXESS™ stent (Biosensors International, Singapore [previously Devax, USA]), a conical, self-expandable stent coated with biolimus A9 . The stent is advanced over a single wire, preferably the wire previously inserted in the most angulated branch, until the distal part of the stent is in front of the carina. The stent is pushed forward during sheath removal and deployed so as to protrude slightly into the two distal branches. One or both distal branches may subsequently be stented with DES. The DIVERGE study , which comprised 302 patients stented in non-LM bifurcations, reported an excellent outcome (stent delivered in 99%, MACE: 7.7%, TLR: 4.3% at 9 months). This stent is well adapted to the treatment of 1,0,0 lesions. The drawbacks associated with this technique are: the fact that both branches of the bifurcation must be predilated, the number of stents required when treating true bifurcation lesions, the overlapping areas, non-adjustable length, the cost and technical expertise required for implantation.
Several stents are used with the “provisional SB stenting strategy” which provides permanent access to both branches and allows theoretical reproducible stenting of the SB ostium. These stents have been arranged into 3 categories: self-alignment devices (SLK View™ [Advanced Stent Technologies, Pleasanton, CA, USA], Frontier™ [Guidant Corporation, Santa Clara, CA, USA], Twin Rail™ [Invatec/Medtronic, Roncadelle, Italy], Nile Croco® [Minvasys, Gennevilliers, France], Petal™ [Boston Scientific, Natick, MA, USA] and Abbott SBA [Abbott Vascular, Redwood City, CA, USA]) , controlled alignment devices from TriReme (TriReme Medical Inc., Pleasanton, CA, USA) and Sidekick™ [Ymed Inc., San Diego, CA, USA]), and “no need for alignment” devices (STENTYS® self apposing stent [STENTYS, Princeton, NJ, USA]) .
Contrary to expectations, optimal use of these stents requires wide operator experience: insertion of two non-twisted wires (easier with the Frontier™ and Xience SBA™ stents which have a mandrel feature allowing simultaneous advancement of the MB and SB catheters until they reach the SB), optimal predilatation of both branches, twisted wires (detected from uneasy stent advancement) which must be corrected before further advancement by withdrawal and re-positioning of one of the wires, and anticipation of inadequate rotation requiring better preparation of the lesion. The decision as to whether the SB requires stenting should be made according to the criteria described above. A randomised study comparing the Twinrail™ vs. a non-dedicated stent in patients treated with the provisional SB stenting strategy demonstrated the superiority of the dedicated stent for technical aspects .
Implantation of the STENTYS® stent, previously coated with Paclitaxel and now with Sirolimus, is achieved by self-deployment of the stent by inflation a balloon breaking an external menbrane. the stent is well adapted to the difference in size between the proximal and distal MB. A guidewire can be inserted into the SB through the stent struts. Balloon inflation enables the connections between struts to be broken, resulting in the stent struts being pushed into the SB ostium. A second DES may be implanted in the SB as required.
A few stents are dedicated to SB stenting: The Sideguard Capella® (Cappella Medical Devices Ltd., BallyBrit, Galway, Ireland) is a conical, self-expandable, eluting stent which may be difficult to position at the ostium.
The Tryton Side Branch stent™ (Tryton Medical, Durham, NC, USA) , dedicated to SB stenting (Figure 30), is equipped with an anchoring system for implantation in the PMV. Both stents can be used as a single stent. However, they are designed to be deployed in the PMV in a T stenting and Culotte configuration respectively. Of these two stents, the most thoroughly assessed so far has been the Tryton Stent™ a bare metal device designed to simplify the culotte technique. The pivotal US trial compared a strategy of provisional SB stenting with DES to systematic SB stenting with the Tryton, followed MB stenting in true bifurcation lesions (SB lesions < 5 mm in length). 704 patients were included and followed up at 9 months . The crossover rate to a two stents technique was < 10% in the provisional SB stenting group. The primary endpoint was target vessel failure (TVF) and the secondary angiographic endpoint was in-segment % diameter stenosis of the SB at nine months. The study failed to demonstrate non-inferiority of the Tryton stent (9-month TVF 17·4% vs 12·8% respectively, P=0·11 for non inferiority), mainly due to a higher rate of peri-procedural MI in the Tryton group (15·1% vs. 10·7%, P=0·11). The SB in-segment diameter stenosis among the angiographic cohort was lower in the Tryton group compared to the provisional group (31·6% vs. 38·6%, P=0·002 for superiority). Interestingly, there was a strong interaction between the size of the SB at baseline, the treatment strategy, and TVF with the Tryton stent, indicating more favorable outcomes in larger SBs (≥2·25 mm diameter per QCA assessment), which was confirmed in a recent paper by Genereux et al . These data suggest that provisional SB stenting should remain the preferred strategy in the treatment of bifurcation lesions. On the other hand, the use of the Tryton SB stent for the treatment of bifurcation lesions involving a large SB or a SB with difficult access remains a very satisfactory approach. A new drug eluting version will be available soon and probably being assessed through a large study.
Several bifurcated stents have been and are currently under evaluation (Medtronic bifurcated stent [Medtronic, Minneapolis, MN, USA]). The main difficulty associated with these types of stent lies in lesion preparation and the potential for wire wrapping.
Figure 30
Schematic drawing of the deployed Tryton stent platform showing it’s different components. The wide stent strut aperture over the transition zone facilitates wiring of the main branch and passage of equipment.
DRUG-COATED BALLOON
In recent years, drug-coated balloon (DCB) technology has emerged as a potential alternative to drug-eluting stents (DES) to prevent restenosis. The technology carries challenges for drug release kinetics, an inability to overcome elastic recoil, and concerns as to whether it can be coupled successfully to BMS. Currently, there are several commercially available DCB in Europe (all CE approved) which all use paclitaxel as active drug and sirolimus DCB are coming. Given that the provisional T-stenting technique is the favored technique, the potential advantages of the use of DCB in the treatment of bifurcations are a homogeneous administration of the drug to the vessel wall (specifically at the SB ostium), no distortion of the original anatomy of the bifurcation and minimization of strut deformation, lower risk of polymer fracture and potential decrease in dual antiplatelet therapy.
Three randomised studies were published during the last 5 years. The DEBIUT study was a physician-initiated randomised, multicentre trial comparing the DIOR-I DCB® (Eurocor GmbH, Bonn, Germany) in MB and SB and subsequent BMS implantation in the MB versus two control groups: balloon angioplasty instead of DCB and BMS in the MB or balloon angioplasty and paclitaxel eluting stent in the MB. A total of 200 patients were included. Pre-treatment of both MB and SB with DCB failed to show angiographic and clinical superiority over conventional BMS, using a provisional T-stenting technique. Moreover DES showed superior angiographic results than DCB and BMS. The objective of the PEPCAD-BIF was to investigate, in patients treated with a provisional SB stenting strategy, the benefit of SB treatment with a DCB compared to balloon angioplasty in 64 patients included in 6 German centres. Angiographic follow-up was achieved in only 75 % of patients. The primary endpoint, late lumen loss (LLL) was 0.13 mm in the DCB vs 0.51 mm in the POBA group (p = 0.013) and restenosis rate was 6 % in the DCB group vs 26 % in the POBA group (p = 0.045). The objective of the BABILON trial was to compare the outcome of patients treated with a provisional SB stenting strategy. In the DCB group sequential MB/SB dilatation was performed, followed by with implantation of a BMS in the MB. In the other group, an everolimus DES was used for treating the MB and in the SB when needed. The primary endpoint, MB LLL at nine months was 0.31±0.48 mm in the DVB group, and 0.16±0.38 mm in the DES group (p=0.15) and the secondary endpoints MACE and TLR were higher in the DCB group (17.3% vs. 7.1%; p=0.105, and 15.4% vs. 3.6%; p=0.045), due to higher MB restenosis rate (13.5% vs. 1.8%; p=0.027). Other randomised studies, with a good design and a large number of patients are needed in this field.
What type of technique for what type of lesion?
THE PROVISIONAL SB STENTING STRATEGY IS CURRENTLY THE GOLD STANDARD TECHNIQUE
The provisional stenting strategy has been involved in almost all comparative randomised and non-randomised trials carried out so far, and has seldom been shown to be inferior to complex strategies. It is currently considered the standard technique, including for pre-market approval purposes in the USA. Comparisons have been performed in all settings of the Medina classification (except for 0,0,1) with the same results. It is currently impossible, however, to index treatment based on the classification of a lesion. The advocates of complex techniques believe, and quite correctly, that these randomised trials have not thoroughly assessed all potential anatomical settings.
WHAT ARE THE SETTINGS REQUIRING PRIMARY USE OF COMPLEX TECHNICAL STRATEGIES?
- The presence of a long lesion in the SB where stent placement may be difficult following MB stenting.
This hypothesis has been tested in the EBC2 study . The study showed non-inferiority of the provisional approach as compared to a systematic two stents technique, but of course we cannot exclude that complex patient were included. Therefore common sense is also very important and it is clear that a long and significant SB lesion will be exposed to a higher risk of restenosis after balloon angioplasty alone as compared to the deployment of a second or third generation DES. - Where access or rewiring to the SB is anticipated to be very difficult.
Stenting the SB first should be the preferred option. Different techniques are possible depending on anatomy and operator’s experience: T stenting, Culotte, DK Crush. The Tryton stent can be also a good approach in this situation especially for SB > 2.5 mm in diameter. - In cases where the risk of SB occlusion during the procedure may be associated with a risk of severe haemodynamic deterioration.
SHOULD THE BIFURCATION ANGLE INFLUENCE THE TECHNICAL APPROACH?
T-shape angulation may increase the technical difficulty and may favour a “SB first technique”.
In this kind of anatomy, T stenting should be preferred as compared to the Culotte or Crush technique.
0,0,1 LESIONS HAVE NEVER BEEN STUDIED IN ANY RANDOMISED TRIAL OR LARGE REGISTRY
These lesions are really difficult to treat and optimal medical treatment remains to date the standard of care. In cases of significant residual ischaemia, several techniques have been suggested and the salient points are summarised thus:
- Balloon angioplasty alone with provisional stenting. Use of a Cutting balloon, in particular, has been proposed as a good option to reduce the need for stenting.
- Ostial stenting, especially in the LAD in the presence of certain IVUS characteristics and certain angles . Today the provisional SB stenting approach (treating the left main toward the LAD) is implemented in the majority of cases .
- Ostial stenting is said to be more accurate when performed with the Szabo technique whereby the stent is partially deployed outside the ostium, a wire is inserted through the most proximal strut of the stent which is positioned in the un-stented distal branch. The stent is subsequently pushed in the bifurcation and blocked on the carina with the wire. Cases of stent dislodgement, however, have been reported .
- SB stenting with MB balloon crush has been proposed but very limited data are available.
- The inverted provisional stenting technique seems to be the most popular and most simple technique in large SBs .
BIORESORBABLE VASCULAR SCAFFOLDS IN BIFURCATION LESIONS
Bioresorbable scaffolds (BRS) represent a promising new technology that theoretically can eliminate the risk of late and very late stent thrombosis observed after deployment of DES. It is clear that at some point after implantation there remains no physical material that could potentially come in contact with blood to create a nidus for a stent-related thrombotic event. The most widely studied BRS to date is the biovascular scaffold (BVS), Absorb (Abbott Vascular, Santa Clara, CA), a poly-L-lactic acid (PPLA) polymer, which has shown promising results in clinical studies. These studies have included patients undergoing relatively simple PCI and have specifically excluded those with planned treatment of lesions with a side-branch ≥2 mm in diameter. The use of bifurcation techniques has been discouraged, since unlike a metallic stent, the polymeric BVS can unravel when deployed beyond recommended diameter limits. Many centres have use BVS in bifurcation lesions , but large prospective registries are lacking. Furthermore, bench testing has shown that there are many limitations with the use of complex techniques or even with FKB that may damage the MB stent. Therefore, the European Bifurcation Club has made recently important recommendation regarding BRS use in bifurcation lesions:
- Wire the SB and the MB.
- Predilate the MB
- Select the MB stent diameter according to the MB distal reference knowing the limitations of post stent deployment further dilatation.
- Use slow stent deployment (2 atmospheres every 5 seconds)
- Use the POT technique to appose the proximal part of the MB stent
- If the SB is not compromised, stop the procedure.
- If the SB is compromised, open the strut toward the SB with a NC balloon and avoid the use of a second BVS for SB treatment.
- Finish the procedure with a final POT
- If SB stenting is needed prefer a DES and finish with a “mini-kiss” .
Commercialization of the ABSORB scaffold has been stopped in 2017, but the story of BRS is probably not finished.
Bifurcation lesions in the left main coronary artery
Left main (LM) lesions with bifurcation involvement account for 70% to 85% of LM cases. The rules are very similar but of course the SB is usually more important and the fact that the guiding catheter is very close to the lesion may add some technical problems . This is discussed separately (Left main coronary artery disease (old)).
Conclusion
The treatment of bifurcation lesions has remained one of the most debated issues since the dawn of interventional cardiology. This frequently encountered and complex lesion has stimulated the interventional cardiologist’s creativity and a number of techniques have been developed and assessed. In the era of DES, the results became very acceptable with the majority of techniques, and randomised studies have confirmed that the provisional SB stenting approach should be the gold standard approach in the majority of cases.
Personal Perspective - Thierry Lefèvre and Thomas Hovasse
Future improvements and simplifications in the treatment of bifurcation lesions may come with the development and refinement of dedicated stents which may be more user-friendly and more adapted to the complex anatomy of the bifurcation lesions (the 3 diameters and need for permanent SB access). However, we are still looking for the ‘Holy Grail’, while provisional SB stenting and POT are becoming the standard of care in the majority of bifurcation lesions.
Thanks to the refinement of conventional techniques, the clinical results are so favorable today (single digit TVR and low risk of stent thrombosis) that it will be very difficult to set up randomised studies between techniques or new devices. Virtual simulation will therefore probably play a central role in assessing and comparing new bifurcation techniques, approaches, dedicated stents and new generation BRS.
- Kassab GS. Scaling laws of vascular trees: of form and function. Am J Physiol Heart Circ Physiol. 2006;290:894-903.
- Kassab GS. Functional hierarchy of coronary circulation: direct evidence of a structure-function relation. Am J Physiol Heart Circ Physiol. 2005;289:559-65.
- Kassab GS. Design of Coronary Circulation: The Minimum Energy Hypothesis. Comput Methods Appl Mech Engrg. 2007;196:3033-3042.
- Kamiya A, Takahashi T. Quantitative assessments of morphological and functional properties of biological trees based on their fractal nature. J Appl Physiol. 2007 Jun;102:2315-23.
- Murray CD. The physiological principle of minimum work: I. The vascular system and the cost of blood volume. Proc Natl Acad Sci USA. 1926;12:207-14.
- Huo Y, Kassab GS. A scaling law of vascular volume. Biophys J. 2009 Jan;96:347-53.
- Finet G, Gilard M, Perrenot B, Rioufol G, Motreff P, Gavit L, Prost R. Fractal geometry of cornary bifurcations : a quantitative coronary angiography and intravascular ultrasound analysis. EuroIntervention. 2008;3:490-98.
- Choy JS, Kassab GS. Scaling of myocardial mass to flow and morphometry of coronary arteries. J Appl Physiol. 2008;104:1259.
- Asakura T, Karino T. Flow patterns and spatial distribution of atherosclerotic lesions in human coronary arteries. Circ Res. 1990;66:1045-66.
- Kalsho G, Kassab GS. Bifurcation asymmetry of the porcine coronary vasculature and its implications on coronary flow heterogeneity. Am J Physiol Heart Circ Physiol. 2004;287:2493-500.
- Chatzizisis YS, Jonas M, Coskun AU, Beigel R, Stone BV, Maynard C, Gerrity RG, Daley W, Rogers C, Edelman ER, Feldman CL, Stone PH. Prediction of the localization of high-risk coronary atherosclerotic plaques on the basis of low endothelial shear stress: an intravascular ultrasound and histopathology natural history study. Circulation. 2008;117:993-1002.
- Shimada Y, Courtney BK, Nakamura M, Hongo Y, Sonoda S, Hassan AH, Yock PG, Honda Y, Fitzgerald PJ. Intravascular ultrasonic analysis of atherosclerotic vessel remodelling and plaque distribution of stenotic left anterior descending coronary arterial bifurcation lesions upstream and downstream of the side branch. Am J Cardiol. 2006 Jul 15;98:193-6.
- Joner M, Finn AV, Farb A, Mont EK, Kolodgie FD, Ladich E, Kutys R, Skorija K, Gold HK, Virmani R. Pathology of drug-eluting stents in humans: delayed healing and late thrombotic risk. J Am Coll Cardiol. 2006 Jul.48;4:202-193.
- Nakazawa G, Yazdani SK, Finn AV, Vorpahl M, Kolodgie FD, Virmani R. Pathological findings at bifurcation lesions: the impact of flow distribution on atherosclerosis and arterial healing after stent implantation. J Am Coll Cardiol. 2010 Apr.55;20:87-1679.
- Van der Giessen AG, Wentzel JJ, Meijboom WB, Mollet NR, Van der Steen AF, Van de Vosse FN, de Feyter PJ, Gijsen FJ. Plaque and shear stress distribution in human coronary bifurcations: a multislice computed tomography study. EuroIntervention. 2009;4:654-61.
- Medina A, Martín P, Suárez de Lezo J, Nóvoa J, Melián F, Hernández E, Suárez de Lezo J, Pan M, Burgos L, Amador C, Morera O, García A. Ultrasound Study of the Prevalence of Plaque at the Carina in Lesions That Affect the Coronary Bifurcation. Implications for Treatment With Provisional Stent. Rev Esp Cardiol. 2011;64:43-50.
- Zack PM, Ischinger T. Experience with a technique for coronary angioplasty of bifurcational lesions. Cathet Cardiovasc Diagn. 1984;10:433-43.
- Meier B, Gruentzig AR, King SB 3rd, Douglas JS Jr, Hollman J, Ischinger T, Aueron F, Galan K. Risk of side branch occlusion during coronary angioplasty. Am J Cardiol. 1984;53:10-4.
- Pinkerton CA, Slack JD, Van Tassel JW, Orr CM. Angioplasty for dilatation of complex coronary artery bifurcation stenosis. Am J Cardiol. 1985;55:1626-8.
- Colombo A, Gaglione A, Nakamura S, Finci L. Kissing stents for bifurcation coronary lesion. Cathet Cardiovasc Diagn. 1993;30:327-30.
- Nakamura S, Hall P, Maiello L, Colombo A. Techniques for Palmaz-Schatz stent deployment in lesions with a large side branch. Cathet Cardiovasc Diagn. 1995;34:353-61.
- Laham RJ, Carrozza JP, Baim DS. Treatment of unprotected left main stenosis with Palmaz-Schatz stenting. Cathet Cardiovasc Diagn. 1996;37:77-80.
- Tierstein PS . Kissing Palmaz-Schatz stents for coronary bifurcation stenoses. Cathet Cardiovasc Diagn. 1996;37:307-10.
- Carrie D, Karouny E, Chouairi S, Puel J. T-shaped stent placement: a technique for the treatment of dissected bifur-cation lesions. Cathet Cardiovasc Diagn. 1996;37:311-3.
- Sheiban I, Albiero R, Marsico F, Dharmadhikari A, Tzifos V, Pagnotta P, Montorfano M, Leonardo F, Saba P, Di Mario C, Colombo A. Immediate and long-term results of T stenting for bifurcation coronary lesions. Am J Cardiol. 2000;85:1141-4, A9.
- Fort S, Lazzam C, Schwartz L. Coronary ’Y’ stenting: a technique for angioplasty of bifurcation stenoses. Can J Cardiol. 1996;12:678-82.
- Schampaert E, Fort S, Adelman AG, Schwartz L. The V-stent: a novel technique for coronary bifurcation stenting. Cathet Cardiovasc Diagn. 1996;39:320-6.
- Khoja A, Ozbek C, Bay W, Heisel A. Trouser-like stenting: a new technique for bifurcation lesions. Cathet Cardiovasc Diagn. 1997;41:192-6.
- Di Mario C, Colombo A. Trousers-stents. How to choose the right size and shape. Cathet Cardiovasc Diagn. 1997;41:197-9.
- Carrié D, Elbaz M, Dambrin G, Saint-Cricq F, Dugrand P, Fourcade J, Puel J. Coronary stenting of bifurcation lesions using T or reverse Y configuration with Wiktor stent. Am J Cardiol. 1998;82:1418-21, A8.
- Chevalier B, Glatt B, Royer T, Guyon P. Placement of coronary stents in bifurcation lesions by the culotte technique. Am J Cardiol. 1998 Oct 15;82:943-9.
- Maillard L, Guerin Y, Drieu L, et al. A Multicenter Registry of Elective Y Reconstruction of Complex Bifurcation Lesions with Bard XT Stents. Am J Cardiol. 1998;84:50S.
- Carlier SG, Colombo A, de Scheerder I, et al. Stenting of bifurcational coronary lesions: results of the multicentric European culottes registry. European Heart Journal. 2001;22:248.
- Robinson NM, Balcon R, Layton CA, Mills PG, Timmis AD, Rothman MT. Intravascular ultrasound assessment of culotte stent deployment for the treatment of stenoses at major coronary bifurcations. J Cardiovasc Intervent. 2001;4:21-7.
- Kobayashi Y, Colombo A, Akiyama T, Reimers B, Martini G, di Mario C. Modified T stenting: a technique for kissing stents in bifurcational coronary lesion. Cathet Cardiovasc Diagn. 1998;43:323-6.
- Sheiban I, Marsico F, Pagnotta P, et al. Modified ``T’’-Stenting Technique for Kissing Stents in Bifurcational Coronary Lesions: Clinical Feasibility and Immediate Angiographic Results. Am J Cardiol. 1998; 84: 50S
- Perin MA, Martinez EE, Ambrose JA, et al. A new method for stenting bifurcation lesions with preservation of side branch access. European Heart J. 2000;21: 640.
- Kobayashi Y, Colombo A, Adamian M, Nishida T, Moussa I, Moses JW. The skirt technique: A stenting technique to treat a lesion immediately proximal to the bifurcation (pseudobifurcation). Catheter Cardiovasc Interv. 2000 ;51:347-51.
- Alberti A, Missiroli B, Nannini C. Skirt technique for coronary artery bifurcation stenting. J Invasive Cardiol. 2000;12:633-6.
- Aroney N. A new technique to guarantee access to the sidebranch during bifurcational coronary stenting. J Invas Cardiol. 2000; 12: 25-28.
- Metzger PDC, Santos RM, Bulle TM. Prospective T-Stenting of Bifurcation Lesions Using a Novel Approach with Simultaneous Stent Positioning Results in High Procedural Success with Improved Clinical Outcomes. Am J Cardiol. 2001;88:61G.
- Spedicato L, Bonin M, Bernardi G, Gelsomino S, Fioretti PM, Morocutti G. Side balloon stenting: a novel technique for bifurcation lesions. J Invasive Cardiol. 2001;13:684-8.
- Lefèvre T, Louvard Y, Morice MC, Loubeyre C, Piéchaud JF, Dumas P. Stenting of bifurcation lesions: a rational approach. J Interv Cardiol. 2001;14:573-85.
- Pan M, Suarez de Lezo J, Medina A, Romero M, Segura J, Ramírez A, Pavlovic D, Hernández E, Ojeda S, Adamuz C.. A stepwise strategy for the stent treatment of bifurcated coronary lesions. A stepwise strategy for the stent treatment of bifurcated coronary lesions. Catheter Cardiovasc Interv. 2002;55:50-7.
- Lefèvre T, Morice MC, Sengottuvel G, Kokis A, Monchi M, Dumas P, Garot P, Louvard Y. Influence of technical strategies on the outcome of coronary bifurcation stenting. EuroIntervention. 2005 May;1(1):31-7.
- Lefevre T, Louvard Y, Morice MC, et al. Stenting of Bifurcation Lesions: Seven-Month Follow-up of a Prospective Study. Am J Cardiol. 1998;84:14S.
- Chevalier B, Guyon P, Glatt B, et al. LAD-Diagonal Bifurcation Lesion: A Comparison Between Complete Stenting Versus Main-Branch Single Stenting. Am J Cardiol. 1998;84:14S.
- Pan M, Suárez de Lezo J, Medina A, Romero M, Hernández E, Segura J, Castroviejo JR, Pavlovic D, Melian F, Ramírez A, Castillo JC. Simple and complex stent strategies for bifurcated coronary arterial stenosis involving the side branch origin. Am J Cardiol. 1999 83:1320-5.
- Lefevre T, Louvard Y, Morice MC, et al. Stenting of “True” Bifurcation Lesions: Predictive Factors of Target Vessel Revascularization at Seven-Month Follow-up. Am J Cardiol. 1999; 84:23P.
- Yamashita T, Nishida T, Adamian MG, Briguori C, Vaghetti M, Corvaja N, Albiero R, Finci L, Di Mario C, Tobis JM, Colombo A. Bifurcation lesions: two stents versus one stent-immediate and follow-up results. J Am Coll Cardiol. 2000;35:1145-51-.
- Al Suwaidi J, Berger PB, Rihal CS, Garratt KN, Bell MR, Ting HH, Bresnahan JF, Grill DE, Holmes DR Jr. Immediate and long-term outcome of intracoronary stent implantation for true bifurcation lesions. J Am Coll Cardiol. 2000;35:929-36.
- Sheiban I, Albiero R, Marsico F, Dharmadhikari A, Tzifos V, Pagnotta P, Montorfano M, Leonardo F, Saba P, Di Mario C, Colombo A. Immediate and long-term results of “T”- stenting for bifurcation coronary lesions. Am J Cardiol. 2000;85:1141-44.
- Anzuini A, Briguori C, Rosanio S, Tocchi M, Pagnotta P, Bonnier H, Gimelli G, Airoldi F, Margonato A, Legrand V, Colombo A. Immediate and long-term clinical and angiographic results from Wiktor stent treatment for true bifurcation narrowings. Am J Cardiol. 2001 Dec 1;88:1246-50.
- Nakamura S, Saito S, Miyauchi T, et al. Stenting of Coronary Bifurcation Lesions: Y-Stenting, T-Stenting, Single Stenting, Immediate and Long-Term Results: Multicenter Registry in Japan. Am J Cardiol. 2002;90:13H.
- Lefevre T, Louvard Y, Morice MC, et al. Evaluation of different approaches to stenting true bifurcation lesions. European Heart Journal. 2002;4:508.
- Assali AR, Teplitsky I, Hasdai D, Rechavia E, Solodky A, Sela O, Butto N, Shor N, Fuchs S, Battler A, Kornowski R. Coronary bifurcation lesions: to stent one branch or both? J Invasive Cardiol. 2004 Sep;16:447-50.
- Hardas SP, Barron GJ, Meredith IT, Harper RW. Bifuration coronary angioplasty using a new side branch accessible stent. Cathet Cardiovasc Diagn. 1998 Sep;45:92-5.
- Colombo A, Airoldi F, Sheiban I, Di Mario C. Successful treatment of a bifurcation lesion with the Carina Bard stent: A case report. Catheter Cardiovasc Interv. 1999;48:89-92.
- Nashed G, Juergens CP, Lowe HC. Second generation bifurcation stent: the rapid development of device technology. J Invasive Cardiol. 1999 Jul;11:444-6.
- Carlier SG, van der Giessen WJ, Foley DP, Carlier SG, van der Giessen WJ, Foley DP, Kutryk MJ, Rensing BJ, Carleton ML, Serruys PW. Stenting with a true bifurcated stent: acute and mid-term follow-up results. Catheter Cardiovasc Interv. 1999;47:361-96.
- Cervinka P, Foley DP, Sabaté M, Costa MA, Serrano P, Ligthart JM, Serruys PW. Coronary bifurcation stenting using dedicated bifurcation stents. Catheter Cardiovasc Interv. 2000; 49:105-11.
- Dibie A, Chevalier B, Fajadet J, et al. First In Man Study with a Coronary Stent Specifically Designed for True Bifurcated Lesions: The DBS Stent. Am J Cardiol. 2002;90:13H.
- Toutouzas K, Stankovic G, Takagi T, Albiero R, Corvaja N, Milici C, Di Mario C, Finci L, Colombo A. A new dedicated stent and delivery system for the treatment of bifurcation lesions: preliminary experience. Catheter Cardiovasc Interv. 2003 Jan;58:34-42.
- Tsuchida K, Colombo A, Lefèvre T, Oldroyd KG, Guetta V, Guagliumi G, von Scheidt W, Ruzyllo W, Hamm CW, Bressers M, Stoll HP, Wittebols K, Donohoe DJ, Serruys PW. The clinical outcome of percutaneous treatment of bifurcation lesions in multivessel coronary artery disease with the sirolimus-eluting stent: insights from the Arterial Revascularization Therapies Study part II (ARTS II). Eur Heart J. 2007;28:433-42.
- Colombo F, Biondi-Zoccai G, Infantino V, Omedé P, Moretti C, Sciuto F, Siliquini R, Chiadò S, Trevi GP, Sheiban I. A long-term comparison of drug-eluting versus bare metal stents for the percutaneous treatment of coronary bifurcation lesions. Acta Cardiol. 2009 Oct;64:583-8.
- Colombo A, Stankovic G, Orlic D, Corvaja N, Liistro F, Airoldi F, Chieffo A, Spanos V, Montorfano M, Di Mario C. Modified T-stenting technique with crushing for bifurcation lesions: immediate results and 30-day outcome. Catheter cardiovasc Interv. 2003;60:145-51.
- Sharma SK, Choudhury A, Lee J, Kim MC, Fisher E, Steinheimer AM, Kini AS.Simultaneous kissing stents (SKS) technique for treating bifurcation lesions in medium-to-large arteries. Am J Cardiol. 2004;94:913-7.
- Colombo A, Moses JW, Morice MC, Ludwig J, Holmes DR Jr, Spanos V, Louvard Y, Desmedt B, Di Mario C, Leon MB. Randomized study to evaluate sirolimus-eluting stents implanted at coronary bifurcation lesions. Circulation. 2004;109:1244-1249.
- Louvard Y, Thomas M, Dzavik V, Hildick-Smith D, Galassi AR, Pan M, Burzotta F, Zelizko M, Dudek D, Ludman P, Sheiban I, Lassen JF, Darremont O, Kastrati A, Ludwig J, Iakovou I, Brunel P, Lansky A, Meerkin D, Legrand V, Medina A, Lefèvre T. Classification of coronary artery bifurcation lesions and treatments: time for a consensus! Catheter Cardiovasc Interv. 2008;71:175-83.
- Pan M, de Lezo JS, Medina A, Romero M, Segura J, Pavlovic D, Delgado A, Ojeda S, Melián F, Herrador J, Ureña I, Burgos L. Rapamycin-eluting stents for the treatment of bifurcated coronary lesions: a randomized comparison of a simple versus complex strategy. Am Heart J. 2004;148:857-64.
- Steigen TK, Maeng M, Wiseth R, Erglis A, Kumsars I, Narbute I, Gunnes P, Mannsverk J, Meyerdierks O, Rotevatn S, Niemelä M, Kervinen K, Jensen JS, Galløe A, Nikus K, Vikman S, Ravkilde J, James S, Aarøe J, Ylitalo A, Helqvist S, Sjögren I, Thayssen P, Virtanen K, Puhakka M, Airaksinen J, Lassen JF, Thuesen L; Nordic PCI Study Group. Randomized study on simple versus complex stenting of coronary artery bifurcation lesions: the Nordic bifurcation study. Nordic PCI Study Group. Circulation. 2006;114(18):1955-61.
- Ferenc M, Gick M, Kienzle RP, Bestehorn HP, Werner KD, Comberg T, Kuebler P, Büttner HJ, Neumann FJ. Randomized trial on routine vs. provisional T-stenting in the treatment of de novo coronary bifurcation lesions. Eur Heart J. 2008;29:2859-67.
- Colombo A, Bramucci E, Saccà S, Violini R, Lettieri C, Zanini R, Sheiban I, Paloscia L, Grube E, Schofer J, Bolognese L, Orlandi M, Niccoli G, Latib A, Airoldi F. Randomized study of the crush technique versus provisional side-branch stenting in true coronary bifurcations: the CACTUS (Coronary Bifurcations: Application of the Crushing Technique Using Sirolimus-Eluting Stents) Study. Circulation. 2009;119:71-8.
- Hildick-Smith D, de Belder AJ, Cooter N, Curzen NP, Clayton TC, Oldroyd KG, Bennett L, Holmberg S, Cotton JM, Glennon PE, Thomas MR, Maccarthy PA, Baumbach A, Mulvihill NT, Henderson RA, Redwood SR, Starkey IR, Stables RH. Randomized Trial of Simple Versus Complex Drug-Eluting Stenting for Bifurcation Lesions: The British Bifurcation Coronary Study: Old, New, and Evolving Strategies. Circulation. 2010;121:1235-43.
- Cheng WJ, Zhou YJ, Zhao YX, Nie B, Guo YH, Wang ZJ, Wang JL. Randomized study on T stenting and small protrusion technique versus simple stenting for patients with coronary artery bifurcation lesions and with big size side branch. Zhonghua Xin Xue Guan Bing Za Zhi. 2010 Feb;38:131-4.
- Mintz GS, Pichard AD, Kent KM, Satler LF, Popma JJ, Leon MB. Axial plaque redistribution as a mechanism of percutaneous transluminal coronary angioplasty. Am J Cardiol. 1996 Feb 15;77:427-30
- Ahmed JM, Mintz GS, Weissman NJ, et al. Mechanism of lumen enlargement during intracoronary stent implantation: an intravascular ultrasound study. Circulation. 2000 Jul 4;102:7-10.
- Koo BK, Waseda K, Kang HJ, Kim HS, Nam CW, Hur SH, Kim JS, Choi D, Jang Y, Hahn JY, Gwon HC, Yoon MH, Tahk SJ, Chung WY, Cho YS, Choi DJ, Hasegawa T, Kataoka T, Oh SJ, Honda Y, Fitzgerald PJ, Fearon WF. Anatomic and functional evaluation of bifurcation lesions undergoing percutaneous coronary intervention. Circ Cardiovasc Interv. 2010 Apr;3:113-9.
- Saucedo JF, Mehran R, Dangas G, Hong MK, Lansky A, Kent KM, Satler LF, Pichard AD, Stone GW, Leon MB. Long-term clinical events following creatine kinase-myocardial band isoenzyme elevation after successful coronary stenting. J Am Coll Cardiol. 2000 Apr;35:1134-41.
- Pflederer T, Ludwig J, Ropers D, Daniel WG, Achenbach S. Measurement of coronary artery bifurcation angles by multidetector computed tomography. Invest Radiol. 2006 Nov;41:793-8.
- Christensen KN, Harris SR, Froemming AT, Brinjikji W, Araoz P, Asirvatham SJ, Lachman N. Anatomic assessment of the bifurcation of the left main coronary artery using multidetector computed tomography. Surg Radiol Anat. 2010 Dec;32:903-9.
- Andriotis A, Zifan A, Gavaises M, Liatsis P, Pantos I, Theodorakakos A, Efstathopoulos EP, Katritsis D. A new method of three-dimensional coronary artery reconstruction from X-ray angiography: validation against a virtual phantom and multislice computed tomography. Catheter Cardiovasc Interv. 2008 Jan 1;71:28-43.
- Ramcharitar S, Daeman J, Patterson M, Van Guens RJ, Boersma E, Serruys PW, Van der Giessen WJ. First direct in vivo comparison of two commercially available three-dimensional quantitative coronary angiography systems. Catheter Cardiovasc Interv. 2008 Jan 1;71:44-50.
- Collingwood R, Bermudez E, Fischell TA. Comparison between three-dimensional angiographic reconstruction and intravascular ultrasound imaging for the measurement of cross-sectional luminal dimensions in intermediate coronary lesions. J Interv Cardiol. 2009 Jun;22:277-81.
- Girasis C, Serruys PW, Onuma Y, Colombo A, Holmes DR Jr, Feldman TE, Bass EJ, Leadley K, Dawkins KD, Morice MC. 3-Dimensional bifurcation angle analysis in patients with left main disease: a substudy of the SYNTAX trial (SYNergy Between Percutaneous Coronary Intervention with TAXus and Cardiac Surgery). JACC Cardiovasc Interv. 2009 Jun;22:277-81.
- Godino C, Al-Lamee R, La Rosa C, Morici N, Latib A, Ielasi A, Di Mario C, Sangiorgi GM, Colombo A. Coronary left main and non-left main bifurcation angles: how are the angles modified by different bifurcation stenting techniques? J Interv Cardiol. 2010; 23(4): 382-93.
- Dvir D, Assali A, Lev EI, Ben-Dor I, Battler A, Kornowski R. Percutaneous interventions in unprotected left main lesions: novel three-dimensional imaging and quantitative analysis before and after intervention. Cardiovasc Revasc Med. 2010 Oct-Dec;11:236-40.
- P. Koller, RD. Safian. Bifurcation Stenosis in Manual of Interventional Cardiology, Physician’s Press. 1996: 229-41.
- Spokojny AM and Sanborn TM. The bifurcation lesion. In:Ellis SG and Holmes DR. Strategic Approaches in Coronary Intervention. Williams and Wilkins, Balitmore, MD. 1996:288.
- Topol EJ. Textbook of Interventional Cardiology, 3rd edition. Philadelphia: W.B. Saunders. 1999.
- Lefèvre T, Louvard Y, Morice MC, Dumas P, Loubeyre C, Benslimane A, Premchand RK, Guillard N, Piéchaud JF. Stenting of bifurcation lesions: classification, treatments, and results. Catheter Cardiovasc Interv. 2000;49:274-83.
- Safian RD, Bifurcation lesions. In: R.D. Safian and M.S. Freed, Editors, The Manual of Interventional Cardiology, Physician’s Press, Royal Oak, MI. (2001), p. 222.
- Hoye A, van Mieghem CA, Ong AT, Aoki J, Rodriguez Granillo GA, Valgimigli M, Tsuchida K, Sianos G, McFadden E, van der Giessen WJ, de Feyter PJ, van Domburg RT, Serruys PW. Treatment of de novo bifurcation lesions: a comparison of Sirolimus- and Paclitaxel-eluting stents. EuroIntervention. 2005 May;1:24-30.
- Medina A, Suarez de Lezo J, Pan M. A new classification of coronary bifurcation lesions. Rev Esp Cardiol. 2006; 59:183.
- Movahed MR, Stinis CT. A new proposed simplified classification of coronary artery bifurcation lesions and bifurcation interventional techniques. J Invasive Cardiol. 2006; 18: 199-204.
- Movahed MR. Is it time to consider the Movahed classification as the preferred classification for coronary bifurcation lesions? EuroIntervention. 2010 Jan;5:652.
- Movahed MR. Studies involving coronary bifurcation interventions should utilize the most comprehensive and technically relevant Movahed coronary bifurcation classification for better communication and accuracy. Am J Cardiol. 2010 Apr 15;105:1204-5.
- Y-Hassan S, Lindroos MC, Sylvén C. A Novel Descriptive, Intelligible and Ordered (DINO) Classification of Coronary Bifurcation Lesions. Circ J. 2010 Dec 24.
- Lansky A, Tuinenburg J, Costa M, Maeng M, Koning G, Popma J, Cristea E, Gavit L, Costa R, Rares A, Van Es GA, Lefevre T, Reiber H, Louvard Y, Morice MC; European Bifurcation Angiographic Sub-Committee. Quantitative angiographic methods for bifurcation lesions: a consensus statement from the European Bifurcation Group. Catheter Cardiovasc Interv. 2009 Feb 1;73:258-66.
- Goktekin O, Kaplan S, Dimopoulos K, Barlis P, Tanigawa J, Vatankulu MA, Koning G, Tuinenburg JC, Mario CD. A new quantitative analysis system for the evaluation of coronary bifurcation lesions: comparison with current conventional methods. Catheter Cardiovasc Interv. 2007 Feb 1;69:172-80.
- Ramcharitar S, Onuma Y, Aben JP, Consten C, Weijers B, Morel MA, Serruys PW. A novel dedicated quantitative coronary analysis methodology for bifurcation analysis. EuroIntervention. 2008; 3: 553-557.
- Girasis C, Schuurbiers JC, Onuma Y, Aben JP, Weijers B, Boersma E, Wentzel JJ, Serruys PW. Two-dimensional quantitative coronary angiographic models for bifurcation segmental analysis: In vitro validation of caas against precision manufactured plexiglas phantoms. Catheter Cardiovasc Interv. 2010 Oct 11.
- Girasis C, Schuurbiers JC, Onuma Y, Serruys PW, Wentzel JJ. Novel bifurcation phantoms for validation of quantitative coronary angiography algorithms. Catheter Cardiovasc Interv. 2010 Jul 2.
- Holm NR, Højdahl H, Lassen JF, Thuesen L, Maeng M. Quantitative coronary analysis in the Nordic Bifurcation studies. Int J Cardiovasc Imaging. 2010 Oct 7.
- Sarno G, Garg S, Onuma Y, Girasis C, Tonino P, Morel MA, van Es GA, Pijls N, Serruys PW. Bifurcation lesions: Functional assessment by fractional flow reserve vs. anatomical assessment using conventional and dedicated bifurcation quantitative coronary angiogram. Catheter Cardiovasc Interv. 2010 Nov 15;76:817-23.
- Furukawa E, Hibi K, Kosuge M, Nakatogawa T, Toda N, Takamura T, Tsukahara K, Okuda J, Ootsuka F, Tahara Y, Sugano T, Endo T, Kimura K, Umemura S. Intravascular ultrasound predictors of side branch occlusion in bifurcation lesions after percutaneous coronary intervention. Circ J. 2005 Mar;69(3):325-30.
- Jang JS, Song YJ, Kang W, Jin HY, Seo JS, Yang TH, Kim DK, Cho KI, Kim BH, Park YH, Je HG, Kim DS. Intravascular ultrasound-guided implantation of drug-eluting stents to improve outcome. A meta-analysis. JACC. 2014 (published ahead of print).
- Chen SL, Ye F, Zhang JJ, Tian NL, Liu ZZ, Santoso T, Zhou YJ, Jiang TM, Wen SY, Kwan TW.. Intravascular ultrasound-guided systematic two-stent techniques for coronary bifurcation lesions and reduced late stent thrombosis. Catheter Cardiovasc Interv. 2013 Feb; 81(3):456-63.
- Park SJ, Kim YK, Park DW, Kim WJ, Lee SW, Suh J, Yun SC, Lee CW, MK, JH, SW, and for the MAIN-COMPARE Investigators. Impact of Intravascular Ultrasound Guidance on Long-Term Mortality in Stenting for Unprotected Left Main Coronary Artery Stenosis. Circulation Cardiovascular Interventions. 2009; 2: 167-177.
- Gonzalo N, Garcia-Garcia HM, Regar E, Barlis P, Wentzel J, Onuma Y, Ligthart J, Serruys PW.In vivo assessment of high-risk coronary plaques at bifurcations with combined intravascular ultrasound and optical coherence tomography. JACC Cardiovasc Imaging. 2009 Apr;2(4):473-82.
- Tyczynski P, Ferrante G, Moreno-Ambroj C, Kukreja N, Barlis P, Pieri E, De Silva R, Beatt K, Di Mario C. Simple versus complex approaches to treating coronary bifurcation lesions: direct assessment of stent strut apposition by optical coherence tomography. Rev Esp Cardiol. 2010 Aug;63:904-14.
- Okamura T, Onuma Y, Yamada J, Iqbal J, Tateishi H, Nao T, Oda T, Maeda T, Nakamura T, Miura T, Yano M, Serruys PW. 3D optical coherence tomography: new insights into the process of optimal rewiring of side branches during bifurcational stenting. EuroIntervention. 2014 (published ahead of print)
- Louvard Y, Lefèvre T, Morice MC. Percutaneous coronary intervention for bifurcation coronary disease. Heart. 2004 Jun;90:713-22. Review.
- Thygesen K, Alpert JS, White HD, for the Joint ESC/ACCF/AHA/WHF Task Force for the Redefinition of Myocardial Infarction. Universal definition of myocardial infarction. Eur Heart J. 2007;28:2525-2538.
- Iakovou I, Schmidt T, Bonizzoni E, Ge L, Sangiorgi GM, Stankovic G, Airoldi F, Chieffo A, Montorfano M, Carlino M, Michev I, Corvaja N, Briguori C, Gerckens U, Grube E, Colombo A. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA. 2005 May; 293:2126-30.
- Ong AT, McFadden EP, Regar E, de Jaegere PP, van Domburg RT, Serruys PW. Late angiographic stent thrombosis (LAST) events with drug-eluting stents. J Am Coll Cardiol. 2005 Jun 21;45:2088-92.
- Kuchulakanti PK, Chu WW, Torguson R, Ohlmann P, Rha SW, Clavijo LC, Kim SW, Bui A, Gevorkian N, Xue Z, Smith K, Fournadjieva J, Suddath WO, Satler LF, Pichard AD, Kent KM, Waksman R. Correlates and long-term outcomes of angiographically proven stent thrombosis with sirolimus- and paclitaxel-eluting stents. Circulation. 2006 Feb 28;113:1108-13.
- Daemen J, Wenaweser P, Tsuchida K, Abrecht L, Vaina S, Morger C, Kukreja N, Jüni P, Sianos G, Hellige G, van Domburg RT, Hess OM, Boersma E, Meier B, Windecker S, Serruys PW. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: data from a large two-institutional cohort study. Lancet. 2007 Feb 24;369:667-78.
- Mishkel GJ, Moore AL, Markwell S, Shelton ME. Correlates of late and very late thrombosis of drug eluting stents. Am Heart J. 2008 Jul;156:141-7.
- Kozuma K, Ota Y, Nagai Y, et al. Clinical and angiographic outcomes with sirolimus-eluting stent for coronary bifurcation lesions. Circ J. 2011 Jan 25;75:306-14.
- Chen SL, Santoso T, Zhang JJ, Ye F, Xu YW, Fu Q, Kan J, Paiboon C, Zhou Y, Ding SQ, Kwan TW. A randomized clinical study comparing double kissing crush with provisional stenting for treatment of coronary bifurcation lesions: results from the DKCRUSH-II (Double Kissing Crush versus Provisional Stenting Technique for Treatment of Coronary Bifurcation Lesions) trial. J Am Coll Cardiol. 2011; 57: 914-20.
- Jensen JS, Galløe A, Lassen JF, Erglis A, Kumsars I, Steigen TK, Wiseth R, Narbute I, Gunnes P, Mannsverk J, Meyerdierks O, Rotevatn S, Niemelä M, Kervinen K, Nikus K, Vikman S, Ravkilde J, James S, Aarøe J, Ylitalo A, Helqvist S, Sjögren I, Thayssen P, Virtanen K, Puhakka M, Airaksinen J, Thuesen L; Nordic-Baltic PCI Study Group.Safety in simple versus complex stenting of coronary artery bifurcation lesions. The nordic bifurcation study 14-month follow-up results. EuroIntervention. 2008 Aug;4:229-33.
- Maeng M, Holm NR, Erglis A, Kumsars I, Niemelä M, Kervinen K, Jensen JS, Galløe A, Steigen TK, Wiseth R, Narbute I, Gunnes P, Mannsverk J, Meyerdierks O, Rotevatn S, Nikus K, Vikman S, Ravkilde J, James S, Aarøe J, Ylitalo A, Helqvist S, Sjögren I, Thayssen P, Virtanen K, Puhakka M, Airaksinen J, Christiansen EH, Lassen JF, Thuesen L; Nordic-Baltic Percutaneous Coronary Intervention Study Group. Long-term results after simple versus complex stenting of coronary artery bifurcation lesions: Nordic Bifurcation Study 5-year follow-up results. J Am Coll Cardiol. 2013; 62: 30-4
- Erglis A, Kumsars I, Niemelä M, Kervinen K, Maeng M, Lassen JF, Gunnes P, Stavnes S, Jensen JS, Galløe A, Narbute I, Sondore D, Mäkikallio T, Ylitalo K, Christiansen EH, Ravkilde J, Steigen TK, Mannsverk J, Thayssen P, Hansen KN, Syvänne M, Helqvist S, Kjell N, Wiseth R, Aarøe J, Puhakka M, Thuesen L; Nordic PCI Study Group. Randomized comparison of coronary bifurcation stenting with the crush versus the culotte technique using sirolimus eluting stents: the Nordic stent technique study. Circ Cardiovasc Interv. 2009 Feb;2:27-34.
- Pan M, Medina A, Suárez de Lezo J et al. Coronary Bifurcation Lesions Treated With Simple Approach. Am J Cardiol. 2011;107:1460 -1465
- Korn HV, Yu J, Ohlow MA, Huegl B, Schulte W, Wagner A, Wassmer G, Gruene S, Petek O, Lauer B. Interventional therapy of bifurcation lesions: a TIMI flow-guided concept to treat side branches in bifurcation lesions--a prospective randomized clinical study (Thueringer bifurcation study, THUEBIS study as pilot trial). Circ Cardiovasc Interv. 2009;2:535-42.
- Niemelä M, Kervinen K, Erglis A, Holm NR, Maeng M, Christiansen EH, Kumsars I, Jegere S, Dombrovskis A, Gunnes P, Stavnes S, Steigen TK, Trovik T, Eskola M, Vikman S, Romppanen H, Mäkikallio T, Hansen KN, Thayssen P, Aberge L, Jensen LO, Hervold A, Airaksinen J, Pietilä M, Frobert O, Kellerth T, Ravkilde J, Aarøe J, Jensen JS, Helqvist S, Sjögren I, James S, Miettinen H, Lassen JF, Thuesen L; Nordic-Baltic PCI Study Group. Randomized comparison of final kissing balloon dilatation versus no final kissing balloon dilatation in patients with coronary bifurcation lesions treated with main vessel stenting: the Nordic-Baltic Bifurcation Study III. Circulation. 2009 Dec;2:535-42.
- Gwon HC, Hahn JY, Koo BK, Song YB, Choi SH, Choi JH, Lee SH, Jeong MH, Kim HS, Seong IW, Yang JY, Rha SW, Jang Y, Yoon JH, Tahk SJ, Seung KB, Park SJ. Final kissing ballooning and long-term clinical outcomes in coronary bifurcation lesions treated with 1-stent technique: results from the COBIS registry. Heart. 2012; 98: 225-31.
- Mortier P, Hikichi Y, Foin N, De Santis G, Segers P, Verhegghe B, De Beule M. Provisional stenting of coronary bifurcations: insights into final kissing balloon post-dilation and stent design by computational modeling. JACC Cardiovasc Interv. 2014; 7(3): 325-33.
- Murasato Y, Iwasaki K, Yamamoto T, Yagi T, Hikichi Y, Suematsu Y, Yamamoto T. Optimal kissing balloon inflation after single-stent deployment in a coronary bifurcation model. EuroIntervention. 2014 Feb 17. pii: 20130414-03. [Epub ahead of print]
- Biondi-Zoccai G, Sheiban I, De Servi S, Tamburino C, Sangiorgi G, Romagnoli E To kiss or not to kiss? Impact of final kissing-balloon inflation on early and long-term results of percutaneous coronary intervention for bifurcation lesions.. Heart Vessels. 2013 Sep 28. [Epub ahead of print].
- Hariki H, Shinke T, Otake H, Shite J, Nakagawa M, Inoue T, Osue T, Iwasaki M, Taniguchi Y, Nishio R, Hiranuma N, Kinutani H, Konishi A, Hirata K. Potential benefit of final kissing balloon inflation after single stenting for the treatment of bifurcation lesions--insights from optical coherence tomography observations. Circ J. 2013;77(5):1193-201. Epub 2013 Feb 27.
- Pan M, Suárez de Lezo J, Medina A, et al. Drug-eluting stents for the treatment of bifurcation lesions: a randomized comparison between paclitaxel and sirolimus stents. Am Heart J. 2007; 153(1): 15.e1-7.
- Yoshimura T, Tanaka A, Mori N, Nakamura D, Taniike M, Makino N, Egami Y, Shutta R, Tanouchi J, Nishino M. Difference of neointimal growth patterns in bifurcation lesions among four kinds of drug-eluting stents: An optical coherence tomographic study. Catheter Cardiovasc Interv. 2014 Feb 5. doi: 10.1002/ccd.25422. [Epub ahead of print].
- Costopoulos C, Latib A, Ferrarello S, Naganuma T, Sticchi A, Filippo F, Giannini F, Basavarajaiah S, Kawaguchi M, Naim C, Candreva A, Carlino M, Chieffo A, Montorfano M, Colombo A. First- versus second-generation drug-eluting stents for the treatment of coronary bifurcations. Cardiovasc Revasc Med. 2013; 14(6): 311-5.
- Hakeem A, Khan FM, Bhatti S, Samad Z, Effat MA, Eckman MH, Helmy T. Provisional vs. complex stenting strategy for coronary bifurcation lesions: meta-analysis of randomized trials. J Invasive Cardiol. 2009 Nov;21:589-95.
- Katritsis DG, Siontis GC, Ioannidis JP. Double versus single stenting for coronary bifurcation lesions: a meta-analysis. Circ Cardiovasc Interv. 2009 Oct;2(5):409-15.
- Brar SS, Gray WA, Dangas G, Leon MB, Aharonian VJ, Brar SK, Moses JW. Bifurcation stenting with drug-eluting stents: a systematic review and meta-analysis of randomised trials. EuroIntervention. 2009 Sep;5(4):475-84.
- Biondi-Zoccai G. Duplicate meta-analyses on coronary bifurcation strategies: when more is less? EuroIntervention. 2010 Jun;6:181-3.
- Zhang F, Dong L, Ge J. Simple versus complex stenting strategy for coronary artery bifurcation lesions in the drug-eluting stent era: a meta-analysis of randomised trials. Heart. 2009 Oct;95(20):1676-81. Review.
- Behan MW, Holm NR, Curzen NP, Erglis A, Stables RH, de Belder AJ, Niemelä M, Cooter N, Chew DP, Steigen TK, Oldroyd KG, Jensen JS, Lassen JF, Thuesen L, Hildick-Smith D. Simple or Complex Stenting for Bifurcation Coronary Lesions: A Patient-Level Pooled-Analysis of the Nordic Bifurcation Study and the British Bifurcation Coronary Study. Circ Cardiovasc Interv. 2011 Jan 4.
- Niccoli G, Ferrante G, Porto I, Burzotta F, Leone AM, Mongiardo R, Mazzari MA, Trani C, Rebuzzi AG, Crea F. Coronary bifurcation lesions: to stent one branch or both? A meta-analysis of patients treated with drug eluting stents. Int J Cardiol. 2010 Feb 18;139:80-91.
- Athappan G, Ponniah T, Jeyaseelan L. True coronary bifurcation lesions: meta-analysis and review of literature. J Cardiovasc Med (Hagerstown). 2010 Feb;11:103-10.
- Zamani P, Kinlay S. Long-term risk of clinical events from stenting side-branches of coronary bifurcation lesions with drug-eluting and bare-metal stents: An observational meta-analysis. Catheter Cardiovasc Interv. 2010 Sep 7.
- Pomerantz RM, Ling FS. Distortion of Palmaz-Schatz stent geometry following side-branch balloon dilation through the stent in a rabbit model. Cathet Cardiovasc Diagn. 1997;40:422-6.
- Ormiston JA, Webster MW, Ruygrok PN, Stewart JT, White HD, Scott DS. Stent deformation following simulated side-branch dilatation: a comparison of five stent designs. Catheter Cardiovasc Interv. 1999;47:258-64.
- Kinoshita T, Kobayashi Y, De Gregorio J, Nameki M, Kuroda N, Yamamoto Y, Miyazaki A, Masuda Y. Difference in security of stent jail between Palmaz-Schatz, NIR, and Multi-Link stents: the effect of balloon inflation through stent struts. Catheter Cardiovasc Interv. 1999;48:230-4.
- Stankovic G, Martini G, Ferraro M, et al. An In-Vitro Assessment of Stent Geometry for Bifurcation Lesions After Kissing Balloon Inflation. Am J Cardiol. 2001;88:60G.
- Brunel P, Leurent B, Banus Y, et al. Stent Mesh Access and Deformation in the Treatment of Coronary Bifurcation Lesions: An In Vitro-In Vivo Study. Am J Cardiol. 2002; 90:78H.
- Ormiston JA, Currie E, Webster MW, Kay P, Ruygrok PN, Stewart JT, Padgett RC, Panther MJ. Drug-eluting stents for coronary bifurcations: insights into the crush technique. Catheter Cardiovasc Interv. 2004 Nov;63:332-6.
- Murasato Y, Suzuka H, Suzuki Y. Incomplete stent apposition in a left main bifurcated lesion after kissing stent implantation. J Invasive Cardiol. 2006;18:E279-84.
- Ormiston JA, Webster MW, El Jack S, Ruygrok PN, Stewart JT, Scott D, Currie E, Panther MJ, Shaw B, O’Shaughnessy B. Drug-eluting stents for coronary bifurcations: bench testing of provisional side-branch strategies. Catheter Cardiovasc Interv. 2006;67:49-55.
- Murasato Y, Horiuchi M, Otsuji Y. Three-dimensional modeling of double-stent techniques at the left main coronary artery bifurcation using micro-focus X-ray computed tomography. Catheter Cardiovasc Interv. 2007; 1;70:211-20.
- Murasato Y.Impact of three-dimensional characteristics of the left main coronary artery bifurcation on outcome of crush stenting. Catheter Cardiovasc Interv. 2007;69:248-56.
- Mortier P, Van Loo D, De Beule M, Segers P, Taeymans Y, Verdonck P, Verhegghe B. Comparison of drug-eluting stent cell size using micro-CT: important data for bifurcation stent selection. EuroIntervention. 2008 ;4:391-6.
- Ormiston JA, Webster MW, Webber B, Stewart JT, Ruygrok PN, Hatrick RI. The crush technique for coronary artery bifurcation stenting: insights from micro-computed tomographic imaging of bench deployments. JACC Cardiovasc Interv. 2008 Aug;1:351-7.
- Hikichi Y, Inoue T, Node K. Benefits and limitations of cypher stent-based bifurcation approaches: in vitro evaluation using micro-focus CT scan. J Interv Cardiol. 2009 Apr;22:128-34.
- Murasato Y, Hikichi Y, Horiuchi M. Examination of stent deformation and gap formation after complex stenting of left main coronary artery bifurcations using microfocus computed tomography. J Interv Cardiol. 2009 Apr;22:135-44.
- Rizik DG, Klag JM, Tenaglia A, Hatten TR, Barnhart M, Warnack B. Evaluation of a bifurcation drug-eluting stent system versus provisional T-stenting in a perfused synthetic coronary artery model.
- Guérin P, Pilet P, Finet G, Gouëffic Y, N’Guyen JM, Crochet D, Tijou I, Pacaud P, Loirand G.Drug-eluting stents in bifurcations: bench study of strut deformation and coating lesions. Circ Cardiovasc Interv. 2010 Apr;3:120-6.
- Mortier P, De Beule M, Van Loo D, Verhegghe B, Verdonck P. Finite element analysis of side branch access during bifurcation stenting. Med Eng Phys. 2009 May;31:434-40.
- Wischgoll T, Choy JS, Kassab GS. Extraction of morphometry and branching angles of porcine coronary arterial tree from CT images. Am J Physiol Heart Circ Physiol. 2009 Nov;297:1949-55.
- Rizik DG, Klag JM, Tenaglia A, Hatten TR, Barnhart M, Warnack B. Evaluation of a bifurcation drug-eluting stent system versus provisional T-stenting in a perfused synthetic coronary artery model. J Interv Cardiol. 2009 Dec;22:537-46.
- Mortier P, Holzapfel GA, De Beule M, Van Loo D, Taeymans Y, Segers P, Verdonck P, Verhegghe B. A novel simulation strategy for stent insertion and deployment in curved coronary bifurcations: comparison of three drug-eluting stents. Ann Biomed Eng. 2010 Jan;38:88-99.
- Chaniotis AK, Kaiktsis L, Katritsis D, Efstathopoulos E, Pantos I, Marmarellis V. Computational study of pulsatile blood flow in prototype vessel geometries of coronary segments. Phys Med. 2010 Apr;26:140-56.
- Williams AR, Koo BK, Gundert TJ, Fitzgerald PJ, LaDisa JF Jr. Local hemodynamic changes caused by main branch stent implantation and subsequent virtual side branch balloon angioplasty in a representative coronary bifurcation. J Appl Physiol. 2010 Aug;109(2):532-40. Epub 2010 May 27.
- Gastaldi D, Morlacchi S, Nichetti R, Capelli C, Dubini G, Petrini L, Migliavacca F. Modelling of the provisional side-branch stenting approach for the treatment of atherosclerotic coronary bifurcations: effects of stent positioning. Biomech Model Mechanobiol. 2010 Oct;9:551-61.
- Moore JE Jr, Timmins LH, Ladisa JF Jr. Coronary artery bifurcation biomechanics and implications for interventional strategies. Catheter Cardiovasc Interv. 2010 Nov 15;76:836-43.
- Gundert TJ, Shadden SC, Williams AR, Koo BK, Feinstein JA, Ladisa JF Jr. A Rapid and Computationally Inexpensive Method to Virtually Implant Current and Next-Generation Stents into Subject-Specific Computational Fluid Dynamics Models. Ann Biomed Eng. 2011 May;39:1423-37.
- Helqvist S, Jørgensen E, Kelbaek H, Aljabbari S, Thuesen L, Flensted Lassen J, Saunamäki K. Percutaneous treatment of coronary bifurcation lesions: a novel extended Y technique with complete lesion stent coverage. Heart. 2006 Jul;92:981-2.
- Chevalier B, Lefevre T, Brunel P, et al. Influence of Side Branch Protection on the Results of Bifurcation Stenting: Insights from the BX Velocity Multicenter Registry. Am J Cardiol. 2001; 88[supp1 5A]:21G 53.
- Terkamp C, Gaede A, Werner PC, Terres W. Combining stenting with the double wire technique effectively prevents side branch occlusion. Z Kardiol. 2002;91:899-904.
- Louvard Y, Lefèvre T, Cherukupalli R et al . Favorable Effect of the “Jailed Wire” Technique When Stenting Bifurcation Lesions. Am J Cardiol. 2003; 6.
- Brunel P, Lefevre T, Darremont O, Louvard Y. Provisional T-stenting and kissing balloon in the treatment of coronary bifurcation lesions: results of the French multicenter TULIPE study. Catheter Cardiovasc Interv. 2006 Jul;68:67-73.
- Aliabadi D, Tilli FV, Bowers TR, Benzuly KH, Safian RD, Goldstein JA, Grines CL, O’Neill WW. Incidence and angiographic predictors of side branch occlusion following high-pressure intracoronary stenting. Am J Cardiol. 1997; 80: 994 - 997.
- Louvard Y, Sashikand G, Lefèvre T, et al. Angiographic predictors of side branch occlusion during the treatment of bicurcation lesions. Cath Cardiovasc Int. 2005 (Abstr. Supp.)
- Vassilev D, Gil RJ. Relative dependence of diameters of branches in coronary bifurcations after stent implantation in main vessel--importance of carina position. Kardiol Pol. 2008 Apr;66:371-8; discussion 379.
- Vassilev D, Gil R. Clinical verification of a theory for predicting side branch stenosis after main vessel stenting in coronary bifurcation lesions. J Interv Cardiol. 2008 Dec;21:493-503.
- Gil RJ, Vassilev D, Rzezak J, S_ysz A, Krzyzewski R, Kulawik T. Influence of parent vessel - side branch distal angle on restenosis rates after main vessel stenting in coronary bifurcation lesion. Kardiol Pol. 2009 Jan;67:36-43.
- Gil RJ, Vassilev D, Formuszewicz R, Rusicka-Piekarz T, Doganov A. The carina angle-new geometrical parameter associated with periprocedural side branch compromise and the long-term results in coronary bifurcation lesions with main vessel stenting only. J Interv Cardiol. 2009 Dec;22:1-10.
- Lilli A, Vecchio S, Giuliani G, Consoli L, Spaziani G, Chechi T, Margheri M. Venture wire control catheter in percutaneous treatment of complex coronary bifurcation. A case report. Minerva Cardioangiol. 2008 Apr;56:255-8.
- Ojeda S, Pan M, Mazuelos F, Romero M, Segura J, Pavlovic D, Crespín M, Suárez de Lezo J. Use of the Venture Wire-Control Catheter for Accessing Side Branches During Provisional Stenting: An Option for Bifurcations With an Unfavorable Anatomy. Rev Esp Cardiol. 2010 Dec;63:1487-1491.
- Burzotta F, De Vita M, Sgueglia G, Todaro D, Trani C. How to solve difficult SB access? EuroIntervention. Suppl. 2010;6:72-80.
- Vassilev D, Gil R, Kwan T, Nguyen T, Nanjundappa A, Doganov A. Extension distance mismatch--an unrecognized factor for suboptimal side branch ostial coverage in bifurcation lesion stenting. J Interv Cardiol. 2010 Aug;23:305-18.
- T. Lefevre, O. Darremont, R. Albiero. Provisional side branch stenting for the treatment of bifurcation lesions. EuroIntervention. Suppl. 2010;6:65-71
- Otsuka Y, Kokubu N, Kasahara Y. Usefulness of a 0.010-inch guidewire compatible balloon for crossing stent-jailed sidebranches. Int J Cardiol. 2009 Jun 23.
- Raja VN, Banerjee S, Brilakis ES. Use of the twin-pass catheter for wiring a jailed side branch. Hellenic J Cardiol. 2010 May-Jun;51:267-70.
- Aminian A, Dolatabadi D, Lalmand J. Small balloon inflation over a jailed wire as a bailout technique in a case of abrupt side branch occlusion during provisional stenting. J Invasive Cardiol. 2010 Sep;449-52.
- Furuichi S, Airoldi F, Colombo A. Rescue inverse crush: a way of get out of trouble. Catheter Cardiovasc Interv. 2007 Nov 1;70:708-12.
- Burzotta F, Trani C, Sianos G. Jailed balloon protection: a new technique to avoid acute side-branch occlusion during provisional stenting of bifurcated lesions. Bench test report and first clinical experience. EuroIntervention. 2010 Feb;5:809-13.
- Catakoglu AB, Aytekin V. The Highway Technique: a new stenting technique to treat coronary bifurcation lesions. EuroIntervention. 2010;5(7):821-5.
- Sezgin AT, Gullu H, Ermis N. Guidewire entrapment during jailed wire technique. J Invasive Cardiol. 2006 Aug;18(8):391-2.
- Burns AT, Gutman J, Whitbourn R. Side-branch wire entrapment during bifurcation PCI: avoidance and management. Catheter Cardiovasc Interv. 2010 Feb 15;75:351-3.
- Brueck M, Scheinert D, Flachskampf FA, Daniel WG, Ludwig J.Sequential vs. kissing balloon angioplasty for stenting of bifurcation coronary lesions. Catheter Cardiovasc Interv. 2002;55:461-6.
- Gwon HC, Choi SH, Song YB, Hahn JY, Jeong MH, Seong IW, Kim HS, Rha SW, Yang JY, Yoon JH, Tahk SJ, Seung KB, Jang Y, Park SJ. Long-term clinical results and predictors of adverse outcomes after drug-eluting stent implantation for bifurcation lesions in a real-world practice: the COBIS (Coronary Bifurcation Stenting) registry. Circ J. 2010 Oct 25;74:2322-8.
- Abdelmeguid AE. New technique for stent jail: another niche for the rotablator. Cathet Cardiovasc Diagn. 1997 Nov;42(3):321-4.
- Rahman S, Leesar T, Cilingiroglu M, Effat M, Arif I, Helmy T, Leesar MA. Impact of kissing balloon inflation on the main vessel stent volume, area, and symmetry after side-branch dilation in patients with coronary bifurcation lesions: a serial volumetric intravascular ultrasound study. JACC Cardiovasc Interv. 2013; 6: 923-31.
- Morino Y, Yamamoto H, Mitsudo K, Nagaoka M, Takeuchi H, Okamoto N, Kozuma K, Matsuzaki A, Tanabe K, Hara K, Tanabe T, Ikari Y. Functional formula to determine adequate balloon diameter of simultaneous kissing balloon technique for treatment of bifurcated coronary lesions: clinical validation by volumetric intravascular ultrasound analysis. Circ J. 2008 Jun;72:886-92.
- Mylotte D, Hovasse T, Ziani A, Lefèvre T, Dumonteil N, Louvard Y, Carrie D. Non-compliant balloons for final kissing inflation in coronary bifurcation lesions treated with provisional side branch stenting: a pilot study. EuroIntervention. 2012; 7: 1162-9
- Mortier P, Hikichi Y, Foin N, De Santis G, Segers P, Verhegghe B, De Beule M. Provisional stenting of coronary bifurcations: insights into final kissing balloon post-dilation and stent design by computational modeling. JACC Cardiovasc Interv. 2014; 7: 325-33.
- Murasato Y, Iwasaki K, Yamamoto T, Yagi T, Hikichi Y, Suematsu Y, Yamamoto T. Optimal kissing balloon inflation after single-stent deployment in a coronary bifurcation model. EuroIntervention. 2014 pii: 20130414-03. [Epub ahead of print].
- Koo BK, Kang HJ, Youn TJ, Chae IH, Choi DJ, Kim HS, Sohn DW, Oh BH, Lee MM, Park YB, Choi YS, Tahk SJ. Physiologic assessment of jailed side branch lesions using fractional flow reserve. J Am Coll Cardiol. 2005 Aug 16;46:633-7.
- Koo BK, Park KW, Kang HJ, Cho YS, Chung WY, Youn TJ, Chae IH, Choi DJ, Tahk SJ, Oh BH, Park YB, Kim HS. Physiological evaluation of the provisional side-branch intervention strategy for bifurcation lesions using fractional flow reserve. Eur Heart J. 2008 Mar;29:726-32.
- Burzotta F, Gwon HC, Hahn JY, Romagnoli E, Choi JH, Trani C, Colombo A. Modified T-stenting with intentional protrusion of the side-branch stent within the main vessel stent to ensure ostial coverage and facilitate final kissing balloon: the T-stenting and small protrusion technique (TAP-stenting). Report of bench testing and first clinical Italian-Korean two-centre experience. Catheter Cardiovasc Interv. 2007 Jul 1;70:75-82.
- Burzotta F, Sgueglia GA, Trani C, Talarico GP, Coroleu SF, Giubilato S, Niccoli G, Giammarinaro M, Porto I, Leone AM, Mongiardo R, Mazzari MA, Schiavoni G, Crea F. Provisional TAP-stenting strategy to treat bifurcated lesions with drug-eluting stents: one-year clinical results of a prospective registry. J Invasive Cardiol. 2009 Oct;21:532-7.
- Al Rashdan I, Amin H. Carina modification T stenting, a new bifurcation stenting technique: clinical and angiographic data from the first 156 consecutive patients. Catheter Cardiovasc Interv. 2009 Nov 1;74:683-90.
- Hussain F. Provisional reverse mini-crush technique for bifurcation angioplasty. J Invasive Cardiol. 2008 May;20:E154-7.
- Cortese B, Limbruno U. A new technique for the treatment of bifurcation lesions: modified reverse crushing. Indian Heart J. 2008 Nov-Dec;60:605-7.
- Robinson NM, Balcon R, Layton CA, Mills PG, Timmis AD, Rothman MT. Intravascular ultrasound assessment of culotte stent deployment for the treatment of stenoses at major coronary bifurcations. Int J Cardiovasc Intervent. 2001 Mar;4:21-27.
- Adriaenssens T, Byrne RA, Dibra A, Iijima R, Mehilli J, Bruskina O, Schömig A, Kastrati A. Culotte stenting technique in coronary bifurcation disease: angiographic follow-up using dedicated quantitative coronary angiographic analysis and 12-month clinical outcomes. Eur Heart J. 2008 Dec;29:2868-76.
- Kawasaki T, Koga H, Serikawa T. Modified culotte stenting technique for bifurcation lesions: the cross-stenting technique. J Invasive Cardiol. 2010 May;22(5):243-6.
- Girasis C, Onuma Y, Wong CK, Kukreja N, van Domburg R, Serruys P. Long-term outcome after the V stenting technique in de novo bifurcation lesions using drug-eluting stents. EuroIntervention. 2009 Jun;5:197-205.
- Sharma SK, Choudhury A, Lee J, Kim MC, Fisher E, Steinheimer AM, Kini AS. Simultaneous kissing stents (SKS) technique for treating bifurcation lesions in medium-to-large arteries. Am J Cardiol. 2004 Oct 1;94:913-7.
- Morocutti G, Werren M, Spedicato L, Bernardi G, Bonin M, Minen G, Fioretti PM. Kissing-stent technique for the treatment of spontaneous coronary artery dissection. Ital Heart J. Suppl. 2000 Dec;1:1586-90.
- Sharma SK. Simultaneous kissing drug-eluting stent technique for percutaneous treatment of bifurcation lesions in large-size vessels. Catheter Cardiovasc Interv. 2005 May;65:10-6.
- Kim YH, Park DW, Suh IW, Jang JS, Hwang ES, Jeong YH, Lee SW, Lee SW, Lee CW, Hong MK, Kim JJ, Park SW, Park SJ. Long-term outcome of simultaneous kissing stenting technique with sirolimus-eluting stent for large bifurcation coronary lesions. Catheter Cardiovasc Interv. 2007 Nov 15;70:840-6.
- Stinis CT, Hu SP, Price MJ, Teirstein PS. Three-year outcome of drug-eluting stent implantation for coronary artery bifurcation lesions. Catheter Cardiovasc Interv. 2010 Feb 15;75:309-14.
- Kinoshita Y, Katoh O, Matsubara T, Ehara M, Nasu K, Habara M, Suzuki T. First clinical experience of flower petal stenting: a novel technique for the treatment of coronary bifurcation lesions. JACC Cardiovasc Interv. 2010 Jan;3:58-65.
- Ge L, Iakovou I, Cosgrave J, Agostoni P, Airoldi F, Sangiorgi GM, Michev I, Chieffo A, Montorfano M, Carlino M, Corvaja N, Colombo A. Treatment of bifurcation lesions with two stents: one year angiographic and clinical follow up of crush versus T stenting. Heart. 2006 Mar;92:371-6.
- Hoye A, Iakovou I, Ge L, van Mieghem CA, Ong AT, Cosgrave J, Sangiorgi GM, Airoldi F, Montorfano M, Michev I, Chieffo A, Carlino M, Corvaja N, Aoki J, Rodriguez Granillo GA, Valgimigli M, Sianos G, van der Giessen WJ, de Feyter PJ, van Domburg RT, Serruys PW, Colombo A. Long-term outcomes after stenting of bifurcation lesions with the crush technique: predictors of an adverse outcome. J Am Coll Cardiol. 2006 May 16;47:1949-58.
- Ramcharitar S, Patterson MS, van Geuns RJ, Serruys PW. Magnetic navigation system used successfully to cross a crushed stent in a bifurcation that failed with conventional wires. Catheter Cardiovasc Interv. 2007 May 1;69:852-5
- Ge L, Airoldi F, Iakovou I, Cosgrave J, Michev I, Sangiorgi GM, Montorfano M, Chieffo A, Carlino M, Corvaja N, Colombo A. Clinical and angiographic outcome after implantation of drug-eluting stents in bifurcation lesions with the crush stent technique: importance of final kissing balloon post-dilation. J Am Coll Cardiol. 2005;46: 613-20.
- Chen S, Zhang J, Ye F, Chen Y, Fang W, Wei M, He B, Sun X, Yang S, Kwan TW. Final kissing balloon inflation by classic crush stenting did not improve the clinical outcomes for the treatment of unprotected left main bifurcation lesions: the importance of double-kissing crush technique. Catheter Cardiovasc Interv. 2008 Feb 1;71:166-72.
- Zhang JJ, Chen SL, Ye F, Yang S, Kan J, Liu YQ, Zhou Y, Sun XW, Zhang AP, Wang X, Chen J. Mechanisms and clinical significance of quality of final kissing balloon inflation in patients with true bifurcation lesions treated by crush stenting technique. Chin Med J (Engl). 2009 Sep 20;122:2086-91.
- Costa RA, Mintz GS, Carlier SG, Lansky AJ, Moussa I, Fujii K, Takebayashi H, Yasuda T, Costa JR Jr, Tsuchiya Y, Jensen LO, Cristea E, Mehran R, Dangas GD, Iyer S, Collins M, Kreps EM, Colombo A, Stone GW, Leon MB, Moses JW. Bifurcation coronary lesions treated with the crush technique: an intravascular ultrasound analysis. J Am Coll Cardiol. 2005 Aug 16;46:599-605.
- Collins N, Seidelin PH, Daly P, Ivanov J, Barolet A, Mackie K, Bui S, Schwartz L, Dzavík V. Long-term outcomes after percutaneous coronary intervention of bifurcation narrowings. Am J Cardiol. 2008 Aug 15;102:404-10.
- Chen SL, Zhang JJ, Ye F, Liu ZZ, Zhu ZS, Lin S, Tian NL, Fang WY, Chen YD, Sun XW, Wei M, Shan SJ, Kan J, Qian J, Yang S, Yuan ZB, Kwan TW, Hu DY. Crush stenting with drug-eluting stents: relevance of coronary bifurcation lesion location on angiographic and clinical outcomes. Clin Cardiol. 2010 Dec;33:E32-9.
- Galassi AR, Colombo A, Buchbinder M, Grasso C, Tomasello SD, Ussia GP, Tamburino C. Long-term outcomes of bifurcation lesions after implantation of drug-eluting stents with the mini-crush technique. Catheter Cardiovasc Interv. 2007 Jun 1;69:976-83.
- Galassi AR, Tomasello SD, Capodanno D, Barrano G, Ussia GP, Tamburino C. Mini-crush versus T-provisional techniques in bifurcation lesions: clinical and angiographic long-term outcome after implantation of drug-eluting stents. JACC Cardiovasc Interv. 2009 Mar;2:185-94.
- Kornowski R. The mini-crush technique for managing bifurcation lesions. Catheter Cardiovasc Interv. 2009 Jul 1;74:85-7.
- Galassi AR, Tomasello SD, Sacchetta G, Seminara D, Canonico L, Tamburino C. The mini-crush technique for the treatment of coronary trifurcation lesions. EuroIntervention. 2008 Nov;4:358-64.
- Lim PO, Dzavík V. Balloon crush: treatment of bifurcation lesions using the crush stenting technique as adapted for transradial approach of percutaneous coronary intervention. Catheter Cardiovasc Interv. 2004 Dec;63:412-6.
- Collins N, Dzavik V. A modified balloon crush approach improves side branch access and side branch stent apposition during crush stenting of coronary bifurcation lesions. Catheter Cardiovasc Interv. 2006 Sep;68:365-71.
- Yang HM, Tahk SJ, Woo SI, Lim HS, Choi BJ, Choi SY, Yoon MH, Park JS, Zheng M, Hwang GS, Kang SJ, Shin JH. Long-term clinical and angiographic outcomes after implantation of sirolimus-eluting stents with a modified mini-crush technique in coronary bifurcation lesions. Catheter Cardiovasc Interv. 2009 Jul 1;74:76-84.
- Chen SL, Ye F, Zhang JJ, Zhu ZS, Lin S, Shan SJ, Liu ZZ, Liu Y, Duan BX, Ge JB. DK crush technique: modified treatment of bifurcation lesions in coronary artery. Chin Med J. 2005; 118:1746-50.
- Jim MH, Ho HH, Miu R, Chow WH. Modified crush technique with double kissing balloon inflation (sleeve technique): a novel technique for coronary bifurcation lesions. Catheter Cardiovasc Interv. 2006;67:403-9.
- Jim MH, Ho HH, Chow WH. Treatment of a double-bifurcation lesion with sirolimus-eluting stents using the sleeve technique. J Invasive Cardiol. 2007 Jan;19:10-4.
- Chen S, Tan H, Lee M; Damras; Sumitsuji; Kawajiri. More modified crush techniques for coronary bifurcation lesions: which one is better? Catheter Cardiovasc Interv. 2007 Feb 15;69:468-9.
- Chen S, Zhang J, Ye F, Zhu Z, Lin S, Shan S, Kwan TW. DK crush (double-kissing and double-crush) technique for treatment of true coronary bifurcation lesions: illustration and comparison with classic crush. J Invasive Cardiol. 2007 Apr;19:189-93.
- Jim MH, Ho HH, Chan AO, Chow WH. Stenting of coronary bifurcation lesions by using modified crush technique with double kissing balloon inflation (sleeve technique): immediate procedure result and short-term clinical outcomes. Catheter Cardiovasc Interv. 2007 Jun 1;69:969-75.
- Chen SL, Zhang JJ, Ye F, Chen YD, Patel T, Kawajiri K, Lee M, Kwan TW, Mintz G, Tan HC. Study comparing the double kissing (DK) crush with classical crush for the treatment of coronary bifurcation lesions: the DKCRUSH-1 Bifurcation Study with drug-eluting stents. Eur J Clin Invest. 2008 Jun;38(6):361-71.
- Jim MH, Ho HH, Ko RL, Siu CW, Yiu KH, Chow WH. Long-term clinical and angiographic outcomes of the sleeve technique on non-left-main coronary bifurcation lesions. EuroIntervention. 2009;5:104-8.
- Zhang JJ, Chen SL, Ye F, Liu ZZ, Zhu ZS, Tian NL, Lin S, Shan SJ. Double kissing crush technique for treatment of true coronary bifurcation lesions: two-year clinical outcomes from DKCRUSH-1 study. Chin Med J (Engl). 2009 Mar 20;122:736-40.
- Chen SL, Kwan TW. Twenty-four-month update on double-kissing crush stenting of bifurcation lesions. J Interv Cardiol. 2009 Apr;22:121-7.
- Chen SL, Zhang JJ, Ye F, Chen YD, Fang WY, Wei M, He B, Sun XW, Yang S, Chen JG, Shan SJ, Tian NL, Li XB, Liu ZZ, Kan J, Michael L, W KT. Effect of coronary bifurcation angle on clinical outcomes in Chinese patients treated with crush stenting: a subgroup analysis from DKCRUSH-1 bifurcation study. Chin Med J (Engl). 2009 Feb 20;122(4):396-402.
- Chen SL, Santoso T, Zhang JJ, Ye F, Xu YW, Fu Q, Kan J, Paiboon C, Zhou Y, Ding SQ, Kwan TW. A randomized clinical study comparing double kissing crush with provisional stenting for treatment of coronary bifurcation lesions: results from the DKCRUSH-II (Double Kissing Crush versus Provisional Stenting Technique for Treatment of Coronary Bifurcation Lesions) trial. J Am Coll Cardiol. 2011;57:914-20.
- Chen SL, Xu B, Han YL, Sheiban I, Zhang JJ, Ye F, Kwan TW, Paiboon C, Zhou YJ, Lv SZ, Dangas GD, Xu YW, Wen SY, Hong L, Zhang RY, Wang HC, Jiang TM, Wang Y, Chen F, Yuan ZY, Li WM, Leon MB. Comparison of double kissing crush versus Culotte stenting for unprotected distal left main bifurcation lesions: results from a multicenter, randomized, prospective DKCRUSH-III study. J Am Coll Cardiol. 2013;61:1482-8.
- Surmely JF, Kinoshita Y, Dash D, Matsubara T, Terashima M, Ehara M, Ito T, Nasu K, Takeda Y, Tanaka N, Suzuki T, Katoh O. Stent strut fracture-induced restenosis in a bifurcation lesion treated with the crush stenting technique. Circ J. 2006 Jul;70:936-8.
- Verheye S, Trauthen B. Axxess Biolimus A9(R) eluting bifurcation stent system. EuroIntervention. 2007 Feb;2(4):506-8.
- Grube E, Buellesfeld L, Neumann FJ, Verheye S, Abizaid A, McClean D, Mueller R, Lansky A, Mehran R, Costa R, Gerckens U, Trauthen B, Fitzgerald PJ. Six-month clinical and angiographic results of a dedicated drug-eluting stent for the treatment of coronary bifurcation narrowings. Am J Cardiol. 2007 Jun 15;99:1691-7.
- Miyazawa A, Ako J, Hassan A, Hasegawa T, Abizaid A, Verheye S, McClean D, Neumann FJ, Grube E, Honda Y, Fitzgerald PJ. Analysis of bifurcation lesions treated with novel drug-eluting dedicated bifurcation stent system: intravascular ultrasound results of the AXXESS PLUS trial. Catheter Cardiovasc Interv. 2007 Dec 1;70(7):952-7.
- Hasegawa T, Ako J, Koo BK, Miyazawa A, Sakurai R, Chang H, Dens J, Verheye S, Grube E, Honda Y, Fitzgerald PJ. Analysis of left main coronary artery bifurcation lesions treated with biolimus-eluting DEVAX AXXESS plus nitinol self-expanding stent: intravascular ultrasound results of the AXXENT trial. Catheter Cardiovasc Interv. 2009;73(1):34-41.
- Verheye S, Agostoni P, Dubois CL, Dens J, Ormiston J, Worthley S, Trauthen B, Hasegawa T, Koo BK, Fitzgerald PJ, Mehran R, Lansky AJ. 9-month clinical, angiographic, and intravascular ultrasound results of a prospective evaluation of the Axxess selfexpanding biolimus A9-eluting stent in coronary bifurcation lesions: the DIVERGE (Drug-Eluting Stent Intervention for Treating Side Branches Effectively) study. J Am Coll Cardiol. 2009 Mar 24;53(12):1031-9.
- Ikeno F, Kim YH, Luna J, Condado JA, Colombo A, Grube E, Fitzgerald PJ, Park SJ, Yeung AC. Acute and long-term outcomes of the novel side access (SLK-View) stent for bifurcation coronary lesions: a multicenter nonrandomized feasibility study. Catheter Cardiovasc Interv. 2006 Feb;67(2):198-206.
- Lefèvre T, Ormiston J, Guagliumi G, Schultheiss HP, Quilliet L, Reimers B, Brunel P, Wijns W, Buettner HJ, Hartmann F, Veldhof S, Miquel K, Su X, van der Giessen WJ. The Frontier stent registry: safety and feasibility of a novel dedicated stent for the treatment of bifurcation coronary artery lesions. J Am Coll Cardiol. 2005 Aug 16;46(4):592-8.
- Radke PW, Jain D, Conrad A, Thomsen C, Remmel M, Kurowski V, Schunkert H, Hartmann F. Evaluation of the dedicated Frontier coronary bifurcation stent: A matched pair analysis with drug-eluting and bare metal stents. Clin Res Cardiol. 2008 Apr;97(4):260-5.
- Del Blanco B, Martí G, Bellera N, Otaegui I, Serra V, Ferreira I, Domingo E, Angel J, Candell J, García-Dorado D. Clinical and procedural evaluation of the Nile Croco® dedicated stent for bifurcations: a single centre experience with the first 151 consecutive non-selected patients. EuroIntervention. 2011;7:216-224.
- Ormiston J, Webster M, El-Jack S, McNab D, Plaumann SS. The AST petal dedicated bifurcation stent: first-in-human experience. Catheter Cardiovasc Interv. 2007 Sep;70(3):335-40.
- Johnson TW, Kay IP, Ormiston JA. A novel paclitaxel-eluting dedicated bifurcation stent: a case report from the first human use Taxus Petal trial. Catheter Cardiovasc Interv. 2009 Apr 1;73(5):637-40.
- Ormiston JA, Lefèvre T, Grube E, Allocco DJ, Dawkins KD. First human use of the TAXUS Petal paclitaxel-eluting bifurcation stent. EuroIntervention. 2010 May;6(1):46-53.
- Sorop O, Hatten TR, van Beusekom HM, Regar E, Ligthart J, Krabbendam-Peters I, Compas L, van der Giessen WJ. Dedicated Everolimus-eluting side branch access system: XIENCE SBA. EuroIntervention. Suppl. 2010, vol 6 (Suppl. J) J155-J160.
- Cervinka P, Bystron M, Spacek R, Kvasnak M, Adhikari S, Jakabcin J. Treatment of bifurcation lesions using dedicated bifurcation stents versus classic bare-metal stents. Randomized, controlled trial with 12-month angiographic follow up. J Invasive Cardiol. 2008 Oct;20(10):516-20.
- Laborde JC, Borenstein N, Behr L, Ramcharitar S. Stentys coronary bifurcation stent. EuroIntervention. 2007 May;3(1):162-5.
- Agostoni P, Verheye S. Novel self-expanding stent system for enhanced provisional bifurcation stenting: Examination by StentBoost and intravascular ultrasound. Catheter Cardiovasc Interv. 2009 Mar 1;73(4):481-7.
- Verheye S, Grube E, Ramcharitar S, Schofer JJ, Witzenbichler B, Kovac J, Hauptmann KE, Agostoni P, Wiemer M, Lefèvre T, Serruys PW, van Geuns RJ. First-in-man (FIM) study of the Stentys bifurcation stent--30 days results. EuroIntervention. 2009 Mar;4(5):566-71.
- Jilaihawi H, Farah B, Laborde JC. The use of self-expanding stents in coronary bifurcations and beyond: a paradigm revisited. EuroIntervention. 2009 Mar;4(5):669-75. Review.
- Doi H, Maehara A, Mintz GS, Dani L, Leon MB, Grube E. Serial intravascular ultrasound analysis of bifurcation lesions treated using the novel self-expanding sideguard side branch stent. Am J Cardiol. 2009 Nov 1;104(9):1216-21.
- Onuma Y, Müller R, Ramcharitar S, van Geuns RJ, Louvard Y, Morel MA, Morice MC, Davis R, Kaplan AV, Lefèvre T, Grube E, Serruys PW. Tryton I, First-In-Man (FIM) study: six month clinical and angiographic outcome, analysis with new quantitative coronary angiography dedicated for bifurcation lesions. EuroIntervention. 2008 Mar;3(5):546-52.
- Magro M, Wykrzykowska J, Serruys PW, Simsek C, Nauta S, Lesiak M, Stanislawska K, Onuma Y, Regar E, van Domburg RT, Grajek S, Geuns RJ. Six month clinical follow-up of the Tryton Side Branch Stent for the treatment of bifurcation lesions - A two centre registry analysis. Catheter Cardiovasc Interv. 2010 Sep 7.
- Onuma Y, Müller R, Ramcharitar S, van Geuns RJ, Louvard Y, Morel MA, Morice MC, Davis R, Kaplan AV, Lefèvre T, Grube E, Serruys PW. Tryton I, First-In-Man (FIM) study: six month clinical and angiographic outcome, analysis with new quantitative coronary angiography dedicated for bifurcation lesions. EuroIntervention. 2008; 3: 546-52.
- Généreux P, Kumsars I, Lesiak M, Kini A, Fontos G, Slagboom T, Ungi I, Metzger DC, Wykrzykowska JJ, Stella PR, Bartorelli AL, Fearon WF, Lefèvre T, Feldman RL, LaSalle L, Francese DP, Onuma Y, Grundeken MJ, Garcia-Garcia HM, Laak LL, Cutlip DE, Kaplan AV, Serruys PW, Leon MB. A randomized trial of a dedicated bifurcation stent versus provisional stenting in the treatment of coronary bifurcation lesions. J Am Coll Cardiol. 2015 Feb 17;65(6):533-43.
- Stella PR, Belkacemi A, Dubois C, Nathoe H, Dens J, Naber C, Adriaenssens T, van Belle E, Doevendans P, Agostoni P. A multicenter randomized comparison of drug-eluting balloon plus bare-metal stent versus bare-metal stent versus drug-eluting stent in bifurcation lesions treated with a single-stenting technique: six-month angiographic and 12-month clinical results of the drug-eluting balloon in bifurcations trial. Catheter Cardiovasc Interv. 2012; 80: 1138-46.
- Medina A, Martín P, Suárez de Lezo J, Amadora C, Suárez de Lezo J, Pan M, Meliána F, Hernández W, Burgos L, Ojeda S, Ramón Ortega J, García A. Vulnerable carina anatomy and ostial lesions in the left anterior descending coronary artery after floating-stent treatment. Rev Esp Cardiol. 2009; 62: 1240-9.
- Cubeddu RJ, Wood FO, Saylors EK, Mann T. Isolated disease of the ostium left anterior descending or circumflex artery: management using a left main stenting technique. Clinical outcome at 2 years. J Invasive Cardiol. 2007 Nov;19(11):457-61.
- Kern MJ, Ouellette D, Frianeza T. A new technique to anchor stents for exact placement in ostial stenoses: the stent tail wire or Szabo technique. Catheter Cardiovasc Interv. 2006 Dec;68:901-6.
- Applegate RJ, Davis JM, Leonard JC.Treatment of ostial lesions using the Szabo technique: a case series. Catheter Cardiovasc Interv. 2008 Nov 15;72:823-8.
- Kern MJ. Anchoring the stent: comment on treatment of ostial lesions using the Szabo technique. A case series by Applegate R et al. Catheter Cardiovasc Interv. 2008 Nov 15;72:829-30.
- Ferrer-Gracia MC, Sánchez-Rubio J, Calvo-Cebollero I. Stent dislodgement during Szabo technique. Int J Cardiol. 2009 Feb 7.
- Gutiérrez-Chico JL, Villanueva-Benito I, Villanueva-Montoto L, Vázquez-Fernández S, Kleinecke C, Gielen S, Iñiguez-Romo A. Szabo technique versus conventional angiographic placement in bifurcations 010-001 of Medina and in aorto-ostial stenting: angiographic and procedural results. EuroIntervention. 2010 Feb;5:801-8.
- Brunel P, Martin G, Bressollette E, Leurent B, Banus Y. Inverted provisional T stenting, a new technique for Medina 0,0,1 coronary bifurcation lesions: feasibility and follow-up. EuroIntervention. 2010 Feb;5:814-20.
- Grundeken MJ, Kraak RP, de Bruin DM, Wykrzykowska JJ. Three-dimensional optical coherence tomography evaluation of a left main bifurcation lesion treated with ABSORB® bioresorbable vascular scaffold including fenestration and dilatation of the side branch. Int J Cardiol. 2013; 168: e107-8.
- Lee IS, Bourantas CV, Muramatsu T, Gogas BD, Heo JH, Diletti R, Farooq V, Zhang Y, Onuma Y, Serruys PW, Garcia-Garcia HM. Assessment of plaque evolution in coronary bifurcations located beyond everolimus eluting scaffolds: serial intravascular ultrasound virtual histology study. Cardiovasc Ultrasound. 2013 Jul 20;11:25.
- Gogas BD, van Geuns RJ, Farooq V, Regar E, Heo JH, Ligthart J, Serruys PW. Three-dimensional reconstruction of the post-dilated ABSORB everolimus-eluting bioresorbable vascular scaffold in a true bifurcation lesion for flow restoration. JACC Cardiovasc Interv. 2011; 4(10): 1149-50.
- Seth A, Sengottuvelu G, Ravisekar V. Salvage of Side branch by provisional ’TAP Technique’ using absorb bioresorbable vascular scaffolds for bifurcation lesions: First case reports with technical considerations. Catheter Cardiovasc Interv. 2014 Feb 15 [Epub ahead of print].
- Miyazaki T, Costopoulos C, Sato K, Naganuma T, Panoulas VF, Figini F, Latib A, Colombo A. Strategy for optimal side-branch positioning of bioresorbable vascular scaffolds in dedicated 2-stent techniques: Insights from optical coherence tomography. Cardiovasc Revasc Med. 2014 Feb 10 [Epub ahead of print].
- Sgueglia GA, D’Errico F, Gioffrè G, De Santis A, Gaspardone A. First ad hoc bioresorbable vascular scaffold bench test: A glimpse into percutaneous bifurcation interventions. Int J Cardiol. 2014 Apr 1;172(3):604-6.
- Dzavik V, Colombo A. The absorb bioresorbable vascular scaffold in coronary bifurcations: insights from bench testing. JACC Cardiovasc Interv. 2014; 7(1): 81-8.
- Darremont O, Motreff P, Guérin O, Pillet R; Leymarie JL. BVS Bench testing in bifurcation lesions. EBC 2013. oral communication.
- Murasato Y, Finet G, Foin N. Final kissing balloon inflation: the whole story. EuroIntervention. 2015 May;11 Suppl V:V81-5.
- Kim YH, Lee JH, Roh JH et al. Randomized Comparisons Between Different Stenting Approaches for Bifurcation Coronary Lesions With or Without Side Branch Stenosis. JACC Cardiovasc Interv. 2015 Apr 20;8(4):550-60.
- Song YB, Hahn JY, Song PS et al. Randomized comparison of conservative versus aggressive strategy for provisional side branch intervention in coronary bifurcation lesions: results from the SMART-STRATEGY (SmartAngioplasty Research Team-Optimal Strategy for Side Branch Intervention in Coronary BifurcationLesions) randomized trial. JACC Cardiovasc Interv. 2012 Nov;5(11):1133-40.
- Yu CW, Yang JH, Song YB et al. Long-term clinical outcomes of final kissing ballooning in coronary bifurcation lesions treated with the 1-stent technique: results from the COBIS II registry (Korean coronary bifurcation stenting registry). JACC Cardiovasc Interv. 2015 Aug 24;8(10):1297-307.
- Finet G, Derimay F, Motreff P, Guerin P, Pilet P, Ohayon J, Darremont O, Rioufol G. Comparative Analysis of Sequential Proximal Optimizing Technique Versus Kissing Balloon Inflation Technique in Provisional Bifurcation Stenting: Fractal Coronary Bifurcation Bench Test. JACC Cardiovasc Interv. 2015 Aug 24;8(10):1308-17.
- First generation versus second generation drug-eluting stents for the treatment of bifurcations: 5-year follow-up of the LEADERS all-comers randomized trial. Grundeken MJ, Wykrzykowska JJ, Ishibashi Y, Garg S, de Vries T, Garcia-Garcia HM, Onuma Y, de Winter RJ, Buszman P, Linke A, Ischinger T, Klauss V, Eberli F, Corti R, Wijns W, Morice MC, di Mario C, Meier B, Jüni P, Yazdani A, Copt S, Windecker S, Serruys PW. Catheter Cardiovasc Interv. 2015 Dec 9.
- Differential Prognostic Effect Between First- and Second-Generation Drug-Eluting Stents in Coronary Bifurcation Lesions: Patient-Level Analysis of the Korean Bifurcation Pooled Cohorts. Lee JM, Hahn JY, Kang J, Park KW, Chun WJ, Rha SW, Yu CW, Jeong JO, Jeong MH, Yoon JH, Jang Y, Tahk SJ, Gwon HC, Koo BK, Kim HS. JACC Cardiovasc Interv. 2015 Aug 24;8(10):1318-31.
- Généreux P, Kini A, Lesiak M, Kumsars I, Fontos G, Slagboom T, Ungi I, Metzger DC, Wykrzykowska JJ, Stella PR, Bartorelli AL, Fearon WF, Lefèvre T, Feldman RL, Tarantini G, Bettinger N, Minalu Ayele G, LaSalle L, Francese DP, Onuma Y, Grundeken MJ, Garcia-Garcia HM, Laak LL, Cutlip DE, Kaplan AV, Serruys PW, Leon MB. Outcomes of a dedicated stent in coronary bifurcations with large side branches: A subanalysis of the randomized TRYTON bifurcation study. Catheter Cardiovasc Interv. 2015 Sep 23.
- Drug eluting balloons as stand alone procedure for coronary bifurcational lesions: results of the randomized multicenter PEPCAD-BIF trial. Kleber FX, Rittger H, Ludwig J, Schulz A, Mathey DG, Boxberger M, Degenhardt R, Scheller B, Strasser RH. Clin Res Cardiol. 2016 Jan 14.
- López Mínguez JR, Nogales Asensio JM, Doncel Vecino LJ, Sandoval J, Romany S, Martínez Romero P, Fernández Díaz JA, Fernández Portales J, González Fernández R, Martínez Cáceres G, Merchán Herrera A, Alfonso Manterola F; BABILON Investigators. A prospective randomised study of the paclitaxel-coated balloon catheter in bifurcated coronary lesions (BABILON trial): 24-month clinical and angiographic results. EuroIntervention. 2014 May;10(1):50-7.
- Ormiston JA, Webber B, Ubod B, Webster MW, White J. Absorb everolimus-eluting bioresorbable scaffolds in coronary bifurcations: a bench study of deployment, side branch dilatation and post-dilatation strategies. EuroIntervention. 2015 Feb;10(10):1169-77.
- Ormiston JA, Webber B, Ubod B, Darremont O, Webster MW. An independent bench comparison of two bioresorbable drug-eluting coronary scaffolds (Absorb and DESolve) with a durable metallic drug-eluting stent (ML8/Xpedition). EuroIntervention. 2015 May;11(1):60-7.
- Onuma Y, Katagiri Y, Burzotta F, Holm N.R., Amabile N, Okamura T, Mintz GS, Darremont O, Lassen JF, Lefèvre T, Louvard Y, Stankovic G, Serruys PW. Joint consensus on the use of OCT in coronary bifurcation lesions by the European and Japanese bifurcation clubs. EuroIntervention 2019;14:e1568-e1577
- Zhou Y, Chen S, Huang L, Hildick-Smith D, Ferenc M, Jabbour R J, Azzalini L, Colombo A, Chieffo A, Zhao X. Definite stent thrombosis after drug-eluting stent implantation in coronary bifurcation lesions: A meta-analysis of 3,107 patients from 14 randomized trials. Catheter Cardiovasc Interv. 2018;92:680–691.
- Hildick-Smith D, Behan MW, Lassen JF, Chieffo A, Lefèvre T, Stankovic G, Burzotta F, Pan M, Ferenc M, Bennett L, Hovasse T, Spence MJ, Oldroyd K, Brunel P, Carrie D, Baumbach A, Maeng M, Skipper N, Louvard Y. The EBC TWO Study (European Bifurcation Coronary TWO): A Randomized Comparison of Provisional T-Stenting Versus a Systematic 2 Stent Culotte Strategy in Large Caliber True Bifurcations. Circ Cardiovasc Interv. 2016;9(9).
- Ormiston JA, Kassab G, Finet G, Chatzizisis YS, Foin N, Mickley TJ, Chiastra C, Murasato Y, Hikichi Y, Wentzel JJ, Darremont O, Iwasaki K, Lefèvre T, Louvard Y, Beier S, Hojeibane H, Netravali A, Wooton J, Cowan B, Webster MW, Medrano-Gracia P, Stankovic G. Bench testing and coronary artery bifurcations: a consensus document from the European Bifurcation Club. EuroIntervention. 2018;13(15):e1794-e1803.
- Flensted Lassen J, Burzotta F, Banning A, Lefèvre T, Darremont O, Hildick-Smith D, Chieffo A, Pan M, Holm N.R., Louvard Y, Stankovic G. Percutaneous coronary intervention for the left main stem and other bifurcation lesions: 12th consensus document from the European Bifurcation Club. EuroIntervention2018;13:1540-1553.
- Burzotta F, Lassen JF, Banning AP, Lefèvre T, Hildick-Smith D, Chieffo A, Darremont O, Pan M, Chatzizisis YS, Albiero R, Louvard Y, Stankovic G. Percutaneous coronary intervention in left main coronary artery disease: the 13th consensus document from the European Bifurcation Club. EuroIntervention. 2018;14(1):112-120.
- Behan MW, Holm NR, de Belder AJ, Cockburn J, Erglis A, Curzen NP, Niemelä M, Oldroyd KG, Kervinen K, Kumsars I, Gunnes P, Stables RH, Maeng M, Ravkilde J, Jensen JS, Christiansen EH, Cooter N, Steigen TK, Vikman S, Thuesen L, Lassen JF, Hildick-Smith D. Coronary bifurcation lesions treated with simple or complex stenting: 5-year survival from patient-level pooled analysis of the Nordic Bifurcation Study and the British Bifurcation Coronary Study. Eur Heart J. 2016 Jun 21;37(24):1923-8.